Embed Size (px)
Citation preview

291
The patient safety movement was galvanized by the Institute of Medicine (IOM) re-port, To Err Is Human: Building a Safer Health System (Kohn, Corrigan, & Donaldson,2000).This report fundamentally changed how providers, policy makers, and the pub-lic view healthcare safety and focused national attention on the mistakes and errorsoccurring in a deficient system that permits 44,000 to 98,000 needless patient deathseach year due to medical error (Kohn et al., 2000). Although certainly one of the mosthighly recognized initiatives, the IOM report was not the first attempt to addresshealthcare safety concerns. White (2004) noted that the earliest safety and quality ef-forts can be traced to 1955, although this work was not specific to patient safety ini-tiatives but rather to patient outcomes, complications, and strategies for establishingmeasures to monitor outcomes.
Approximately 40 years later, in the mid-1990s, interest in medical errors and pa-tient safety peaked with the convening of the first Annenberg Conference on PatientSafety, the establishment of the National Patient Safety Foundation (NPSF), andPresident Clinton’s formation of the Advisory Commission on Consumer Protectionand Quality in the Health Care Industry. In 1996, the Joint Commission launchedits Sentinel Event Policy for the voluntary reporting of sentinel events. By 2000, con-tinued momentum in the patient safety and quality movement led the Agency forHealth Care Policy and Research (AHCPR) to change its name to the Agency for Healthcare Research and Quality (AHRQ) and become a funding powerhousefor research focused on patient safety, error reduction, strategic planning specific topatient safety, and technology utilization in the interest of enhancing quality of care(White, 2004).
Patient Safety: PreventingUnintended Consequences
and Reducing ErrorsPatti Rager Zuzelo, EdD, RN, MSN, ACNS-BC*
C H A P T E R N I N E
* Dr. Zuzelo would like to acknowledge the contributions of JoAnne Phillips, MSN, RN,CCRN, CCNS. Her first edition chapter, The Patient Safety CNS: A New Role for anEstablished Systems Expert, is incorporated into this revised chapter.
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 291
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

Within this same period of time, the Business Roundtable established the LeapfrogGroup, an organization with the mission of triggering “giant leaps forward in thesafety, quality, and affordability of health care by supporting informed healthcare de-cisions by those who use and pay for health care; and promoting high-value healthcare through incentives and rewards (Leapfrog Group, 2007).
CNSs have been involved in workplace safety initiatives throughout this trajectoryand are uniquely positioned to serve as patient safety experts across a variety of care set-tings. As patient safety is indistinguishable from quality care (Aspden, Corrigan, Wol-cott, & Erickson, 2004), the CNS’s goal of delivering quality patient care is in concertwith, and contributes to, creating and sustaining an environment of safety.This chapterintroduces CNSs to current patient safety perspectives and opportunities while sharingsuggestions for Web sites, tools, and resources that may be used to create and sustain aculture of safety through the integration of evidence-based practice with patient safetypractices, as defined by the Agency for Health Research and Quality (AHRQ) (2001).
Human Error and Types of ErrorMost practicing nurses are well aware of the high rates of errors and near misses thatoccur on a daily basis across the healthcare system.The number of actual errors and pre-vented errors is staggering. Appreciating the various types of errors and their triggersmay assist CNSs in planning and implementing targeted strategies that minimize errorlikelihood and improve patient outcomes. Reason’s work (1990) on human error pro-vides interesting theoretical and practice perspectives on basic error mechanisms, typesand consequences of errors, and techniques for assessing and reducing the risks of errors.
Human error theory (HET) (Reason, 1990) suggests that organization failures incomplex systems cause accidents. Reason (1990) asserts that the term error denotes anintentional act. Other error types depend upon two kinds of failure—slips and lapses—and mistakes. Errors may be active or latent. Latent errors lie dormant for a long periodof time until they align with enough other factors to breech the system’s defenses.
The alignment of latent failures and a variety of triggering events is referred to asthe dynamics of accident causation, or the Swiss cheese model of accident causation(Figure 9-1).The figure illustrates a trajectory of accident opportunity that penetratesseveral defensive systems and is the result of complex interactions between latent fail-ures and triggering events. In this model, latent failures at the managerial levels com-bine with psychological precursors, and unsafe acts within a context of local triggeringevents lead to an accident opportunity. When these factors and influences align, acci-dents are more likely to occur, characterized by the holes of a Swiss cheese wedgealigning to allow for unimpeded passage through the cheese wedge. A few examplesof organizational failures include lack of administrative commitment to safety, blurredsafety responsibilities, and poor training (Wolf, 2007).
Reason (1990) points out that very few unsafe acts actually result in damage or in-jury, even in systems that are unprotected. Findings from a focus group study explor-ing the influence of technologies on registered nurses’ work illustrate the many waysthat nurses work around and bypass technology-related rules and routines in efforts
292 Chapter 9 Patient Safety: Preventing Unintended Consequences and Reducing Errors
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 292
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

to meet patient care needs, save time, or minimize frustrations. Rarely do these sys-tem breeches lead to patient harm (Zuzelo, Gettis, Hansall, & Thomas, 2008). How-ever, when mistakes do occur, they may be catastrophic.
Reason (1990) pessimistically observes that while engineered safety devices offerbarriers against most single errors, human and mechanical, there are no guaranteedtechnological defenses against the accumulation of latent failures that provide oppor-tunities for errors within organizations, including high-risk healthcare systems (seeExemplar 9-1). Reducing the likelihood of errors by minimizing latent failures, scru-tinizing and improving systems, and rapidly evaluating the effectiveness of processchanges are requisite activities to promote safety and certainly fall within the purviewof CNS practice.
Accident causation theory is very relevant to CNS practice and is applicable to largehealthcare organizations as well as to specific types of clinical care areas. As an exam-ple, critical care poses great risk for patients related to (1) increased patient acuity,(2) high frequency of invasive interventions, (3) high medication volume, (4) need for
Human Error and Types of Error 293
Local triggersIntrinsic defectsAtypical conditions
Latent failures at themanagerial levels
Trajectory of accidentopportunity
Defense-in-depthPsychologicalPrecursors
UnsafeActs
Figure 9-1 The dynamics of accident causation.The diagram shows a trajectory of acci-dent opportunity penetrating several defensive sysems. This results from a complex inter-action between latent failures and a variety of local triggering events. It is clear from thisfigure, however, that the chances of such a trajectory of opportunity finding loopholes in allof the defenses at any one time is very small.Source: James Reason (1990). Human error. © Cambridge University Press, 1990. Reprinted with permis-sion of Cambridge Univerity Press.
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 293
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

speedy decision-making processes and associated intervention, and (5) other factors,including patient characteristics. In one study, researchers found that critical care pa-tients experienced 1.7 errors per day, 29% with the potential to cause significant harmor death (Pronovost, Thompson, Holzmueller, Lubomski, & Morlock, 2005). Acrossthe United States, that data extrapolates to 85,000 errors every day, of which 24,650are potentially life threatening. Nursing homes and ambulatory care settings are alsonot immune from error. In fact, because the number of outpatient visits each year far
294 Chapter 9 Patient Safety: Preventing Unintended Consequences and Reducing Errors
Exemplar 9-1
The Unsafe Act: Case of the Infusion PumpTim Bradley, RN, is a new intensive care unit nurse with 1 year experience. One evening,Tim is presented with a newly admitted, critically ill patient requiring intravenous antibi-otics, high-volume fluid resuscitation, and vasopressor and inotropic support therapy totreat progressive shock.The patient is deteriorating, and Tim is rapidly responding to eachailing system.
This particular shift, there had been a registered nurse sick call. This individual was notreplaced.The remaining nurses were very busy providing care to unstable patients. As a re-sult, Tim was independently handling his patient’s care needs.
Tim’s patient was prescribed dopamine 400 mg/250 ml @ 7 micrograms/kilogram/minute. The patient weighed 80 kilograms.
Unit policy required high-risk medication infusions via Smart Pump devices capable ofidentifying and preventing adverse drug events (ADE) when used as designed. Tim wasfamiliar with the correct use of the Smart Pump infusion devices and had been correctlyin-serviced; however, during his orientation, his preceptor had also encouraged Tim to by-pass the pump technology. Tim’s colleagues shared with him a variety of ways to avoid“dealing with the drug library and all those alerts!”The rationale was to “save time” by “by-passing” the information required when setting up the infusion device alerts.
Tim was in a hurry. His patient required many medications. Tim felt rushed and pres-sured. When he saw the dopamine infusion order, he decided to hang the medicationwithout the use of the Guardrails alerts. His intent was to go back after hanging the re-maining medications and set up the dopamine infusion as per policy.
Tim calculated the dopamine infusion rate. He set the infusion pump as per his calcula-tion. Tim did not realize that he had mistakenly calculated an infusion rate of 70 micro-grams/kilograms/minute. Within a short period of time, the patient exhibited tachycardiaand ventricular irritability with increased blood pressure significantly above the desired meanarterial pressure. Scared that he had made an error, Tim immediately rechecked thedopamine dosage and quickly discovered his error.The patient did not suffer apparent unto-ward effects once the dose was corrected; however, certainly the ADE could have been fatal.
This exemplar provides an overview of an unsafe act that violated an established rulebecause the rule violation was perceived as a routine, common act. Nurses had violated thisparticular rule on many occasions but the preconditions of nurse inexperience, high acuity,and inadequate supports in combination with established workarounds or shortcuts con-tributed to the actual adverse drug event.
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 294
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

exceeds the number of inpatient visits, the opportunity for error in that setting is alsoconsiderable (Aspden et al., 2004).
The frequencies and costs of patient safety incidents (PSI) that occurred in the hos-pitalized Medicare population are staggering. From 2004 to 2006, patient safety inci-dents (PSIs) cost the Medicare program $8.8 billion and resulted in 238,337potentially preventable deaths (HealthGrades, 2006). HealthGrades analyzed 41 mil-lion Medicare patient records and identified that those patients treated at top-performing hospitals had approximately a 43% lower chance of experiencing one ormore medical errors than if treated at the poorest-performing hospitals.
While HealthGrades found that the overall death rate among Medicare benefici-aries that developed one or more patient safety incidents had decreased by almost 5%during the 2-year period, four indicators had increased when compared to a 2004baseline. These indicators included postoperative respiratory failure, postoperativepulmonary embolism or deep vein thrombosis, postoperative sepsis, and postoperativeabdominal wound separation/splitting. These key areas are included in the currentfocus of regulatory (e.g., Joint Commission and Centers for Medicare and MedicaidServices [CMS]) (CMS and Joint Commission, 2008) and recommending (e.g., In-stitute for Healthcare Improvement [IHI]) agencies.
Since the release of the IOM report (Kohn et al., 2000), there has been an abun-dant volume of published patient safety-focused literature. Multiple recommendingand regulatory agencies offer guidelines and mandates. Many organizations provideevidence-based practice guidelines to assist clinicians in providing standardized evi-dence-based care.
The volume of materials and ever-changing safety standards and best practices maybe overwhelming to CNSs, particularly those who are new to putting patient safetyprinciples into practice. The CNS is absolutely pivotal in assessing the clinical envi-ronment for accident and error opportunities, collaborating with appropriate teammembers to proactively improve systems or to meaningfully react to occurrences, andrapidly evaluating the outcomes of systems changes. Actively engaging in this workrequires a preliminary review of the definitions of terms commonly used in patientsafety projects and publications (Table 9-1). The CNS concentrating on a patientsafety role integrates all the skill and competencies described in role-based CNS con-ceptualizations (Hamric, 1989; Oncology Nursing Society, 2003) and influence-basedmodels (American Association of Critical-Care Nurses [AACN], 2002; National As-sociation of Clinical Nurse Specialists [NACNS], 2004).
Creating a Just Culture for Patient SafetyCulture is a shared set of beliefs and values about how people work individually andtogether as teams (Phillips, 2005). It delineates a shared set of values and beliefs thatinfluences communication, social relations, and actions (Friersen, Farquhar, &Hughes, 2006). Achieving and sustaining a culture of safety requires an understand-ing of the values and beliefs within a particular organization. The safety culture of anorganization is the product of individual and group values, attitudes, perceptions,
Creating a Just Culture for Patient Safety 295
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 295
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

