-
Cardiovascular
Pathology
inflammatory
heart diseases
Semmelweis University
2nd Department of Pathology
_______ _______
2014/2015 Autumn Semester
Tibor Glasz MD PhD
_______ _______
-
Inflammatory cardiac diseases ____________________
_____________________
-
Inflammatory heart diseases
- Endocarditides - parietal
- valvular
- Myocarditis
- Pericarditis
Pancarditis
-
Endocarditides
-
The infective endocarditides
- Risk groupes: ~ rheumatic or degenerative valvular deformities
~ congenital valvular vitia
~ valvular prostheses
~ arterial long-term catheter
~ intravenous drug abusers (15% of cases,
here: localisation typically tricuspidal!)
- Infective agents: ~ almost always bacteria (Staphylococcus
auerus, Streptococcus viridans, Gonococci,
Enterobacteria; in immunodeficiency: so-called
opportunistic bacteria)
~ seldom fungi (in immunodeficiency /AIDS/ and
iv. drug abusers)
-
- Clinical forms:
~ acute: sudden beginning with high fever and septic crisis >
despite antibiotics mortality very
high
~ subacute (endocarditis subacuta infectiva/lenta):
begins inconspicuously with uncharacteristic
systemic symptoms (weakness, fever, weight loss)
The infective endocarditides
-
- Morphology: the same in both forms: ~ valvular vegetations
along the closing lines of the
valves: small, finely granular to gross polypoid, stenosing
~ the material of the vegetations may harbour large
amounts of infective agents and is highly friable >
danger
of embolism > formation of metastatic abscesses
~ valve destruction (endocarditis ulcerosa) through
necrosis, ulceration, thrombotic deposits > sacculation
(so-called valvular aneurysm) and rupture > sudden valve
insufficiency
~ extension of tissue destruction to neighbouring parts of
the aorta or myocardium > so-called paravalvular abscess,
paravalvular leak > cardiac/circulatory catastrophy!
~ in severe cases involvement of the cordae and parietal
endocardium is also possible
The infective endocarditides
-
Photoarchive of post-mortem documentation;
2nd Department of Pathology,
Semmelweis University
Destructive infective subacute endocarditis of the aortic valves
with
paravalvular abscess and septation within abscess. Risk factor
to this
had apparently been a degenerative calcifying valvular
deformity.
-
Photoarchive of post-mortem documentation;
2nd Department of Pathology,
Semmelweis University
Destructive infective subacute endocarditis of the aortic
valves
with paravalvular abscess. Risk factor to this had
apparently
been a degenerative calcifying valvular deformity.
-
Photoarchive of post-mortem documentation;
2nd Department of Pathology,
Semmelweis University
Ulcerative
endocarditis
(formerly known as
endocarditis
ulcerosa maligna)
with massive
vegetations,
complete tissue
demolition,
paravalvular leak
and involvement of
the parietal
endocardium. The
severe valvular
insufficiency
resulted in a
rounded dilatation
of the left ventricle.
-
Collection of the Museum of Pathology;
2nd Department of Pathology,
Semmelweis University
Ulcerative endocarditis of the aortic valves with massive valve
destruction,
valvular insufficiency and excentric myocardial hypertrophy
-
Photoarchive of post-mortem documentation;
2nd Department of Pathology,
Semmelweis University
Thrombopolypoid subacute endocarditis of the mitral valves
with antecedent degenerative calcification of the valve base
-
Photoarchive of post-mortem documentation;
2nd Department of Pathology,
Semmelweis University
Thrombopolypoid subacute endocarditis of the mitral valves
with antecedent degenerative calcification of the valve base
-
Ulcerative and perforating endocarditis of the mitral valves
Collection of the Museum of Pathology;
2nd Department of Pathology,
Semmelweis University
-
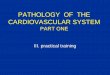
Thrombopolypoid
subacute
endocarditis of the
mitral valves. The
cordae are
severely
thickened,
referring to
recurrence of
valvular disease.
