-
8/7/2019 Pediatric Coccidioidomycosis
1/20
Pediatric Coccidioidomycosis
Author: Archana Chatterjee, MD, PhD, Professor of Pediatrics,
Medical Microbiology andImmunology, and Pharmacy, Division of
Pediatric Infectious Diseases, Chief of Division of
Pediatric Infectious Diseases, Creighton University School of
Medicine; Hospital Epidemiologistand Medical Director of Infection
Control, Children's HospitalCoauthor(s): Catherine O'Keefe, DNP,
APRN, Assistant Professor of Nursing and PediatricNurse
Practitioner, Pediatric Infectious Diseases, Creighton University
Medical Center
Introduction
Background
Coccidioides species is a species of dimorphic fungi endemic in
the soil of the southwesternUnited States and some areas of Mexico,
Central America, and South America. Inhalation of
spores results in coccidioidomycosis, which is an acute
pulmonary infection that is oftenasymptomatic but may manifest as a
flulike illness or pneumonia. Occasionally, severeprogressive
pneumonia or residual pulmonary sequelae can result.1,2,3
Although occurring rarely, dissemination is most commonly
observed in a host with underlyingimmunosuppression or other risk
factors. Common sites of dissemination include skin, bone,joint,
and meninges.3
Amphotericin and oral azoles are the mainstays of antifungal
therapy for coccidioidomycosis.Duration of therapy for the
infection is often prolonged and may last several months to
years,with lifelong suppression needed in certain
patients.1,2,3,4
Pathophysiology
Coccidioides species is found in a saprophytic or vegetative
phase in the soil and in laboratoryculture and in a parasitic or
tissue phase in the host.1In the saprophytic phase, the organism
isdescribed as mycelia with branching septate hyphae. The aerial
mycelia contain rectangularspores (ie, arthroconidia) surrounded by
nonviable cells, thus creating a fragile structure.
Uponfragmentation of the hyphae, the infectious arthroconidia
become airborne spores (spherules)measuring 8-30 m in
diameter.4These spores are inhaled by the host and reach the
pulmonaryalveoli; however, they also can be introduced into skin or
soft tissue by inoculation into woundsor by trauma.
Pulmonary infection can result from inhalation of a single spore
in humans. Increased exposureoccurs with disruption of soil, which
can occur with earthquakes, wind or dust storms,
farming,construction, archeological excavations, or with drought
following heavy rains. High inoculumexposures are more likely to
result in symptomatic disease. Primary infection most often
occursin the dry months of the summer or fall. Person-to-person
transmission does not occur. Rarecases of infection from
contaminated fomites (eg, contaminated plaster cast, dusty
clothing) havebeen reported.5
-
8/7/2019 Pediatric Coccidioidomycosis
2/20
The incubation period of coccidioidomycosis averages 10-16 days,
with a range from less than 7to 30 days.2The spores enlarge to
spherules that are round double-walled structures
measuringapproximately 20-100 m in diameter. The spherules undergo
internal division within 48-72hours until they are filled with
hundreds to thousands of offspring (ie, endospores). Rupture ofthe
spherules leads to the release of endospores, which mature to form
more spherules.5The
spherules and endospores are not infectious.
Most Coccidioides species infections remain confined to the lung
and hilar nodes. The bodyresponds to the presence of the endospores
with activation of complement and release ofchemotactic factors. An
intense, primarily neutrophilic, inflammatory reaction follows;
however,the recruited neutrophils and macrophages are unable to
kill the organisms because the spherulesare resistant to
phagocytosis. T-cell mediated immunity is important for killing and
clearing ofthe organism; therefore, deficiencies in this arm of the
immune system render the host of thefungus extremely vulnerable to
disease and dissemination.5
With dissemination, cell-mediated immunity can become impaired
further, often resulting in
anergy to skin tests. The mechanism for this effect on
cell-mediated immunity is unclear,although many theories have been
postulated. Antigen overload, suppressor cells, formation ofimmune
complexes, and elaboration of immunosuppressive substances by the
fungi maycontribute to the impairment in cell-mediated
immunity.5Eventually, immunity may recover withtreatment and
control of the coccidioidomycosis.
