Embed Size (px)
Citation preview

33ournal ofNeurology, Neurosurgery, and Psychiatry 1997;62:334-340
Pathogenesis of cervical spondylotic myelopathy
David N Levine
AbstractObjective-To determine whether eitherof two mechanical theories predicts thetopographic pattern of neuropathology incervical spondylotic myelopathy (CSM).The compression theory states that thespinal cord is compressed between aspondylotic bar anteriorly and the liga-menta flava posteriorly. The dentate ten-sion theory states that the spinal cord ispulled laterally by the dentate ligaments,which are tensed by an anterior spondy-lotic bar.Methods-The spinal cord cross section,at the level of a spondylotic bar, is mod-elled as a circular disc subject to forcesapplied at its circumference. These forcesdiffer for the two theories. From the pat-tern of forces at the circumference thedistribution of shear stresses in the inte-rior of the disc-that is, over the trans-verse section of the spinal cord-iscalculated. With the assumption thathighly stressed areas are most subject todamage, the stress pattern predicted byeach theory can be compared to the topo-graphic neuropathology of CSM.Results-The predicted stress pattern ofthe dentate tension theory corresponds tothe reported neuropathology, whereas thepredicted stress pattern of the compres-sion theory does not.Conclusions-The results strongly favourthe theory that CSM is caused by tensilestresses transmitted to the spinal cordfrom the dura via the dentate ligaments.A spondylotic bar can increase dentatetension by displacing the spinal cord dor-sally, while the dural attachments of thedentate, anchored by the dural rootsleeves and dural ligaments, are displacedless. The spondylotic bar may alsoincrease dentate tension by interferinglocally with dural stretch during neckflexion, the resultant increase in duralstress being transmitted to the spinal cordvia the dentate ligaments.
Flexion of the neck increases dural ten-sion and should be avoided in the conserv-ative treatment of CSM. Both anteriorand posterior extradural surgical opera-tions can diminish dentate tension, whichmay explain their usefulness in CSM.The generality of these results must be
tempered by the simplifying assumptionsrequired for the mathematical model.
(7 Neurol Neurosurg Psychiatry 1997;62:334-340)
Keywords: myelopathy; cervical spondylosis; biome-chanics
The pathogenesis of cervical spondyloticmyelopathy (CSM) is still not firmly estab-lished, even though CSM is a very commonand well known condition. Several theories ofpathogenesis have been proposed, but therehas been no conclusive demonstration thatany one theory explains the reported neu-ropathology better than the others. The pur-pose of this paper is to review the varioustheories of pathogenesis, to determine whatpathology each predicts, and to decide whichtheory, if any, best explains the neuropatho-logical findings.The oldest' and still most often cited theory
is that CSM is caused by mechanical com-pression. It is thought that the spinal cord iscompressed between a spondylotic bar anteri-orly' and the ligamenta flava posteriorly.2 Thespinal cord is most vulnerable to such com-pression during extension of the neck, whenthe ligamenta flava bulge into the spinalcanal,3 decreasing its anteroposterior depth,while the anteroposterior dimension of thespinal cord itself increases.4 People with con-genitally narrow spinal canals are more vul-nerable to this pinching of the spinal cordbetween an anterior spondylotic bar and theposterior ligamenta flava.A second mechanical theory5 is that CSM is
caused by tensile stresses transmitted to thespinal cord from the dentate ligaments, whichattach the lateral pia to the lateral dura. Thespondylotic bar displaces the spinal cord pos-teriorly, but this displacement is resisted bythe dentate ligaments. The dural attachmentsof the dentate ligaments provide a fixed point,so that dentate tension can increase when thespinal cord is displaced posteriorly. The duralattachments do not move because the duralsac is constrained by the dural root sleeves,which are held fixed in the neural foramina.The spinal cord is most vulnerable duringflexion of the neck, when the dura is unfolded,and the nerve roots and dentate ligaments arerelatively taut.4The major non-mechanical theories are
vascular. They have arisen not because ofevidence of vascular occlusion in any neu-ropathological study of CSM, but ratherbecause of the assumed inability of themechanical theories to predict the pathologi-cal lesions. For example, Greenfield,6 whileacknowledging a role for mechanical damage,thought that ischaemia was needed to accountfor the lesions in the ventral portions of the
Department ofNeurology, New YorkUniversity MedicalCenter, New York,USAD N LevineCorrespondence to:Dr David N Levine, RIRM311, 400 E 34 Street, NYC,NY 10016, USA.Received 12 February 1996and in revised form10 September 1996Accepted 11 November 1996
334 on A
ugust 3, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.62.4.334 on 1 April 1997. D
ownloaded from

Pathogenesis of cervical spondylotic myelopathy
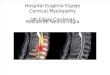
Figure 1 Topography ofneuropathology ofCSM.The top row shows myelinstained cross sections of thespinal cord at the level ofaspondylotic barfrom tworepresentative cases studiedat postmortem. On the leftis case 4 ofBrain et al 9and on the right is case 3ofMair and Druckman.'On the bottom is aschematic diagramadaptedfrom Ogino et al'3with permission. The darkshading indicates the mostvulnerable areas, affectedin even mild cases, theintermediate shadingdesignates moderatelyvulnerable regions, and thelight shading indicatesareas damaged only insevere cases. The unshadedareas are spared.