Photoarchive of post-mortem
documentation;
2nd Department of Pathology,
Semmelweis University
-
- Clinical presentation: ~ Schottmllers triad (endocarditis
ulcerosa;
splenic infarctions; embolic focal nephritis)
~ Oslers nodule: lividity, swelling and tenderness of the
periungual finger areas / distal phalanges through
(micro)emboli
~ sepsis
- Endocarditis of valvular prostheses: ~ vegetations along the
sutures of the prostheses:
paravalvular abscess and leak
The infective endocarditides
-
- Non-bacterial thrombotic endocarditis (formerly known as
Endo-carditis marantica)
~ sterile, small vegetations of fibrin and thrombocytes
in the closing line of valves
~ in the background there is often enhanced blood-
clotting in severely diseased patients with bad general
status (terminal tumour disease, chronic renal failure,
chronic sepsis)
- Liebman-Sacks endocarditis (SLE-endocarditis) ~ 1-4 mm large,
verrucous vegetations in the closing line
and on the undersurface of valves
~ fibrinoid necrosis, fibrosis, valvular deformity and
vitia are possible
~ histologically demonstration of so-called hematoxyphil-
bodies
Special forms of endocarditides /
non-infectious endocarditides
-
- Carcinoid-endocarditis ~ tumour site in the GI (appendix,
duodenum)
~ primarily alterations of the tricuspid valves
~ vitrous-firm thickening of the valve cusps
~ similar alterations of the pulmonary semilunar valves, the
endocardium of the right ventricle and in the pulmonary
trunk possible
~ cause: high blood titer of tumour products: Serotonin,
Kallikrein, Bradikinin, Histamine, Prostaglandins,
Tachikinins)
- Accompanying endocarditis ~ as with acute myocardial
infarction
~ typically a parietal localisation
Special forms of endocarditides /
non-infectious endocarditides
-
Vitrous-firm thickening of the tricuspid valves
with carcinoid-endocarditis
Photoarchive of post-mortem documentation;
2nd Department of Pathology,
Semmelweis University
-
Accompanying endocarditis with
chronic myocardial infarction
Photoarchive of post-mortem documentation;
2nd Department of Pathology,
Semmelweis University
-
- Endocarditis syphilitica/luetica ~ extension of a luetic
aortitis onto the aortic valves
~ valves thickened and firm, with insufficiency in the later
phase
- Endocarditis in rheumatoid arthritis (primary chronic
polyarthritis PCP)
~ alterations similar to those seen with luetic valvulitis
Special forms of endocarditides /
non-infectious endocarditides
-
Photoarchive of post-mortem documentation;
2nd Department of Pathology,
Semmelweis University
-
Myocarditides
-
Myocarditides
- Clinical presentation: ~ presentation with slight symptoms or
even without
any symptoms whatsoever possible
~ sometimes causes sudden progression into heart failure
or arrhythmias > sudden death syndrome
~ all age groups can be affected, most frequently in young
adults
- Classification: ~ referring to pathogenesis: infectious;
non-infectious;
idiopathic
-
Infectious myocarditides
- Viral myocarditides:
~ Coxsackie A, B; Influenza; Echovirus; EBV; HIV; CMV
- Bacterial myocarditides:
~ Diphteria; Leptospira; Meningococci; Borrelia (Lyme-
disease)
- Protozonal myocarditides:
~ Trypanosoma (Morbus Chagas); Toxoplasmosis
- So-called specific myocarditides:
~ rheumatic fever; tuberculosis; syphilis
-
Non-infectious myocarditides
- Physical myocarditides:
~ irradiation therapy (ionising radiations); electric shock
- Chemical myocarditides:
~ heavy metals; drugs (cytostatics, Sulfonamides,
Penicillin)
- Post-streptococcal myocarditides:
~ as a component of rheumatic fever
- Transplantational myocarditis:
~ during rejection reaction
-
Idiopathic myocarditides
- Giant cell myocarditis
- Fiedlers myocarditis
- Sarcoidosis
-
Morphology
- Macroscopy: ~ loose and flabby dilation of the ventricles
~ patchy cut surface of the myocardium with sporadic
small foci of hemorrhages
~ dilation of the atrioventricular ostia > relative
insufficiency of valves
- Microscopy: ~ important: the primarily diseased structure is
the
interstitium!
~ interstitial edema with lymphocytic, plasmacellular,
histiocytic, mastocytic infiltration
~ fibroblastic proliferation > interstitial fibrosis
~ cardiac muscle cell damaging (myocytolysis,
microinfarctions) are only secondary
-
http://images.md
Fatal myocarditis in a child
-
http://images.md
Interstitial lymphocytic infiltration
in viral myocarditis
-
Pericarditides
-
Acute pericarditides
- Fibrinous pericarditis (pericarditis sicca): ~ most frequent
form of pericarditis: macroscopically cor
villosum (hairy heart) on auscultation: friction noise in
rhythm of heart beatings
~ accompanying pericarditis with acute myocardial
infarction (so-called pericarditis epistenocardiaca)
~ viral pericarditides Coxsackie A, B; HSV; Influenza
(symptomatically leading sign is thoracal pain, so it is a
diagnostic problem to differentiate from an acute
myocardial infarction!)
~ uremia
~ rheumatic fever (pancarditis rheumatica)
~ autoimmune diseases (PCP, SLE)
~ iatrogeneous pericarditis (after pericardiotomy)
-
- Serous pericarditis: ~ an infrequent form: in polyserositis,
pericardial
carcinosis (pericarditis carcinomatosa)
- Purulent pericarditis: ~ bacterial or fungal infection
~ extension from neighbouring structures: pleural
empyema, lobar pneumonia, infectious endocarditis,
myocardial abscess
~ extension from distant infection through blood stream
(sepsis)
~ iatrogeneous: after cardiosurgery (rare)
~ severe form: pericardial sack is filled with pus
(empyema pericardii)
- Chylous pericarditis: ~ with metastatic tumour disease
Acute pericarditides
-
Fibrinous pericarditis
Photoarchive of post-mortem documentation;
2nd Department of Pathology,
Semmelweis University
-
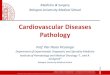
Subacute purulent
pericarditis: the
pericardial space
is filled with
massive
exsudation of
fibrinous-purulent
character. Partial
septation of the
pericardial mass is
already evident.
Photoarchive of post-mortem documentation;
2nd Department of Pathology,
Semmelweis University
-
Fibrinous pericarditis: aspect of the
so-called cor villosum (hairy heart)
Photoarchive of post-mortem documentation;
2nd Department of Pathology,
Semmelweis University
-
Chronic pericarditides
- Constrictive pericarditis (concretio pericardii): ~
organisation of unresolvable exsudates as result of an
acute pericarditis
~ stricture of the orifices of the large (primarily venous)
vascular trunks through pericardial scarring > severe
circulatory failure
- Adhesive mediastino-pericarditis (accretio pericardii): ~
adhesive fibrosis of the parietal myocardium to/with
mediastinal structures
- Posttuberculotic pericarditis: ~ organisation of massive
caseous exsudation
(pericarditis tuberculosa caseosa) with formation of a
partly calcified pericardial fibrosis (so-called Panzerherz)
-
Rheumatic fever _________ ___________
-
The rheumatic fever
- Definition: an acute, immunopathogenic, systemic,
non-purulent
inflammation, that represents disease of the complete
mesenchymal
system of the body and so, belongs to the so-called collagen
diseases.
