Embed Size (px)
Citation preview

e121
Volume 41, Number 3, 2021
Submitted June 25, 2020; accepted July 30, 2020. ©2021 by Quintessence Publishing Co Inc.
The posterior maxilla has traditionally presented a challenge for successful placement of dental implants due to a combination of poor bone quality, ridge atrophy, and pneumatization of the sinus floor following tooth extraction. However, with the successful and predictable surgical outcomes reported in the literature, more clinicians and patients are choosing an implant-supported restoration in the edentulous posterior maxilla. Consequently, sinus elevation and augmentation have gained more popularity. Extensive research has been conducted on types of bone graft materials and implants, less-invasive techniques to perform sinus augmentation, and timing for implant placement for sinus grafting. Despite the predictability of the techniques and biomaterials employed in sinus grafting procedures, intra- and postoperative complications are common. Much of the current literature discusses the local risk factors related to sinus augmentation, with few studies focusing on the patient-related risk factors. The purpose of this review is to identify, evaluate, and discuss the possible management of patient-related risk factors to allow for more predictable maxillary sinus floor augmentation outcomes. Int J Periodontics Restorative Dent 2021;41:e121–e128. doi: 10.11607/prd.5265
Patient-Related Risk Factors for Maxillary Sinus Augmentation Procedures: A Systematic Literature Review
1 Ashman Department of Periodontology and Implant Dentistry, New York University College of Dentistry, New York, New York, USA.
2 Ashman Department of Periodontology and Implant Dentistry, New York University College of Dentistry, New York, New York, USA; Private Practice, New York, New York, USA.
3 Ashman Department of Periodontology and Implant Dentistry, New York University College of Dentistry, New York, New York, USA; Implant Dentistry Research & Education Foundation (International Congress of Oral Implantologists) Scientific Advisory Board, New York, New York, USA.
Correspondence to: Dr Stuart J. Froum, 17 W. 54th Street, Suite 1C/D, New York, NY 10019, USA. Fax: 212-246-7599. Email: [email protected]
The posterior maxilla has tradi-tionally presented a challenge for successful placement of dental implants. This is due to a combi-nation of poor bone quality, ridge atrophy, and pneumatization of the sinus floor following tooth ex-traction. With the successful and predictable surgical outcomes re-ported in the literature, more clini-cians and patients are choosing an implant-supported restoration in the edentulous posterior maxilla.1,2 Consequently, sinus elevation and augmentation have gained more popularity. The conventional sinus augmentation approach includes preparation of a lateral wall window through which the sinus membrane is carefully elevated, then the cre-ated space is filled with a bone graft or bone substitute material. Implant placement can then be performed with a delayed or simultaneous pro-tocol.3,4
In 1996, the Sinus Consensus Conference concluded that sinus augmentation should be consid-ered a highly predictable and ef-fective therapeutic modality.5 Ex-tensive research has since been conducted on types of bone graft materials and implants, less invasive techniques to perform sinus aug-mentation, and timing for implant placement for sinus graft. Implant survival rates have been reported to range from 81% to 95%, depending
Martin Leung, BDS1
Reem Alghamdi, DDS1
Inés Fernandez Guallart, DDS1
Marco Bergamini, DDS1/Paul Y. C. Yu, DDS1
Stuart J. Froum, DDS2/Sang-Choon Cho, DDS3
© 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER. © 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

The International Journal of Periodontics & Restorative Dentistry
e122
on the combination of graft materi-als and implant surfaces.6 The Sinus Consensus Conference was revis-ited in 2016 and reaffirmed the va-lidity of the sinus graft. It concluded that noninductive materials with slow resorption might be superior than inductive materials in forming and maintaining bone.7
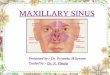
Despite the predictability of the techniques and biomaterials em-ployed in sinus graft procedures, intra- and postoperative compli-cations are common, like sinusitis, rhinosinusitis, fistulae, migration of the implant into the maxillary sinus, infection, sinus membrane perfora-tion, excessive bleeding, and perfo-rations in the buccal flap (Figs 1 and 2).8,9 Much of the current literature discusses the local risk factors relat-ed to sinus augmentation, with few studies focusing on patient-related risk factors.10
The purpose of this review is to identify, evaluate, and discuss the possible management of patient-re-lated risk factors that can contribute to intra- and extraoperative compli-cations, allowing for more predict-able maxillary sinus floor augmenta-tion outcomes.
