Embed Size (px)
DESCRIPTION
Pediatric and Neuromuscular Orthopedics. Objectives. 11%-self-care-comfort -avoid complications Identify signs and symptoms in selected pediatric and neuromuscular disorders. Outline nursing interventions for medical and surgical protocols. - PowerPoint PPT Presentation
Citation preview

Pediatric and
Neuromuscular Orthopedics

Objectives
• 11%-self-care-comfort -avoid complications
• Identify signs and symptoms in selected pediatric and neuromuscular disorders.
• Outline nursing interventions for medical and surgical protocols.
• List strategies to maximize function in patients and families with neuromuscular disorders

Development
• Infancy 0-18 months
• Toddler 18 mos – 3 yrs
• Pre-school 3-5 yrs
• School age 6-12 yrs
• Adolescence 13 –19

Pediatric Differences
• Visualization – ossification – ultrasound – X-ray
• Bone• Thick periosteum• Metaphyseal growth• Re-modeling

Nursing Intervention
• Nursing see Table 11-1 from Core Curriculum 4th ed.
• Child’s developmental level• Parent and child’s ability to learn• Amount disorder interferes with:
– ADLs– Growth– Learning Ability– Social Adjustment

Nursing Intervention
Parents
• Realistic expectations
• Understanding of the disease/disorder
• Follow-up with treatment
• Response to public inquiry

Nursing Intervention
• Team approach – Include child in decisions
• Play – Independence, socialization, – Creativity, problem solving

Upper Extremity Disorders
• Congenital anomalies• Syndactyly webbing 2+
digits • Polydactyly extra digits• Congenital
amputations /deficiencies• Brachial plexus injuries

Lower Extremity Disorders
• DDH• Legg-Calvé-Perthes • Intoeing,
torsional problems• SCFE (presentations)• Limb length inequality• Osteomyelitis, septic
joint• Trauma

Developmental Dislocation of the Hip
• DDH
• F>M 1:500-1000 births
• Breech, 1st born
• Family history

Developmental Dislocation of the Hip
• Physical Exam - hip clicks and clunks
• Barlow’s – push hip out back • Ortolani’s abduct click in • Decreased abduct• Unequal skin folds• Ultrasound - X-ray

DDH Rx
• Pavlik, abd. splint
• Traction Bryant’s/ mod Bryant's
• Surgical reduction closed vs open
• Spica cast

DDH Nursing Care
• Traction
• Neurovascular Exam – Amputation 2° necrosis
• Cast syndrome
• Can be fatal

Talipes Equinovarus
• “Clubbed Foot” 1.24:1000 births
• M 2x > F• Inversion adduction and
equinus of the forefoot• Fixed rigid deformity• Etiology: controversial• Uterine position• Idiopathic

Talipes Equinovarus
• Dx: clinical apparent
• Calf smaller, Achilles short
• Rx:Stretching
• Casting
• Surgical releases

Talipes Equinovarus
• Nursing, watch toes in cast
• Foot will be smaller!
• Rocker bottom from push up on metatarsals
• Can play sports

Intoeing
• Most common complaint!
• Metatarsus adductus
(foot deformity)
• Tibial torsion
• Femoral anteversion

Metatarsus Adductus
• Foot deformity– 1:1000 births– Dx: exam– Rx: stretching
• long leg molded cast
• surgery

Tibial Torsion
• Physiologic bowing of tibia• 2º intrauterine position • NORMAL for toddler• No treatment unless present
at 8 years of age
• Nursing - bring grandparent to appointment

Femoral Anteversion
• Curvature of the femur
• After 3 yrs resolves by 8yrs
• Brace not effective• Osteotomy if
functional problems after 8 yrs

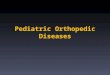
cubitusvarus
coxavalgagenu
varum
heelvarus metatarsus
varus
cubitusvalgus
genuvalgum
halluxvalgus
heelvalgus
coxavara
Va us

Genu Valgus
• Knock knees
• Joint laxity -medial collateral ligs.
• Common: 3 - 5 years
• improves by 7 years
• normal angulation
• girls: 7 - 9° valgus
• boys: 4 - 6° valgus

Genu Varus
• ^ dist between knees >2.5
cm
• W/ ankles together
• external torsion of femur
• improves spontaneously
by 18 - 24 mos
in early amb & heavy
children

Blount’s Disease
• X-ray changes medial prox tibia
• 50% unilat. tibial bowing• ^Black, ^obese, • Rx: no Δ 6 mos bracing• Surgical >30 mos old w/o
Rx or structural / functional deform

Blount’s Disease
• Rx: • Corrective prox.
osteotomy.• Hemiepiphysiodesis• External fixator
– Some with gradual correction

Osteogenesis Imperfecta “OI”
• Brittle bone disease fracture with minimal stress
• Multiple types some fatal
• Etiology: autosomal dominant vs. recessive
• Defect collagen synthesis
• 1:20,000 births

