Embed Size (px)
Citation preview

PBL CV 2
Pathophysiology of coronary artery disease

Coronary artery disease (CAD)• Leading cause of death in US• Accounts for half of the nearly 1 million deaths from CVD each year
– Atherosclerosis of the coronary arteries is the major cause of CAD• Although atherothrombosis (intra-coronary thrombosis) also plays a role
• CAD is progressive degenerative disease that begins in childhood and manifests itself in middle to late adulthood as an acute coronary syndrome (ACS)
• In affluent societies, coronary artery disease causes severe disability and more death than any other disease, including cancer.
• It manifests as – angina– silent ischaemia– unstable angina– myocardial infarction– arrhythmias– heart failure– sudden death.

Anatomy of heart and vessels

Cardiac vessels• Heart receives blood through left and right coronary arteries
– Come off as first branches of aorta• Right coronary artery (RCA) gives off acute marginal branches to the RV and in 85% of
people gives off branches to inferior aspect (posterior descending artery [PDA]) and posterior aspect (posterolateral branches) of the LV
• This is referred to as right-dominant circulation• Left main coronary artery is quite short and bifurcates into left anterior descending (LAD)
and left circumflex (LCx) arteries– LAD gives off diagonal branches that supply to the anterior aspect of the LV, and the LCx gives off
obtuse marginal branches that supply the lateral aspect of the LV– In 10% of people, the LCx gives rise to both the posterior descending and posterolateral arteries
(left-dominant circulation)• In 5% of people, the RCA gives rise to the posterior descending artery and the LCx gives rise
to the posterolateral arteries (codominant circulation)• Small collateral vessels interconnect the coronary arteries• THESE COLLATERALS ARE NONFUNCTIONAL IN THE NORMAL SETTING BUT PROVIDE AN
ALTERNATE ROUTE OF BLOOD FLOW IF THE CORONARY ARTERY BECOMES STENOSED.

Atherosclerosis
• Atheroclerosis is a chronic inflammatory and healing response of the arterial wall to endothelial injury. Lesion progression occurs through the interaction of modified lipoproteins, macrophages and T lymphocytes with the normal cellular constituents of the arterial wall

Pathophysiology of atherosclerosisAtherosclerosis occurs through the following events:• Endothelial injury
– Causes increased vascular permeability, leukocyte adhesion and thrombosis
• Accumulation of lipoproteins in the vessel wall– Mainly LDL and its oxidised forms
• Monocyte adhesion to the endothelium– Followed by migration into the intima and transformation into
macrophages and foam cells• Platelet adhesion• Factor release from activated platelets, macrophages and
vascular wall cells inducing smooth muscle cell recruitment• Smooth muscle cell proliferation and ECM production• Lipid accumulation both extracellularly and within cells
(macrophages and smooth muscle cells)

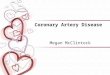
Development of atherosclerosis throughout life

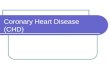
Histology of atherosclerotic plaque
• F – fibrous cap• C – central necrotic lipid core• L – lumen• Arrow points to segment of wall that
is free of plaque– Therefore this plaque is termed
‘eccentric’
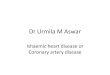
Higher magnification at junction of fibrous cap and core
• Arrowheads point to areas of calcification
• Arrows point to areas of new vascularisation

Progression and outcomes of atherosclerotic plaques
When a plaque produces:• > 50% diameter stenosis or • > 75% reduction in cross sectional areareduced blood flow through the coronary artery during exertion may lead to angina.

Outcomes of plaques• Plaques with a large lipid core and a
relatively thin fibrous cap are more likely to rupture than those with a thick fibrous cap
• Outcomes of plaques are:– aneurysm and ruptur– occlusion of vessel by thrombus– critical stenosis
• It is important to note that the composition of plaques is dynamic – It has been shown that the precipitating
lesion in patients who develop MI or other ACS (acute coronary syndromes) is not necessarily a severely stenotic and haemodynamically significant lesion before its acute change
– This means that an asymptomatic individual with plaques showing only mild to moderate luminal stenosis may have an unpredictable risk of a severe coronary event
A shows plaque rupture without superimposed thrombus, B shows acute coronary thrombosis superimposed on an atherosclerotic plaque with disruption of the fibrous cap leading to MIArrows point to site of plaque rupture

Flow diagram for management of Angina

References
• Robbins and Cottran• BMJ Review article 2003– “ABC of interventional cardiology -Pathophysiology and investigation of coronary artery
disease”• Ever D Grech