- Pathogenesis: Cross reaction against own structures
(connective
tissue ground substance) a few weeks after pharyngitis caused
by
Sterptococcus -haemolyticus A
- Typical symptoms: (a) high fever
(b) carditis
(c) wandering polyarthritis
(polyarthritis rheumatica/migrans)
(d) subcutaneous rheumatic nodules
(e) erythema marginatum of the skin
(f) chorea minor
-
The rheumatic heart disease
- valvular endocarditis
- myocarditis
- pericarditis
rheumatic pancarditis
-
The rheumatic endocarditis
- acute phase: edema of the heart valves rich in
mucopolysaccha-
rides with friable, soft, wipable, reddish vegetations, 1-2 mm
large,
along the closing line of the valves, made of masses of
thrombocytes
complete regression growing of capillaries into the valve
tissue
- transition into a chronic rheumatic endocarditis:
- organisation of the vegetations
- scarring, gross calcification of valves
- deforming, conflusion of valvular commissures
- formation of rheumatic vitia
-
Thrombopolypoid acute
rheumatic vegetations on the
mitral valve cusps
Collection of the Museum of Pathology;
2nd Department of Pathology,
Semmelweis University
-
Thrombopolypoid acute
rheumatic vegetations on the
mitral valve cusps
Photoarchive of post-mortem documentation;
2nd Department of Pathology,
Semmelweis University
-
- Topography: Mitral valves 70-75% Mitral- and aortic valves
25%
Tricuspid- and pulmonary valves very rarely
- Pathophysiology: transition in a chronic rheumatic heart
disease lasts long (5-30) years
probability for a chronic heart disease after an
acute rheumatic fever is quite variale: 18-65%
rheumatic fever shows a tendency to recur: the
cardial alterations will be after each recurrence more
severe: endocarditis rheumatica recidivans/recurrens
cardiac valve anomalies (e.g. congenital
bicuspidy) enhance the risk for rheumatic valve disease
The rheumatic endocarditis
-
Congenital bicuspidy
http://images.md
-
The rheumatic myocarditis
- Pathologic forms: acute Aschoffs nodules chronic fibrosis
- Aschoffs nodules:
small perivascular foci of inflammation gathering of
lymphocytes, macrophages
and plasmacells
fibrinoid necrosis and degeneration of
collagen possible
+
Anitschkovs cells are histiocytes with
gathering of chromatin substance in the centre of
the nucleus: owls eye pattern
Aschoffs multinuclear giant cells result from
confluence of Anitschkovs histiocytes
-
Photoarchive of post-mortem documentation;
2nd Department of Pathology,
Semmelweis University
Macroscopic aspect of
rheumatic myocarditis with
nodular patchiness of the
cut surface and foci of
interstitial hemorrhages
-
http://images.md
-
Aschoffs nodules http://images.md
-
Anitschkovs histiocyte
Aschoffs giant cell
http://images.md
Anitschkovs histiocyte
-
http://www-medlib.med.utah.edu/WebPath
-
http://images.md
Anitschkovs histiocyte
-
The rheumatic fever - Rheumatic granulomes (Aschoffs
nodules):
- in the pericardium (pericarditis rheumatica)
- in joint capsules and periarticular soft tissues
(polyarthritis migrans) spontaneous regression
- Subcutaneous rheuma nodules:
multiple, 5-10 mm large nodules in the region of the
affected joints (e.g. around the olecranon, patella)
spontaneous regression
- Chorea minor: unvoluntary, jerky, excessive motion of the
extremities resulting from an encephalitis of the
extrapyramidal system, typically in childhood
and somewhat more frequently in girls spontaneous
regression
-
The clinical appearance of rheumatic nodules
http://images.md
-
http://images.md
The clinical appearance of rheumatic nodules
-
Chorea minor
http://images.md
Unvoluntary, jerky
movements of the
extremities
Hand writing of a patient
before... and after
spontaneous regression. (The actual status of the hand writing
is applicable
for monitoring the general state of the disease.)
