Embed Size (px)
Citation preview

Paper Title: THEORETICAL APPROACH TO ELECTRONIC PRESCRPTION SYSTEM
IN WOLAITA SODO UNIVERSITY REFERAL HOSPITAL
Author Name/s Mesfin Leranso Betalo
Affiliation: (PHD Scholar, Msc IT ,Bsc Comp.Sc)
City: Wolaita Sodo
Country: Ethiopia
Email: [email protected]
International Journal of Advancements in Research & Technology, Volume 7, Issue 11, November-2018 ISSN 2278-7763 25
IJOART Copyright © 2018 SciResPub.
IJOART

ABSTRACT WHO has defined health as “a state complete physical, mental, and social well-being and not the
mere absence of diseases or infirmity”. It is generally concerned with the anatomical integrity
and physiological functioning of the body. It means the ability to perform routine tasks without
any physical restriction. The fault in the process of prescription causes many deaths
The tendency to use advanced technology in Wolaita Sodo University Referral hospital have put
forward electronic prescription. Electronic prescription is considered as the main solution to
overcome the major drawbacks of the paper-based medication prescription, such as
transcription errors. This study aims to provide practical information concerning electronic
prescription system to a variety of stakeholders.
Methods: In this review study, The Method and techniques used to analyze the existing system
and designing electronic system includes, interview, document analysis, practical observation
Results: There are many problems with the paper prescription system which, according to
studies have jeopardized patients‟ safety and negatively affected the outcomes of medication
therapy. All of these problems are remedied through the implementation of e-prescriptions.
Conclusions: The sophistication of electronic prescription and integration with EHR will
become a reality, if all its stakeholders collaborate in developing fast and secure electronic
prescription systems. This will result in widespread adoption of the system.
Keywords: Electronic Prescribing; Utilization; Standards
International Journal of Advancements in Research & Technology, Volume 7, Issue 11, November-2018 ISSN 2278-7763 26
IJOART Copyright © 2018 SciResPub.
IJOART

1. Introductions
WHO has defined health as “a state complete physical, mental, and social well-being and not the
mere absence of diseases or infirmity”. It is generally concerned with the anatomical integrity
and physiological functioning of the body. It means the ability to perform routine tasks without
any physical restriction. The fault in the process of prescription causes many deaths In addition
to natural diseases, which I am going to deal it.
I believe that the basis for improving hospital operation is shifting the day to day manual
operation of the hospital into computer based system but it is true that the majority enterprises
that is found in Ethiopia does not use computer base system as a result I can be a witness for the
problem occurred due to the manual system they use and the time it take to perform the day to
day operation.
From this perspective when I look at the Electronic prescription process in the Wolaita Sodo
University Teaching Referral Hospital and as a general, which is delivered through manual have
many errors.
These errors result from a number of factors. The most frequent source of error is
miscommunication between the provider and the pharmacist. Communication errors stem most
often from illegible handwriting, unclear abbreviations and dose indications, unclear telephone
or verbal orders, and ambiguous orders and problems. Unreadable or vague prescriptions result
in unsuspected and large amount of patient deaths.
Finally, by observing this problem I am motivated to analyses and works on manual system
prescription process to s electronic prescription process in the hospital (EPCS).
Prescription is task of a doctor in which it is the process of giving treatment to the diseases.
This process involves analyzing and writing patient history or patient chief compliance, writing
diagnose, give appropriate treatment (Rx) to the diagnosed diseases, making some calculation of
dosage specially for pediatrics, analyzing drug appropriateness (contraindication, indication,
allergy, and extra), and finally transmitting the treatment to the dispenser.
E-prescription is the processing of a drug prescription in an electronic form, starting from the
medical professional prescribing the drug and ending with the actual dispensing to the patient,
including the process of drug selection and demand, with the data always stored electronically.
E-Prescribing can be defined as “entering a prescription for a medication into an automated data
entry system (handheld, PC, or other), and thereby generating a prescription electronically,
instead of handwriting the prescription on paper”
E-Prescription is a tool for prescribers to electronically send an accurate, error-free and
understandable prescription directly to a pharmacy from the point-of-care. It allows the patient to
improve the safety through electronically checking patient allergies contraindication etc, security
and accuracy of his prescriptions, save his time during handling prescription renewals by making
it electronically with his pharmacy.
International Journal of Advancements in Research & Technology, Volume 7, Issue 11, November-2018 ISSN 2278-7763 27
IJOART Copyright © 2018 SciResPub.