posterior columns that are often present insevere cases. Both arterial and venousischaemic mechanisms have been discussed.Mair and Druckman7 suggested that compres-sion of the anterior spinal artery and itsbranches in the spinal cord caused CSM.Taylor8 considered that compression of theradicular arteries in the intervertebral foram-ina caused CSM. Brain et a19 thought thatcompression of veins on the anterior aspect ofthe spinal cord by a spondylotic bar wasimportant.
Despite the lack of consensus regardingpathogenesis there is little disagreement aboutthe neuropathological findings (fig 1) inCSM.7 9-13 The spinal cord at the level of thespondylotic bar is flattened in the anteropos-terior dimension but not in the transversedimension. The damage is most severe incross sections at the level of the spondyloticbar. There the lateral columns are the mostvulnerable, and in them the involved areas areoften wedge shaped with the apex medial andthe base lateral. In more severe cases the dam-age extends further medially to involve theintermediate portions of the grey matter andthe ventral portions of the posterior columns.Microscopically, there is demyelination andgliosis of the affected white matter and loss ofnerve cells and gliosis in the affected grey mat-ter. Above and below the level of the spondy-lotic bar the damage becomes progressivelyless severe, and Wallerian degeneration is seenin the posterior columns rostral to the level ofcompression and in the lateral columns caudalto it.
I have developed a model of the spinal cordthat allows calculation of the pattern ofstresses in the cross section of the cord at thelevel of an anterior spondylotic bar. The pur-pose of this paper is to present these calcula-tions and to compare the predicted stresseswith the topography of the neuropathologicaldamage. In this manner it should be possibleto decide whether one, both, or none of themechanical theories should be accepted.
MethodsThe spinal cord at the level of a spondyloticbar is modelled as a circular disc subject toforces applied at its circumference. The loca-tion and nature of these forces differ in the twomechanical theories. Both have in common ananterior compressive force produced by thespondylotic bar. The first theory (fig 2A) pos-tulates bilateral posteriorly applied compres-sive forces directed anteriorly and slightlymedially, produced by the ligamenta flava.The second theory (fig 2B) postulates laterallyapplied tensile forces directed laterally andslightly anteriorly, produced by the dentate lig-aments. These two different patterns ofapplied force will produce two different distrib-utions of stress in the spinal cord cross section.The stress at any point in the disc can be
resolved into two parts: a uniform pressure ortension and a pure shear. Because nervous tis-sue is relatively incompressible, little harm iscaused by changes in the uniform pressure.'4It is the shear stress, which causes distortionor deformation of nerve tissue, that results intissue damage.'5 In an isotropic medium thedistribution of damage should correspond tothe topographic distribution of the shearstresses. Each mechanical theory predicts aspecific distribution of shear stresses over theinvolved cross section of the spinal cord. Acomparison of the predicted distributions withthe neuropathological data may therefore be atest of the theory's validity.The stresses are calculated as follows (fig
2G):(1) A coordinate system is established withthe origin at the centre of the circular spinalcord cross section. The x axis is positive ante-riorly, and they axis is positive to the right.(2) The locations of the forces at the circum-ference are specified in terms of their x-y coor-dinates. The direction of each force isdesignated by the angle it makes with the xaxis. The magnitudes of the forces are con-strained by the requirements of mechanicalequilibrium. Specifically:
335
4:v-
on August 3, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.62.4.334 on 1 A
pril 1997. Dow
nloaded from

336 Levine
B
L R F5
F,
Anterior
The magnitude of each force is constrained tobe:
F4 = F, = }cos60(3) At a given interior point (x, y) of the spinalcross section the stress is determined by sum-
F4 L ming the contributions of the three forces atAl the circumference. To determine the contribu-
tion of a single force, the arc length over whichit is distributed is divided into a large numberN of small, equal segments. The force at eachelement, of magnitude
F,f = N (i = l to 5)N
C
Txy; >
x
Txy_1-io
r~~~~~~~f
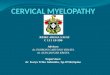
Figure 2 (A) The compressive model and (B) the dentate tension model ofCSM. F, isthe force exerted by the spondylotic bar, F2 and F, are the forces exerted by the ligamentaflava, and F4 and F, are the forces exerted by the dentate ligaments. R = right, L = left,Ant = anterior. (C) Variables used in calculating stresses. f represents one element of thedistributedforce F,, r is the radial distance from the point of application off to the point(x, y), represented by the small circle, a is the angle between r and the direction off, andis the angle between the direction offand the tangent to the disc at the point of applicationoff The small triangle surrounding (x, y), with one side parallel to r, a second sideperpendicular to r, and a third side parallel to the x axis, is used to calculate ay and T-rfrom ur and is reproduced with these stresses illustrated at the upper right. Another triangle,with the third side parallel to they axis, is used to calculate ax and is shown at the lowerright.
(a) In both models (fig 2A, B) the disc force,Fl, is applied anteriorly, uniformly distributedover an arc length of 600 centred on the x axis.It is directed posteriorly, perpendicular to thetangent to the circumference at each point ofthe arc. Its magnitude is given an arbitraryvalue 1.(b) In the first model (fig 2A) the ligamentumflavum forces F2 and F, are applied posterolat-erally, the locations of the two forces beingsymmetric with respect to the x axis. Thus F2 iscentred 300 to the left and F, 300 to the right ofthe axis. Each force is uniformly distributedover an arc length of 300. The forces aredirected anteromedially at an angle of 300 tothe x axis. The magnitude of each force isconstrained by the requirement of physicalequilibrium to be:
F2 = F, = 1cos30
(c) In the second model (fig 2B) the dentateligament forces F4 and F, are applied laterally.Each is centred 150 anterior to they axis and isdistributed uniformly over a narrow arc of 4°.The forces are directed laterally and slightlyanteriorly at an angle of 600 with the x axis.
is considered to be applied at the midpoint ofthe element. These elements are representedschematically by the arrowheads in fig 2, butfor the calculations presented here each Fi isdivided into 200 elements-that is, N = 200.The contribution at (x, y) from the jth ele-
ment (i = 1 to N) of the ith force is determinedaccording to Timoshenko.'6 It consists (fig2C) of the sum of a purely radial stress ,- anda uniform stress p,j with magnitudes
-2fcosai,1
_ fsinA3,,.7rd
where rij is the length of the ray from the pointof application of the jth element of the ithforce to the point (x, y), aij is the anglebetween the direction of the jth element of theith force and the ray of length rij, d is the diam-eter of the spinal cord, and ,Pij is the anglebetween the direction of the jth element of theith force and the tangent to the circle at thepoint of application of the force.
Because the radial stresses at (x, y) from thedifferent elements of a force differ in direction,they cannot be summed (integrated) directly.They must first be transformed into stressesreferable to a common set of directions. By thelaws of statics each radial stress aJr can betransformed into a normal stress ox in the xdirection, a normal stress aY in the y direction,and a shear stress parallel to the coordinateaxes in the x-y plane -r" (fig 2C) according tothe formulae:
, = (J,y ° 2i,,1~ 2
cry w -sin2aijj= -a,j sina,4 cosa,,
For the ith force, the normal stress in the xdirection, url, the normal stress in the y direc-tion, cr, and the shear parallel to the axes inthe x-y plane, rixy, at the point (x, y), can nowbe obtained by summation over the index j.