-
the rheumatic heart alterations can have however dramatic
complications:
- Complications: acute congestive cardiac insufficiency >
death
valvular vegetations > systemic
embolisation
chronic valve vitia
further periods of infectious
endocarditides (acute recidivations)
The rheumatic fever
-
Vitia __ __
-
Vitium cordis
- Definition: morphologic and functional heart valve disease
- Forms: stenosis > < insufficiency
~ both forms result in a pathophysiologic overload
of the heart (stenosis pressure overload/hypertrophy;
insufficiency volume overload/hypertrophie)
~ until the heart is capable to balance pathologic
overload through use of its reserves, the vitium is
compensated
~ as soon as reserve capacities of the heart are
exhausted, the vitium will be decompensated
~ in stenosis dominates a muscular hypertrophy
~ in insufficiency dominates a ventricular dilatation
-
Mitral valve vitia
- Insufficiency:
~ left ventricle and atrium are dilated and slightly
hypertrophic
~ pulmonary congestion results later in a excentric
right heart hypertrophy/failure
- Stenosis:
~ the left ventricle is underloaded, so slightly atrophic
~ the left atrium is on the contrary distinctly dilated
and hypertrophic
~ in severe cases of mitral stenosis results the
pathomorphology of a fishmouth stenosis (german:
Knopflochstenose buttonhole stenosis )
-
Fishmouth stenosis of the
mitral valves with severe
atrial dilatation
Collection of the Museum of Pathology;
2nd Department of Pathology,
Semmelweis University
-
Aortic valve vitia
- Insufficiency:
~ excentric left ventricular hypertrophie
- Stenosis:
~ primarily concentric hypertrophy of the left
ventricle, which turns excentric as decompensation
supervenes
~ backward pulmonary congestion and right heart
failure develops only later
~ a similar situation is seen in hypertonic heart
disease
-
Degenerative valvular base calcification and combined
aortic valve vitium (stenosis + insufficiency)
Collection of the Museum of Pathology;
2nd Department of Pathology,
Semmelweis University
-
Most severe degenerative
aortic vitium (stenosis)
with a residual lumen of a
few millimeters of the
original aortic transsection
surface
Collection of the Museum of Pathology;
2nd Department of Pathology,
Semmelweis University
-
Collection of the Museum of Pathology;
2nd Department of Pathology,
Semmelweis University
Most severe degenerative
aortic vitium (stenosis)
with a residual lumen of a
few millimeters of the
original aortic transsection
surface
-
Infrequent form of a valve vitium: valvula fenestrata. The
hemodynamic effect of this
alteration is shown by the left ventricular hypertrophie.
Collection of the Museum of Pathology;
2nd Department of Pathology,
Semmelweis University
-
Acute valvular insufficiency (vitium cordis) in infective
endocarditis
Photoarchive of post-mortem documentation;
2nd Department of Pathology,
Semmelweis University
-
Complications of the vitia
- Cor pulmonale chronicum
~ secondary overload on the right ventricle resulting from
backward congestion from the diseased left heart: right
ventricular dilatation and severe muscular hypertrophy
- Relative valvular insufficiency ~ severe ventricular
dilatation is followed by expansion of
the atrioventricular orifice, so the valve cusps are no more
capable of covering the enlarged lumen surface
- Ball thrombus
~ spherical, free-floating or to the wall loosely adherent
thrombus in the dilated atrium or auricula
- Induratio brunea pulmonum (brown induration of the lungs) ~ in
chronic left heart failure develops long-term
congestion and relative hypoxia of lung tissue
~ heart failure cells and interstitial fibrosis
-
Valvular surgery in case of vitia: implantation of valvular
prostheses
Collection of the Museum of Pathology;
2nd Department of Pathology,
Semmelweis University
-
Collection of the Museum of Pathology;
2nd Department of Pathology,
Semmelweis University
Valvular surgery in case of vitia: implantation of valvular
prostheses
-
Semmelweis University
2nd Department of Pathology
_______ _______
2014/2015 Autumn Semester
Tibor Glasz MD PhD
_______ _______
Cardiovascular
Pathology
- further aspects -
-
Cardiomyopathies ____________ ____________
-
Cardiomyopathies
Definitions:
- primary (idiopathic) cardiomyopathies: progressive myocardial
diseases
of unknown origin that after variously long periods lead to a
therapy
resistant circulatory insufficiency.
- secondary cardiomyopathies: progressive, diffuse myocardial
diseases, that may be identical to the idiopathic forms in their
clinical and pathologi-
cal presentation, yet can be derived from a detectable
origin.
Therapy is possible only by heart transplantation.
-
Primary (idiopathic) cardiomyopathies
The following 3 groups are defined according to basic
clinico-pathological
differences:
(a) dilatative (congestive) cardiomyopathy
(b) hypertrophic (obstructive) cardiomyopathy
(c) restrictive (obliterative) cardiomyopathy
-
Dilatative/congestive cardiomyopathy (DCM) - Morphology -
- morphologic criteria: severely enlarged heart (weight
sometimes 3 times
the normal cor bovinum) with extremely dilated, ball-shaped
ventricles,
rounded apex, from basis to apex progressively thinning wall and
parietal
thrombi.
- further macroscopic alterations: atrial thrombosis; myocardium
loose, patchy-fibrotic, pale; valves secondarily and relatively
insufficient.
Coronary arteries and valves morphologically intact!
- microscopy: no diagnostic alterations, only signes of a
muscular hypertrophy (enlarged muscle fibers and nuclei) and
secondary signes of a
relative coronary insufficiency (myocytolysis,
microinfarctions-microscars,
interstitial fibrosis, single fiber necroses)
-
Postmortem Photo Archive of the 2nd Dept. of Pathology;
Semmelweis University
Dilatative
cardiomyopathy.
Note the rounded
ventricle with
local endocardial
thickenings
representing
organized
remnants of
former parietal
thromboses.
-
- presentation in all age-groups, yet, most frequently in the
young
- appearance sporadic, only seldom familiar (here genetic
background possible),
sometimes molecular biologic traces of enteroviral genom
detectable (viral
myocarditis in the anamnesis?)