Frequency
United States
Incidence averages approximately 150,000 cases of
coccidioidomycosis per year. This estimateis greater than the
100,000 cases per year previously cited in the literature as a
result ofpopulation increases in southern Arizona and central
California, where the organism isendemic.6,4Coccidioides species is
endemic in soil in the southwestern United States,
includingCalifornia (especially the San Joaquin Valley), western
Texas, New Mexico, and the deserts ofArizona. In endemic areas, the
annual risk of infection is 2-4% among healthy individuals.
Theorganism's habitat is characterized as the lower Sonoran life
zone, with an arid-to-semiaridclimate, alkaline dry soil, hot
summers, moderate-to-low rainfall of 5-20 in/y, and inability
togrow at altitudes greater than 3700 feet.1,6,7
Coccidioidomycosis can be observed in nonendemic areas due to
travel, population mobility,immunosuppression, and reactivation.
Diagnosis often is delayed in nonendemic areas becausecoccidioidal
infection initially is not considered in the
differential.2,3,5,8Domesticated, zoo, andwild animals can also be
infected with Coccidioides species.
Coccidioidal disease has a significant socioeconomic impact in
the United States. An otherwisehealthy individual diagnosed with
symptomatic coccidioidomycosis may miss more than 1month of school
or work. Recent estimates of antifungal medication costs range from
$5000-20,000 per person per year of therapy for the disease.3,9
-
8/7/2019 Pediatric Coccidioidomycosis
3/20
International
Coccidioides species (specifically C posadasii) is also found in
northern Mexico and some partsof Central and South America; all
areas are located between 40 latitude, north and south.2,10,11
M
ortality/M
orbidity
Mortality is extremely uncommon with primary coccidioidomycosis.
Approximately 90-95% ofinfections resolve without sequelae;
however, 5-10% have severe or progressive pneumonia,including
nodules or peripheral thin-walled cavities, with a smaller
proportion resulting inchronic pulmonary or extrapulmonary disease.
Dissemination is uncommon (approximately0.5% of infections in
whites), typically involves infection of the skin, bone or joint,
lymph nodes,or CNS, and is associated with increased morbidity and
mortality. In the host who isimmunocompromised, the risk of
dissemination is much higher (up to 30-50%), and mortalitycan be as
high as 70% even with appropriate therapy.2,3,5
Race
No race predilection for primary infection with Coccidioides
species is observed. Disseminationis more common in Filipinos and
blacks and possibly in other Asians, Hispanics, and
NativeAmericans. The risk of dissemination is 175 times greater in
Filipinos and 10 times greater inblacks than in non-Hispanic
whites.4Some studies have suggested genetic bases to
thepredisposition to dissemination, including a possible
association with blood group type B.12
Sex
Increased incidence of primary coccidioidal infection may be
apparent in older boys and men
because of occupational exposure. Women who are pregnant,
especially during the thirdtrimester and in the peripartum period,
are at higher risk for dissemination than the
generalpopulation.4,13,14
Age
In general, dissemination is less common in children than in
adults. Neonatal infection is rare14;however, infants can
experience severe disease within the first few months of life,
especially ifexposed to a large respiratory inoculum.
Clinical
History
In patients with suspected coccidioidomycosis, a history of
travel or residence in an endemicarea is very important in
establishing the risk of exposure. The exposure may be as limited
asdriving through an endemic area.1,2,3,4,5,15,16
y Patients with primary pulmonary coccidioidal infection may
have the following:
-
8/7/2019 Pediatric Coccidioidomycosis
4/20
o Fevero Localized adventitious breath soundso Mild respiratory
distresso Arthritis and rash (classic rash is erythema multiforme
[EM] or erythema nodosum [EN])
y In general, a patient with disseminated coccidioidomycosis may
have signs of the following:o Chronic illnesso Weight losso Fevero
Lymphadenopathy: The physical examination depends on the site of
involvement and is
relatively nonspecific.
Physical
In most patients with coccidioidal infection, the primary
infection is in the lungs. In 60-65% ofindividuals affected with
coccidioidomycosis, primary pulmonary infection is
asymptomatic.Extrapulmonary primary infections can occur with
trauma causing a puncture wound from acontaminated object.