N N
= Iu' j+ ZPi,
N N
i= +ti+ iji=l j=1
N
i I
Summation over the index i combines the
A
F3
R
F,
Anterior
on August 3, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.62.4.334 on 1 A
pril 1997. Dow
nloaded from

Pathogenesis of cervical spondylotic myelopathy
forces to yield the total stress ax, a7,Y. for thepoint (x, y). Thus for the first model,
ax = (7X + ax, + ax2Cy = arYl + arY2 + arY3txy = -xxy+ T-y+ T3
and for the second model,
arx = rxj + afx + a'xCr = a'jy + Cr'4 + 015TXY = TXy + Tx + Xy
Finally, the maximum shear stress rm,, at thepoint (x, y) can be calculated:
Tmax= ( 2 xy2
(4) Tmax is determined for each point of the cir-cular cross section. Tmn,x can then be plottedacross the disc by converting the value at eachpoint to a value on a grey scale to facilitatecomparison with the neuropathological data.The above calculations were performed and
the graphs plotted on a Macintosh Quadra800 computer using the Matlab softwaresystem. 17
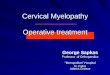
ResultsFigure 3A shows the topography of maximumshear predicted by the compressive theory.The greatest stresses cut two linear swaths thatrun predominantly in an anteroposterior direc-tion, from the ligamenta flava posterolaterallyto the spondylotic bar anteriorly. To eitherside-the central portion of the cord mediallyand the lateral columns laterally-the stress isintermediate in magnitude. Of note, the mostlateral portions of the lateral columns are rela-tively free of stress.
Figure 3B shows the topography of maxi-mum shear predicted by the theory of dentateligament tension. The greatest stresses liealong a transverse line extending from onedentate ligament to the other. Along this linethe stresses are considerably greater laterallythan medially. Thus the lateral columns aresubjected to the most stress, especially theirmost lateral portions, whereas the intermedi-ate portions of the grey matter and the ventral
portions of the posterior columns are alsostressed, but to a lesser degree. The anteriorcolumns and the dorsal portions of the poste-rior columns are relatively unstressed.
DiscussionCOMPARISON OF THE MECHANICAL THEORIESWITH NEUROPATHOLOGYIt is evident that there is a remarkable corre-spondence between the topography of theneuropathology of CSM (fig 1) and the spatialdistribution of stresses predicted by the den-tate tension hypothesis (fig 3B). By contrast,there is very little correspondence with thestresses predicted by the compression hypothe-sis (fig 3A). All neuropathological studiesagree that the lateral columns are most vulner-able to damage, especially the most lateralportions. In the dentate tension model the lat-eral portions of the lateral columns are themost highly stressed regions, whereas in thecompression model these regions sustain rela-tively little stress. As the disease processbecomes more severe, the neuropathologyextends medially to involve the spinal greymatter and the ventral portions of the poste-rior columns. In both models these regions aresubject to intermediate levels of stress. Theneuropathological studies also agree that evenin advanced CSM the anterior columns andthe posterior portions of the posterior columnsremain relatively free of disease. In the dentatetension model these areas are relatively free ofstress, whereas in the compression model theanterior columns are subject to considerablestress.
THE DENTATE TENSION HYPOTHESISThe present model of increased dentate ten-sion was designed to test the hypothesis ofKahn,5 in which the primary pathogeneticevent is stretching of the dentate ligaments as aresult of posterior displacement of the spinalcord by a spondylotic bar. The stretchingoccurs because the dural attachment of the lig-aments remains fixed, anchored by the duralroot sleeves which resist displacement of thedural sac.
Several experimental studies, in both human
Figure 3 Plot ofcalculated maximal shearstresses at each point of thecross section of the spinalcord model. Lightershading signifies greaterstress. (A) Thecompressive model; (B)the dentate tension model.R = right; L = left.
::: .:
.:... .::
-;? ,..
*: -f: °S.; 'a
*m L:.. .: ,S
.,^:,..X..5X°':Sd k:
:} <.:,:-s:: :.:. 0.