- the clinical picture is that of a slowly developping, therapy
resistant circulatory
insufficiency
- begins slowly, lingering over the years with atypical
complaints, the diagnosis is
established generally in the stage of the circulatory
insufficiency
- the end-diastolic volume increases progressively, the ejection
fraction decreases
- leads in 5-10 years to death
Dilatative/congestive cardiomyopathy (DCM) - Clinical aspects
-
-
- cardiac muscle contractility is secured by the strength of the
sarcomeric
contraction as well as by its transmission from sarcomer to
sarcolemma and further
to the extracellular matrix
- the connection between sarcomer and sarcolemma is given by the
dystrophin-
sarcoglycane proteincomplex
- certain mutations of the dystrophin gene (on the X-chromosome)
lead to selective
absence of the dystrophin in the myocardium (>>DCM) but
not in the skeletal
musculature (e.g. no Duchenne-Beckers muscle dystrophy)
- mutation of the -sarcoglycane gene >> DCM
- mutation of the distal part of the myocardium-specific actin
(contacting part
between actin and dystrophin with the help of a protein named
desmin) and
mutations of desmin >> DCM
- further mutations of e.g. binding structures between
neighbouring muscle cells, or
that of the energy production can lead to DCM
Dilatative/congestive cardiomyopathy (DCM) - Molecular
characteristics -
-
Hypertrophic/obstructive cardiomyopathy (HCM) - Morphology -
- macroscopically: severely enlarged heart (weight sometimes
1000g cor
bovinum) with a disproportionate left heart hypertrophy
especially at the
septum >> decreased ability to dilatation (compliance) and
stenosis of the
way leading out from the ventricle with cardiac insufficiency
>> hence
synonym terms: asymmetrical septal hypertrophy (ASH);
idiopathic
hypertrophic subaortic stenosis (IHSS)
- microscopically: a diagnostic picture: (a) extreme hypertrophy
of the
muscle fibers; (b) enlarged, bizarr nuclei with pale perinuclear
rim (halo);
(c) very typically irregular-chaotic, syntitially woven fiber
connections:
beside normal end-to-end connections there are end-to-side and
side-to-side
fiber connections. This chaotic micromorphology explaines the
clinicallly
often experienced cardiac arrhythmias.
-
- ethiology and pathogenesis unknown, the genetic background
is
however proven (HCM is an inherited disease)
- clinical symptomes appear only around the 30th year of
life
- first angina and dyspnoe on body excersize
- conduction abnormalities are often seen (arrhythmias)
- sudden cardiac death is possible
- with the disease at end stage, there is a therapy resistant
cardiac
insufficiency
Hypertrophic/obstructive cardiomyopathy (HCM) - Clinical aspects
-
-
- generally it is a familiar disease with autosomal dominant
inheritence and varying penetrance
- rarely sporadic appearance through de novo mutations is
possible
- HCM is a disease of the sarcomer: as well the thick (myosin)
as the
thin (actin, tropomyosin, etc.) filament genes may be
affected
Hypertrophic/obstructive cardiomyopathy (HCM) - Molecular
characteristics -
-
Restrictive/obliterative cardiomyopathy (RCM) - General comments
-
- a rare disease
- important is the restricted ability of the heart ventricle to
dilate (reduced
diastolic filling)
- the ventricle is capable neither of contracting nor of
expanding to the
desirable degree
- the combined systolic and diastolic derangement leads to
cardiac insuffi-
ciency
- the disease is generally detected very late, in the stage of
cardiac insuffi-
ciency
- according to classic understanding basis of the disease lies
in the parietal
endocardium, namely (a) an endocarditis parietalis fibroplastica
secundum
Loeffler; or (b) an endomyocardial fibrosis
-
- in the background there is a severe peripheral and
interstitial
eosinophilia (sometimes even an eosinophilic leukemia)
- it is a lethal disease
- the atypical, degranulated, circulating eosinophils cause
endo-
myocardial necrosis by their toxic substances >>
thickening and
scarring of the endocardium and the subendocardium >>
formation
of parietal thrombi >> organisation of thrombi >>
the very rigid
endocardium leads to myocardial motility derangements
Restrictive/obliterative cardiomyopathy (RCM) - Endocarditis
parietalis fibroplastica secundum Loeffler -
-
- endocardial changes as with Loefflers endocarditis, yet
without an
eosinophylia
- it is most frequently seen in the first 2 years of life, in
adults rare
- the proliferating connective tissue that thickens the
parietal
endocardium infiltrates also into the subendocardial
myocardium
- prognosis depends on dimensions of the disease: focal
endocardial
thickenings can remain symptomless, whereas a diffuse disease
leads
quickly to cardial decompensation and death
Restrictive/obliterative cardiomyopathy (RCM) - Endomyocardial
fibrosis -
-
Museum of Pathology;
2nd Dept. of Pathology; Semmelweis University
Restrictive
cardiomyopathy
of a new-born.
Note thickened
left-ventricular
endocardium.
-
Secondary cardiomyopathies
- diffuse myocardial diseases of known origin >>
important, that with the therapy
of the causative circumstances also the cardiac status gets
relief or will even be
cured
- (a) alcoholic cardiomyopathy the most frequent cause, that
leads to a dilatative
cardiac disease. No coronary sclerosis. First symptoms are
arrhythmias without
congestive signes. Beside a normal coronarogram angina pectoris
is possible. At
the beginning the developping heart insufficiency can be
reversed by alcohol
abstinence and specific supportive cardiotherapy. With continued
alcohol abuse an
irreversible circulatory decompensation will follow. Cause of
death is often
embolisation from parietal thrombi.
- (b) peripartal (pregnancy-linked) cardiomyopathy in the 3rd
trimester of
pregnancy or within 6 weeks after birth. Disease characteristics
as with a
dilatative cardiomyopathy. Specific therapy makes a complete
recovery possible.