Osteogenesis Imperfecta “OI”
• Dx: Clinical deformities
• Blue sclera, shepherds crook
deformity
• Dentinogenesis, deafness
• Radiographs
• Biopsy
• Bone density

Osteogenesis Imperfecta “OI”• Rx brief Light wt. immob• I-M rods “Bailey” grows
with child• Pamidronate treatment • Pain meds. • “Brittle baby” NO BP’s
signs Don’t pull limbs, • Physical NOT mental
handicap• Encourage independence

Legg Calvé Perthes
• Aseptic necrosis femoral head
• Idiopathic vs heredity
• M 4x >F 1:2000 births
• Age 3-12 years

Legg Calvé Perthes
• Sx: Knee, hip,
thigh pain
• Limp
• Decreased ROM
• Dx: exam / X-ray

Slipped Capital Femoral Epiphysis
Endocrine/ obesity/ growth / trauma
• F 8-15yrs. M 10-17yrs• 1 : 10,000 adolescents • Sx: Hip, knee, pain (long duration)• Limp, decreased ROM• Dx: Hallmark sign- lack of internal
rotation• X-ray -“Ice cream falling off the
cone

Slipped Capital Femoral Epiphysis
• Rx: bedrest, • N W B, crutches • Surgical pinning • Teach S&S for other
hip - >50%

Limb Length Inequality
• Congenital vs acquired
• Sx: short limb, limp, back pain
• Dx: X-ray, CT, bone
age

Limb Length Inequality Rx:
• < 2cm no treatment
• 2-6 cm lifts epiphysiodesis
• >6 - 15cm shorten opposite limb
• Limb lengthening, external fixation

Limb Length Inequality
• Nursing
• Pain management
• Pin care
• Compartment syndrome
• Emotional support

Osgood-Schlatter’s Disease
• F 8-13 yrs M 11-15 yrs
• Sx: painful swelling tibial tubercle
• cosmetic deformity

Osgood-Schlatter’s Disease
• Dx: exam • X-ray traction
apophysitis• Rx: rest, ice,
stretch hamstrings
• Casting

Trauma
• Leading cause of death in children
• Common injuries (see table 11-3 )
• Child abuse – Battered Child Syndrome

Trauma: Child Abuse
• 3.14 million children reported abused
• Physical abuse
• Greatest < 3 years (66-78%)
• 30% under 6 mos

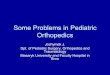
Salter-Harris Classification
1 2 3 4 5

Child Abuse - Fractures
• Most common presentation!
• >30% under 3 mos.
• 70% under 6 mos.(1yr) are inflicted

Common Fractures Inflicted
• Metaphyseal
• Rib Fxs seen in 5-20%
of abused
• Scapular/distal clavicle/ night stick
• Vertebral fx. or subluxation

Common Fractures Inflicted
• Finger Fx. In non-ambulating child
• Humerus Fx. (X supracondylar) < 3 Yrs.
• Bilateral, multiple, or Fxs in different stages of healing
• Complex skull Fx

Fracture treatment

Questions
Linsey, 5 months old presents with knee swelling which of the following would prompt you to file for suspected child abuse:
A. Septic joint with staph on aspirationB. Mongolian spots about the lower backC. Metaphyseal fractures of the distal femurD. Parent are obviously worried and seem
really nice.

Questions
Three year old Stephanie has a history on limping and refusing to put weight on her left leg. She is lying with her leg externally rotated. You are admitting her for:
A. Traction to treat her Perthes disease and high fever.
B. Observation for bracing of her septic hip.C. fever, high white count Perthes treatment.D. Severe malaise, fever, pre-op for septic hip
aspiration.

Questions
An 18 month old infant is admitted to your unit with a fractured femur. You notice blue sclera and shepherd crook deformities of his arms. You would:
A. Hang “Brittle Baby” sign on his cribB. Change his diapers lifting him by the feetC. Keep his medication strictly by weight
even if ineffective to prevent overdosing.D. Use real plasters for casting.

Achondroplasia
• Most common dwarfing syndrome
• 1 of every 26,000 live births M>F
• Etiology: abnormal endochondral
ossification
• genetic defect autosomal dominant
– 90% spontaneous mutations

Achondroplasia
• Hypotonia resulting in slow motor development
• C-spine injuries secondary to poor head control
• Low back pain 2° to spinal stenosis
• Thoracolumbar kyphosis hyperlordosis
• longitudinal growth most affected
• difficulty performing ADL’s

Scoliosis
• Lateral curvature of the spine
• Congenital
• Paralytic
• Neuromuscular
• Idiopathic = most common

Idiopathic Scoliosis
• M=F, Rx 10x more• 3% teens screened• Rx - <20° none• 20-40° brace - to
prevent further curvature
• >40 PSF sequential fixation w/graft

Questions
Your neighbor says her 13 year old daughter has scoliosis and the brace is not making it better she might need surgery. You know:
A. She would improve the curve if she wore the brace.
B. Her curve must be close to 40°,and bracing dose not make it better.
C. Surgery should be performed to make her back completely straight.
D. She will have osteoporosis if it is not fixed immediately.