Material and Methods
The patient-related risk factors evaluated in this study include the following: cardiovascular disease and anticoagulant drugs; diabetes; osteoporosis and antiresorptive drugs; organ transplant and immu-nosuppressive therapy; cigarette smoking/vaping; antibiotic allergy; thickened sinus membrane; age; and gender.
An electronic search was per-formed in Medline (PubMed) for articles published from 1993 to 2020. The search was limited to the English language. Terms included were “maxillary sinus augmenta-tion” combined with each of the following terms: “cardiovascular disease,” “anticoagulants,” “diabe-tes,” “osteoporosis,” “antiresorptive drugs,” “organ transplant,” “immu-nosuppression,” “smoking,” “vap-ing,” “antibiotic allergy,” “Schneide-rian membrane,” “flap attachment,” “gender,” and “age.” To be included in the study, publications needed to be either human or relevant animal studies, reviews (including system-atic reviews and meta-analyses), clinical studies with at least a 2-year
follow-up, clinical trials, controlled clinical studies, comparative studies, and congress/consensus reports. In vitro and preclinical studies, reports based on questionnaires, studies not meeting the inclusion criteria, studies not available in English, and studies published before 1993 were excluded. The keyword search re-vealed 799 articles. Of these, 52 articles were selected that best de-scribed patient-related risk factors.
Results
Cardiovascular Disease and Anticoagulant Drugs
Cardiovascular disease combined with anticoagulation drug therapy is a risk factor for sinus augmenta-tion procedures due to the patient’s increased risk of bleeding. With an aging population and high inci-dence of cardiovascular diseases in developed societies, there is an increased prevalence of patients taking some form of anticoagulant therapy.11 The main objective of this therapy is to reduce the occurrence of thromboembolism.11 The medications
Fig 1 Clinical view of a perforated sinus membrane.
Fig 2 Clinical view of (a) an infection following a maxillary sinus augmentation procedure and (b) a Penrose drain used to manage the infection.
a b
© 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER. © 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

e123
Volume 41, Number 3, 2021
are divided into two predominant groups: anticoagulants and anti-platelet drugs.
Anticoagulant medications work by interfering with specific clotting factors on the pathway of hemostasis. Although warfarin is the gold standard for anticoagu-lant therapy and is still widely pre-scribed, direct-acting anticoagu-lants (DOAGs) such as dabigatran (Pradaxa), rivaroxaban (Xarelto), and apixaban (Eliquis) are preferred due to the equal or superior efficacy and an improved safety profile.12,13 However, DOAGs lack standardized laboratory monitoring, such as inter-national normalized ratio (INR), and lack anticoagulation reversal agents except for dabigatran. Prothrom-bin time and thrombin time blood tests are ineffective for DOAGs as they can only be used as qualitative tests to confirm if there is an antico-agulant effect.12 Furthermore, it has been established that anticoagula-tion therapy is a risk factor for major oral surgery procedures. According to Scully et al,14 a procedure is con-sidered to be major oral surgery if it involves harvesting of autogenous bone grafts, the raising of extensive flaps, or placing an implant in sites where there is a risk of extending outside the bony envelope during osteotomy preparation. As such, an-ticoagulant medication is a risk fac-tor for maxillary sinus augmentation.
Antiplatelet medications such as aspirin and clopidogrel (Plavix) are commonly prescribed to prevent thrombosis in patients with isch-emic heart disease or a history of coronary angina, myocardial infarc-tion, or stent implantation.15 Careful
consideration must be given to the management of these medications before commencing sinus augmen-tation.15 The risk of a patient with coronary heart disease developing an ischemic stroke must be weighed against the risk of postoperative bleeding in such patients. Studies have shown no relevant increase in the rate of postoperative bleeding for implant placement procedures in patients continuing antiplatelet medication.16–18 However, withdraw-al of such medications seriously in-creases the risk of adverse cardiac and brain ischemic events.19,20 As maxillary sinus augmentation is more complex in nature than den-tal implant placement, consultation with the patient’s cardiovascular physician is necessary to properly manage the antiplatelet regime prior to sinus augmentation surgery. Furthermore, platelet aggregation and bleeding time typically do not return to baseline levels until 10 days after sinus augmentation and/or implant placement and cannot be measured with a diagnostic pa-rameter such as INR, as they do not inhibit the coagulation pathway.