competencies, and patterns of behavior that combine to determine the commitmentto, and the style and proficiency of, an organization’s health and safety management(AHRQ, 2001).
The notion of a “just culture” is relatively recent and denotes a culture where peoplecan report mistakes, errors, accidents, or waste without negative repercussions(AHRQ, 2008a). In a just culture, individuals remain accountable for their actions butthey are not held responsible for flawed systems that permit earnest, trained people toerr. Sharing and disclosure are prominent features of a just culture because efficienciesand quality improvement processes depend on the frontline staff to drive improve-ments, and such drive requires a sense of safety. Staff must feel empowered to point outerrors, defects, and systems failures that could cause patient harm (AHRQ, 2008a). Ajust culture is not an “anything goes” culture. In other words, individuals may be heldpersonally accountable for intended actions that are unsafe and violate rules. But, inhighly protected systems with established defense systems, such unsafe acts are morelikely in a highly specific, often atypical, set of circumstances (Reason, 1990).
Organizations with a positive safety culture have characteristics in common. Theseorganizations have leaders who support bidirectional communications founded onmutual trust, with the ability for all employees to speak up and raise concerns, as wellas the willingness to listen when others have a concern. In addition, there are shared
296 Chapter 9 Patient Safety: Preventing Unintended Consequences and Reducing Errors
Table 9-1 DEFINITIONS OF KEY TERMS IN PATIENT SAFETY
Term Definition
Error
Near miss
Patient safety
Incident
Adverse event
Source: Aspden et al., 2004; Pronovost et al., 2005.
Mistakes made in the process of care that result in, or havethe potential to result in, harm to the patient.An act of commission or omission that could have harmedthe patient, but did not do so as a result of chance (IOM).The absence of the potential for, or occurrence of, healthcare-associated injury to patients. Created by avoiding medicalerrors as well as taking action to prevent medical errors fromcausing injury. Mistakes include failure of a planned action tobe completed as intended or the use of a wrong plan toachieve an aim. These can be the result of an action that istaken (error of commission) or an action that is not taken(error of omission).Unexpected or unanticipated events or circumstances notconsistent with the routine care of a particular patient, whichcould have, or did, lead to an unintended or unnecessaryharm to a person, or a complaint, loss, or damage.An injury resulting from a medical intervention.
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 296
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

perceptions of the importance of safety, coupled with a systems approach to analysis ofsafety issues (Friersen et al., 2006; Helmreich, 2005). Patient safety permeates the cul-ture, and there is an emphasis on continuous improvement (Friersen et al., 2006).Highly reliable organizations (HROs) tend to be exceptionally consistent and are par-ticularly good at avoiding error (AHRQ, 2008b). HROs are characterized by severalorganizing concepts: (1) sensitivity to operations with staff maintaining an ongoingorganizational awareness; (2) reluctance to simplify; (3) preoccupation with failure;(4) deference to expertise; and (5) resilience (AHRQ, 2008b).
Progress toward creating a culture of patient safety requires honest, routine error re-porting. Errors and near misses are reported in organizations in which staff feels safereporting errors. In organizations with a culture of patient safety, the emphasis is onwhy the error occurred, versus who made the error (see Figure 9-2). Leaders use errorsto help staff evaluate processes and learn how to prevent a recurrence of an error,rather than to blame.Two strategies encouraged by the Joint Commission that can as-sist with error analysis are failure mode and effects analysis (FMEA) and root causeanalysis strategies (RCA) (De Rosier & Stalhandske, 2006; Duwe, Fuchs, & Hansen-Flashen, 2005).
What strategies can the CNS use to assess the culture of safety within the practiceenvironment? AHRQ has tools posted on its Web site that can be downloaded free ofcharge to facilitate assessment of the safety culture within a hospital or nursing home.The tools are designed to provide institutions with the opportunity to assess their pa-tient safety cultures, track changes in safety over time, and evaluate the influence ofpatient safety interventions (AHRQ, 2008c).
Results of the AHRQ survey will assist the CNS and other members of the lead-ership team to assess the perception of patient safety within their organizations,whether errors are reported and discussed in an appropriate forum, and whetherthere is an atmosphere of continuous learning based on the principles of patientsafety. Each healthcare institution can use the completed survey data to calculatetheir percentage of positive responses on each item. Those data can be submitted toAHRQ for entry into a national database. The AHRQ Hospital Survey on PatientSafety Culture allows comparisons between the submitting hospital and other simi-lar hospitals. This report enables each hospital to compare itself to the benchmarkhospitals (AHRQ, 2008c).
Safety culture assessments are useful tools for measuring organizational conditionsthat lead to adverse events and patient harm in hospitals. The assessment is the start-ing point from which action planning begins and patient safety changes evolve (Sora& Nieva, 2003). Reassessments serve as barometers to measure the success of im-provement interventions. Once the cultural assessment is complete, the CNS can usethe data to integrate evidence-based guidelines into everyday practice for patient care.
Creating a Safe EnvironmentArmed with the culture assessment findings, the CNS must continue to examine thepractice environment with an eye on safety. Through assessment and analysis of the
Creating a Safe Environment 297
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 297
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

practice environment, the CNS begins to understand potential root causes of errorswithin that environment. The majority of medical errors do not occur as the result ofone person’s actions, but are the result of faulty systems, processes, and conditions thatlead people to make mistakes or fail to prevent them (Phillips, 2005).
298 Chapter 9 Patient Safety: Preventing Unintended Consequences and Reducing Errors
ASSESS - ERR™Medication System WorksheetPatient MR#
(if error reached patient)Date of error:
Drug(s) involved in error:
Non-formulary drug(s)?Drug sample(s)?Drug(s) packaged in unit dose/unit of use?Drug(s) dispensed from pharmacy?Error within 24 hours of admission, transfer, or after discharge?Did the error reach the patient?Source of IV solution:
Date information obtained:
Incident #✓ if no callback identified:Patient age:
Brief description of the event: (what, when, and why)
❑ Yes❑ Yes❑ Yes❑ Yes❑ Yes❑ Yes❑ Pharmacy IV admixture
❑ No❑ No❑ No❑ No❑ No❑ No
❑ Nursing IV admixture❑ Manufacturer premixed solution
❑ Testing ❑ Additional observation ❑ Gave antidote ❑ Care escalated (transferred, etc.) ❑ Additional LOS ❑ Other
Possible causes Y/N CommentsCritical patient information missing?(age, weight, allergies, BS, lab values, pregnancy, patientidentity, location, renal/liver impairment, diagnoses, etc.)
Critical drug information missing?(outdated/absent references, inadequate computer screening,inaccessible pharmacist, uncontrolled drug formulary, etc.)
Miscommunication of drug order?(illegible, ambiguous, incomplete, misheard, ormisunderstood orders, intimidation/faulty interaction, etc.)Drug name, label, packaging problem?(look/sound-alike names, look-alike packaging,unclear/absent labeling, faulty drug identification, etc.)
Drug stoage or delivery problem?(slow turn around time, inaccurate delivery, doses missing orexpired, multiple concentrations, placed in wrong bin,etc.)
Drug delivery device problem?(poor device design, misprogramming, free-flow, mixed uplines, IV administration of oral syringe contents, etc.)
Environmental, staffing, or workflow problems?(lighting, noise, clutter, interruptions, staffing deficiencies,workload, inefficient workflow, employee safety, etc.)
Lack of staff education?(competency validation, new or unfamiliar drugs/devices,orientation process, feedback about errors/prevention, etc.)
Patient education problem?(lack of information,noncompliance, not encouraged to askquestions, lack of investigating patient inquiries, etc.)
Lack of quality control or independent check systems?(equipment quality control checks, independent checks forhigh alert drugs/high risk patient population drugs etc.)
Did the patient require any of the following actions after the error that you would not have done if the event had not occurred?
Patient outcome:
@2006 Institute for Safe Medication Practices
Figure 9-2 Assess-ERR Medication Safety System Worksheet.Source: © 2006, Institute for Safe Medication Practices. Reprinted with permission.
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 298
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

AHRQ has identified factors that contribute to errors: communication, inadequateflow of information, human problems, patient-related issues, organizational transferof knowledge, staffing patterns and work flow, technical failures, and inadequate poli-cies and procedures (AHRQ, 2003). Table 9-2 presents each of these factors with anexample of how they apply to bedside practice.
When assessing the role each factor plays in contributing to errors within the prac-tice environment, the CNS must also assess how staff has adapted its practice to workaround systematic obstructions to completing work. Nurses have unparalleled skill atdeveloping workarounds. In other words, what can the nurse do to solve the issue forthe patient today?
Although this strategy does garner short-term success, it creates long-term prob-lems. As a simple example, if a nurse does not have a patient’s medications and solvesthis problem by borrowing medications from another patient, this exemplifies first-order problem solving (Tucker & Edmondson, 2002). The nurse has met the needs ofthe patient in the immediate period by securing the needed medications. But, ofcourse, the medications are now no longer available for the patient for whom theywere intended.
In examining this simple issue, numerous other issues arise: What about the patientwhose medications were taken (his or her dose is now missing)? What if it is a slightlydifferent dose? What will keep this situation from arising tomorrow? Bedside nurses’role supports first-order problem solving. Nurses at the point-of-care do not have theresources (mainly time) to do second-order problem solving (Tucker & Edmondson,2002).
The role of the CNS in this scenario is critical. Second-order problem solving in-volves a system analysis of why the error occurred—what part of the system failed thenurse and the patient (Tucker & Edmondson, 2002). To have more than a temporaryfix, the root cause of the problem must be uncovered. It is often easier to work aroundproblems, especially when the staff nurses believe that they have reported this issuepreviously and no action has been taken. The CNS must partner with the staff nurseto investigate the concern and to craft a reasonable, efficient solution to the clinicalproblem. Partnering facilitates staff buy-in, because the nurses helped to broker thesolution. The CNS must make it easier for staff to do the right thing while making itmore difficult to do a workaround.
One essential support to sustaining a culture of safety is the creation of a healthywork environment (HWE). The attributes of a healthy work environment are symbi-otic with a culture of patient safety. The American Association of Critical-CareNurses’ (AACN) Healthy Work Environment standards demonstrate a commitmentto creating a positive work environment that facilitates safety (Barden, 2005). Eachstandard is clarified by essential (absolutely required, fundamental), standard (author-itative statement), and critical elements (structures, processes, programs, and behav-iors required for a standard to be achieved).
The first healthy work environment standard is skilled communication; nursesmust be as proficient in communication skills as they are in clinical skills.The conceptof communication is complex, encompassing verbal, written, and nonverbal skills. Inreviewing sentinel events, the Joint Commission has identified team communication
Creating a Safe Environment 299
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 299
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

300 Chapter 9 Patient Safety: Preventing Unintended Consequences and Reducing Errors
Table 9-2 FACTORS THAT CONTRIBUTE TO ERRORS
Factor Description Examples of Interventions for CNS
Communication Verbal/nonverbal,written (e.g., in e-mail communication).Between any mem-bers of the team:nurse, physician,family, support staff,therapists.NPSG #2: “Improvethe effectiveness ofcommunicationamong caregivers”( Joint Commission,2006).
1. Conduct briefings: Role-model efficient and effectivebidirectional communicationwith all team members. Whenpreparing to perform a proce-dure, review each step beforebeginning to prevent miscom-munication.
2. Be assertive: Create an envi-ronment where any member ofthe team feels comfortable invoicing their concern. Utilizethe SBAR strategy to commu-nicate a message that is clearand concise.
3. Develop situational awareness:Place signs outside the patient’sdoor, be sure all staff are awareof patients who are “at risk” forfalls or other clinical issues.
4. Understand the differencebetween the novice and theexpert in making decisions:Decisions are made based onpast experience, and becausethe novice has little past expe-rience, he or she may rely moreon the CNS to support his orher decision-making process.
5. Conduct debriefings: After asignificant clinical event, re-view with the staff the pre-event situation, the event, andthe response to the event. Lis-ten to the staff ’s perception ofwhat happened. The CNS maybe able to use the informationto plan future education.
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 300
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

Creating a Safe Environment 301
Table 9-2 (continued)
Factor Description Examples of Interventions for CNS
Communication(continued)
Inadequate flow of information
Human problems
Members of the teammay not have the in-formation they needto appropriately carefor the patient.NPSG #2, to“Improve the effec-tiveness of communi-cation,” includes arequirement for astandardized handoffof communications( Joint Commission,2006).How standards ofcare, policies, andprocedures arefollowed.Other factors thatplay a role: fatigue,stress, distractions,interruptions, and
6. SBAR strategy: Develop atemplate for the use of theSBAR strategy, including a fewkey clinical characteristics. Forexample, if caring for a thoracicpopulation, always include anassessment of breath soundsand pattern of breathing.
1. Examine the handoff processwithin the practice environ-ment; include nurses, physi-cians, pharmacists, etc.
2. Partner with other members ofthe team to create a handofftool that would enable clear,concise communication.
1. CNS plays a key role in the design, development, imple-mentation, and evaluation ofpolicies.
2. Partner with the nurse managerand bedside nurses to establishthe standards of care within thepractice environment.
3. Evaluate the practice environ-ment for factors that may influence care.
4. Develop a peer-review processto enable the staff to hold eachother accountable for caredelivered.
(continues)
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 301
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