IJOART
2. Literature reviews
2.1 Electronic Prescription
2.1.2 The Concept of Electronic Prescription
Electronic prescription is a reality far beyond the simply using computers to write and save
prescriptions . In fact, electronic prescription (e-prescription) is a broad term that means using
the computer devices to enter, modify, review and generate or transmit medication prescriptions
that prepare two-way transmissions between the point of care and the dispenser. This form of
technology would safely transmit prescription or prescription-related information between
stakeholders (prescribers, dispensers, pharmacies, health plans, and health insurers) either
directly or through an intermediary (including an electronic prescription network) using
electronic media. E-prescription transfers prescriptions from prescribers to pharmacies, refills
and renewals requests from pharmacies to providers, prescription benefit and formulary
information and fills status notification for prescribers. Therefore, the utilization of electronic
systems in prescription can facilitate the communication of a prescription, aid the choice, and
supply the medication by decision support and finally provides a robust audit trail for the entire
medication process.
There are several main steps in creating and managing prescriptions electronically. Firstly, a user
of the system signs in by some sort of authentication to prove his or her identification. In the next
step, a clinician identifies a patient within the electronic prescription system and the electronic
prescription process begins. These data should be readily available to the clinician prior to
entering new prescriptions. Different devices in multiple environments are used in three
activities of the electronic prescription process, such as selecting a medication, entering
parameters and signing the prescription. Also, clinical decision support is utilized through
reviewing alerts and reminders in these activities. Then, the verified prescription was directly or
indirectly transferred to pharmacy for dispensing. Prescription Refill and renewal requests are
also automated in e-prescription cycle, illustrated in Figure 1. Moreover, prescription claims are
transmitted electronically from pharmacy to payers.
International Journal of Advancements in Research & Technology, Volume 7, Issue 11, November-2018 ISSN 2278-7763 28
IJOART Copyright © 2018 SciResPub.
IJOART

Fig 1. Modeling diagram of Electronic Prescription System.
International Journal of Advancements in Research & Technology, Volume 7, Issue 11, November-2018 ISSN 2278-7763 29
IJOART Copyright © 2018 SciResPub.
IJOART

2.4 The Role Player of the E-Prescription System
Player represents anything or anyone participates in the system. This may include people,
external system, and other organization. In the existing prescription system there are different
players namely patient, prescriber or doctor or dispensers and porter. The above-mentioned
players are discussing below:
Patient
The patient tells the porter about their basic demography to be registered as history and describe
their chief compliance to the doctor, and also tells whether they have taken any drug, any history
of allergy or hyper sensitivity to a certain drug if any and if they know. After this they will buy
the drug prescribed for them from pharmacy.
prescriber
The prescriber will go over the contra indications and drug-drug interactions, checking dosage of
the drug being prescribed, consider cost of the drug and potency of the drug and consider all
patient history to write prescription.
Dispenser
They read the prescription and they will give prescribed drug and tell patients or their attendants
how to take the drug. If they have questions, vague prescription, and refill request they will
return it to the prescriber. If the prescribed drug is not available he informs his patient to by the
drug from outside.
Porter
When the patient comes to the hospital the porter will attends him and take his patient
demography and assign appropriate OPD depending on his case.
2.5 Class Diagram for Practical Approach
The researcher used this diagram to identify the Classes and its attributes and the
operation as follows which helps for design level of class diagram.
International Journal of Advancements in Research & Technology, Volume 7, Issue 11, November-2018 ISSN 2278-7763 30
IJOART Copyright © 2018 SciResPub.