Laboratory workers and children are especially at risk for
cutaneous or softtissue lesions, including chancres, with regional
lymphadenitis.1,2,3,4,5,15,16
y Pulmonary coccidioidomycosis15o Pulmonary coccidioidomycosis
may be difficult to differentiate from other acute or
subacute respiratory infections with fever.Most symptomatic
primary infections are not
easily diagnosed as coccidioidomycosis unless classic findings
(eg, EM, EN) are present in
an endemic area.
o Because most patients recover spontaneously, pursuing
documentation of coccidioidalinfection is not imperative unless the
patient is immunocompromised or has signs of
severe progressive disease or dissemination.
y Primary coccidioidomycosis3,4o Symptomatic patients with
primary coccidioidomycosis have a range of presentations
from brief upper respiratory infection or flulike illness to
lobar pneumonia. The most
common symptoms are cough, fever, fatigue, chest pain, dyspnea,
and hemoptysis.
More severe manifestations include pleural effusions,
pericarditis, and rare
presentations mimicking bacterial pneumonia and sepsis.
o Skin manifestations are common with primary infection. More
than 50% of children withprimary coccidioidomycosis develop rashes
that begin as diffuse, evanescent,
maculopapular rashes or urticaria. The host may develop EM or EN
after 3-21 days. EM
is more common in children. Although nonspecific, EN is the
classic presentation in an
endemic area. Prognostically, EN is suggestive of low risk of
dissemination since it
correlates with development of cell-mediated immunity. EN occurs
less often in persons
outside of endemic areas and occurs infrequently in blacks,
Hispanics, and Filipinos.In
adults, females are affected with EN much more frequently than
males.
o Other common symptoms of primary coccidioidomycosis include
arthralgias, arthritis,and myalgias. The syndrome of valley fever
includes fever, arthralgias, and EN or EM.
Headaches and anorexia also can be present. Infants and older
children can present
with stridor from laryngeal infection.
o Primary infection of the newborn rarely occurs. Infection of
the genital tract of themother can result in placental involvement,
coccidioidal endometritis, and aspiration of
-
8/7/2019 Pediatric Coccidioidomycosis
5/20
infected amniotic fluid by the fetus. Both congenital and
perinatal transmission of
Coccidioides species have been reported.
o Although the illness, especially the fatigue, may persist for
weeks to months, 90-95% ofprimary pulmonary infections resolve
without sequelae. Of patients with primary
coccidioidomycosis, 5-10% have persistent pulmonary nodules or
cavities on chest
radiography. The cavitary pulmonary lesions often are
thin-walled, asymptomatic, and
resolve spontaneously. Cavities larger than 6 cm in diameter are
at greater risk for
rupture and require surgery.
o Occasionally, the pneumonia can be severe or progressive or
dissemination can occur. Inaddition, chronic pulmonary infection
can occur, particularly in hosts who are
immunocompromised or those with underlying diabetes. Children
rarely develop
chronic pulmonary lesions.
y Disseminated coccidioidomycosis17o Consider disseminated
coccidioidomycosis in individuals with persistent fevers or
malaise; chronic pulmonary infiltrates or nodules; or skin, soft
tissue, or bone lesions in
the appropriate epidemiologic setting.
o A higher risk of infection is suggested after a large inoculum
exposure to soil, such asfrom windstorms, digging, farming, and
construction.
o Approximately 0.5-1% of individuals with coccidioidomycosis
develop disseminateddisease. Dissemination usually occurs weeks to
months after the initial infection but
may occur after 1 year in a host who is immunocompromised. In
addition, reactivation
of treated primary disease may occur at any time in a host who
is immunosuppressed.
o Widespread miliary disease is very rare but may progress
rapidly and is often fatal. Thepresence of diffuse reticulonodular
or miliary pulmonary infiltrates from
coccidioidomycosis suggests an underlying immunodeficiency.
Hosts who are
immunocompromised can have concurrent aggressive primary
pulmonary disease and
dissemination.
o Infection in the host who is immunocompromised is fulminant,
especially with T-celldysfunction in patients with H
IV18
, solid organ transplantation
19,20
, and/or lymphoma.Patients who are immunosuppressed from
high-dose corticosteroid or anti-tumor
necrosis factor (TNF) therapy are also at increased risk for
dissemination. Patients with
organ transplants are at the greatest risk for disseminated
coccidioidomycosis in the
first year posttransplant. Ten percent of patients who are HIV
positive and reside in
endemic areas contract active coccidioidal disease each year. In
particular, adults
infected with HIV with CD4 counts less than 250 are at
significant risk for active disease.