302 Chapter 9 Patient Safety: Preventing Unintended Consequences and Reducing Errors
Table 9-2 (continued)
Factor Description Examples of Interventions for CNS
Patient-related issues
Organizational transfer of knowledge
Staffing patterns/workflow
multitasking.Incomplete assess-ment, which mayinclude allergies, orduplicate or missingmedications.NPSG #8 requires ac-curate and completereconciliation of med-ications across thecontinuum of care.Patient identifica-tion, utilizing twounique identifiers(NPSG #1) ( JointCommission, 2006).Formal transfer ofknowledge occursduring orientation,education, and com-petency assessments.Informal.
Supplies: disjointed,missing, not easilyavailable to the nurse.Assignmentsgeographicallyundesirable.
1. Monitor patient identification:As you make rounds on eachpatient, ask the patient if thestaff have been checking his orher identification.
2. Ensure that there is a clearprocess if the identification isincorrect.
3. Partner with bedside nurses,pharmacists, physicians, andnursing leadership to establisha process for medicationreconciliation.
1. In collaboration with other ex-perts, design, develop, andevaluate clinical competenciesas they relate to the care of adefined population.
2. Develop a tool for a brief ori-entation to your practice areafor staff who are pulled, poolnurses, or agency staff. Includeemergency equipment, sup-plies, medications, a short les-son on how to contact thephysicians; anything that isimportant about your patientpopulation.
1. Review work by Ebright andcolleagues who have studiedthe flow of “nurse work”(Ebright, 2004).
2. Start with one simple project:What does a nurse need toperform safe, aseptic intra-
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 302
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

Creating a Safe Environment 303
as a top contributor to sentinel events ( Joint Commission, 2006). Healthcare organi-zations are obligated to help staff develop excellent communication skills. Skilledcommunicators focus on finding solutions and desirable outcomes, advancing col-laborative relationships, listening as intently as they speak, and demonstrating mutual
Table 9-2 (continued)
Factor Description Examples of Interventions for CNS
Staffing patterns/workflow(continued)
Technical failures
Inadequate policies and procedures
Source: AHRQ, 2003; Phillips, 2005.
Frequent interruptions/distractions.Mechanical devicescan malfunction.
Policies that are toolong, too wordy, outof date, or not easilyaccessible will not beutilized.
venous line care? If the care isdone at the patient’s bedside,the supplies should be at thebedside, not in the supplyroom.
3. Discuss with the staff changesin where/how medications are prepared to decrease, andeventually eliminate interruptions/distractionswhen preparing medications.
1. Ensure that contact numbersfor experts (in house or fromthe companies) are easily acces-sible, particularly for life-sus-taining equipment; for example,ventricular assist devices.
2. Plan and execute drills for allequipment that is low volume,high risk (continuous renal re-placement machines, postcar-diac arrest hypothermia devices).
1. Participate in policy reviewand revision, with an eye forpracticality (e.g., if the policy is28 pages single spaced, it is notlikely to be used).
2. Promote electronic availabilityof nursing policies and medi-cation information (e.g.,online policy manuals or medi-cation manuals).
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 303
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

respect (Barden, 2005). The CNS must role model expert communication techniquesand offer constructive feedback to staff nurses as they develop their communicationskill sets.
One strategy that has been effective in facilitating clear, direct communicationamong caregivers is the SBAR strategy. SBAR is an acronym for situation, background,assessment, and recommendation (Leonard, Graham, & Bonacum, 2004). SBAR is a sit-uational briefing model characterized by appropriate assertion, critical language, andawareness and education. It is a vital model designed to address the different commu-nication styles used and valued by nurses, physicians, and other clinicians (Table 9-3).
304 Chapter 9 Patient Safety: Preventing Unintended Consequences and Reducing Errors
Table 9-3 SBAR
30–60 Second Communication
Situation
Background
Assessment
Recommendation
Source: Leonard et al., 2004; Phillips, 2005.
What is happening with the patient?Example:“Hello, Dr. Jones, this is Susan, I am calling from 2West. I am taking care of Mr. Green in room 212,a patient of Dr. Johnson’s who went to the OR today for a colectomy. He has been back from the PACU for 4 hours. I have just reassessed him.”What is the important clinical information?“Over the past 4 hours, his BP has dropped from120/78 to 90/58, his heart rate has increased from 70 to100, his respiratory rate is 24, and his urine output was80 mL/hour for the first 2 hours and has dropped to 30mL each hour for the past 2 hours.He is receiving IV fluids, D5.45NS + 20 meq KCL at125 mL/hour.His postop labs were unremarkable, his hemoglobinwas 10.2.His estimated blood loss was 450 mL.”What do you think the problem is?“I think he is dry.”What do you think he needs? If you think the patientneeds to be seen by the physician or nurse practi-tioner, do not be afraid to say so.“I think he needs more fluid.”
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 304
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

Creating a Safe Environment 305
The CNS can assist staff with developing a template for communicating withphysicians and other team members using the SBAR strategy and incorporating theconsistent use of particular elements that relate to the specific patient population. Forexample, if caring for a neuroscience population, the assessment of the GlasgowComa Score (GCS) would always be included in every communication. Additionalstrategies to improve communication include conducting briefings, being assertive,developing situational awareness, understanding the differences in expert and novicedecision making, and conducting debriefings (Volker & Clark, 2004). Communica-tion successes will develop over time and will occur only with practice, repetition, andconstructive feedback to staff.
The second healthy work environment standard is true collaboration: Nurses mustbe relentless in pursuing and fostering true collaboration.True collaboration can buildon the relationships fostered through skilled communication. It is a relationshipgrounded in respect and trust. Nurse–physician collaboration is one of the threestrongest predictors of nurse empowerment. One of the critical elements of true col-laboration is that “every team member contributes to the achievement of commongoals by giving power and respect to each person’s voice, integrating individual differ-ences, resolving competing interests, and safeguarding the essential contribution eachmust make in order to achieve optimal outcomes” (Barden, 2005, p. 21). Authenticcollaboration is revealed through relationships with other nurse leaders, physicians,and administrators.
The third standard is effective decision making: Nurses must be valued and com-mitted partners in making policy, directing and evaluating clinical care, and leadingorganizational operations (Barden, 2005). Nurses have primary responsibility for pa-tient safety, but only 8% of physicians recognize the nurse as part of the decision-making team (Cook, Hoas, Guttmannova, & Joyner, 2004). Effective decision making bridges the autonomy–accountability gap by empowering nurses to be the decision-making authority in the care of their patient.
The fourth healthy work environment standard addresses appropriate staffing:Staffing must ensure the effective match between patient needs and nurse competen-cies (Barden, 2005). Some CNSs may play a functional role in staffing by either beingaccountable to make sure enough staff is present or filling in when staffing is short.One clear role for the CNS in any staffing pattern is to collaborate with the nursemanager and staff nurses to look at the nurse work flow and the relationship tostaffing. Are there staff members uninvolved in patient care for parts of the day thatcould have time schedules flexed? Are there times when the CNS must partner withthe manager to assert that the staff has reached a critical workload point and cannottake any more patients? This standard builds on the first, second, and third standards,wherein all the skills can combine to provide excellent communication, collaboration,and decision making to solve complex staffing issues.
Meaningful recognition is the fifth standard: Nurses must be recognized and mustrecognize others for the value each brings to the work of the organization (Barden,
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 305
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

2005). Recognition was important to 75% of the nurses in the healthy work environ-ment study. A formalized process for recognition is essential for it to be effective. TheCNS must be knowledgeable about recognition programs nationally (as with profes-sional organizations), regionally (as with local chapters or statewide awards), or withinthe organization. The CNS must lead the recognition initiative to ensure that excel-lence in clinical practice, communication, patient–family relationships, and other keyperformance measures are recognized.
The final standard is authentic leadership: Nurse leaders must fully embrace theimperative of a healthy work environment, authentically live it, and engage others inthe achievements (Barden, 2005). Authentic leaders are supported by their organiza-tion in developing skills and competency in skilled communication, true collabora-tion, effective decision making, meaningful recognition, and authentic leadership.Establishing and sustaining a practice environment that is supported by the conceptsin the healthy work environment standards contributes to a hospital culture rich insafety, which contributes to an environment of patient safety.
Safety and Quality OrganizationsThe complexity of regulatory agencies and recommending organizations withinhealth care is extraordinary. The CNS is frequently held accountable for compliancewith multitudes of guidelines, competencies, rules, and regulations. In developingclinical programs for improvement, which may be in response to a regulatory require-ment, the CNS must partner with the bedside nurse to collaborate with numerousdisciplines to establish compliance strategies for each regulation or guideline.
Joint Commission accreditation is a nationwide seal of approval indicating that or-ganizations meet high performance standards. The Joint Commission and JointCommission International were designated in 1995 as the World Health Organiza-tion (WHO) Collaborating Centre for Patient Safety Solutions (WHO Collaborat-ing Centre for Patient Safety Solutions, 2008).
There are numerous regulatory and recommending agencies that address health-care safety and quality; many of their recommendations overlap and are quite similargiven their shared evidence base. Key organizations include, but are not limited to, theCenter for Medicare and Medicaid (CMS), Institute for Healthcare Improvement(IHI), AHRQ, National Patient Safety Goals (NPSG), Joint Commission, and Na-tional Quality Foundation (NQF).
Tools of the TradeThe World Wide Web has dramatically influenced patient care delivery. The role ofthe CNS in patient safety is inextricably linked to the use of electronically availabletools in the form of assessment tools, guidelines, and other references, many of whichcan be downloaded without charge. Professional organizations, not-for-profit (NFP)recommending organizations, governmental agencies, regulatory bodies, and evidence-based practice Web sites offer many useful resources (refer to Tables 9-4 through 9-8).
306 Chapter 9 Patient Safety: Preventing Unintended Consequences and Reducing Errors
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 306
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

Tools of the Trade 307Ta
ble
9-4
EXA
MP
LES
OF
WEB
SIT
ES W
ITH
PA
TIEN
T SA
FET
Y IN
FOR
MA
TIO
N (P
SI):
PR
OFE
SSIO
NA
L O
RG
AN
IZA
TIO
NS
Web
Sit
eCo
nten
tsCN
S B
enef
its
http
://w
ww
.aac
n.or
g/W
D/H
WE
/D
ocs/
HW
ESt
anda
rds.
Am
eric
an A
ssocia
tion
ofC
riti
cal
Car
e Nur
ses (
AA
CN
)A
cces
sed:
Dec
embe
r 9,2
008
http
://w
ww
.ons
.org
/pub
licat
ions
/po
sitio
ns/p
atie
ntsa
fety
.sht
ml
Onc
olog
y N
ursin
g So
ciety
(ON
S)A
cces
sed:
Dec
embe
r 9,2
008
http
://w
ww
.aor
n.or
g/ab
outa
orn/
who
wea
re/p
atie
ntsa
fety
first
Asso
ciati
on o
fper
iOpe
rati
ve R
egist
ered
N
urse
s (A
OR
N)
Acc
esse
d:D
ecem
ber 9
,200
8
Hea
lthy
wor
k en
viro
nmen
t sta
ndar
ds:
Six
key
fact
ors i
n cr
eatin
g an
d su
stai
ning
ahe
alth
y w
ork
envi
ronm
ent (
HW
E).
Ava
ilabl
eto
dow
nloa
d th
e fu
ll do
cum
ent o
r the
exe
cutiv
esu
mm
ary.
Prac
tice
Ale
rts:
Ele
ven
succ
inct
,dyn
amic
evi
denc
e-ba
sed
guid
elin
es d
esig
ned
to c
lose
the
rese
arch
–pr
actic
e ga
p an
d fa
cilit
ate
stan
dard
ized
pr
actic
e.
Posi
tion
stat
emen
t on
patie
nt sa
fety
Iden
tifyi
ng,c
olle
ctin
g,an
d de
velo
ping
clin
ical
and
educ
atio
nal r
esou
rces
to im
prov
e pa
tient
safe
ty in
the
surg
ical
sett
ing.
In a
dditi
on:
•G
ener
al re
sour
ces—
links
to n
umer
ous
patie
nt sa
fety
site
s•
AO
RN
reso
urce
s and
jour
nal a
rtic
lere
fere
nces
Prov
ides
evi
denc
e-ba
sed
guid
elin
esth
at su
ppor
t the
six
key
fact
ors i
ncr
eatin
g a
HW
E.T
he C
NS
can
op-
erat
iona
lize
thes
e gu
idel
ines
tom
eet t
he n
eeds
of t
he p
ract
ice
envi
ronm
ent.
Onc
olog
y nu
rses
can
use
this
stat
e-m
ent t
o fo
rmul
ate
thei
r ow
n po
si-
tion
stat
emen
t on
patie
nt sa
fety
.
Res
ourc
es o
n th
is si
te a
pply
to p
eri-
oper
ativ
e,po
stop
erat
ive
and
proc
e-du
ral s
taff
.The
se re
sour
ces c
an b
eus
ed to
dev
elop
edu
catio
n pr
o-gr
ams,
orie
ntat
ion
prog
ram
s,an
dpa
tient
safe
ty p
rogr
ams.
(con
tinu
es)
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 307
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