IJOART
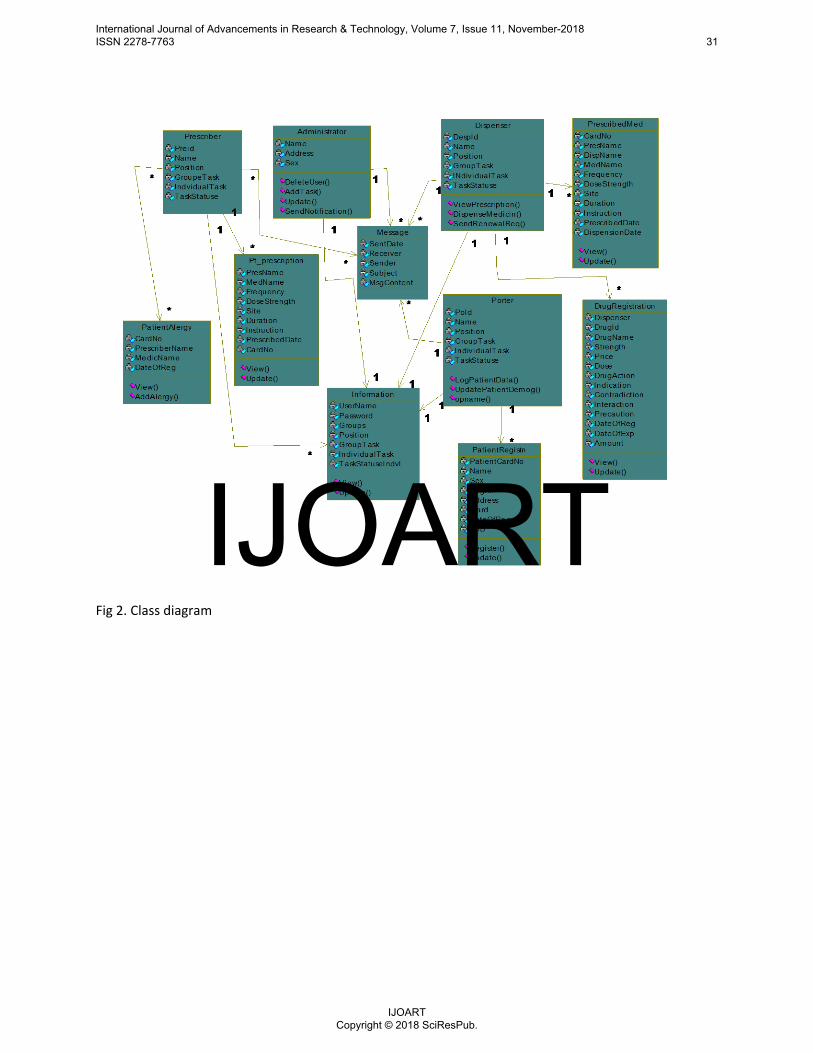
Fig 2. Class diagram
International Journal of Advancements in Research & Technology, Volume 7, Issue 11, November-2018 ISSN 2278-7763 31
IJOART Copyright © 2018 SciResPub.
IJOART
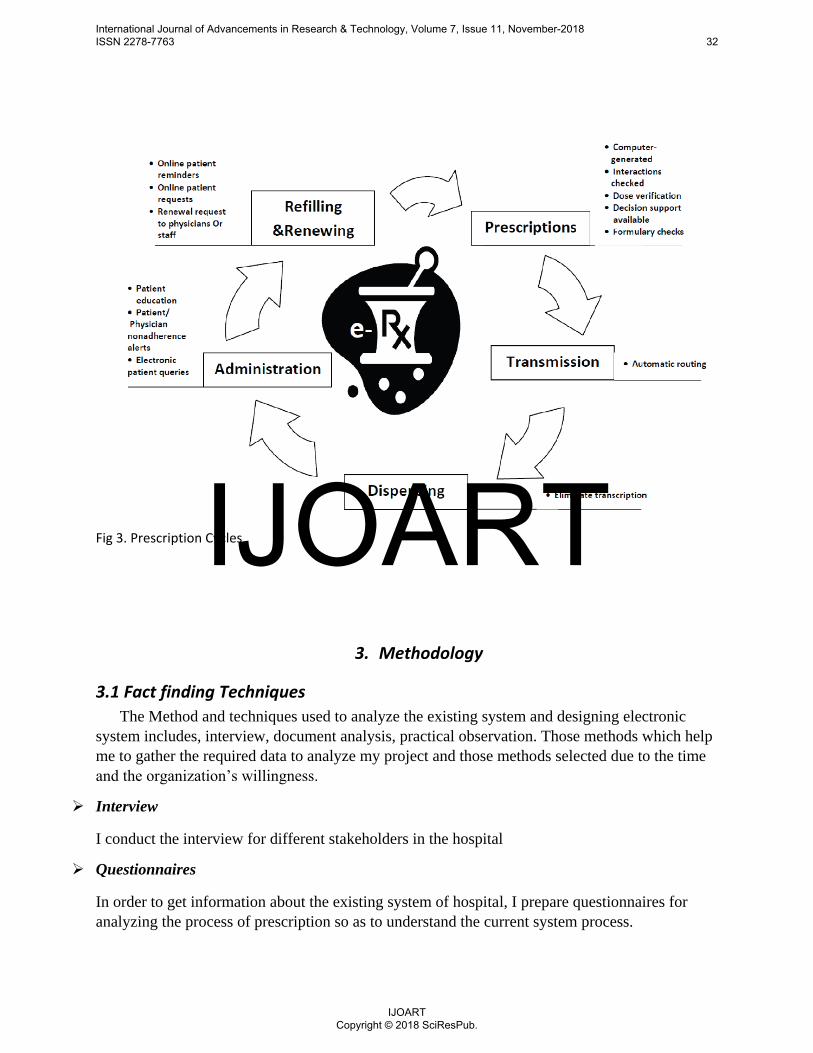
Fig 3. Prescription Cycles
3. Methodology
3.1 Fact finding Techniques
The Method and techniques used to analyze the existing system and designing electronic
system includes, interview, document analysis, practical observation. Those methods which help
me to gather the required data to analyze my project and those methods selected due to the time
and the organization‟s willingness.