For patients taking anticoagu-lant and antiplatelet medications, medical clearance from the treat-ing physician outlining the need for a “drug vacation” is essential prior to treatment, in conjunction with the availability of coagulation laboratory tests such as INR if ap-plicable. INR values should be ob-tained within 24 hours before the dental procedure.11 Values of 2.0 to 3.5 are usually considered appropri-ate for surgical clearance for sinus augmentation. However, medical
clearance is still the deciding factor. One method of determining the risk of a patient taking an anticoagulant during a sinus augmentation proce-dure is to perform, when necessary, a smaller surgical procedure; if this is not needed, thorough scaling and root planing can be done to assess the bleeding tendency prior to sinus augmentation surgery.
Diabetes Mellitus
Diabetes mellitus is a relative risk factor for maxillary sinus augmen-tation procedures. Uncontrolled diabetes has been associated with an increased susceptibility to infec-tion because of a compromised host response contributing to post-operative infection, a decrease in graft turnover, and creating inci-sions in the line opening.21 Mareno Varquez et al22 found that 30 out of 147 diabetic patients developed postoperative complications with sinus augmentation procedures. Another study found that diabetes demonstrated a four-fold increase in risk of postoperative swelling us-ing a transcrestal sinus approach.23 This was further influenced by the antibiotic regimen, whereby amoxi-cillin reduced the probability of inci-dence by 60%.23 In the same study, looking at lateral window sinus aug-mentation, diabetes was observed as a factor in developing postop-erative swelling, mild postoperative bleeding, delayed wound healing, membrane exposure, and flap de-hiscence.23
On the molecular level, the mechanism by which this may occur
© 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER. © 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

The International Journal of Periodontics & Restorative Dentistry
e124
has been described in the literature as physiologic alteration induced by a hyperglycemic state (uncontrolled diabetes). Such events have been implicated in causing modifications in (1) the function of neutrophils, monocytes, and macrophages, (2) connective tissue metabolism, (3) normal osseous healing, (4) the formation of advanced glycation end products, and (5) the produc-tion of proinflammatory cytokines such as IL-1ß and TNF-α.23
To manage diabetic patients, sinus augmentation surgery should be scheduled after proper medical clearance and acceptable glycemic control.21 The measure for glycemic control is an HbA1c less than 7%.
Osteoporosis and Antiresorptive Drugs
The condition of osteoporosis alone is not an absolute risk factor for si-nus augmentation procedures. It has been observed that fractures in patients with osteoporosis heal similarly to healthy patients. The as-sumption that a decrease in bone mineral density and altered bone mineral metabolism affects sinus healing and implant osseointegra-tion is controversial due to the lack of quality studies available.24
However, antiresorptive drugs (ARDs) are often prescribed for os-teoporotic patients. These medica-tions alter bone metabolism and as such are a relative risk factor for sinus augmentation procedures. Furthermore, they are used in the management of skeletal metastases of malignancies, to prevent events
like fractures, and to limit pain and metastatic spread. Use of ARDs has traditionally been divided accord-ing to the route of administration (ie, oral, subcutaneous, intravenous). The current understanding, how-ever, is that dose is more impor-tant than route of administration.25 Thus, low- and high-dose ARDs can be administered today through all three routes. Primarily, a low dose is used for osteoporosis treatment, whereas a high dose is used in can-cer patients with bone metastases. Patients on ARD have a risk of de-veloping medication-related osteo-necrosis of the jaw (MRONJ), a spe-cific complication directly related to these types of drugs that can have devastating consequences for the individual patient.25 Despite this theoretical risk, clinical studies have demonstrated contrary results. In a study that evaluated sinus augmen-tation with guided bone regenera-tion in patients on bisphosphonates, 47 mandibular bone blocks were grafted using the split bone block technique and 14 maxillary sinus augmentations were implemented. A total of 71 implants were placed and restored after 4 months. Of the 47 grafted bone sites, 45 healed without complication with success-ful integration of all implants.26