308 Chapter 9 Patient Safety: Preventing Unintended Consequences and Reducing Errors
Tab
le 9
-4(c
on
tin
ued
)
Web
Sit
eCo
nten
tsCN
S B
enef
its
•L
ist o
f pat
ient
safe
ty jo
urna
ls an
d ne
wsle
tter
s•
Patie
nt sa
fety
boo
ks a
nd m
edia
•Jo
int C
omm
issi
on p
atie
nt sa
fety
pra
ctic
eson
line
•Jo
urna
l sca
n•
Posi
tion
stat
emen
t on
patie
nt sa
fety
•N
urse
con
sulta
tion
oppo
rtun
ities
•C
orre
ct si
tes s
urge
ry to
olki
t•
Nat
iona
l Tim
e-O
ut D
ay
Site
is d
esig
ned
to p
rom
ote
safe
ane
sthe
sia
patie
nt c
are
by e
duca
ting
the
publ
ic.C
on-
tain
s nee
d-to
-kno
w in
form
atio
n fo
r ane
sthe
-si
a pa
tient
s:•
“Pat
ient
Can
dor E
ssen
tial f
or S
afe
Ane
sthe
siaC
are”
;the
full
stor
y di
scus
ses t
he im
port
ance
of fu
ll di
sclo
sure
to th
e an
esth
esia
pro
vide
r.•
“New
Ane
sthe
sia
Stan
dard
s for
Off
ice
Sur-
geri
es”;
refle
cts t
he A
AN
A n
ew st
rict
stan
-da
rds f
or o
ffic
e su
rger
ies.
•“C
onsc
ious
Sed
atio
n”;d
iscu
sses
whi
ch ty
pes
of su
rger
y an
d pr
oced
ures
can
be
done
with
cons
ciou
s sed
atio
n.
Thi
s site
con
tain
s ext
ensi
ve re
-so
urce
s for
pat
ient
edu
catio
n,w
hich
coul
d be
inco
rpor
ated
into
a p
re-o
ped
ucat
ion
prog
ram
.
http
://w
ww
.ane
sthe
siap
atie
ntsa
fety
.co
mA
mer
ican
Asso
ciati
on o
fNur
seA
nest
heti
sts (
AA
NA
)A
cces
sed:
Dec
embe
r 9,2
008
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 308
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

Tools of the Trade 309Ta
ble
9-4
(co
nti
nu
ed)
Web
Sit
eCo
nten
tsCN
S B
enef
its
Lin
k to
“Ane
sthe
sia
and
Your
Chi
ld,”
prov
ides
a st
ory
and
a co
lori
ng b
ook
for c
hild
ren
who
are
abou
t to
have
ane
sthe
sia
to a
llay
fear
s.
Site
con
tain
s res
ourc
es fo
r bot
h th
e nu
rse
and
the
patie
nt/f
amily
.•
Lin
k to
ask
a c
linic
al p
ract
ice
ques
tion
and
num
erou
s org
aniz
atio
nal c
omm
ittee
s,su
chas
edu
catio
n an
d ev
iden
ce-b
ased
pra
ctic
e•
Nur
sing
Cor
e C
urri
culu
m fo
r Per
iane
sthe
sia
Nur
ses
•Fo
r pat
ient
s,an
ext
ensi
ve se
ctio
n on
wha
t to
expe
ct fr
om th
e pr
e-ad
mis
sion
inte
rvie
wth
roug
h di
scha
rge
The
Rol
e of
the
Nur
se E
xecu
tive
in P
atie
ntSa
fety
:1.
Lea
d cu
ltura
l cha
nge
2.Pr
ovid
e sh
ared
lead
ersh
ip3.
Bui
ld e
xter
nal p
artn
ersh
ips
4.D
evel
op le
ader
ship
com
pete
ncie
s
The
pre
-adm
issi
on in
terv
iew
can
begi
n th
e pr
oces
s of m
edic
atio
nre
conc
iliat
ion,
to c
ompl
y w
ith th
eJo
int C
omm
issi
on N
atio
nal P
atie
ntSa
fety
Goa
l on
med
icat
ion
reco
n-ci
liatio
n.
The
CN
S ca
n pa
rtne
r with
the
nurs
e ex
ecut
ive
to le
ad c
ultu
ral
chan
ge a
cros
s dis
cipl
ines
,as w
ell a
sde
velo
p an
d dr
ive
patie
nt sa
fety
ini-
tiativ
es a
cros
s the
org
aniz
atio
n.
http
://w
ww
.asp
an.o
rgA
mer
ican
Socie
ty o
fPer
iane
sthe
-sia
Nur
ses (
ASP
AN
)A
cces
sed:
July
23,
2006
http
://w
ww
.aon
e.or
g/ao
ne/
pdf/
Rol
e%20
of%
20th
e%20
Nur
se%
20E
xecu
tive%
20in
%20
Patie
nt%
20Sa
fety
%20
Too
lkit_
July
2007
Am
erica
n A
ssocia
tion
ofN
urse
Exe
cu-
tive
s (A
ON
E)
Acc
esse
d:D
ecem
ber 9
,200
8
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 309
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

310 Chapter 9 Patient Safety: Preventing Unintended Consequences and Reducing Errors
Tab
le 9
-5EX
AM
PLE
S O
F W
EB S
ITES
WIT
H P
SI:N
OT-
FOR
-PR
OFI
T “R
ECO
MM
END
ING
”O
RG
AN
IZA
TIO
NS
Web
Sit
eCo
nten
tsCN
S B
enef
its
http
s://
ww
w.e
cri.o
rg/P
ages
/de
faul
t.asp
xE
CR
I Ins
titu
teA
cces
sed:
Dec
embe
r 9,2
008
http
://w
ww
.ism
p.or
gIn
stit
ute f
or S
afe M
edica
tion
P
ract
ices (
ISM
P)A
cces
sed:
Dec
embe
r 9,2
008
Des
igna
ted
by A
HR
Q/W
orld
Hea
lth O
rgan
i-za
tion
as a
n ev
iden
ce-b
ased
pra
ctic
e ce
nter
.A
dmin
iste
rs:N
atio
nal Q
ualit
y M
easu
res
Cle
arin
g H
ouse
;Nat
iona
l Gui
delin
esC
lear
ingh
ouse
Com
plet
e lis
t of t
echn
olog
y as
sess
men
ts a
ndev
iden
ce-b
ased
repo
rts
A “c
onsu
mer
repo
rts”
for m
edic
al d
evic
esM
DSR
—m
edic
al d
evic
e in
cide
nt a
nd h
azar
din
form
atio
nP
ublis
hes H
ealth
Dev
icesj
ourn
al
Ext
ensi
ve re
sour
ces f
or st
aff a
nd p
atie
nts:
•E
duca
tion:
new
slet
ters
,edu
catio
nal p
ro-
gram
s,se
lf-as
sess
men
ts,p
atie
nt sa
fety
vid
eo
•M
edic
atio
n sa
fety
tool
s and
reso
urce
s:hi
gh-
aler
t med
icat
ion
list,
conf
used
dru
g lis
t,er
ror-
pron
e ab
brev
iatio
n lis
t,do
-not
-cru
sh li
st•
“Pat
hway
s for
Med
icat
ion
Safe
ty”;
an e
xten
-si
ve p
rogr
am fo
r med
icat
ion
safe
ty th
at c
anbe
dow
nloa
ded
for f
ree
•U
SP—
ISM
P M
edic
atio
n E
rror
repo
rtin
gsy
stem
The
CN
S pl
ays a
key
role
in p
rod-
uct s
elec
tion.
The
tech
nolo
gy a
s-se
ssm
ent o
n th
e E
CR
I Web
site
can
assi
st in
ass
essi
ng th
e sa
fety
of a
tech
nolo
gy,a
s wel
l as o
ffer
ing
ano
nbia
sed
com
pari
son
of d
iffer
ent
prod
ucts
that
pro
vide
the
sam
ete
chno
logy
.The
CN
S ca
n al
so se
ekou
t gui
delin
es fo
r a b
road
rang
e of
clin
ical
issu
es.
Man
y to
ols w
ill a
ssis
t with
com
pli-
ance
with
Join
t Com
mis
sion
NP
SGto
:•
Impr
ove
the
safe
ty o
f usi
ng m
edic
a-tio
ns
•A
ccur
atel
y an
d co
mpl
etel
y re
conc
ilem
edic
atio
ns a
cros
s the
con
tinuu
mof
car
e“P
athw
ays f
or M
edic
atio
n Sa
fety
”w
ill g
uide
the
CN
S in
cre
atin
g a
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 310
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

Tools of the Trade 311Ta
ble
9-5
(co
nti
nu
ed)
Web
Sit
eCo
nten
tsCN
S B
enef
its
•L
inks
to n
umer
ous p
atie
nt sa
fety
site
s•
Asse
ss-E
RR
Med
icati
on S
yste
m W
orks
heet
tofa
cilit
ate
med
icat
ion
use
syst
em e
valu
atio
ns(F
igur
e 9-
2)
Nat
iona
l Pat
ient
Saf
ety
Foun
datio
n:•
Cre
ate
a co
re b
ody
of k
now
ledg
e•
Dev
elop
a c
ultu
re re
cept
ive
to sa
fety
•R
aise
pub
lic a
war
enes
s•
Fost
er c
omm
unic
atio
ns
Spon
sors
edu
catio
nal p
rogr
ams,
patie
nt sa
fety
fello
wsh
ips;
educ
atio
nal v
ideo
s,ne
wsl
ette
rs
Res
ourc
es a
re a
vaila
ble
for p
atie
nts,
fam
ilies
,an
d ca
regi
vers
med
icat
ion
safe
ty p
rogr
am a
s a c
ol-
labo
rativ
e w
ith p
harm
acy.
Mon
thly
new
slet
ter c
onta
ins i
nfor
-m
atio
n to
impr
ove
med
icat
ion
ad-
min
istr
atio
n pr
oces
s.
“Whe
n th
ings
go
wro
ng…
”is a
docu
men
t fro
m th
e H
arva
rd H
os-
pita
ls to
teac
h ph
ysic
ians
and
nur
ses
wha
t to
do if
som
ethi
ng g
oes
wro
ng.T
he C
NS
can
use
this
inco
llabo
rativ
e fo
rum
s for
phy
sici
ans
and
nurs
es to
dis
cuss
pla
ns o
n ho
wto
resp
ond
whe
n an
adv
erse
eve
ntoc
curs
.
http
://w
ww
.nps
f.org
Nat
iona
l Pat
ient
Saf
ety
Foun
dati
on
(NPS
F)
Acc
esse
d:D
ecem
ber 9
,200
8
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 311
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

312 Chapter 9 Patient Safety: Preventing Unintended Consequences and Reducing Errors
Tab
le 9
-6EX
AM
PLE
S O
F W
EB S
ITES
WIT
H P
SI:G
OV
ERN
MEN
T A
GEN
CIE
S
Web
Sit
eCo
nten
tsCN
S B
enef
its
http
://w
ww
.ahr
q.go
v/cl
inic
/pts
afet
y/pd
f/pt
safe
ty.p
dfA
genc
y fo
r Hea
lthca
re R
esea
rch
and
Qua
lity
(AH
RQ
)A
cces
sed:
Dec
embe
r 9,2
008
http
://w
ww
.ahr
q.go
v/qu
al/
patie
ntsa
fety
cultu
re/h
osps
urvi
ndex
.ht
mA
genc
y fo
r Hea
lthca
re R
esea
rch
and
Qua
lity
(AH
RQ
)A
cces
sed:
May
6,2
009
http
://w
ww
.psn
et.a
hrq.
gov
AH
RQ
Pat
ient
Saf
ety
Net
wor
kA
cces
sed:
Dec
embe
r 9,2
008
“Mak
ing
Hea
lthca
re S
afer
:Cri
tical
ana
lysi
s of
Patie
nt S
afet
y Pr
actic
es (2
001)
.”T
he a
im o
fth
is e
xten
sive
doc
umen
t was
to c
olle
ct a
nd re
-vi
ew e
xist
ing
evid
ence
on
prac
tices
rele
vant
toim
prov
ing
patie
nt sa
fety
.Ele
ven
prac
tices
wer
eid
entif
ied
and
rate
d m
ost h
ighl
y in
term
s of
stre
ngth
of e
vide
nce.
Hos
pita
l Sur
vey
on P
atie
nt S
afet
y C
ultu
re(2
004)
:how
to a
dmin
iste
r the
surv
ey,h
ow to
anal
yze
and
inte
rpre
t the
resu
lts
Thi
s res
ourc
e is
ava
ilabl
e as
an
e-m
ail f
rom
the
AH
RQ
,whi
ch p
rovi
des a
con
tinuo
usly
up-
date
d,an
nota
ted,
and
care
fully
sele
cted
col
lec-
tion
of p
atie
nt sa
fety
new
s,lit
erat
ure,
tool
s,an
dre
sour
ces.
Als
o co
ntai
ns th
e “p
atie
nt sa
fety
clas
sics
,”in
clud
ing
the
mos
t inf
luen
tial,
fre-
quen
tly c
ited
artic
les,
book
s,an
d re
sour
ces i
npa
tient
safe
ty.
The
se e
leve
n pr
actic
es c
an b
e in
te-
grat
ed in
to a
uni
t-ba
sed
patie
ntsa
fety
pro
gram
.
The
CN
S ca
n us
e th
is to
ol to
beg
inan
env
iron
men
tal a
sses
smen
t of t
hepa
tient
safe
ty c
ultu
re o
f the
pra
ctic
ear
ea.
Sinc
e th
is is
aut
omat
ical
ly se
ntfr
om th
e A
HR
Q,i
t kee
ps th
e C
NS
abre
ast o
f all
the
key
rece
nt p
atie
ntsa
fety
lite
ratu
re.
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 312
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