Interview
I conduct the interview for different stakeholders in the hospital
Questionnaires
In order to get information about the existing system of hospital, I prepare questionnaires for
analyzing the process of prescription so as to understand the current system process.
International Journal of Advancements in Research & Technology, Volume 7, Issue 11, November-2018 ISSN 2278-7763 32
IJOART Copyright © 2018 SciResPub.
IJOART
Data collection
Observations were conducted by a Medical, Nursing and pharmacy student, aiming to collect
data across a range of scheduled drug rounds, and to be as unobtrusive as possible. Nurses gave
verbal consent prior to being observed. The study was approved locally as a service evaluation;
research ethics approval was not required.
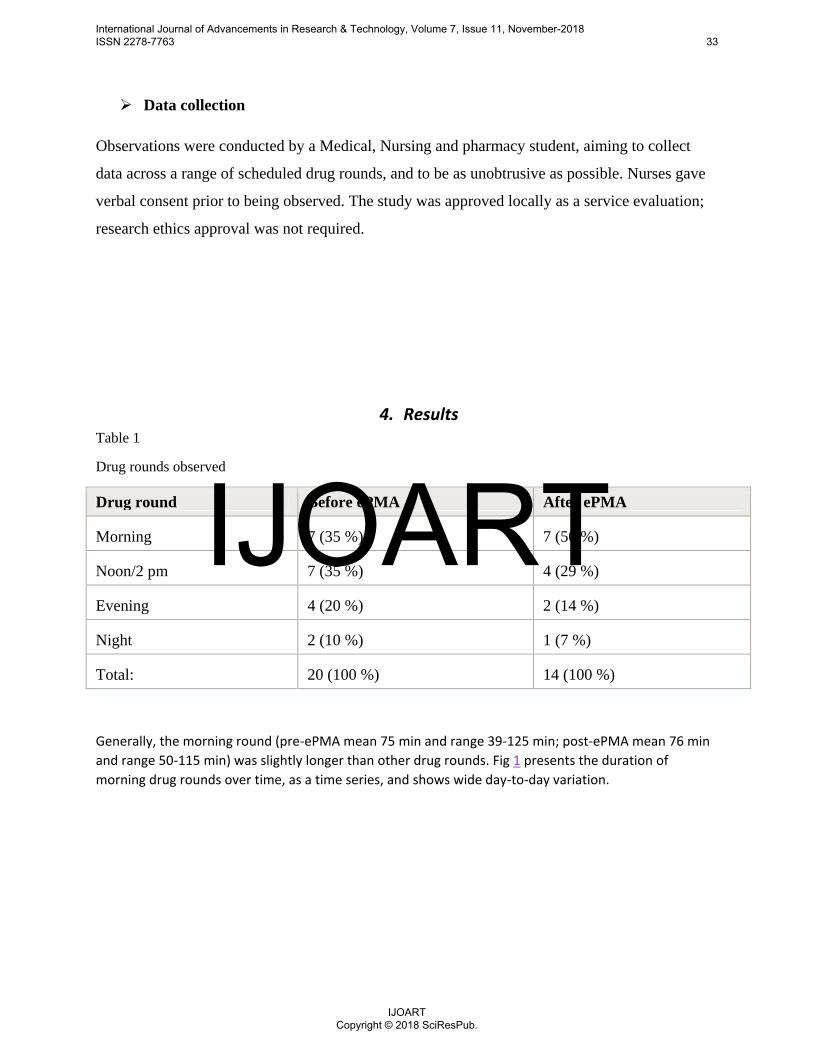
4. Results Table 1
Drug rounds observed
Drug round Before ePMA After ePMA
Morning 7 (35 %) 7 (50 %)
Noon/2 pm 7 (35 %) 4 (29 %)
Evening 4 (20 %) 2 (14 %)
Night 2 (10 %) 1 (7 %)
Total: 20 (100 %) 14 (100 %)
Generally, the morning round (pre-ePMA mean 75 min and range 39-125 min; post-ePMA mean 76 min
and range 50-115 min) was slightly longer than other drug rounds. Fig 1 presents the duration of
morning drug rounds over time, as a time series, and shows wide day-to-day variation.