Nonetheless, individual patient assessment is important and must be carried out before a sinus aug-mentation procedure. For example, the risk of MRONJ increases with dose and duration of ARD intake.26 The benefits of the “drug holiday” concept in implant therapy are un-clear.26 A drug holiday should be only considered after consultation
with the treating physician. Sinus augmentation procedures are cur-rently not recommended in patients on high-dose ARD intake.26 Prophy-lactic use of antibiotics and postop-erative antiseptics (eg, chlorhexi-dine) are recommended when sinus augmentation procedures are per-formed in patients with low-dose ARD intake.26
A suggested method to assess the risk of MRONJ is to measure the C-terminal telopeptide of col-lagen (CTX) as described by Marx et al.27 CTX is a metabolic product from normal bone turnover and can be measured in the blood. As bone turnover is decreased with anti-resorptive agents, the CTX value will also decrease, indicating a high risk for MRONJ.28,29 However, meta-analyses have not indicated CTX as a valid predictive value for risk of MRONJ due to a lack of evidence from multiple studies.30
As such, for this group of pa-tients, a medical consultation with the treating physician and medical clearance is essential prior to con-ducting sinus augmentation proce-dures.
Organ Transplant and Immunosuppressive Therapy
Traditionally, patients with immuno-compromised conditions are often contraindicated for sinus augmen-tation because of the risk of infec-tion, impaired wound healing, and altered bone metabolism.31 The medications used to treat these patients have evolved over time to reduce comorbidity. A case report
© 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER. © 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

e125
Volume 41, Number 3, 2021
describing ridge augmentation and extended bilateral sinus eleva-tion procedures in a liver-transplant patient with a 28-month follow-up suggests that the class of immu-nosuppressant therapy may make a difference.32 By using tacrolimus combined with mycophenolate mofetil instead of cyclosporin A with prednisone, the patient did not show any clinical or radiologic signs of preoperative bone impairment.33 Furthermore, this drug protocol may reduce complications, includ-ing renal toxicity and those related to bone metabolism.32
In managing patients on im-munosuppressive therapy, a medi-cal consultation with the treating physician and medical clearance are essential prior to conducting sinus augmentation procedures.
Cigarette Smoking/Vaping
Cigarette smoking has been estab-lished as a risk factor for complica-tions of sinus augmentation surgery. The negative influence of smoking has been attributed to decreased tissue oxygenation capacity, altera-tions in microcirculation, effects on fibroblasts and connective tissue, and effects on chemotaxis and ad-herence in leukocyte phagocyto-sis.34–37
Complications rates have been found to increase in situations where guided bone regeneration is performed simultaneously with sinus augmentation.38 However, few studies evaluated complication rates with sinus augmentation pro-cedures alone. Cigarette smoking
has been widely associated with an impact on host response by de-creasing neutrophil and phagocyto-sis functions.39 Moreover, the risk of subgingival infection in individuals with a current smoking habit is 2.3× greater than in nonsmokers or indi-viduals with a past history of smok-ing.40 Smoking was also associated with a higher membrane exposure rate, flap dehiscence, and excessive pain in guided bone regeneration procedures.34 Further studies are required to confirm the detrimen-tal effect of smoking on incidence of sinus membrane perforation and bleeding during sinus elevation pro-cedures.41
There are no clinical studies as-sessing the effect of electronic ciga-rette smoking on periodontal and peri-implant bone and soft tissues. From the experimental evidence currently available, it seems that electronic cigarette smoking may negatively influence the outcome of dental implant therapy in a manner similar to conventional smoking by enhancing oxidative stress in peri-odontal and peri-implant tissues and augmenting alveolar bone loss. Thus, well-designed clinical studies are needed in this regard.42
Antibiotic Allergy
Amoxicillin allergy has been sug-gested as a contraindication for sinus augmentation procedures. When a patient demonstrated an allergy to amoxicillin, traditionally clindamycin was prescribed as the alternative. However, a recent study showed that sinus augmentation
failure occurred in patients who received prophylactic clindamycin therapy.43 In the retrospective ob-servational study, 1,874 patients received sinus augmentations prior to dental implant placement, and 9 patients developed infection of the sinus graft material. A common trait observed with these 9 patients was a reported penicillin allergy, and all had been prescribed clindamycin.