Tools of the Trade 313Ta
ble
9-6
(co
nti
nu
ed)
Web
Sit
eCo
nten
tsCN
S B
enef
its
Med
ical
err
ors a
nd p
atie
nt sa
fety
:•
Onl
ine
jour
nals
•41
pat
ient
safe
ty d
ocum
ents
for s
taff
and
patie
nts
•Pa
tient
Saf
ety
Tas
k Fo
rce
info
rmat
ion
•T
he F
eder
al Q
ualit
y In
tera
genc
y C
oord
ina-
tion
Qul
C T
ask
Forc
e:en
sure
s tha
t all
fed-
eral
age
ncie
s tha
t pur
chas
e,pr
ovid
e,st
udy,
orre
gula
te h
ealth
care
serv
ices
are
wor
king
in a
coor
dina
ted
way
tow
ard
the
com
mon
goa
l of
impr
ovin
g th
e qu
alit
y of
car
e•
Con
fere
nces
and
wor
ksho
ps
Nur
sing
act
iviti
es a
ssoc
iate
d w
ith th
e A
HR
Q:
•N
ursi
ng re
sear
ch•
Res
earc
h fu
ndin
g •
Too
ls a
nd re
sour
ces;
for e
xam
ple,
palli
ativ
ew
ound
car
e at
the
end
of li
fe•
Lis
t of 1
6 lin
ks fo
r nur
sing
reso
urce
s•
Kee
ping
pat
ient
s saf
e:T
rans
form
ing
the
wor
k en
viro
nmen
t for
nur
ses
Tea
mw
ork
is a
n es
sent
ial c
ompo
-ne
nt in
pat
ient
safe
ty.T
his s
ite c
on-
tain
s a li
nk to
:AH
RQ
’s M
edic
alT
eam
wor
k an
d Pa
tient
Saf
ety:
Com
pete
ncie
s on
know
ledg
e,sk
ill,
and
attit
udes
.The
CN
S ca
n us
eth
ose
com
pete
ncie
s to
stru
ctur
e a
team
app
roac
h to
a n
umbe
r of c
lini-
cal i
nitia
tives
;the
dev
elop
men
t of a
rapi
d re
spon
se te
am is
a g
ood
ex-
ampl
e.In
add
ition
to a
cces
s to
the
onlin
e jo
urna
ls,t
he in
form
atio
nco
ntai
ned
in th
e pa
tient
safe
ty d
oc-
umen
ts is
ext
ensi
ve.
In a
sses
sing
a c
linic
al is
sue,
this
site
prov
ides
link
s to
the
AH
RQ
Evi
-de
nce-
Bas
ed P
ract
ice
Cen
ter,
Na-
tiona
l Gui
delin
es C
lear
ingh
ouse
,N
atio
nal Q
ualit
y M
easu
res C
lear
-in
ghou
se,a
nd o
ther
s.T
he C
NS
can
utili
ze a
ll th
ese
links
to b
egin
est
ab-
lishi
ng a
foun
datio
n of
evi
denc
e fo
ran
y cl
inic
al is
sue.
http
://w
ww
.ahr
q.go
v/qu
al/
erro
rsix
.htm
Age
ncy
for H
ealth
care
Res
earc
h an
d Q
ualit
y (A
HR
Q)
Acc
esse
d:D
ecem
ber 9
,200
8
http
://w
ww
.ahr
q.go
v/ab
out/
nurs
ing
Age
ncy
for H
ealth
care
Res
earc
h an
dQ
ualit
y (A
HR
Q)
Acc
esse
d:D
ecem
ber 9
,200
8
(con
tinu
es)
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 313
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

314 Chapter 9 Patient Safety: Preventing Unintended Consequences and Reducing Errors
Tab
le 9
-6(c
on
tin
ued
)
Web
Sit
eCo
nten
tsCN
S B
enef
its
Cas
e st
udie
s are
pre
sent
ed fr
om se
vera
l dis
ci-
plin
es,w
ith re
view
s by
cont
ent e
xper
ts in
that
disc
iplin
e
Ext
ensi
ve W
eb si
te,s
pons
ored
by
the
Vet
eran
’sA
dmin
istr
atio
n,de
sign
ed fo
r pat
ient
s and
staf
f:
•C
ultu
re c
hang
e•
Patie
nt sa
fety
for p
atie
nts
•A
lert
s and
adv
isor
y ex
ampl
e:pa
per o
n an
ti-co
agul
atio
n vu
lner
abili
ty•
FME
A (f
ailu
re m
ode
and
effe
cts
anal
ysis
)/R
CA
(roo
t cau
se a
naly
sis)
pro
cess
:E
xten
sive
dis
cuss
ion
on F
ME
A a
s it r
elat
esto
hea
lth c
are
•P
ublic
atio
ns in
clud
e “To
pics
in P
atie
nt S
afet
y”•
Patie
nt sa
fety
reso
urce
s,in
clud
ing
info
rma-
tion
on th
e Pa
tient
Saf
ety
Rep
ortin
g Sy
stem
(PSR
S) a
nd h
uman
fact
ors r
esou
rces
•T
oolk
its o
n fa
lls,h
and
hygi
ene,
and
ensu
ring
corr
ect p
atie
nt su
rger
y
Cas
e ex
ampl
es m
ay b
e us
ed to
rein
-fo
rce
the
impo
rtan
ce o
f the
NP
GS.
Rec
ent s
elec
t cas
es il
lust
rate
mis
take
nid
entit
y an
d a
case
of t
rans
ition
failu
re.
Thi
s Web
site
con
tain
s vol
umes
of
use
ful i
nfor
mat
ion
the
CN
S m
ay u
se to
add
ress
the
patie
ntsa
fety
cul
ture
with
in th
e pr
actic
een
viro
nmen
t:•
PSA
T•
Use
of t
he R
CA
pro
cess
to e
valu
ate
fact
ors i
nvol
ved
in a
n er
ror
•H
and
hygi
ene
prog
ram
•Fa
lls p
reve
ntio
n pr
ogra
m•
Patie
nt sa
fety
wor
ksho
p cu
rric
ulum
http
://w
ww
.web
mm
.ahr
q.go
vA
HR
Q M
&M
:Mor
bidi
ty a
ndM
orta
lity
Rou
nds o
n th
e Web
Acc
esse
d:D
ecem
ber 9
,200
8
http
://w
ww
.pat
ient
safe
ty.g
ovN
atio
nal C
ente
r for
Pat
ient
Saf
ety
Acc
esse
d:D
ecem
ber 9
,200
8
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 314
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

Tools of the Trade 315Ta
ble
9-6
(co
nti
nu
ed)
Web
Sit
eCo
nten
tsCN
S B
enef
its
•Pa
tient
Saf
ety
Ass
essm
ent T
ool (
PSA
T)
that
exa
min
es si
x el
emen
ts o
f pat
ient
safe
ty:
man
agem
ent a
nd le
ader
ship
,pat
ient
safe
tym
anag
emen
t pro
gram
,Joi
nt C
om-
mis
sion
com
plia
nce,
proc
urem
ent a
nd e
quip
-m
ent m
anag
emen
t,re
calls
and
VA
ale
rts/
ad-
viso
ries
,pat
ient
safe
ty p
olic
ies,
tool
s,an
d ai
ds
Prod
uct r
ecal
lsPr
oduc
t saf
ety
New
s for
hea
lth e
duca
tors
and
stud
ents
Onl
ine
data
base
s:M
aude
,MD
R (m
edic
al d
evic
e re
port
ing)
,M
edw
atch
Haz
ard
sum
mar
ies:
e.g.
,ant
icoa
gula
tion
vuln
erab
ility
Gui
delin
es fo
r com
plet
ing
a he
alth
care
failu
rem
odes
and
eff
ect a
naly
sis
Gui
delin
es fo
r ens
urin
g co
rrec
t sur
gery
The
CN
S pl
ays a
key
role
in p
rod-
uct s
elec
tion
and
eval
uatio
n of
new
prod
ucts
.Whe
n th
e C
NS
has b
een
aske
d to
run
a tr
ial o
f a p
artic
ular
piec
e of
tech
nolo
gy o
r equ
ipm
ent,
the
FDA
dat
abas
e ca
n pr
ovid
e in
-fo
rmat
ion
on w
heth
er th
at p
artic
u-la
r tec
hnol
ogy/
bran
d ha
s bee
nre
port
ed to
the
FDA
as h
avin
g be
endy
sfun
ctio
nal o
r cau
sed
inju
ry to
apa
tient
or s
taff
mem
ber.
In le
adin
g an
initi
ativ
e on
han
dhy
gien
e,th
is W
eb si
te h
as a
Pow
er-
Poin
t pre
sent
atio
n,po
ster
s,ot
her
med
ia m
ater
ials
,and
num
erou
s
http
://w
ww
.fda.
gov
Food
and
Dru
g A
dmin
istra
tion
(FD
A)
Acc
esse
d:D
ecem
ber 9
,200
8
http
://w
ww
.va.
gov/
ncps
/sa
fety
topi
cs.h
tml
Nat
iona
l Cen
ter f
or P
atie
nt S
afet
y(N
CPS
)A
cces
sed:
Dec
embe
r 9,2
008
(con
tinu
es)
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 315
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

316 Chapter 9 Patient Safety: Preventing Unintended Consequences and Reducing Errors
Tab
le 9
-6(c
on
tin
ued
)
Web
Sit
eCo
nten
tsCN
S B
enef
its
Falls
tool
kit
An
exte
nsiv
e ha
nd h
ygie
ne p
rogr
amPa
tient
Saf
ety
Ass
essm
ent T
ool
AH
RQ
and
Am
eric
an M
edic
al A
ssoc
iatio
nna
tiona
l gui
delin
es c
lear
ing
hous
e
tool
s for
the
CN
S to
use
in th
is in
i-tia
tive,
from
cal
cula
ting
the
amou
ntof
wat
erle
ss so
ap to
the
time
it ta
kes
to c
lean
han
ds w
ith th
e w
ater
less
soap
.
CN
Ss c
halle
nged
with
a n
ew p
a-tie
nt p
opul
atio
n sh
ould
star
t by
goin
g to
the
evid
ence
to se
e w
hat
has a
lread
y be
en p
ublis
hed.
Gui
de-
lines
on
this
site
are
evi
denc
e ba
sed.
http
://w
ww
.gui
delin
es.g
ovA
HR
Q a
nd A
mer
ican
Med
ical
Asso
ciati
onA
cces
sed:
Dec
embe
r 9,2
008
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 316
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