International Journal of Advancements in Research & Technology, Volume 7, Issue 11, November-2018 ISSN 2278-7763 33
IJOART Copyright © 2018 SciResPub.
IJOART
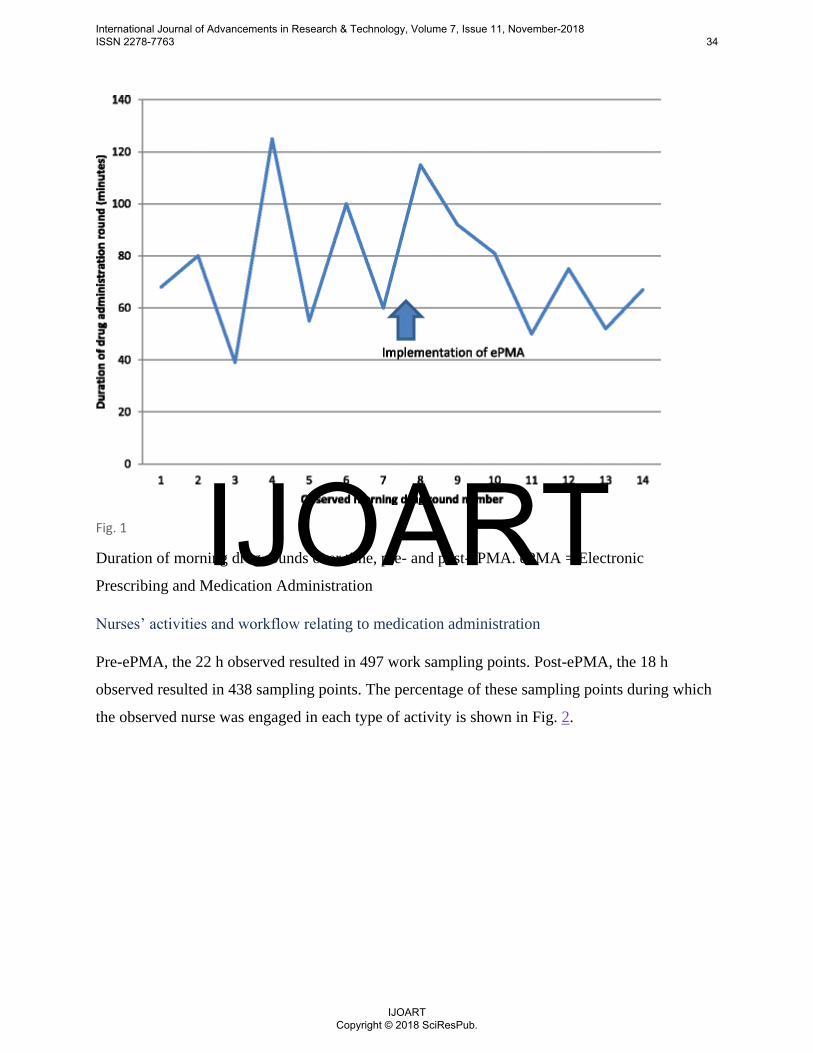
Fig. 1
Duration of morning drug rounds over time, pre- and post-ePMA. ePMA = Electronic
Prescribing and Medication Administration
Nurses‟ activities and workflow relating to medication administration
Pre-ePMA, the 22 h observed resulted in 497 work sampling points. Post-ePMA, the 18 h
observed resulted in 438 sampling points. The percentage of these sampling points during which
the observed nurse was engaged in each type of activity is shown in Fig. 2.
International Journal of Advancements in Research & Technology, Volume 7, Issue 11, November-2018 ISSN 2278-7763 34
IJOART Copyright © 2018 SciResPub.