., .V
*:: :;::
B
R
Anterior
L
337
A
.:?zl-....i
R
Anteri- r
on August 3, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.62.4.334 on 1 A
pril 1997. Dow
nloaded from

Levine
cadavers and in animals, have considered thequestions of whether the dentate ligamentsconstrain posterior displacement of the spinalcord within the dural sac'8 20 and whether thenerve root sleeves anchor the dural tube to pro-vide a fixed point for the dentate ligaments toact.'9 21 The results of these studies can be syn-thesised and understood only by taking intoaccount the degree of flexion-extension of thespine. In extension the dura, the dural nerveroot sleeves, and the dentate ligaments areslack. The root sleeves do not hold the duraforward, and the dentate ligaments do not pre-vent posterior displacement of the spinal cordwithin the dural sac. In flexion, however, thespinal canal lengthens and the dura isstretched. The dural root sleeves may alsobecome taut and anchor the dural tube. Duraltension is transmitted to the dentate ligaments,which stretch the spinal cord axially and resistposterior displacement of the cord within thedural tube.
There is another means by which dentateligament tension can be increased, to which theresults of our model also apply. Any increase inlongitudinal tension in the dura is transmittedto the spinal cord as an increase in both longi-tudinal and radial tension, because the dentatefibres run mediolaterally as well as rostro-caudally. Tencer et al 21 found that although theelastic properties of the dura were uniformthroughout its length, the degree of duralstretch during flexion of the spine was muchgreater in the cervical than in the thoracic andlumbar regions. This difference in longitudinalstretch was independent of any tetheringeffects of the dural root sleeves or ligaments,because it persisted when the nerve roots andligaments were cut. Tencer et al speculatedthat friction between the dura and the anteriorsurface of the thoracic spinal canal may inter-fere with stretching of the dura and increasethe tension more rostrally. Reid'9 suggestedthat similar frictional effects may apply to flex-ion in the presence of a localised spondyloticprotrusion. Adams and Logue22 showed alocalised increase in dural stretch adjacent to apoint of dural fixation in human cadavers. Theincreased dural tension could be transmitted tothe spinal cord through the dentate ligaments.Thus the primary pathogenetic event need notbe direct pressure of the spondylotic bar on thespinal cord, but rather interference with duralstretch during flexion.
Either of these mechanisms of dentate liga-ment stress can explain two additional neu-ropathological features of CSM. Firstly, thepronounced flattening of the spinal cord in theanteroposterior dimension at the level of thespondylotic bar is probably produced by thetransmission of increased lateral and longitudi-nal tension from the dentate ligaments to thespinal cord. Because nervous tissue is relativelyincompressible the resulting longitudinal andtransverse elongations will be accompanied bya compensatory contraction in the remaininganteroposterior dimension. Secondly, thicken-ing and fibrosis have been described in thedentate ligaments, in the dura, and in the duralroot sleeves.'01123 Such fibrosis probably repre-
sents a physiological response to chronicallyraised levels of stress in these tissues.20
VASCULAR THEORIESThe close correspondence between the pre-dicted pattern of shear stress and the topogra-phy of the spinal cord pathology eliminates theneed to postulate a separate vascular hypothesis.Ironically, Kahn,5 who first postulated the den-tate tension hypothesis, gave impetus to non-mechanical hypotheses by presenting anerroneous stress analysis, in which a main"pressure wave" involved the anterior columnsin addition to other pressure waves involvingthe lateral columns. It is highly likely that thiserror was caused by failing to represent theforce exerted by the disc as distributed over theanterior part of the circumference of the cordand instead representing the force as localisedto a single point or a highly concentratedregion. When the force is represented correctlyas distributed, the anterior pressure wave dis-appears and the anterior columns remainunstressed, corresponding to their beingspared neuropathologically.
There is little or no supportive evidence formost of the vascular hypotheses. Neuro-pathology studies have rarely if ever reportedoccluded vessels. The restricted longitudinaldistribution of the spinal cord damage is evi-dence against occlusion of a vertebral artery orone of its major radicular vessels. The topogra-phy of the damage in the cross section at thelevel of the spondylosis is evidence againstocclusion of the anterior spinal artery, becausethe anterior columns are spared. Neither is thetopography of damage consistent with thehypothesis of venous congestion leading toinfarction. The slowly progressive evolution ofCSM, often over many years, is also difficult toexplain on a vascular basis, as is the not infre-quent improvement after decompressivesurgery.A mechanical hypothesis, however, can be
consistent with one type of vascular theory.Shear stresses cause tissue damage by distort-ing tissue. Thus small intramedullary vesselscan be damaged along with neurons, nerve cellprocesses, and neuroglia. Breig et a124 haveshown that transversely running blood vesselsbecome elongated as the spinal cord isstretched transversely with resulting narrowingof the vessels' cross section. Such narrowingmight cause reduction in blood flow. Theresulting ischaemia could contribute to theneuropathology.