Tools of the Trade 317Ta
ble
9-7
EXA
MP
LES
OF
WEB
SIT
ES W
ITH
PSI
:REG
ULA
TOR
Y A
GEN
CIE
S
Web
Sit
eCo
nten
tsCN
S B
enef
its
http
://w
ww
.ccf
orpa
tient
safe
ty.o
rgW
HO
Col
labo
rati
ng C
entr
e for
Pa
tien
t Saf
ety
Solu
tion
sA
cces
sed:
Dec
embe
r 9,2
008
Patie
nt S
afet
y Pr
actic
esR
esou
rces
,pat
ient
safe
ty to
ols,
case
s stu
dies
•T
ools
/res
ourc
es in
clud
ing
a lin
k to
app
roxi
-m
atel
y 40
pat
ient
safe
ty W
eb si
tes
•A
war
ds
•C
ase
stud
ies
•Pa
tient
safe
ty g
ood
prac
tices
•A
rtic
les/
new
slet
ter
Faci
litat
es fi
ndin
g pa
tient
safe
ty g
oals
and
prac
tices
by
usin
g dr
op-d
own
men
us•
Cau
ses o
f adv
erse
eve
nts/
type
s of e
vent
s•
U.S
.nat
iona
l pat
ient
safe
ty g
oals
/in
tern
atio
nal p
atie
nt sa
fety
goa
lsPa
tient
safe
ty li
nk,n
ewsl
ette
rL
inks
to p
atie
nt sa
fety
pra
ctic
es,p
rodu
cts a
ndse
rvic
es,a
nd re
sour
ces.
Arc
hive
s ava
ilabl
eon
line
Off
icia
l new
slet
ter:
Col
labo
rati
ons
(qua
rter
ly;e
lect
roni
c)
The
CN
S ob
serv
es th
at th
e cu
lture
of sa
fety
is n
ot in
grai
ned
in th
epr
actic
e ar
ea.T
here
is a
sam
ple
out-
line
for a
pat
ient
safe
ty p
rogr
am.
In in
vest
igat
ing
a se
ntin
el e
vent
via
the
root
cau
se a
naly
sis m
echa
nism
,th
is si
te w
alks
the
CN
S th
roug
h th
eca
uses
of a
dver
se e
vent
s and
type
sof
adv
erse
eve
nts t
hat m
ight
be
unco
vere
d.So
lutio
n se
ts fo
r loo
k-al
ike,
soun
d-al
ike
med
icat
ion
nam
es,p
atie
ntid
entif
icat
ion,
com
mun
icat
ion
dur-
ing
hand
-off
s,an
d pe
rfor
man
ce o
fco
rrec
t pro
cedu
re a
t cor
rect
bod
ysi
te.
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 317
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

318 Chapter 9 Patient Safety: Preventing Unintended Consequences and Reducing Errors
Tab
le 9
-8EX
AM
PLE
S O
F W
EB S
ITES
FO
R E
VID
ENC
E-B
ASE
D P
RA
CTI
CE
Web
Sit
eCo
nten
tsCN
S B
enef
its
http
://w
ww
.ohs
u.ed
u/ep
cO
rego
n E
vide
nced
-Bas
ed P
ract
ice C
ente
rA
cces
sed:
Dec
embe
r 9,2
008
http
://w
ww
.joan
nabr
iggs
.edu
.au/
abou
t/ho
me.
php
Joan
na B
rigg
s Ins
titu
teA
cces
sed:
Dec
embe
r 9,2
008
OH
SU is
an
evid
ence
d-ba
sed
prac
tice
cent
erth
at c
ondu
cts s
yste
mat
ic re
view
of h
ealth
care
topi
cs fo
r fed
eral
and
stat
e ag
enci
es a
nd p
riva
tefo
unda
tions
.The
se re
view
s rep
ort t
he e
vide
nce
from
clin
ical
rese
arch
stud
ies a
nd th
e qu
alit
y of
that
evi
denc
e fo
r use
by
polic
y m
aker
s in
deci
-si
ons o
n gu
idel
ines
Inte
rnat
iona
l Res
earc
h an
d D
evel
opm
ent U
nit,
whi
ch p
rovi
des a
col
labo
rativ
e ap
proa
ch to
the
eval
uatio
n of
evi
denc
e de
rive
d fr
om a
div
erse
rang
e of
sour
ces,
incl
udin
g ex
peri
ence
,exp
er-
tise,
and
all f
orm
s of r
igor
ous r
esea
rch
The
CN
S is
the
lead
er in
the
intr
o-du
ctio
n of
the
conc
epts
of e
vide
nced
-ba
sed
prac
tice.
Eith
er o
f the
se W
ebsi
tes p
rovi
des g
uida
nce
on “w
here
tost
art”
in in
trod
ucin
g ev
iden
ce-b
ased
prac
tice
at th
e be
dsid
e.
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 318
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

Educating New and Experienced Nurses:Electronic Resources for the CNSPatient safety as a discipline is a relatively new phenomenon. Many nurses, as well asother healthcare providers, did not explore the science of safety and error reduction orthe relationship of culture to patient safety during formal nursing education experi-ences. Nurses may be inclined to consider patient safety as closely aligned with thetraditional five rights of medication administration. These five “rights” include rightpatient, right drug, right dose, right route, and right time. Many nurses will recalllearning these rights by rote as students, and new orientees were often drilled aboutthese rules during clinical experiences involving medication or treatment deliveries.Nurses may continue to view these five rights as the gold standard of error prevention;however, these five rights are best viewed as the desired outcomes of safe medicationpractices (Federico, 2007).They do not offer strategies for nurses interested in achiev-ing these goals other than a rather bewildering perception that error is the result of in-dividual performance and good nurses do not make mistakes (Federico, 2007). Giventhat nurses do not come to work intending to commit errors, opportunities for errorand accident reduction must be more broadly based than relying on drilled processes.
CNSs interested in using creative, evidence-based resources for educating new-to-practice nurses as well as more experienced staff without much formal exposure tohealth safety and quality topics will appreciate the opportunities available throughQuality and Safety Education for Nurses (2007), a comprehensive resource funded bythe Robert Wood Johnson Foundation (see Exemplar 9-2).
Educating New and Experienced Nurses: Electronic Resources for the CNS 319
Exemplar 9-2
Promoting Safety by Influencing New-to-Practice NursesGeralyn Altmiller, EdD, MSN, APRN
Quality improvement and patient safety initiatives are much broader and more evidence-based than suggested by simplistic and systematized rules historically emphasized in basicnursing education. Recognizing the need for change, the Robert Wood Johnson Founda-tion spawned a national movement to change the way that nurses are prepared for patientcare delivery by funding the Quality and Safety in Nursing Education (QSEN) grantthrough the University of North Carolina, Chapel Hill (2005). The grant provided 15pilot schools across the nation with the opportunity to integrate practices for quality im-provement and patient safety standards into their nursing curricula. As this national move-ment to improve preparation in prelicensure education of all nurses grows, recentlygraduated nurses are entering the workforce with varying degrees of competency in ad-dressing patient safety concerns.
The CNS has a particularly important role in bridging the gap between prelicensurenursing education and the first work position of new-to-practice nurses. Providing re-
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 319
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

320 Chapter 9 Patient Safety: Preventing Unintended Consequences and Reducing Errors
sources and opportunities that connect practitioners to nationally accepted standards andby supporting and developing safety initiatives, CNSs model the transformation of nurs-ing practice into a higher quality, safer endeavor.
The Institute for Healthcare Improvement (IHI) Web site (n.d.) contains a wealth ofresources to assist the CNS as she or he supports those new to the profession of nursing.One such resource is Transforming Care at the Bedside (TCAB) (IHI, 2003), an initiativedeveloped to connect nursing education to the vision of improving bedside care for thepatient. Using the easily downloadable TCAB storyboard (IHI, 2008b), the CNS canconnect the newly graduated nurse to the new skill sets being implemented across the na-tion to provide patient-centered care. The storyboard promotes personal accountabilityand situational awareness as tools to avoid codes, reduce readmission rates, prevent falls,and improve patient satisfaction.
At the same Web site, CNSs may access the 5 Million Lives Campaign (IHI, 2008a).This initiative works toward preventing 5 million incidents of medical harm by askinghealthcare institutions to adhere to 12 safety-focused interventions. By clicking the Ma-terials tab, the CNS has access to free slide presentations that demonstrate strategies forimplementing the 12 interventions, along with blueprints for educational presentations tostaff, updates on the latest prevention interventions, and related articles.
An important role of the CNS is to introduce the new language of safety and qualitycare improvement to the new-to-practice nurse or to the uninitiated seasoned profes-sional. Value-added nursing care, which is the care that directly contributes to an improvedoutcome for the patient (such as rounding on the unit), or workarounds, the term thatidentifies routes to circumvent the established work system (obtaining meds from anotherpatient’s drawer rather than the pharmacy), may be terms more commonly used in thework environment but missing from some aspects of nursing education at present, therebycreating a communication barrier for the new graduate RN. To bridge that gap, theAgency for Healthcare Research and Quality (AHRQ) provides a Glossary (n.d.) of cur-rent terms as a resource on its Web site.
Many times new-to-practice nurses are uncomfortable communicating with othermembers of the healthcare team, particularly when they believe a patient concern is notbeing attended to. Improving communication skills can be facilitated by the CNS usinghelpful tools available through the AHRQ such as TeamSTEPPS (AHRQ, 2005). TheTeamSTEPPS site contains free slide show downloads for presentations as well as shortvignettes in high-resolution video that are designed to familiarize healthcare workers withcurrent trends in communication techniques and risk-reduction practices. On the Website, there are many examples of safe communication practices that can be used to increasethe attention of other healthcare team members such as CUS (I’m Concerned, Uncom-fortable, Safety) or DESC (Describe the situation, Express feelings about the situation,Suggest other alternative actions, Consequences of current actions are stated).
The Joint Commission is an organization that is frequently discussed in healthcare set-tings but many new-to-practice nurses do not have a clear understanding of what the JointCommission does or how it functions within the healthcare setting. It is a national organ-ization that accredits healthcare facilities. In doing so, hospitals are graded based on theirability to demonstrate that they follow the standards set by the Joint Commission to main-tain a highly reliable practice setting. Not only does this accreditation assure the public
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 320
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

Educating New and Experienced Nurses: Electronic Resources for the CNS 321
that the hospital is meeting standards, but it provides a measure that insurance companiesuse to determine their willingness to refer members to that facility. The CNS promotescompliance of the standards when she or he helps staff members understand the value ofaccreditation and the pivotal role of nurses in the process.
Familiarizing new-to-practice nurses with the Joint Commission Web site (n.d.) pro-motes a sense of personal accountability for system improvement to ensure patient safety.The Patient Safety tab provides concrete information regarding the current National Pa-tient Safety Goals, abbreviations that are not acceptable due to high error potential, andextensive materials that can be used to demonstrate and promote patient safety practices.The Sentinel Event tab provides a root cause analysis framework that presents a step-by-step walk through the process. Using this resource, the CNS demonstrates to the new graduate that there are usually multiple factors that contribute to error. The rootcause analysis specifically identifies those factors and frequently reveals that error is at-tributed to systems failure. The CNS empowers the new-to-practice nurse when that in-dividual recognizes that reporting an adverse event can lead to quality improvementbecause only then can the root cause be identified and the system or process be correctedto reduce risk.
In addition, the Joint Commission Sentinel Event tab highlights current alerts. Mostnotable is the alert that workplace intimidation and aggression is a threat to patient safety.The Joint Commission has mandated that all healthcare systems address hostile work en-vironment behavior by January 2009 as a risk-reduction strategy. Many times, new-to-practice nurses are the most vulnerable to intimidation by peers in the workplace as theyhave known knowledge deficits. Intimidation interferes with their acquisition of knowl-edge and skill development. Cognitive rehearsal of shielding responses (Griffin, 2004) hasbeen an effective strategy that the CNS can teach new-to-practice nurses. It enables themto recognize that the intimidating behavior is a result of stress and frustration and not apersonal affront, thereby allowing the new graduate to respond in an intellectual mannerrather than respond emotionally.
The unfolding case study is a learning strategy that has been promoted by QSEN(2007) to increase critical thinking in undergraduate nursing education.This approach canbe used by the CNS to promote critical thinking in new-to-practice nurses by stimulatingreal-world decision making. The CNS can access descriptions of actual workplace adverseevents on the AHRQ’s Patient Safety Network (n.d.) by clicking the Patient SafetyPrimers tab. Based on these descriptions, the CNS can develop unfolding case scenariosthat cultivate critical thinking and decision-making skills. The CNS can utilize the un-folding case study method as a strategy to inform new-to-practice nurses of the availableresources at the institution that should be utilized to achieve a positive outcome for pa-tients in similar situations.
Lastly, the CNS functions as a bridge between research and practice. Many new-to-practice nurses have a familiarity with evidence-based practice but are not sure how it isimplemented in the clinical setting.The Cochrane Collaboration (n.d.) is an internationaldatabase that the CNS can access to retrieve the latest information regarding appropriateinterventions. AHRQ’s National Guideline Clearinghouse (2008) provides recommenda-tions and rating schemes of the strength of evidence for specific diseases and health prob-
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 321
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