o Signs of dissemination include persistent fever, toxicity, and
development ofextrapulmonary lesions. Coccidioides species has a
predilection for the lungs, skin, soft
tissue, joints, and CNS, especially the meninges.
o The skin is the most common site of extrapulmonary
disease.21In most types ofdisseminated disease, the skin eventually
is involved. The classic skin manifestation of
coccidioidomycosis is a verrucous granuloma at the nasolabial
fold. Other typical lesions
include granulomatous papules, nodules, and plaques, especially
on the head. These
lesions can progress to subcutaneous involvement, sinus tracts,
abscesses, and chronic
ulcers. Differential diagnoses of coccidioidal skin lesions
include tuberculosis, syphilis,
other fungi, actinomycetes, sarcoid, warts, and squamous cell
carcinoma.
o Coccidioidomycosis also affects joints, causing synovitis.
Knees are the most commonjoints involved, followed by ankles and
wrists. Infection of the bone typically causes a
chronic osteomyelitis, often draining to soft tissue and
creating fistulae. Long bones, as
-
8/7/2019 Pediatric Coccidioidomycosis
6/20
well as bones of the hands, feet, pelvis, and skull, may be
involved. Approximately 60%
of incidents of coccidioidomycosis are limited to a single bone,
with 20% involving 2
bones and 10% involving 3 bones. Vertebral osteomyelitis can
affect any part of the
vertebra, sparing the disc, but putting the patient at risk of
meningitis.22
o Approximately 50% of patients with disseminated
coccidioidomycosis acquireCNSdisease. It can occur acutely with
primary infection or later with dissemination and can
be the only site of dissemination. CNS coccidioidomycosis can
present with headache,
vomiting, nuchal rigidity, change in mental status, lethargy,
confusion, ataxia, diplopia,
and focal neurologic signs.23Coccidioidal meningitis is usually
chronic with insidious
onset, in contrast to meningitis from bacterial causes.
Typically a granulomatous and
suppurative basilar process, coccidioidal meningitis can also
involve the brain
parenchyma and spinal cord with granulomas and abscesses.
Hydrocephalus is a
common sequela and is often present at initial diagnosis in
children.
o Although the skin, lungs, joints, soft tissue, and meninges
are the most common sites forcoccidioidal dissemination
17, infection of almost every other organ system has been
reported. At autopsy, involvement of the liver, spleen, kidney,
adrenal glands, psoas
muscle, heart, thyroid, and prostate has been noted. These
infected sites rarely are
responsible for the presenting signs or symptoms. Infection of
the thyroid gland hasbeen reported to result in a thyroid abscess
and thyrotoxicosis.
Ocular coccidioidomycosis can present as a lacrimal gland fossa
mass or witheye pain, photophobia, and other symptoms of
chorioretinitis or iridocyclitis.
Hepatic infection is usually asymptomatic but can be part of a
hepatic-pulmonary syndrome with a brief hepatitis-like illness,
hepatic granulomas, and
eosinophilia.
Coccidioidal infection of the biliary tree is uncommon but has
been reported topresent as abdominal pain and obstructive jaundice.
Intestinal obstruction and
peritonitis have also been reported to be secondary to
coccidioidal infection.
Coccidioidal infection of the genitourinary tract can result in
nodules orgranulomas, abscesses, or fistulae in the kidney, ureter,
bladder, prostate,epididymis, or testes.
Differential Diagnoses
Actinomycosis Lymphadenopathy
Acute Lymphoblastic Leukemia Lymphoproliferative Disorders
Acute Myelocytic Leukemia Meningitis, Aseptic
Aspergillosis Meningitis, Bacterial
Atypical Mycobacterial InfectionMycoplasma Infections
Blastomycosis Nocardiosis
Brucellosis Osteomyelitis
Catscratch Disease Parainfluenza Virus Infections
-
8/7/2019 Pediatric Coccidioidomycosis
7/20
Chronic Granulomatous DiseasePneumococcal Infections
FeverWithout a Focus Respiratory Syncytial Virus Infection
Histiocytosis Sarcoidosis
Histoplasmosis Toxoplasmosis
Influenza Tuberculosis
Legionella Infection Wegener Granulomatosis
Workup
Laboratory Studies
The following studies may be indicated in
coccidioidomycosis:
y Nonspecific laboratory testso Nonspecific laboratory tests
include an elevated erythrocyte sedimentation rate (ESR),
leukocytosis, and eosinophilia (>5% in 27% of patients with
coccidioidomycosis).
o Patients with coccidioidal meningitis may have cerebrospinal
fluid (CSF) pleocytosis witha mononuclear predominance, decreased
glucose, and elevated protein.
o One study has suggested an association between low serum
mannose-binding lectin(MBL) levels and symptomatic
coccidiodomycosis.