-
- (c) Hemochromatosis genetic derangement of iron uptake and
-stockage. Iron
reserves appear pathologically also in parenchymal cells causing
functional
alterations in many organs: liver, pancreas, heart, skin, etc.
The clinical
appearance of the heart disease that of a DCM. Later the
myocardium develops
progressiv rigidity through accumulating iron contents, so the
clinical picture turns
into one resembling a RCM. Macroscopically the myocardium is
stiffened, dark
coloured. Microscopically the muscle fibers are massively
overloaded with iron
containing hemosiderin pigment (positive Prussian-blue
reaction).
- (d) Amyloidosis the amyloid protein is deposited in the
myocardial interstitium
and in small vessels >> thickening of myocardium all over
the heart (especially in
the left ventricle). A cardiac insufficiency with lung edema and
systolic functional
decrease develops typically in an unexpected, abrupt manner.
Myocardium stif-
fened and rigid with a waxy-glassy hue on the cut surface
>> the clinical presen-
tation is that of a RCM. Microscopically amyloid is seen as a
homogenous eosino-
phylic material (congo red staining positive).
Secondary cardiomyopathies
-
- (e) Sarcoidosis in 8% of patients with sarcoidosis also
cardiac disease
develops. Sarcoidotic granulomas appear in the pericardium
and
myocardium (most frequently in the upper third of the
interventricular
septum and in the papillary muscles). The clinical picture is
dominated by
arrhythmias. The overall picture as with RCM. Arrhythmias may
lead to
sudden cardiac death.
Secondary cardiomyopathies
-
Cardiac decompensation _________________ _________________
-
Cardiac decompensation - General comments -
- it is the end stage of severe heart diseases; prognosis
bad
- the clinical progression is defined by the basic disease, age,
overall status and
other factors (e.g. social status of the patient)
- acute cardiac decompensation: as with myocardial infarction,
valve rupture in
destructive endocarditis
- chronic cardiac decompensation: as with non-treated
hypertension, chronic
valvular endocarditis, cardiomyopathies
- pump failure (forward failure) disturbance of
contractility
- filling failure (backward failure) disturbance of
dilatation
- at the beginning cardiac decompensations are generally one
sided: either left-
or right heart failure, which can later combine
-
- causes are:
- ischemic heart disease
- hypertension
- vitia (other than a mitral stenosis)
- diseases of the myocardium (cardiomyopathies)
- backward failure: congestion of the lungs with chronic
pulmonary edema, heart
failure cells, brown stiffening of the lungs (induratio brunea
pulmonum)
- clinically: dyspnoe; orthopnoe; nocturnal respiratory
complaints; frequent and
blood-stained coughs; hydrothorax with compression and
atelectasis of the lungs
(atelectasia e compressione); cerebral hypoxia with sleepiness
(stupor) and rarely
hypoxic encephalopathy up to coma; decreased renal filtration,
salt and water
retention, peripheral edemas
Cardiac decompensation - Left heart failure -
-
- most frequently in combination with a left heart failure
congestive
cardiac decompensation
- isolated right heart failure develops in only 15% of the
cases, especially
with
- mitral stenosis
- some congenital vitia
- cor pulmonale
- pulmonary fibrosis
- clinically: congestion of the superficial jugular veins; lower
limb edema
(anasarca); sometimes hydrothorax; hypoxic encephalopathy as
with left
heart failure; liver congestion with development of a severe
nutmeg liver
and a so-called cardiac cirrhosis; hepato-splenomegaly;
congestive
gastroenteritis; ascites
Cardiac decompensation - Right heart failure -
-
Museum of Pathology;
2nd Dept. of Pathology; Semmelweis University
Cardiac decompensation. Cavities of both sides are tremendously
dilated.
-
Tumors of the heart _____________ _____________
-
Primary cardiac tumors
- Benign
- Myxoma 25%
- Lipoma 8%
- Papillary fibroelastoma 8%
- Rhabdomyoma 7%
- Mesothelioma of the AV-Nodule 2%
- Malignant
- Angiosarcom a 7%
- Rhabdomyosarcoma 5%
- Mesothelioma 4%
- Fibrosarcoma 3%
-
Secondary cardiac tumors
- in 5% of all malignancy-related death cases cardiac metastases
can
be found
- primary tumor locations in order of frequency are
- pulmonary carcinoma
- mammary carcinoma
- renal cell carcinoma
- malignant melanoma
- lymphoma / leukemia
-
Myxoma - most frequent tumor of the heart
- originates from the parietal endocardium
- macroscopy: a soft, greyish-reddish, sessile or steeled,
varyingly large tumor
- microscopy: very loose, myxoid stroma with disseminated small
vessels, on the surface a
covering layer endothelium
- danger of complication in approx. 50% of the cases is systemic
embolisation from
fragmented tumor particles
- the lesion can unequivocally be detected radiologically
- therapy: operative resection; healing rate high; recurrences
infrequent
- familiar appearance as a so-called Carney-syndrome possible:
multiple cardiac myxomas,
sometimes extracardiac (e.g. cutaneous) myxomas, patchy dermal
pigmentation, endocrine
hyperfunction >> in case of a myxoma, echocardiography of
closer relatives is indicated
- differential diagnosis against an organized parietal thrombus
is both macro- and micro-
scopically often probematic
-
Papillary fibroelastoma
- it is probably a residuum of an organized thrombus
- a bunch-like formation at the semilunar and cuspidal valves
with hairy, repeatedly
bifurcating, thin branches and endothelial lining on the
surface, usually measuring cca. 1cm
- most frequent localisation: aortic valves >> danger of
complication: stenosis or occlusion
of the coronary ostia with angina pectoris or even sudden
cardiac death
Rhabdomyoma
- most frequent in new-borns and small children
- possible presentation with tuberous sclerosis
- no real tumor, but a hamartoma*
- in the left ventricular myocardium multiple nodules, sometimes
with elevation of the
endocardial inner surface
*Hamartoma a tumor-like lesion with tissue components, that are
also present under normal conditions of the
presenting localisation, the morphologic composition and
percentage relations of which being however abnormal.