IJOART
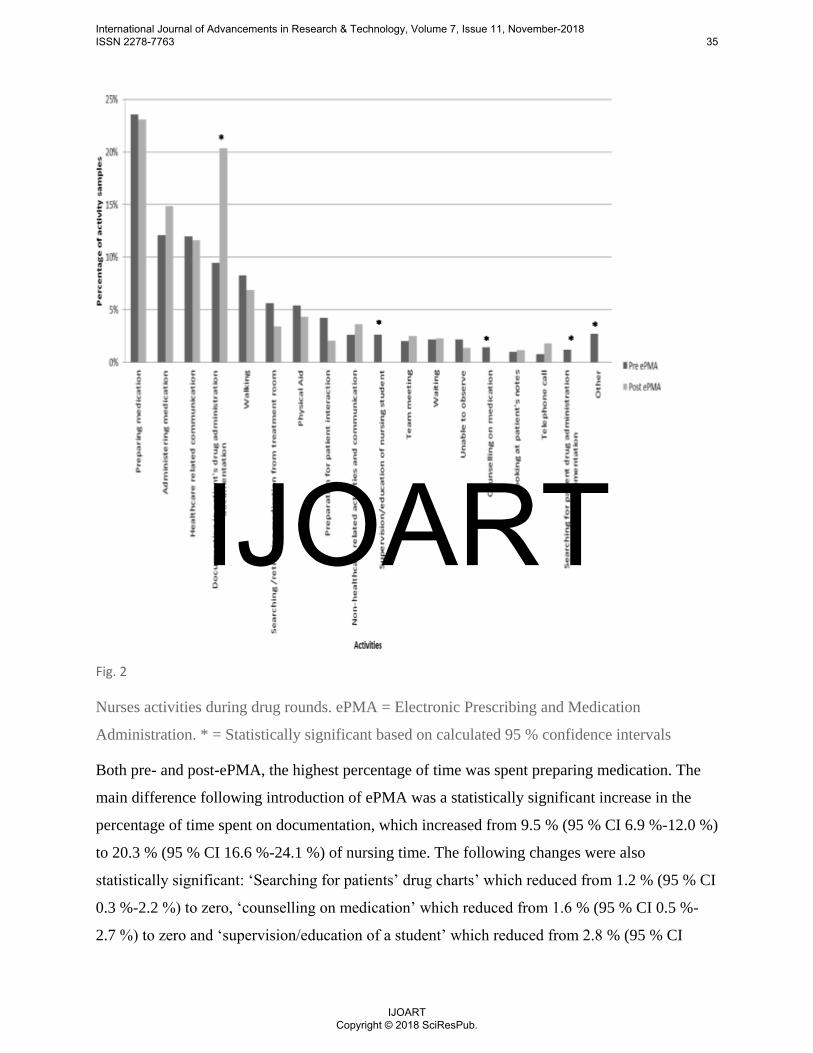
Fig. 2
Nurses activities during drug rounds. ePMA = Electronic Prescribing and Medication
Administration. * = Statistically significant based on calculated 95 % confidence intervals
Both pre- and post-ePMA, the highest percentage of time was spent preparing medication. The
main difference following introduction of ePMA was a statistically significant increase in the
percentage of time spent on documentation, which increased from 9.5 % (95 % CI 6.9 %-12.0 %)
to 20.3 % (95 % CI 16.6 %-24.1 %) of nursing time. The following changes were also
statistically significant: „Searching for patients‟ drug charts‟ which reduced from 1.2 % (95 % CI
0.3 %-2.2 %) to zero, „counselling on medication‟ which reduced from 1.6 % (95 % CI 0.5 %-
2.7 %) to zero and „supervision/education of a student‟ which reduced from 2.8 % (95 % CI
International Journal of Advancements in Research & Technology, Volume 7, Issue 11, November-2018 ISSN 2278-7763 35
IJOART Copyright © 2018 SciResPub.
IJOART
1.4 %-4.3 %) to zero. The change in time spent supervising students is due to the student nurses‟
rotations changing over the course of the study which meant that no students remained on the
wards following ePMA implementation.