ASSUMPTIONS AND LIMITATIONS OF THEMODELThe model that we have employed involvesseveral assumptions and simplifications.Firstly, the equations that we have used are fora homogeneous and isotropic substance, andthe spinal cord is neither homogeneous norisotropic. The main source of inhomogeneityis that the grey matter is slightly less rigid thanthe white matter. We therefore expect that themodel underestimates the extent of damage tothe border between grey matter and whitematter, where stresses are accentuated because
338 on A
ugust 3, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.62.4.334 on 1 April 1997. D
ownloaded from

Pathogenesis of cervical spondylotic myelopathy
of the inhomogeneity.2' The anisotropy of thespinal cord is not a major problem because itresults primarily from the craniocaudal orien-tation of the long white matter tracts. Mymodel, however, applies only to a single crosssection, in which, on a macroscopic level, thespinal cord is more nearly isotropic. Secondly,I have used equations for plane stress andstrain, which assume that adjacent segments ofthe spinal cord exert no shear stress on thesegment in question, but rather exert, at most,a uniform tension or compression. This islikely not to be the case. Further, I have mod-elled the cervical spinal cord cross section as acircle whereas it is more elliptical than circu-lar. Both of these simplifications mean that Icannot draw precise quantitative conclusionsfrom the data. However, I have not attemptedto do so. Rather, I have looked for qualitativepatterns and have shown a major differencebetween the predictions of the two hypotheses.There is no reason to think that this differencewould be significantly altered by these simpli-fying assumptions. Finally, I have assumedthat the spinal cord is an elastic structurewhereas it is viscoelastic26-that is, it is subjectto plastic deformation. In a condition ofchronic stresses such as CSM the viscousbehaviour is evidenced by the permanent flat-tening and widening of the spinal cord evenafter it is removed at necropsy and thus freedof stress. In such viscoelastic substances theimmediate response to stresses of modestdegree is elastic in nature, and viscous flowthen occurs to alleviate the stress if it persists.The viscous flow dampens the peaks of shearstress but does not alter its overall topographicpattern.25 Thus there is no reason to think thatthe viscous behaviour of the spinal cord wouldalter the substantial qualitative differencebetween the two mechanical theories.
THERAPEUTIC IMPLICATIONSIf the dentate tension hypothesis is correctthere are several implications with regard tothe treatment of CSM. As flexion increasestension in the dura, dentate ligaments, andspinal cord, CSM can be treated conservativelyby a restraining collar limiting mobility of thecervical spine. In particular, flexion of the cer-vical spine should be avoided. Improvementhas been reported in nearly half of patientstreated with a cervical collar.27-29
In patients not responsive to conservativetreatment removal of the spondylotic barthrough an anterior surgical approach may besuccessful by removing the source of posteriorpressure on the spinal cord and the source ofinterference with stretching of the dura duringflexion. Fixation of the vertebrae bordering thespondylotic bar with a bone graft may also helpby reducing spinal mobility. The surgery failsin about 25% of cases,29 possibly because post-operative adhesions between the anterior duraand the anterior wall of the spinal canal maycause increased tension in the dura duringneck flexion.22
Surgical laminectomy alone would seemunhelpful because the problem is not one ofcompression by the posterior elements of the
spine. Yet the reported benefits of laminec-tomy are not clearly worse than those of ante-rior surgery.29 30 There are several possibleexplanations for the beneficial effects oflaminectomy. Firstly, facetectomy is often per-formed with laminectomy and seems toimprove outcome." 32 Facetectomy releases thetethering of the dural sac by the dural rootsleeves in the foramina, removing the fixedpoint against which the dentate ligaments canbe stretched. It has also been suggested33 thatfacetectomy reduces the support of the poste-rior elements of the spine, thus tipping the ver-tebrae into extension, releasing tension in thedura and the dentate ligaments. However, sim-ilar benefit can result from extensive laminec-tomy without facetectomy.'4" After extensiveunroofing of the cervical spinal canal the poste-rior dura bulges dorsally into the site of decom-pression, and gas myelography shows that thecervical spinal cord has a milder lordotic curveand courses more posteriorly within the duralsac, no longer in contact with the spondyloticbar.2936 Because the anterior dura is anchoredto the anterior wall of the spinal canal, dorsalmigration of the posterior dura must beaccompanied by a decrease in the transversedimension of the dural sac if intradural volumeremains constant. This decrease in width willrelax the dentate ligaments. However, the pos-terior bulging of the dural tube may also reflectincreased filling with CSF." Even so, dorsalmigration of the posterior dura will displacethe dural attachments of the dentate ligamentssomewhat posteriorly. The posterior dura willhave a straighter course and may need todevelop less tension during neck flexion. Inaddition the extensive posterior scar that even-tually develops may serve to limit flexion of thecervical spine and thus any remaining stresseson the dura. Like the anterior approach, exten-sive laminectomy fails in a minority of cases,possibly because the posterior scar maytighten, compress the dura during neck flex-ion,'7 and increase the tension in the dentateligaments.