-
Mesothelioma of the AV-nodule
- a typically cystic tumor in the location of the AV-nodule
measuring
from microscopically small up to even 3 cm
- the tumor is connatal, that develops during the embryonal
period,
primarily in females
- danger of complication: recurrent fits of Adams-Stokes
syndrome
already in childhood; complete AV-blockage; sudden cardiac death
of
unknown origin in a young person >> often makes the
implan-tation
of a pacemaker inevitable
-
Aneurysms Vessel dissections _____________________
_____________________
-
Aneurysms
Definitions:
- aneurysm: a circumscribed lumen dilatation that exceeds
generally 150% of the
original lumen.
- ectasy: diffuse dilatation of a vessel.
- causes:
- degeneration of mural structures by atherosclerosis
(atheroma)
- infection of vascular wall structures (aneurysma
mycoticum/infectivum)
- aneurysm formation in tertiary syphilis ascending aorta
- constitutional weekness of the vascular wall (so-called
berry-aneurysms)
- trauma
-
Aneurysms - Localisations -
-
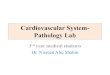
Aneurysms
A1 = fusiform; A2 =saccular, A3 = berry-aneurysm,
B = pseudoaneurysm (indeed: a perivascular hematoma),
C = dissecting aneurysm (indeed: dissection of the vessel wall
layers)
Real an
eury
sms
An
eury
sm m
imics
-
Aneurysms
- morphology
- aneurysma verum (real aneurysm) vascular wall structures
are detectable in the aneurysmal wall. Forms: (a) fusiform
and
(b) saccular (special form: berry-aneurysm of cranial
arteries)
- aneurysma spurium (fake aneurysm) e.g. posttraumatically,
after catheterization. The perivascular hematoma looks from
the
outside as if it was a real aneurysm.
- complications:
- rupture (the larger the aneurysm, the higher the risk)
- usuration (pressure-linked atrophy or erosion) of
neighbouring
body parts (e.g. vertebrae)
- thrombosis
- embolisation
-
Museum of Pathology;
2nd Dept. of Pathology; Semmelweis University
Berry-aneurysm of the left internal carotid artery
just before its joining the cranial basal vessels
-
Museum of Pathology;
2nd Dept. of Pathology; Semmelweis University
Saccular aneurysm of
the aortic arch
-
Museum of Pathology;
2nd Dept. of Pathology; Semmelweis University
Fusiform aneurysm of the
descending thoracic aorta
-
Museum of Pathology;
2nd Dept. of Pathology; Semmelweis University Huge chronic
aneurysm of the
postero-apical two-third of the left
ventricular wall
-
Museum of Pathology;
2nd Dept. of Pathology; Semmelweis University
Chronic aneurysm of the postero-lateral
left ventricular wall with thrombosis
-
Dissection
- definition: a longitudinally expanding detachment of vascular
wall layers
resulting in the formation of a secondary (false) lumen that
runs parallel to
the original one.
- pathogenesis: wall layers detachment is possible through -
constitutional weekness (Marfans syndrome: weekness of the
elastic fibers and deposition of mucoid substances: cystic
medial
degeneration of Erdheim-Gsell)
- atherosclerosis (atheromatous intimal plaques with intimal
rupture
and distally from here detachment of the degenerated wall
layers
under the pulsating blood stream. A second, more distal
intimal
tear may lead to reunification of the two blood ways, or else,
an
adventitial tear to perivascular hemorrhage.)
- hypertension
-
- complications:
- infarction of the supplied organ
- rupture with hematoma of the neighbouring regions
(retroperito-
neal hematoma; hemascos; hematopleura; hemopericardium)
>>
exsanguination
- clinical apperance of the aortic dissection:
- typical age: 40-60th years of life. With Marfans syndrome yet
in
youth possible.
- on palpation: a pulsating abdominal mass
- complaint: sudden, anihilating, knife-stabbing-like
thoracal/abdo-
minal pain >> sometimes followed by an acute abdomen
syndrome
- the more dangerous type of the aortal dissections is the
proximal
form (Typ A, or DeBakey I. and II.)
- somewhat less dangerous is the distal type (Typ B./DeBakey
III.)