The primary alternative antibiot-ic recommendation has changed for patients with a true penicillin allergy. It is recommended that azithromycin be given with a loading dose of 500 mg, then 250 mg for an additional 4 days.44 The U.S. Food and Drug Ad-ministration recently placed a black box warning on clindamycin for risk of Clostridium difficile infection. Therefore, clindamycin should only be prescribed if the patient cannot take penicillin or azithromycin.
Sinus Membrane Thickness
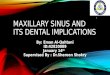
The thickening of the sinus mem-brane as identified on radiographs is commonly associated with sinus-itis (Fig 3). Mild mucosal thickening is often asymptomatic and considered a normal radiographic finding. How-ever, mucosal thickening > 2 mm is indicative of sinusitis.45 Patients requiring implant placement with sinus augmentation often present with a thickened membrane. Stud-ies have found a mucosal thickening of > 2 mm in 62.6% of patients pre-senting for implant placement in the posterior maxilla.46
If the sinus membrane is too thick, it can block the osteomeatal
© 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER. © 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

The International Journal of Periodontics & Restorative Dentistry
e126
process when elevated (Fig 3). The patency of the osteomeatal com-plex is essential for overall sinus health. Any blockage of the com-plex can lead to major complica-tions, such rhinosinusitis.47 Studies have shown a significantly greater risk for obstruction of the osteome-atal process where mucosal thicken-ing is > 5 mm.48,49
Gender/Age
Although gender and age cannot be considered risk factors for sinus augmentation procedures, their relationship with sinus membrane thickness has been investigated. The thicker membrane will allow for greater ease in membrane elevation from the sinus cortical floor and less risk of membrane perforation. In a study by Zimmo et al,50 age was found to be a factor influencing membrane thickness, with younger patients exhibiting thicker mem-branes. Two studies46,51 demon-strated that gender influenced the
dimension of the sinus membrane, with females having healthier mem-branes. This was refuted in a study by Lim et al,52 which found that si-nus membrane thickness was not in-fluenced by age or gender. Further studies are required to confirm the validity of these trends.
Discussion
Having cardiovascular disease and taking anticoagulants, uncontrolled diabetes, antiresorptive drugs, im-munosuppressive therapy, amoxi-cillin allergy, and cigarette smoking have been identified as patient- related risk factors for sinus aug-mentation procedures.
Where the patient has a pre-existing condition (such as cardio-vascular disease and diabetes mel-litus) or has had an organ transplant, management of these patients re-quires a consultation with the treat-ing physician and medical clearance prior to commencing sinus augmen-tation procedures. Cigarette smok-ing is an established risk factor for sinus augmentation procedures and should be ceased by the patient pri-or to treatment. Where the patient has an amoxicillin allergy, azithromy-cin is considered the alternative an-tibiotic of choice.44 Trends between gender/age and sinus membrane thickness have been studied, but they are not considered to be es-tablished risk factors for sinus aug-mentation procedures. A thickened sinus membrane of > 5 mm is a risk factor, as it can block the osteome-atal process when elevated, causing major complications.
Despite the current under-standing of patient-related risk factors, there are a low number of clinical studies relating to sinus aug-mentation procedures alone. These studies often focus on establishing risk for implant therapy or bone augmentation procedures. Further studies are required to evaluate patient-related risk factors for sinus augmentation procedures.
Conclusions
Predictable outcomes in maxillary sinus augmentation procedures not only require consideration of local factors but also on identifica-tion, evaluation, and management (where possible) of patient-related risk factors. Based on a systematic review of the literature, established patient-related risk factors include cardiovascular disease, diabetes mellitus, immunosuppression from organ transplantation, cigarette smoking, amoxycillin allergy, and a thickened sinus membrane. Due to the low number of clinical studies, further research is required to evalu-ate patient-related risk factors for si-nus augmentation procedures.