Neuromuscular Disorders
• Nursing see Table 2 Core Curriculum 3rd ed.• Level of knowledge of the disease
– Realistic expectations– Activities with-in patient limits
• Psychological & functional levels• Support systems• Bowel/bladder function• Skin, Nutrition, Immobility

Neuromuscular Disorders
• Fatigue
• Communication
• Intellectual stimulation
• Dressing
• Emotional needs

Neuromuscular Disorders
• Non Progressive – Cerebral Palsy– Myelodysplasia- Spina Bifida– Arthrogryposis

Cerebral Palsy - CP
• Motor disorder following anoxia to cerebral cortex
• Single largest disability in children• 1-5:1,000 • Time of occurrence
– Prenatal 80%– Perinatal 5%– Postnatal 15%

Cerebral Palsy- CP
• Dx:• Spastic quadriplegia –
cortical motor tract
• Athetotic – extrapyramidal tract
• Ataxic – cerebellum /balance disturb
• Rigid - mixed

Cerebral Palsy- CP
• Nursing
• Parental education non progressive
• Mainstream as much as possible
• Grieve loss of typical child

Myelodysplasia - Spina Bifida
• Group of malformations of spine/post. laminae of vertebra fail to close
• Occulta 20-25% all births– some with no symptoms
• Cystica - Sac – Meningocele – meningeal sac– Myelomeningocele – spinal cord too!
• Has neuro deficits distal to lesion• Hydrocephalus 90%

Myelodysplasia - Spina Bifida
• F > M 1: 1,000 births• Etiology: genetic, folic
acid, valproic acid• Dx: clinical exam, X-ray,
MRI• Rx: neuro, ortho, urologic• Wide range of symptoms

Myelodysplasia- Spina Bifida
• Nursing – multi-disciplinary
team
• Promote mobility, ADLs, diet,
• Bowel bladder program
• Latex precautions
• Neuro status – shunt problems
• Insensate skin, water temp, braces
• Multiple ortho corrections

Arthrogryposis
• Non-progressive disorder with multiple congenitally rigid joints
• Etiology: unknown
0.03% general population
• Dx: clinical exam X-ray, muscle bx.

Arthrogryposis
• Rx: Aggressive PT
at birth
• Casting, bracing, surgical releases
• Normal intelligence

Progressive
– Muscular Dystrophy– Neurofibromatosis– Peroneal Muscular Atrophy– Friedrich’s Ataxia– Polio

Muscular Dystrophy - Myopathy
• Progressive hereditary degenerative weakness of skeletal muscles
• 2-3 of 10,000 males• DX: Muscle Bx. ^ CPK abnormal EMG• Gower’s sign –climb up legs w/ hands• Many types Duchenne’s most common &
severe < 20 yr life span• Becker’s seen at 7yrs < 40 yr life span

Muscular Dystrophy
• Nursing
• Depression – frustration - guilt
• Respiratory - cardiac complications
• Malignant hyperthermia

Neurofibromatosis
• Von Recklinghausen’s disease
• Progressive
• Tumors in central and peripheral nervous system
• 1:400,000 births M=F , 4 Stages
• Dx: café au lait spots >6
• Lisch nodules in iris

Neurofibromatosis
• Instigated by puberty • Spinal deformities 10-15%• Scoliosis, pseudoarthrosis• Most common predisposition to
cancer for children• Elephantitis• Nursing - genetic counseling• Multi system effected
(See table 13 Core Curriculum)

Questions
The single largest cause of disability in children is
A. Neurofibromatosis
B. Myelodysplasia
C. Arthrogryposis
D. Cerebral Palsy

Questions
John is 11 year old pubertal male. He is being seen today for scoliosis screening you notice has 6 large light brown spots on his trunk. You worry that he is in stage
A. 4 of neurofibromatosisB. 2 of myasthenia gravisC. 2 of Von Recklinghausen’s diseaseD. 5 of osteogenesis imperfecta

Peroneal Muscular Atrophy
• Charcot-Marie-Tooth – hereditary atrophy of peripheral and motor nerve roots & freq spinal cord
• Etiol: unknown 2-5 100,000 people M>F
• Dx: decrease sensation / function
• Rx: orthotics – surgical releases
• Genetic counseling

Friedrich’s Ataxia
• Hereditary degeneration of the spinal cord and cerebellum
• M=F presents 5-20 yrs.
• Dx: unsteady gait (ataxia) 1st symptom
• Aggravated by puberty <40 yr life span
• Fibromyopathic changes heart muscle

Polio
• Acute infection of nervous system by polio virus
• Incidence rising due to immunization refusal by parents
• Sx: fever malaise, muscle pain, paralysis, some recover 4 mos-2yrs
• Rx: symptomatic post polio 20yrs• Immunizations

Thank-you!