322 Chapter 9 Patient Safety: Preventing Unintended Consequences and Reducing Errors
lems. The CNS can promote the use of these sites with new-to-practice nurses as a meansto determine the appropriate care required for their patients.
There are many resources available to the CNS working with new-to-practice nursesthat will support a smooth transition from the prelicensure educational setting to the workenvironment.The CNS needs to recognize the significant role he or she plays in the trans-formation that occurs when a nurse enters the workforce and is confronted with the chal-lenges to provide high-quality, safe patient care in a rapid-paced, constantly evolvingprofession. A toolkit of resources (see Table 9-9) is an invaluable asset.
Table 9-9 TOOLKIT OF INTERNET RESOURCES FOR THE CNS WORKING WITH NEW-TO-PRACTICE NURSES
Resource Web Site Address
AHRQ: GlossaryAHRQ: National Guideline ClearinghouseAHRQ: Patient Safety NetworkAHRQ: TeamSTEPPS
The Cochrane CollaborationIHI: Transforming Care at the Bedside
IHI: Transforming Care at the Bedside Storyboard
IHI: 5 Million Lives Campaign
QSEN Teaching Strategies
The Joint Commission
http://www.webmm.ahrq.gov/glossary.aspxhttp://www.guideline.gov/compare/synthesis.aspxhttp://psnet.ahrq.govhttp://dodpatientsafety.usuhs.mil/index.php?name=News&file=article&sid=31http://www.cochrane.orghttp://www.ihi.org/IHI/Programs/StrategicInitiatives/TransformingCareAtTheBedside.htmhttp://www.ihi.org/NR/rdonlyres/F81270CD-B8BC-47D5-B2A6-BDA550096AA9/4252/TCABStoryboardFall2006FINAL.pdfhttp://www.ihi.org/IHI/Programs/Campaignhttp://qsen.org/teachingstrategies/search_strategies#resultshttp://www.jointcommission.org
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 322
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

Case Study: Development and Implementationof a Rapid Response Team
The majority of hospitalized patients experience antecedent physiologic abnormali-ties prior to cardiopulmonary arrests. When these abnormalities occur outside an in-tensive care unit, they are often unrecognized or are not responded to in a timely,appropriate manner by the hospital care team. This may be partially due to a reducedawareness of the importance of these physiologic abnormalities in the spectrum ofdisease or perhaps due to competing clinical responsibilities on the part of the physi-cian or nurse practitioner. This scenario becomes increasingly complex in academicmedical centers, as the most junior-level physicians typically perform the triage, clin-ical management, and communication around these critical events.
A rapid response team (or medical emergency team) is a team of critical care clini-cians who can respond to the bedside of a deteriorating patient before a catastrophicevent (e.g., cardiac or respiratory arrest) occurs. The goal of the team is to reduce thenumber of cardiac arrests and unanticipated intubations outside the ICU throughclinical staff members’ heightened awareness to signs of physiologic deterioration andthrough the development of a mobile team that can provide immediate critical care tothe bedside.
The IHI Save 100,000 Lives campaign had designated the development of a rapidresponse team as one of the six interventions to decrease unanticipated mortality. Thesubsequent 5 Million Lives campaign, launched in December 2006, continues to ad-vocate for rapid response teams and the other five original interventions while alsoadding new interventions selected to reduce harm (IHI, 2008a). IHI provides manyuseful, effective, and cost-efficient resources for CNSs interested in beginning pro-grams designed to improve healthcare safety. It is an “absolute must” Web site thatshould be easily accessible to CNSs and professional staff.
Kleinpell and Gawlinski (2005) have developed a nine-step process to guide theCNS in planning and implementing an outcomes-driven initiative. Table 9-10 de-scribes an example of a process to establish a rapid response team, one of the recom-mendations of the IHI Save 100,000 Lives campaign and continued with the 5 Million Lives campaign. The model can be used to develop other safety-relatedinterventions, such as programs to decrease central line infections and ventilator-associated pneumonia (IHI, 2008b).
Skill breadth, competence, and familiarity with multiple roles uniquely positionsthe CNS to play a pivotal role in patient safety. The CNS is able to integrate knowl-edge of patient safety with evidence-based practice to improve outcomes (Phillips,2005). The role of the CNS in patient safety will continue to expand exponentially;thus, the introduction of the CNS into the world of patient safety is just the begin-ning of a successful journey toward creating a culture of safety, integrated withevidenced-based practice to produce the highest quality of care possible.
Case Study: Development and Implementation of a Rapid Response Team 323
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 323
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

324 Chapter 9 Patient Safety: Preventing Unintended Consequences and Reducing Errors
Tab
le 9
-10
DEV
ELO
PIN
G A
RA
PID
RES
PO
NSE
TEA
M
Step
s in
the
Pro
cess
Inte
rven
tion
s
Fin
d/Id
enti
fy o
utco
me
vari
able
s tha
tth
e C
NS
can
impa
ct.
CN
S Sk
ills/
Rol
es:
Col
labo
rato
r,cl
inic
al le
ader
,res
earc
h(H
amri
c,19
89)
Org
aniz
e a
team
:Who
are
the
key
stak
ehol
ders
?C
NS
Skill
s:C
hang
e ag
ent,
colla
bora
tor,
role
mod
el(H
amri
c,19
89)
Cla
rify
cur
rent
kno
wle
dge
of th
epr
acti
ce is
sue
to b
e re
solv
ed.
CN
S Sk
ills/
Rol
es:
Res
earc
h,co
llabo
rato
r,pa
tient
advo
cate
,cha
nge
agen
t(H
amri
c,19
89)
1.D
ecre
ase
code
s/ai
rway
em
erge
ncie
s out
side
the
ICU
.2.
Dec
reas
e un
plan
ned
tran
sfer
s to
the
ICU
.3.
Impr
ove
nurs
e/ca
regi
ver s
atis
fact
ion
by p
rovi
ding
a su
ppor
t sys
tem
for t
hest
aff t
o ca
ll w
hen
thei
r pat
ient
is in
dis
tres
s.
1.E
ngag
e se
nior
lead
ersh
ip:p
hysi
cian
s,nu
rsin
g,ad
min
istr
atio
n.2.
Oth
er st
akeh
olde
rs:n
ursi
ng,h
ouse
staf
f and
trai
ning
dire
ctor
s,re
spir
ator
yth
erap
y,ph
arm
acy.
1.Pr
epar
atio
n ph
ase
incl
udes
acc
urat
e co
llect
ion
of b
asel
ine
leve
ls o
f ser
ious
adve
rse
even
ts a
nd c
ardi
ac a
rres
ts.
2.W
hat p
erce
nt o
f cod
es o
r air
way
em
erge
ncie
s occ
ur o
utsi
de th
e IC
U?
3.W
hat p
erce
nt o
f cod
es o
r air
way
em
erge
ncie
s are
acc
ompa
nied
by
clin
ical
ante
cede
nts?
4.W
ere
the
clin
ical
ant
eced
ents
reco
gniz
ed?
5.W
hat i
s the
und
erst
andi
ng o
f the
staf
f of e
arly
det
ectio
n of
phy
siol
ogic
dete
rior
atio
n?6.
Wha
t com
mun
icat
ion
stra
tegi
es a
re u
tiliz
ed to
acc
urat
ely
and
conc
isel
y ge
tth
e m
essa
ge a
cros
s?7.
SBA
R (s
ituat
ion,
back
grou
nd,a
sses
smen
t,re
com
men
datio
n).
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 324
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

Case Study: Development and Implementation of a Rapid Response Team 325Ta
ble
9-1
0(c
on
tin
ued
)
Step
s in
the
Pro
cess
Inte
rven
tion
s
Und
erst
and
sour
ces o
f var
iati
on.
CN
S Sk
ills/
Rol
es:
Res
earc
h,co
nsul
tant
,edu
cato
r,pa
tient
advo
cate
(Ham
ric,
1989
)
Sele
ct p
ract
ices
and
stra
tegi
es fo
rim
prov
emen
t.C
NS
Skill
s/R
oles
:C
linic
al le
ader
,edu
cato
r,ch
ange
age
nt(H
amri
c,19
89)
Pla
n fo
r im
plem
enta
tion
.C
NS
Skill
s/R
oles
:C
linic
al le
ader
,rol
e m
odel
,edu
cato
r,co
nsul
tant
(Ham
ric,
1989
)
1.W
hen
clin
ical
det
erio
ratio
n is
reco
gniz
ed,h
ow is
that
clin
ical
pre
sent
atio
nre
spon
ded
to b
y th
e nu
rse?
Hou
se st
aff?
2.W
hat b
arri
ers p
reve
nt th
e be
dsid
e pr
actit
ione
r fro
m c
allin
g fo
r hel
p (c
allin
gth
e at
tend
ing
phys
icia
n) w
hen
his o
r her
gut
inst
inct
sugg
ests
it is
the
righ
tth
ing
to d
o?
1.E
stab
lish
a tr
igge
r too
l to
prov
ide
the
staf
f with
a c
oncr
ete
refe
renc
e fo
r whe
nto
cal
l the
team
.Inc
lude
at l
east
one
cav
eat t
hat r
elat
es to
that
“gut
feel
ing.
”2.
Des
ign
the
team
bas
ed o
n cu
rren
tly a
vaila
ble
pers
onne
l.T
eam
con
stru
ctio
nva
ries
from
hos
pita
l to
hosp
ital.
Tea
ms a
re a
s sim
ple
as th
e IC
U c
harg
e nu
rse
and
resp
irat
ory
ther
apis
t to
as c
ompl
ex a
s an
eigh
t-m
embe
r tea
m le
d by
an
inte
nsiv
ist.
3.D
evel
op p
roto
cols
for p
ract
ice
if ne
eded
.4.
Def
ine
team
role
dur
ing
activ
atio
n.5.
Prov
ide
team
lead
ersh
ip.
6.A
sses
s,in
terv
ene,
stab
ilize
,arb
itrat
e to
app
ropr
iate
leve
l of c
are.
7.C
omm
unic
ate,
com
mun
icat
e,co
mm
unic
ate!
8.E
stab
lish
a fe
edba
ck m
echa
nism
for t
he re
spon
se te
am to
feed
back
info
rma-
tion
to th
e te
ams t
hat m
ade
the
calls
.
1.D
evel
op e
duca
tiona
l cur
ricu
lum
.2.
Bed
side
pra
ctiti
oner
s.3.
Res
pond
ing
team
.
(con
tinu
es)
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 325
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

326 Chapter 9 Patient Safety: Preventing Unintended Consequences and Reducing Errors
Tab
le 9
-10
(co
nti
nu
ed)
Step
s in
the
Pro
cess
Inte
rven
tion
s
Pla
n fo
r im
plem
enta
tion
.(c
ontin
ued)
Do
the
inte
rven
tion
s acc
ordi
ng to
the
plan
.C
NS
Skill
s/R
oles
:R
esea
rch,
educ
atio
n,ch
ange
age
nt,r
ole
mod
el,e
xper
t pra
ctiti
oner
(Ham
ric,
1989
)
4.P
hysi
cian
s,nu
rses
,the
rapi
sts,
tech
nici
ans,
virt
ually
any
one
who
com
es in
cont
act w
ith th
e pa
tient
,pag
e op
erat
ors.
5.D
ata
man
agem
ent.
6.D
ocum
enta
tion
whi
le o
n th
e sc
ene.
7.W
hy te
am w
as c
alle
d,w
ho c
alle
d,in
terv
entio
ns,o
utco
mes
,com
mun
icat
ion
with
att
endi
ng p
hysi
cian
.8.
Log
and
ana
lyze
cal
ls a
nd “m
isse
d op
port
uniti
es.”
9.P
ublic
rela
tions
(nee
d at
leas
t fiv
e ve
nues
to g
et th
e w
ord
out)
.10
.Po
ster
s,fly
ers.
11.
Gra
nd ro
unds
for n
ursi
ng,m
edic
ine,
any
depa
rtm
ent.
12.
Pres
ent a
t dep
artm
enta
l mee
tings
.13
.D
iscu
ss a
t uni
t-ba
sed
mee
tings
.14
.“R
oads
how
,”or
trav
elin
g in
serv
ice,
brin
ging
the
info
rmat
ion
to th
e st
aff o
n th
eflo
ors.
1.O
pera
tiona
lize
team
as p
lann
ed.
2.P
hase
I or
pilo
t for
a d
efin
ed p
erio
d of
tim
e.3.
Ana
lyze
eac
h ca
ll to
iden
tify
area
s of o
ppor
tuni
ty.
4.C
linic
al re
view
:Why
wer
e ca
lls p
lace
d? W
hat h
appe
ned
at th
e be
dsid
e?5.
Ope
ratio
nal r
evie
w:D
id e
very
thin
g go
as p
lann
ed? D
id th
e te
am sh
ow u
p?
Did
the
equi
pmen
t wor
k? D
id y
ou n
eed
som
ethi
ng th
at y
ou d
idn’
t hav
e?
Did
you
nee
d so
meo
ne w
ho w
as n
ot a
vaila
ble?
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 326
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