Acknowledgments
The authors report no conflicts of interest re-lated to this study.
Fig 3 CBCT scan of a thickened sinus membrane leading to blockage of the osteomeatal process.
© 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER. © 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

e127
Volume 41, Number 3, 2021
References
1. Fugazzotto PA, Vlassis J. Report of 1633 implants in 814 augmented sinus areas in function for up to 180 months. Im-plant Dent 2007;16:369–378.
2. Fugazzotto PA. Success and failure rates of 1,344 6- to 9-mm-length rough-surface implants placed at the time of transalveolar sinus elevations, restored with single crowns, and followed for 60 to 229 months in function. Int J Oral Maxillofac Implants 2017;32:1359–1363.
3. Boyne PJ, James RA. Grafting of the maxillary sinus floor with autog-enous marrow and bone. J Oral Surg 1980;38:613–616.
4. Wallace SS, Tarnow DP, Froum SJ, et al. Maxillary sinus elevation by lateral win-dow approach: Evolution of technology and technique. J Evid Based Dent Pract 2012;12(suppl 3):161–171.
5. Jensen OT, Shulman LB, Block MS, Iacono VJ. Report of the Sinus Consen-sus Conference of 1996. Int J Oral Maxil-lofac Implants 1998;13:11–45.
6. Pjetursson BE, Tan WC, Zwahlen M, Lang NP. A systematic review of the suc-cess of sinus floor elevation and survival of implants inserted in combination with sinus floor elevation: Part I: Lateral ap-proach. J Clin Periodontol 2008;35:216–240.
7. Aludden HC, Mordenfeld A, Hallman M, Dahlin C, Jensen T. Lateral ridge augmentation with Bio-Oss alone or Bio-Oss mixed with particulate autog-enous bone graft: A systematic review. Int J Oral Maxillofac Surg 2017;46:1030–1038.
8. Schwartz-Arad D, Herzberg R, Dolev E. The prevalence of surgical complica-tions of the sinus graft procedure and their impact on implant survival. J Peri-odontol 2004;75:511–516.
9. Wallace SW, Testori T. Complications in lateral window sinus elevation sur-gery. In: Froum SJ (ed). Dental Implant Complications: Etiology, Prevention, and Treatment, ed 2. Wiley Blackwell, 2016:396–426.
10. Testori T, Weinstein T, Taschieri S, Wallace SS. Risk factors in lateral win-dow sinus elevation surgery. Periodon-tol 2000 2019;81:91–123.
11. Madrid C, Sanz M. What influence do anticoagulants have on oral implant therapy? A systematic review. Clin Oral Implants Res 2009;20(suppl 4)96–106.
12. Conway SE, Hwang AY, Ponte CD, Gums JG. Laboratory and clinical monitor-ing of direct acting oral anticoagulants: What clinicians need to know. Pharma-cotherapy 2017;37:236–248.
13. Witt DM, Clark NP, Kaatz S, Schnurr T, Ansell JE. Guidance for the practical management of warfarin in the treat-ment of venous thromboembolism. J Thromb Thrombolysis 2016;41:187–205.
14. Scully C, Hobkirk J, Dios PD. Dental endosseous implants in the medically compromised patient. J Oral Rehabil 2007;34:590–599.
15. Eikelboom JW, Hirsh J, Spencer FA, Baglin TP, Weitz JI. Antiplatelet drugs antithrombotic therapy and preven-tion of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2012;141(suppl):e89s–e119s.
16. Tabrizi R, Khaheshi I, Hoseinzadeh A, Rezvanpour B, Shafie S. Do antiplatelet drugs increase the risk of bleeding after dental implant surgery? A case-and-crossover study. J Oral Maxillofac Surg 2018;76:2092–2096.
17. Bajkin BV, Urosevic IM, Stankov KM, Petrovic BB, Bajkin IA. Dental extrac-tions and risk of bleeding in patients taking single and dual antiplatelet treatment. Br J Oral Maxillofac Surg 2015;53:39–43.