Although the most direct surgical approachto relieving excessive tension in the dentate lig-aments may be to open the dura and to sectionthe ligaments, intradural operations result inmore extensive adhesions, often involving thespinal cord itself.38 Several studies have failedto show an advantage to intradural section ofthe dentate ligaments,3" 3639 and the procedurehas largely been abandoned. It seems that it ispossible to relax the excessive tension in thedentate ligaments with either an anterior or aposterior approach that remains extradural.
I thank Dr Paul Cooper and Dr Al Goodgold for reading andcommenting on an earlier version of the manuscript.
1 Stookey B. Compression of the spinal cord due to ventralextradural cervical chondromas. Arch Neurol Psychiatry1928;20:275-9 1.
2 Stoltmann HF, Blackwood W. The role of the ligamentaflava in the pathogenesis of myelopathy in cervicalspondylosis. Brain 1964;87:45-50.
3 Taylor AR. The mechanism of injury to the spinal cord inthe neck without damage to the vertebral column. J BoneJoint Surg 1951;33B:543-7.
4 Breig A. Biomechanics of the central nervous system: some basicnormal andpathologic phenomena concerning spine, discs andcord. Chicago: Year Book Publishers, 1960:76-95.
339 on A
ugust 3, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.62.4.334 on 1 April 1997. D
ownloaded from

Levine
5 Kahn EA. The role of the dentate ligaments in spinal cordcompression and the syndrome of lateral sclerosis. JNeurosurg 1947;4: 191-9.
6 Greenfield JG. Lesions of the nervous system associatedwith diseases or malformations of the cranium and spinalcolumn. In: Blackwood W, McMenemey WH, Meyer A,Norman RM, Russell DS, eds. Greenfield's Neuro-pathology. London: Edward Arnold Ltd, 1971:656-61.
7 Mair WGP, Druckman R. The pathology of spinal cordlesions and their relation to the clinical features in protru-sion of cervical intervertebral discs. Brain 1953;76:70-91.
8 Taylor AR. Vascular factors in the myelopathy associatedwith cervical spondylosis. Neurology 1964;14:62-8.
9 Brain WR, Northfield DWC, Wilkinson M. The neurologi-cal manifestations of cervical spondylosis. Brain 1952;75:187-225.
10 Bedford PD, Bosanquet FD, Russell WR. Degeneration ofthe spinal cord associated with cervical spondylosis.Lancet 1952;ii:55-9.
11 Wilkinson M. The morbid anatomy of cervical spondylosisand myelopathy. Brain 1960;83:589-617.
12 Ono K, Ota H, Tada K, Yamamoto T. Cervical myelopathysecondary to multiple spondylotic protrusions: a clinico-pathologic study. Spine 1977;2: 109-25.
13 Ogino H, Tada K, Okada K, Yonenobu K, Yamamoto T,Ono K, Namiki H. Canal diameter, anteroposterior com-pression ratio, and spondylotic myelopathy of the cervicalspine. Spine 1983;8:1-15.
14 Grundfest H. Effects of hydrostatic pressure upon theexcitability, the recovery, and the potential sequence offrog nerve. Cold Spring Harbor symposia on quantitativebiology 1936;4: 179-87.
15 Holbourn AHS. Mechanics of head injuries. Lancet 1943;2:438-41.
16 Timoshenko S. Theory of elasticity. New York and London:McGraw-Hill Book Co, 1934:104-8.
17 Matlab: High performance numeric computation and visualiza-tion software. Natick, MA: The MathWorks Inc, 1993.
18 Stoltmann HF, Blackwood W. An anatomical study of therole of the dentate ligaments in the cervical spinal canal. J7Neurosurg 1966;24:43-6.