- early diagnosis may offer the chance of a successful
operative
intervention (vascular prosthesis)
Dissection
-
Photomicrograph by Glasz, T;
Semmelweis University, 2nd. Dept. of Pathology Dissection of the
arterial wall layers
-
Vasculitides ________ ________
-
Vasculitides of the large vessels
- Giant cell arteritis (temporal arteritis)
- over the 50th year of life; generally in females; affected are
the aorta, its large branches, the extracranial branches of the
carotid
artery (like the temporal artery)
- cause unknown (immunpathogenesis against wall structures
is
possible)
- morphology: a segmental granulomatous panarteritis with
giant
cells and elastic fiber fragmentation; later mural fibrosis
- clinically painful thickening of the vessels; pain in the
facial and
mandibular region; fever; weekness; muscular pain in the
neck
and the shoulders; on involvement of the ophtalmic artery
visual
complaints or even blindness may occur
-
- Takayashu-Arteritis - in females under 40 years;
- affected are the aorta and its elastic large branches: the
classical
topography is the aortic arch
- morphology: histologically an initial sign is the inflammation
of
the vasa vasorum; followed by a non-segmental, granulomatous
panarteritis with giant cells upon long segments of the
affected
vessel; later mural fibrosis; wall thickening at the
branchings-off of
the side vessels of the aortic arch causing vascular stenosis
and
weekness of the pulse in the arm (pulseless disease)
- clinically in the early stage general chronic inflammatory
symp-
tomes (fever, weekness, weight loss); in later stage symptomes
of
the vessel stenoses (ophtalmologic, neurologic alterations)
Vasculitides of the large vessels
-
- Polyarteritis nodosa - affected are the visceral main vessels
and their primary side branches
(the mesenteric, lienal, renal, hepatic, coronary, etc.
arteries)
- all organs may be affected (other than the lungs)
- alterations of varying ages appear synchronously in several
arteries: a
segmental, nodular, necrotizing panarteritis
- initially fibrinoid necrosis of wall structures, later
fibrosis; the necrotic
damaged segments dilate aneurysmatically: macroscopically a
pearl chain-
like aspect; later vascular thrombosis
- peak of prevalence in young adults
- clinically fever, abdominal and muscular pains (often with
melena); later
occlusive symptomes: infarctions of various organs (a very
colourful
clinical picture) >> on affection of the kidneys:
hypertension
- immunsuppressive therapy (corticosteroids) gives remission up
to 90%
of the cases
Vasculitides of the middle sized vessels
-
- Kawasaki-Arteritis - develops in children younger than 5 years
of age in the asiatic continent
- affected are the visceral, most frequently the coronary
arteries: a seg-
mental, necrotizing panarteritis >> myocardial
infarction
- exact cause unknown (suspected is an immunpathogenesis with
malfunc-
tion of T-cells and macrophages)
- in case cutaneous purpures, mucosal inflammations, enlargement
of
lymphatic nodules also occur: muco-cutaneous lymphnode
syndrome
- Morbus Buerger (thrombangitis obliterans) - affects severely
smoking males under 40 years in the small to middle
sized muscular arteries of the (primarily lower) extremities
- smoking plays a probable role: hypersensitivity against
tobacco
- a segmental panarteritis with thrombosis; later intimal
fibrosis, organiza-
tion of thrombi, recanalisation
- pain in resting position refers to affection of the
neighbouring nerves
- smoking abstinence brings spectacular amelioration
Vasculitides of the middle sized vessels
-
- Schnlein-Henochs Purpure - IgA-deposition in small vessels
- begins with infection of the upper respiratory tract around
the 5th year of life
- clinically: fever, joint pains, cutaneous purpures, melena,
hematuria, IgA-nephro-
pathy
- generally a spontanous healing follows
- Wegeners Granulomatosis - necrotizing, granulomatous
inflammation of the upper & lower respiratory organs
- furthermore, all over the body, focal, necrotizing
vasculitides of small vessels +
glomerulonephritis possible
- begins around the 40th year of age; without therapy leads to
death within a year
- clinically: two-sided, necrotizing pneumonitis; chronic
sinusitis; nasopharyngeal
ulcerations; renal damage
- immunsuppressors may successfully be applied
- Churg-Strau Syndrom - eosinophylic, granulomatous, respiratory
inflammation with necrotizing small
vessel vasculitis + asthma bronchiale
Vasculitides of the small vessels
-
Pathology of the veins _______________ _______________
-
Demonstration of the venous valves and their function (XVII.
century)
-
Varicosity - dilation of the veins in the lower extremities
- insufficiency of venous valves >> chronic venous
insufficiency
- primary varices (hormonal, working, etc. conditions)
- secondary varices (e.g. after thrombosis of the lower limb
veins)
- phlebosclerosis (by recurring phlebitides, drog abusers)
Thrombosis of the deep veins - lower limb veins,
periprostatic-periuteral plexus
- clinically: swelling, pains
- collaps of the nearby capillaries: paleness of the limb
(phlegmasia alba dolens)
- affection of the collateral veins: decrease of venous drainage
of the whole limb
(phlegmasia coerulea dolens)
- consequencies: propagation; rethrombosis; thrombembolism;
organisation of
thrombi, postthrombotic syndrome, ulcus cruris venosum
-
Postmortem Photo Archive of the 2nd Dept. of Pathology;
Semmelweis University Thrombosis of the
periprostatic venous plexus
-
Postmortem Photo Archive of the 2nd Dept. of Pathology;
Semmelweis University
Thrombosis of the
periprostatic venous plexus
-
Museum of Pathology;
2nd Dept. of Pathology; Semmelweis University
Pylethrombosis: blood clotting
in the portal vein
-
Museum of Pathology;
2nd Dept. of Pathology; Semmelweis University
Paradox embolism: an embolus just in the phase of transition
from the
right to the left circulation through the opening of a patent
foramen ovale
-
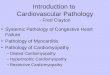
Museum of Pathology;
2nd Dept. of Pathology; Semmelweis University
Esophageal varices.
Note rough inner surface over
meandering submucosal veins
with a mucosal rupture.
-
Museum of Pathology;
2nd Dept. of Pathology; Semmelweis University
Esophageal varices
on cut surface