18. Akhlaghi F, Khaheshi I, Amirhassani S, Tabrizi R. Do antiplatelet drugs increase the risk of bleeding after tooth extrac-tion? A case-crossover study. Int J Oral Maxillofac Surg 2017;46:1475–1478.
19. Biondi-Zoccai GG, Lotrionte M, Agostoni P, et al. A systematic review and meta-analysis on the hazards of discontinuing or not adhering to aspirin among 50,279 patients at risk for coronary artery dis-ease. Eur Heart J 2006;27:2667–2674.
20. Maulaz AB, Bezerra DC, Michel P, Bogousslavsky J. Effect of discontinuing aspirin therapy on the risk of brain isch-emic stroke. Arch Neurol 2005;62:1217–1220.
21. Fiorellini JP, Nevins ML. Dental implant considerations in the diabetic patient. Periodontol 2000 2000;23:73–77.
22. Mareno Varquez JC, Gonzalez de Rivera AS, Gil HS, Mifsut RS. Compli-cation rate in 200 consecutive sinus lift procedures: Guidelines for prevention and treatment. J Oral Maxillofac Surg 2014;72:892–901.
23. Askar H, Di Gianfilippo R, Ravida A, Tattan M, Majzoub J, Wang HL. Inci-dence and severity of postoperative complications following oral, periodon-tal, and implant surgeries: A retrospec-tive study. J Periodontol 2019;90:1270–1278.
24. Dao TT, Anderson JD, Zarb GA. Is os-teoporosis a risk factor for osseointegra-tion of dental implants? Int J Oral Maxil-lofac Implants 1993;8:137–144.
25. Schliephake H, Sicilia A, Nawas BA, et al. Drugs and diseases: Summary and con-sensus statements of group 1. The 5th EAO Consensus Conference 2018. Clin Oral Implants Res 2018;29:93–99.
26. Khoury F, Hidajat H. Extensive autog-enous bone augmentation and implan-tation in patients under bisphosphonate treatment: A 15-case series. Int J Peri-odontics Restorative Dent 2016;36:9–18.
27. Marx RE, Cillo JE Jr, Ulloa JJ. Oral bisphosphonate-induced osteonecro-sis: Risk factors, prediction of risk us-ing serum CTX testing, prevention, and treatment. J Oral Maxillofac Surg 2007;65:2397–2410.
28. Shin EY, Kwon YH, Herr Y, Shin SI, Chung JH. Implant failure associated with oral bisphosphonate-related osteonecro-sis of the jaw. J Periodontal Implant Sci 2010;40:90–95.
29. Gross HB. Bisphosphonate-induced osteonecrosis: Dental considerations. Compend Contin Educ Dent 2008;2:112–113.
30. Flichy-Fernández AJ, Alegre-Domingo T, González-Lemonnier S, et al. Study of serum CTX in 50 oral surgical patients treated with oral bisphosphonates. Med Oral Patol Oral Cir Bucal 2012;17:e367–e370.
31. Katranji A, Fotek P, Wang HL. Sinus aug-mentation complications: Etiology and treatment. Implant Dent 2008;17:339–349.
32. Dalla Torre D, Burtscher D. Ridge augmentation in an organ transplant patient. Int J Oral Maxillofac Surg 2016;45:658–661.
33. Haywood S, Abecassis M, Levitsky J. The renal benefit of mycophenolate mofetil after liver transplantation. Clin Transplant 2011;25:e88–e95.
34. Barone A, Santini S, Sbordone L, Crespi R, Covani U. A clinical study of the out-comes and complications associated with maxillary sinus augmentation. Int J Oral Maxillofac Implants 2006;21:81–85.
35. Levin L, Herzberg R, Dolev E, Schwartz-Arad D. Smoking and complications of onlay bone grafts and sinus lift op-erations. Int J Oral Maxillofac Implants 2004;19:369–373.
© 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER. © 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

The International Journal of Periodontics & Restorative Dentistry
e128
36. Sarine CL, Austin JC, Nickel WO. Effects of smoking on digital blood flow veloc-ity. JAMA 1974;229:1327–1328.
37. MacFarlane GD, Herzberg MC, Wolff LF. Refractory periodontitis associated with abnormal polymorphonuclear leuko-cyte phagocytosis and cigarette smok-ing. J Periodontol 1992;63:908.