Sour
ce:K
lein
pell
and
Gaw
linsk
i,20
05;P
hilli
ps,2
005.
Case Study: Development and Implementation of a Rapid Response Team 327Ta
ble
9-1
0(c
on
tin
ued
)
Step
s in
the
Pro
cess
Inte
rven
tion
s
Che
ck/a
naly
ze/r
evie
w d
ata
CN
S Sk
ills/
Rol
es:
Col
labo
rato
r,re
sear
cher
(Ham
ric,
1989
)
Put
impr
ovem
ent i
nto
effe
ct,h
old
gain
s,an
d es
tabl
ish
less
ons l
earn
ed.
CN
S Sk
ills/
Rol
es:
Cha
nge
agen
t,co
llabo
rato
r,cl
inic
alle
ader
,rol
e m
odel
,pat
ient
adv
ocat
e(H
amri
c,19
89)
1.R
evie
w d
ata
from
eac
h ev
ent f
or c
linic
al a
nd o
pera
tiona
l eff
icie
ncie
s.2.
Com
pare
pre
inte
rven
tion/
post
inte
rven
tion
data
for c
hang
es in
rate
s of c
odes
outs
ide
the
ICU
,una
ntic
ipat
ed tr
ansf
ers t
o th
e IC
U,a
nd u
nant
icip
ated
mor
talit
y.
1.E
valu
ate
proc
ess a
nd m
ake
appr
opri
ate
chan
ges t
o tr
igge
r too
l,do
cum
enta
-tio
n to
ol,t
eam
not
ifica
tion
proc
ess,
or te
am a
ctiv
ities
at t
he b
edsi
de.
2.C
ontin
ue to
revi
ew d
ata
to e
stab
lish
succ
ess o
f pro
gram
.3.
Invo
lve
staf
f in
satis
fact
ion
surv
ey to
asc
erta
in th
e ef
fect
on
nurs
ing
satis
fact
ion.
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 327
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

328 Chapter 9 Patient Safety: Preventing Unintended Consequences and Reducing Errors
ReferencesAmerican Association of Critical-Care Nurses (AACN). (2002). Scope of practice and stan-
dards of professional performance for the acute and critical care clinical nurse specialist. AlisoViejo, CA: Author.
American Association of Critical-Care Nurses (AACN). (2005). AACN standards for es-tablishing and sustaining healthy work environments. A journey to excellence. Retrieved July7, 2006, from http://www.aacn.org/aacn/pubpolcy.nsf/Files/HWEStandards/$file/HWEStandards.pdf
Agency for Health Research and Quality (AHRQ). (2001). Patient safety practices: Prac-tices rated by strength of evidence. In Making health care safer: A critical analysis of pa-tient safety practices (Evidence report/technology assessment Number 43, AHRQPublication No. 01-E058). Retrieved July 23, 2006, from http://ahrq.gov/clinic/ptsafety/pdf/ptsafety.pdf
Agency for Health Research and Quality (AHRQ). (2003) Chapter 2: Efforts to re-duce medical errors: AHRQ’s response to senate committee on appropriations. In Pa-tient safety initiative: Building foundations reducing risk. Retrieved July 23, 2006, fromhttp://www.ahrq.gov/qual/pscongrpt/psini2.htmAgency for Health Research and Quality (AHRQ). (2008a). Appendix B. High reliability
organization learning network operational advice from the Exempla Healthcare site visit. Re-trieved December 8, 2008, from http://www.ahrq.gov/qual/hroadvice/hroadviceapb.pdf
Agency for Health Research and Quality (AHRQ). (2008b). Transforming hospitals intohighly reliable organizations. Retrieved December 8, 2008, from http://www.ahrq.gov/qual/hroadvice/hroadvice1.htm
Agency for Health Research and Quality (AHRQ). (2008c). Patient safety culture surveys.Retrieved December 8, 2008, from http://www.ahrq.gov/qual/hospculture
Aspden, P., Corrigan, J. M., Wolcott, J., & Erickson, S. M. (Eds.). (2004). Committee onData Standards for Patient Safety. Patient safety: Achieving a new standard for care. Wash-ington, DC: National Academies Press.
Barden, C. (Ed). (2005). AACN standards for establishing and sustaining healthy work envi-ronments. Retrieved July 23, 2006, from http://www.aacn.org/aacn/pubpolcy.nsf/Files/HWEStandards/$file/HWEStandards.pdf
Centers for Medicare and Medicaid Services (CMS) and Joint Commission. (2008). Spec-ifications Manual for National Hospital Inpatient Quality Measures Discharges 10-01-08(4Q08) through 03-31-09 (1Q09). Retrieved October 26, 2008, from http://www.jointcommission.org/NR/rdonlyres/304A9AA7-0C23-46F8-A94C-A14C25744690/0/NHQM_v25b_pdf_add76513.zip
Cook, A. F., Hoas, H., Guttmannova, K., & Joyner, J. C. (2004). An error by any othername. American Journal of Nursing, 104, 32–43.
De Rosier, J., & Stalhandske, E. (2006). Veteran’s Administration Center for Patient Safety:Veterans Health Administration: Root cause analysis (RCA). Retrieved July 23, 2006, fromhttp://www.va.gov/ncps/Cogaids/RCA/index.htm#
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 328
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

Duwe, B., Fuchs, B., & Hansen-Flashen, J. (2005). Failure mode and effects analysis ap-plication to critical care medicine. Critical Care Medicine, 21, 21–30.
Federico, F. (2007). The five rights of medication administration.Topics. Medication systems. Im-provement stories. Retrieved November 3, 2008, from http://www.ihi.org/IHI/Topics/PatientSafety/MedicationSystems/ImprovementStories/FiveRightsofMedicationAdministration.htm
Friersen, M. A., Farquhar, M. B., & Hughes, R. G. (2006). The nurse’s role in promoting aculture of patient safety. Center for American Nurses. Retrieved July 23, 2006, fromhttp://www.ana.org/mods/mod780/role.pdf
Hamric, A. B. (1989). History and overview of the clinical nurse specialist. In A. B. Ham-ric & J. B. Spross (Eds.). The clinical nurse specialist in theory and practice. Philadelphia,PA: W. B. Saunders.
HealthGrades. (2006). Third annual patient safety in America study. Retrieved December 8,2008, from http://www.healthgrades.com/media/dms/pdf/patientsafetyinamericanhospitalsstudy2006.pdf
Helmreich, R. (2005). Culture of safety. Risk and quality management strategies: HRC sup-plement A. Retrieved December 8, 2008, from http://www.ecri.org/Documents/Patient_Safety_Center/HRC_CultureofSafety.pdf
Institute for Healthcare Improvement (IHI). (2008a). Protecting 5 million lives from harm PowerPoint. Retrieved December 8, 2008, from http://www.ihi.org/NR/rdonlyres/7AE7044B-C006-4A5F-896E-
Institute for Healthcare Improvement (IHI). (2008b). Protecting 5 million lives from harm.Retrieved December 8, 2008, from http://www.ihi.org/IHI/Programs/Campaign/Campaign.htm?TabId=1
Institute for Safe Medication Practices. (2006). Assess-ERR medication system worksheet.December 8, 2008, from http://www.ismp.org/Tools/AssessERR.pdf
Joint Commission. (2006). National patient safety goals, 2007. Retrieved July 23, 2006,from http://jointcommission.org/Patientsafety/NationalPatientSafetyGoals/07_hap_cah_npsgs.htm
Kleinpell, R., & Gawlinski, A. (2005). Assessing outcomes in advanced practice nursingpractice. AACN Clinical Issues, 16, 43–57.
Kohn, L., Corrigan, J., & Donaldson, M. (Eds.). (2000). To err is human: Building a saferhealth system. Washington, DC: National Academies Press.
Leapfrog Group. (2007). Our mission:The Leapfrog Group mission statement. Retrieved Oc-tober 20, 2008, from http://www.leapfroggroup.org/about_us/our_mission
Leonard, M., Graham, S., & Bonacum, D. (2004). The human factor: The critical impor-tance of effective teamwork and communication in providing safe care. Quality andSafety in Healthcare, 13(Suppl. 1), i85–i90.
National Association of Clinical Nurse Specialists (NACNS). (2004). Statement on clinicalnurse specialist practice and education (2nd ed.). Harrisburg, PA: Author.
References 329
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 329
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

330 Chapter 9 Patient Safety: Preventing Unintended Consequences and Reducing Errors
Oncology Nursing Society. (2003). The role of the advanced practice nurse in oncology care.Retrieved July 24, 2006, from http://www.ons.org/publications/positions/AdvancePractice.shtml
Phillips, J. (2005). Neuroscience CC: The role of the APN in patient safety. AACN Clini-cal Issues, 16, 580–591.
Pronovost, P. J., Thompson, D. A., Holzmueller, C. G., Lubomski, L. H., & Morlock, L.L. (2005). Defining and measuring patient safety. Critical Care Clinics, 21, 1–19.
Quality and Safety Education for Nurses. (2007). Home page. Retrieved November 3,2008, from http://www.qsen.org
Reason, J. (1990). Human error. New York: Cambridge University Press.Sora, J., & Nieva, V. (2003). Safety culture assessment: A tool for improving patient safety
in healthcare organizations. Quality and Safety in Healthcare, 12(Suppl. 2), ii17–ii23.Tucker, A. L., & Edmondson, A. C. (2002). When problem solving prevents organiza-
tional learning. Journal of Organizational Change Management, 15, 122–138.Volker, D. L., & Clark, A. P. (2004). Taking the high road: What should you do when an
adverse event occurs, Part II. Clinical Nurse Specialist, 18, 180–182.White, S. V. (2004). Patient safety issues. In J. Byers & S. White (Eds.), Patient safety:
Principles and practice. New York: Springer.Wolf, Z. (2007). Pursuing safe medication use and the promise of technology. Medical-
Surgical Nursing Journal, 16, 92–100.World Health Organization Collaborating Centre for Patient Safety Solutions. (2008).
About us. Retrieved November 3, 2008, from http://www.ccforpatientsafety.org/31588Zuzelo, P., Gettis, C., Hansell, A., & Thomas, L. (2008). Describing the influence of tech-
nologies on registered nurses’ work. Clinical Nurse Specialist, 22(3), 132–240.
Exemplar 9-2 ReferencesAgency for Healthcare Research and Quality (AHRQ). (2005). TeamSTEPPS. Retrieved
July 9, 2008, from http://dodpatientsafety.usuhs.mil/index.php?name=News&file=article&sid=31
Agency for Healthcare Research and Quality (AHRQ). (2008). National guideline clear-inghouse. Retrieved on July 30, 2008, from http://www.guideline.gov/compare/synthesis.aspx
Agency for Healthcare Research and Quality (AHRQ). (n.d.). Patient safety network. Re-trieved July 30, 2008, from http://psnet.ahrq.gov
Agency for Healthcare Research and Quality (AHRQ). (n.d.) Web M&M: Glossary. Re-trieved July 28, 2008, from http://www.webmm.ahrq.gov/glossary.aspx
Cochrane Collaboration. (n.d). Homepage. Retrieved July 30, 2008, from http://www.cochrane.org
Ebright, P. R. (2004). Understanding nurse work. Clinical Nurse Specialist, 18, 168–170.
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 330
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

Exemplar 9-2 References 331
Griffin, M. (2004). Teaching cognitive rehearsal as a shield for lateral violence: An inter-vention for newly licensed nurses. Journal of Continuing Education in Nursing, 35(6),257–263.
Institute for Healthcare Improvement (IHI). (2003). Transforming care at the bedside. Re-trieved July 8, 2008, from http://www.ihi.org/IHI/Programs/StrategicInitiatives/TransformingCareAtTheBedside.htm
Institute for Healthcare Improvement (IHI). (2006a). 5 Million Lives campaign. RetrievedJuly 30, 2008, from http://www.ihi.org/IHI/Programs/Campaign
Institute for Healthcare Improvement (IHI). (2006b). Transforming care at the bedside sto-ryboard. Retrieved July 8, 2008, from http://www.ihi.org/NR/rdonlyres/F81270CD-B8BC-47D5-B2A6-BDA550096AA9/4252/TCABStoryboardFall2006FINAL.pdf
Institute for Healthcare Improvement. (n.d.). Homepage. Retrieved July 30, 2008, fromhttp://www.ihi.org/ihi
Joint Commission. (n.d.) Homepage. Retrieved July 30, 2008, from http://www.jointcommission.org
Quality and Safety in Nursing Education (QSEN). (2005). Overview. Retrieved July 8,2008, from http://qsen.org/about/overview
Quality and Safety in Nursing Education (QSEN). (2007). Search teaching strategies. Re-trieved July 30, 2008, from http://qsen.org/teachingstrategies/search_strategies#results
61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 331
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.

61141_CH09_291_332.qxd 7/30/09 11:42 AM Page 332
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.



















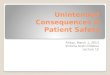

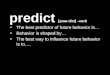





![20110712 Unintended Consequences 12[1].07](https://img.pdfslide.net/doc/110x75/577d278b1a28ab4e1ea429b5/20110712-unintended-consequences-12107.jpg)