19 Reid JD. Effects of flexion-extension movements of thehead and spine upon the spinal cord and nerve roots. JNeurol Neurosurg Psychiatry 1960;23:214-21.
20 Cusick JF, Ackmann JJ, Larson SJ. Mechanical and physio-logical effects of dentatotomy. J Neurosurg 1977;46:767-75.
21 Tencer AF, Allen BL, Ferguson RL. A biomechanicalstudy of thoracolumbar spinal fractures with bone in thecanal: Part III, mechanical properties of the dura and itstethering ligaments. Spine 1985;10:741-7.
22 Adams CBT, Logue V. Studies in cervical spondyloticmyelopathy: I. Movement of the cervical roots, dura andcord, and their relation to the course of the extrathecalroots. Brain 1971;94:557-68.
23 Frykholm R. Defcrmities of dural pouches and strictures ofdural sheaths in the cervical region producing nerve rootcompression: a contribution to the etiology and operativetreatment of brachial neuralgia. J Neurosurg 1947;4:403-13.
24 Breig A, Turnbull I, Hassler 0. Effects of mechanicalstresses on the spinal cord in cervical spondylosis: a studyon fresh cadaver material. J7 Neurosurg 1966;25:45-56.
25 Holbourn AHS. The mechanics of trauma with special ref-erence to herniation of cerebral tissue. Jf Neurosurg 1944;1: 190-200.
26 Tunturi AR. Elasticity of the spinal cord, pia, and denticu-late ligament in the dog. J Neurosurg 1978;48:975-9.
27 Campbell AMG, Phillips DG. Cervical disc lesions withneurological disorder: differential diagnosis, treatment,and prognosis. BMg 1960;2:481-5.
28 Nurick S. Natural history and results of surgical treatment ofthe spinal cord disorder associated with cervical spondy-losis. Brain 1972;95:101-8.
29 Epstein JA, Epstein NE. The surgical management of cervi-cal spinal stenosis, spondylosis, and myeloradiculopathyby means of the posterior approach. In: The cervicalspine research society editorial committee, eds. The cervi-cal spine 2nd ed. Philadelphia: JB Lippincott Co, 1989:625-43.
30 Rowland LR. Surgical treatment of cervical spondyloticmyelopathy: time for a controlled trial. Neurology 1992;42:5-13.
31 Bishara SN. The posterior operation in treatment of cervicalspondylosis with myelopathy: a long-term follow-upstudy. Jf Neurol Neurosurg Psychiatry 1971 ;34:393-8.
32 Scoville WB, Dohrmann GJ, Corkill G. Late effects of cer-vical disc surgery. JNeurosurg 1976;45:203-10.
33 Breig A, El-Nadi AF. Biomechanics of the cervical spinalcord: relief of contact pressure on and overstretching of thespinal cord. Acta Radiologica-Diagnosis 1966;4:602-24.
34 Aboulker J, David M, Metzger J, et al. Myelopathieschroniques par stenose du trou occipital et du canal cervi-cal. Rev Neurol (Paris) 1964;111:197-208.
35 Alsharif H, Ezzat S, Hay A, Motty NA, Malek SA. Theresults of surgical treatment of spondylotic radiculo-myelopathy with complete cervical laminectomy andposterior foramen magnum decompression. ActaNeurochirurgica 1979;48:83-100.
36 Bakay L. Postoperative myelography in spondylotic cervicalmyelopathy. Acta Neurochirurgica 1973;28: 123-33.
37 Gonzalez-Feria L. The effect of surgical immobilizationafter laminectomy in the treatment of advanced cases ofcervical spondylotic myelopathy. Acta Neurochirurgica1975;31:185-93.
38 Oiwa T, Hirabayashi K, Uzawa M, Ohira T. Experimentalstudy on postlaminectomy deterioration of cervicalspondylotic myelopathy. Spine 1985;10:717-21.
39 Gorter K. Influence of laminectomy on the course of cervi-cal myelopathy. Acta Neurochirurgica 1976;33:265-81.
340 on A
ugust 3, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.62.4.334 on 1 April 1997. D
ownloaded from