38. Sakkas A, Schramm A, Winter K, Wilde F. Risk factors for post-operative com-plications after procedures for autolo-gous bone augmentation from different donor sites. J Craniomaxillofac Surg 2018;46:312–322.
39. Zambon JJ, Grossi SG, Machtei EE, Ho AW, Dunford R, Genco RJ. Ciga-rette smoking increases the risk for subgingival infection with periodontal pathogens. J Periodontol 1996;67(suppl 10):1050–1054.
40. Askar H, Gianfilippo R, Ravida A, Tattan M, Majzoub J, Wang HL. Incidence and severity of postoperative complications following oral, periodontal, and implant surgeries: A retrospective study. J Peri-odontol 2019;90:1270–1278.
41. Ghasemi S, Fotouhi A, Moslemi N, Chinipardaz Z, Kolahi J, Paknejad M. Intra- and postoperative complications of lateral maxillary sinus augmentation in smokers vs nonsmokers: A system-atic review and meta-analysis. Int J Oral Maxillofac Implants 2017;32:759–767.
42. Javed F, Rahman I, Romanos GE. To-bacco-product usage as a risk factor for dental implants. Periodontol 2000 2019;81:48–56.
43. Khoury F, Javed F, Romanos GE. Sinus augmentation failure and postoperative infections associated with prophylactic clindamycin therapy: An observational case series. Int J Oral Maxillofac Im-plants 2018;33:1136–1139.
44. Lockhart PB, Tampi MP, Abt E, et al. Ev-idence-based clinical practice guideline on antibiotic use for the urgent manage-ment of pulpal- and periapical-related dental pain and intraoral swelling. A report from the American Dental Asso-ciation. J Am Dent Assoc 2019;150:906–921.e12.
45. Vallo J, Suominen-Taipale L, Huumonen S, Soikkonen K, Norblad A. Prevalence of mucosal abnormalities of the maxil-lary sinus and their relationship to den-tal disease in panoramic radiography: Results from the Health 2000 Health Examination Survey. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;109:e80–e87.
46. Janner SF, Caversaccio MD, Dubach P, Sendi P, Buser D, Bornstein MM. Characteristics and dimensions of the Schneiderian membrane: A radio-graphic analysis using cone beam com-puted tomography in patients referred for dental implant surgery in the pos-terior maxilla. Clin Oral Implants Res 2011;22:1446–1453.
47. Chandra RK, Pearlman A, Conley DB, Kern RC, Chang D. Significance of os-teomeatal complex obstruction. J Oto-laryngol Head Neck Surg 2010;39:171–174.
48. Carmeli G, Artzi Z, Kozlovsky A, Segev Y, Landsberg R. Antral computerized to-mography pre-operative evaluation: Re-lationship between mucosal thickening and maxillary sinus function. Clin Oral Implants Res 2011;22:78–82.
49. Shanbhag S, Karnik P, Shirke P, Shanbhag V. Cone-beam computed tomographic analysis of sinus membrane thickness, ostium patency, and residual ridge heights in the posterior maxilla: Implica-tions for sinus floor elevation. Clin Oral Implants Res 2014;25:755–760.
50. Zimmo N, Insua A, Sinjab K, Chan HL, Shaikh L, Wang HL. Impact of sex, age, and season on sinus membrane thick-ness. Int J Oral Maxillofac Implants 2018;33:175–180.
51. Schneider AC, Bragger U, Sendi P, Caversaccio MD, Buser D, Bornstein MM. Characteristics and dimensions of the sinus membrane in patients referred for single-implant treatment in the pos-terior maxilla: A cone beam computed tomographic analysis. Int J Oral Maxil-lofac Implants 2013;28:587–596.
52. Lim HC, Nam JY, Cha JK, et al. Retro-spective analysis of sinus membrane thickening: Profile, causal factors, and its influence on complications. Implant Dent 2017;26:868–874.
© 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER. © 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.