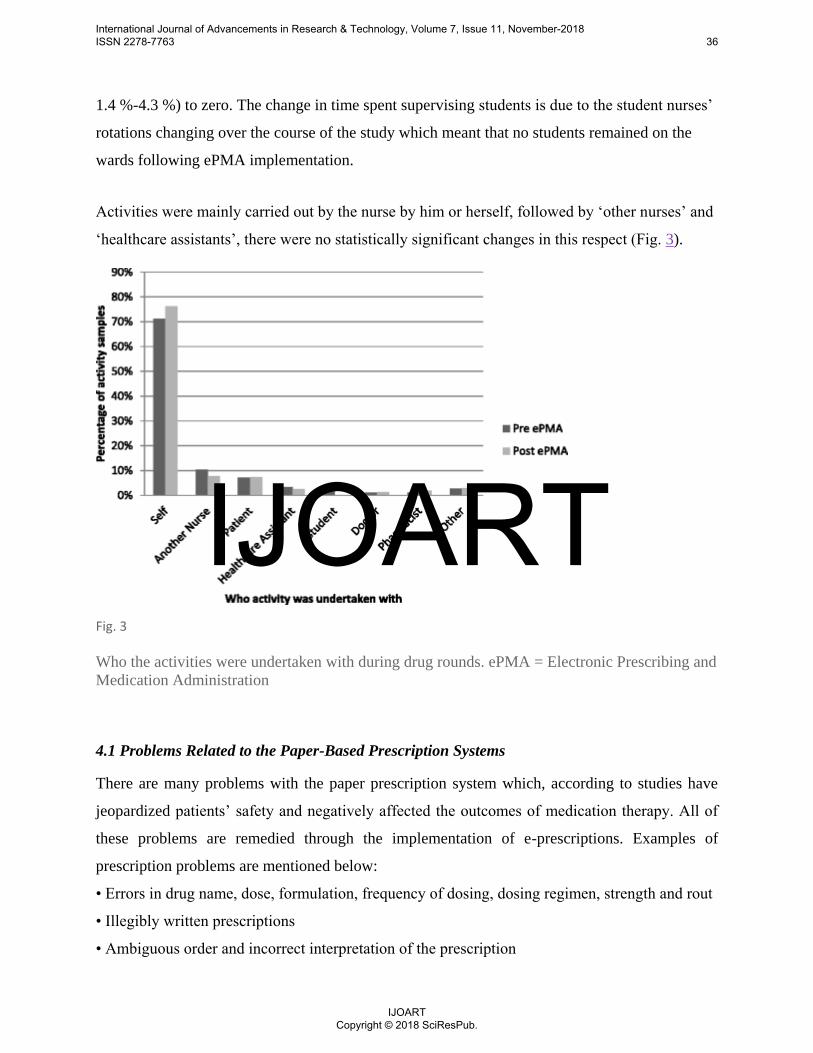
Activities were mainly carried out by the nurse by him or herself, followed by „other nurses‟ and
„healthcare assistants‟, there were no statistically significant changes in this respect (Fig. 3).
Fig. 3
Who the activities were undertaken with during drug rounds. ePMA = Electronic Prescribing and
Medication Administration
4.1 Problems Related to the Paper-Based Prescription Systems
There are many problems with the paper prescription system which, according to studies have
jeopardized patients‟ safety and negatively affected the outcomes of medication therapy. All of
these problems are remedied through the implementation of e-prescriptions. Examples of
prescription problems are mentioned below:
• Errors in drug name, dose, formulation, frequency of dosing, dosing regimen, strength and rout
• Illegibly written prescriptions
• Ambiguous order and incorrect interpretation of the prescription
International Journal of Advancements in Research & Technology, Volume 7, Issue 11, November-2018 ISSN 2278-7763 36
IJOART Copyright © 2018 SciResPub.
IJOART
• Unclear telephone or verbal orders
• Prescriptions issued to the wrong patient
• Missing prescriber or patient data
• Omission of medication, high rate of prescription fraud imposing costs on pharmacies
• Rewriting prescriptions in physicians‟ offices and pharmacies
• Re-entering all the prescription details into pharmacy and paying system by hand
• Giving potential rise to re-keying errors
• Incompleteness of information on patient medication histories
• Repetitive medication treatment
• Miscommunication due to illegible handwriting in ordering, distributing and administering of
medications
• Unclear abbreviations and dose designations
• Poor tools for managing adverse drug interactions
• High rate of adverse drug reactions
• Complexity of medication selection due to wide variety of pharmaceutical products
• High cost for handling prescriptions
• Risk of losing, damaging and hefting a paper prescription
5. Conclusions:
The sophistication of electronic prescription and integration with EHR will become a reality,
if all its stakeholders collaborate in developing fast and secure electronic prescription
systems. It is plausible that the required infrastructure should be provided for implementation
of the national integrated electronic prescription systems in countries without the system.
Given the barriers to the implementation and use, policymakers should consider multiple
strategies and offer incentives to encourage e-prescription initiatives. This will result in
widespread adoption of the system.
International Journal of Advancements in Research & Technology, Volume 7, Issue 11, November-2018 ISSN 2278-7763 37
IJOART Copyright © 2018 SciResPub.