24
y Serology1,2,3,4,5,25,26o Serologic testing is helpful for
confirmation of the diagnosis and prognostication of
coccidioidal infection. False-positive serology tests are
rare.
o Coccidioidal immunoglobulin M (IgM) is present in 75% of
patients with acute infectionand is more sensitive than complement
fixation (CF) for early infection. IgM usually
appears within 1-3 weeks after the onset of symptoms and lasts
3-4 months; however,
IgM may persist and/or reappear with reactivation.
o Methods to evaluate coccidioidal IgM include latex
agglutination, enzyme immunoassay,immunodiffusion, tube
precipitins, and immunoelectrophoresis. IgM only is useful
qualitatively, as the magnitude does not correlate with
dissemination or extent of
disease.
o Immunodiffusion and CF methods can detect coccidioidal
immunoglobulin G (IgG). TheCF titer is useful as a quantitative
measure of the extent and progression of disease.
Most titers are positive by 3 months after infection onset,
persist 6-8 months, and
disappear as infection resolves.o The CF titer may be low or
absent in mild or asymptomatic disease or in
immunosuppressed patients. Approximately 95-100% of patients
with titers less than or
equal to 1:16 do not have disseminated disease. High titers
greater than or equal to 1:32
persist in severe, untreated extrapulmonary or disseminated
disease.
o Coccidioidal CF titers of the serum and cerebrospinal fluid
can be followed to monitorthe effect of treatment on disease and
predict relapses.
y Culture
-
8/7/2019 Pediatric Coccidioidomycosis
8/20
o Culture ofCoccidioides species from infected tissue or fluids
often is possible within 3-4days of inoculation on laboratory
media, even when spherules are not present on direct
examination.
o In culture, the spherules can convert to arthroconidium and
grow in the lab in theinfectious mycelial phase; therefore, notify
the laboratory of the possibility of
coccidioidomycosis so that appropriate precautions and equipment
may be used.
o After the cultures begin to grow, a chemiluminescentDNA probe
can identify theorganism.
y Susceptibility testing ofCoccidioides species in one report
revealed uniform susceptibility tomost antifungal agents.
27
Imaging Studies
y Radiography1,2,3,4,5,15,16,17,21,22o In primary pulmonary
infection, the chest radiograph depicts nonspecific changes,
including segmental or lobar infiltrates, hilar adenopathy, and
small pleural effusions.
o Five percent of patients may have nodules, cavitation,
bronchiectasis, or calcificationsdepicted on the radiograph. The
cavitary pulmonary lesions are often thin-walled,
asymptomatic, and resolve spontaneously. Cavities larger than 6
cm in diameter are at
greater risk for rupture and require surgery.
o In certain patients with coccidioidomycosis, especially
immunocompromised patients,the chest radiograph can reveal diffuse
nodular densities. Nodules and adenopathy can
be difficult to differentiate from malignancy or other
infectious processes.
o Radiographic changes in primary pulmonary coccidioidomycosis
often resolvespontaneously, albeit slowly.
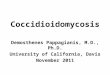
o In patients with osteomyelitis, bone radiographs may show
lytic lesions, periostealelevation, and bony destruction.
o
Coccidioidal osteomyelitis of the right elbow. Plain film
radiograph. Photograph
by Preeyacha Pacham, MD.
CT/MRI
y The high-resolution CT scan can further delineate extent of
pulmonary and lymph nodeinvolvement.
y
-
8/7/2019 Pediatric Coccidioidomycosis
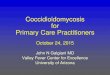
9/20
Pulmonary nodule from infection with Coccidioides species.
CTscan of the chest.
Photograph by Preeyacha Pacham, MD.
[ CLOSE WINDOW]
Pulmonary nodule from infection with Coccidioides species.
CTscan of the chest.