IJOART
5. Recommendations and Suggestions
The related studies performed in Wolaita Sodo University Teaching Referral Hospital have
highlighted a high frequency of medication error, quantitative and qualitative problems and
imperfections in the current prescription system. Moreover, these studies have emphasized on the
impact of computerized provider order entry (CPOE) on reducing medication error and
improving patient safety, and also the patients' willingness to refill their prescriptions
electronically and obtain more information about the administration of medication via
information technology.
6. Reference
1. NHS Connecting for Health (2007). ePrescribing functional specification for NHS
Trusts. http://www.connectingforhealth.nhs.uk/systemsandservices/eprescribing/
baselinefunctspec.pdf Accessed 5 December 2008.
2. Hellstrom L, Waern K, Montelius E, Astrand B, Rydberg T, Petersson G. Physicians'
attitudes towards ePrescribing--evaluation of a Swedish full-scale implementation. BMC Med
Inform Decis Mak. 2009;9:37.
3. Joia LA, Magalhaes C. Implementation of an electronic prescription system in Brazilian
general hospital: understanding source of resistance. EJISDC. 2009;39(2):1-18.
4. Cusack CM. Electronic health records and electronic prescribing: promise and pitfalls. Obstet
Gynecol Clin North Am. 2008;35(1):63-79.
5. Griffin JP. Venetian treacle and the foundation of medicines regulation. Br J Clin
Pharmacol. 2004;58(3):317-25.
6. Hypponen H, Salmivalli L, Sumi R. Organizing for a national infrastructure project: the case
of the Finnish electronic prescription; Proceeding of the 38th Hawaii international conference
on system science; 3-6 January 2005; Hilton Waikoloa Village, Big Island, Hawaii. 2005.
7. Adang E, Voordijk L, Jan van der Wilt G, Ament A. Cost-effectiveness analysis in relation to
budgetary constraints and reallocative restrictions. Health Policy. 2005;74(2):146-56.
8. Phillips DP, Christenfeld N, Glynn LM. Increase in US medication-error deaths between
1983 and 1993. The Lancet. 1998;351(9103):643- 644.
9. Institiute of Medicine. To err is human: building a safer health system. Washangton DC:
2000. Available from: http://www.pro-
International Journal of Advancements in Research & Technology, Volume 7, Issue 11, November-2018 ISSN 2278-7763 38
IJOART Copyright © 2018 SciResPub.
IJOART

vidersedge.com/ehdocs/ehr_articles/to_err_is_human_%20 building_a_safer_health_system-
exec_summary.pdf.
10. Mosleh A, Darbooy SH, Khoshnevis Ansari SH, Mohammadi M. Drug prescription based on
WHO indicators: Tehran university of medical sciences facilities with pharmacy]. Teh Uni
Med J. 2007;65(2):12-15.
11. IMS Institute for Healthcare Informatics. The use of medicines in the United States: Review
of 2010 USA. [updated 13 Jan 2013];2012. Available from:
http://www.imshealth.com/imshealth/Global/Content/
IMS%20Institute/Documents/IHII_UseOfMed_report%20.pdf.
12. Oliven A, Michalake I, Zalman D, Dorman E, Yeshurun D, Odeh M. Prevention of
prescription errors by computerized, on-line surveillance of drug order entry. Int J Med
Inform. 2005;74(5):377-86.
13. Dean B, Schachter M, Vincent C, Barber N. Causes of prescribing errors in hospital
inpatients: a prospective study. The Lancet. 2002;359(9315):1373-78.
14. Costa AL, de Oliveira MM, Machado Rde O. An information system for drug prescription
and distribution in a public hospital. Int J Med Inform. 2004;73(4):371-81.
15. Ekedahl A. Problem prescriptions in Sweden necessitating contact with the prescriber before
dispensing. Res Social Adm Pharm.
2. Han YY, et al. Unexpected increased mortality after implementation of a commercially sold
computerized physician order entry system”, Pediatrics 2005;116 (6): 1506-12.
To do this system starting from the requirement analysis to the implementation I used the
following materials.
Glossary
o CPOE computerized provider order entry
o SQL: Structural Query Language
o ID Identification Card
o UML: Unified Modeling Language
o UI: User Interface
International Journal of Advancements in Research & Technology, Volume 7, Issue 11, November-2018 ISSN 2278-7763 39
IJOART Copyright © 2018 SciResPub.
IJOART





