Photograph by Preeyacha Pacham, MD.
y MRI may help better delineate the extent of bone, joint, and
overlying soft tissue involvement,including sinus tracts or
fistulae. A bone scan may detect multiple sites of bony
involvement.
y CT or MRI of the brain in patients with CNS involvement may
demonstrate meningealenhancement, granulomas, or abscesses. In
addition, patients often have signs of hydrocephalus
on imaging. Therefore,MRI may be better in this respect to
evaluate the patency of the
aqueduct ofSylvius.
Other Tests
y Skin tests5
-
8/7/2019 Pediatric Coccidioidomycosis
10/20
o Skin testing is not helpful in making the diagnosis of
coccidioidomycosis because itcannot distinguish between past and
acute infection; however, skin tests can be useful
as epidemiologic or research tools.
o A positive skin test is 5 mm or more of induration observed 48
hours after intradermalapplication. The skin test becomes positive
10-45 days after infection or 2-21 days after
symptom onset.
o Anergy is common in patients with disseminated disease, even
without underlyingimmunosuppression. In addition, a low level of
cross-reactivity with blastomycosis and
histoplasmosis occurs.
Procedures
y Perform lumbar puncture in patients with fever, headache,
nuchal rigidity, meningismus, mentalstatus changes, or ataxia.
16,17
y Bronchoscopy with bronchoalveolar lavage, needle aspiration,
and/or lung biopsy may beindicated with persistent or progressive
infections, especially in hosts who are
immunocompromised.
y Synovial biopsy may be needed to document coccidioidal
dissemination to a joint.Histologic Findings
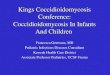
y Histopathologic specimens of affected tissues may reveal the
pathognomonic spherules onhematoxylin-eosin or silver stains.
y
Coccidioidal spherules rupturing and releasing endospores.
Gomori methenamine
silver (GMS) stain. Photograph by Joseph Rabban, MD.
[ CLOSE WINDOW]
-
8/7/2019 Pediatric Coccidioidomycosis
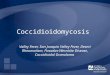
11/20
Coccidioidal spherules rupturing and releasing endospores.
Gomori methenamine
silver (GMS) stain. Photograph by Joseph Rabban, MD.
y Spherules may be observed in tracheal aspirates; purulent
material; biopsies of lymph nodes,skin, or organs; joint fluid;
urine; and, less commonly, cerebrospinal fluid.
y Tissue lesions consist of granulomas with abundant giant cells
and histiocytes, with or withoutacute inflammation.
y Caseous necrosis, fibrous changes, and rare calcification can
also be found.Treatment
Medical Care
Antifungal therapy is not usually necessary for uncomplicated
acute primarycoccidioidomycosis. For many patients, management of
uncomplicated acute primarycoccidioidal pneumonia mainly relies on
periodic reassessment of symptoms and resolution ofany radiographic
findings. However, some experts propose treatment of all
symptomaticpatients; currently the data from prospective controlled
trials in this area are insufficient.Initiation of therapy is
warranted for specific situations, such as for patients with
severeprogressive pulmonary disease or with concurrent risk factors
fordissemination.10,1,2,3,4,5,15,16,17,18,21,22,23
y Indicators of severity of illness for which to consider
therapy of acute primary pulmonaryinfection include the
following:
3
o Continuous fever for longer than 1 montho Night sweats for
longer than 3 weekso Weight loss greater than 10%o Prominent or
persistent hilar adenopathy
-
8/7/2019 Pediatric Coccidioidomycosis
12/20
o Large (>50% of one lung) or bilateral pulmonary
infiltrateso Complement fixation (CF) titers greater than or equal
to 1:16o Persistent symptoms for longer than 2 monthso Inability to
worko Age older than 55 years
y Risk factors for dissemination for which treatment should be
initiated include the following:o Primary infection during infancyo
Primary infection during pregnancy, especially in the third
trimester, or immediately
postpartum
o Immunosuppressiono Chronic debilitation or underlying disease,
including diabetes mellitus or preexisting
cardiopulmonary disease
o High inoculum exposureso Certain ethnicities, such as Filipino
or black
y Typical antifungal therapy of acute primary pulmonary
coccidioidomycosis in these high-riskgroups consists mainly of oral
azoles at the recommended adult doses (usually 200-400 mg/d)
for 3-6 months duration (see Medication). During pregnancy,
amphotericin B is the treatment of
choice because the azoles may be teratogenic.y Initially treat
patients with diffuse pulmonary disease (ie, miliary or
reticulonodular infiltrates)
with amphotericin B or high-dose fluconazole for several weeks
until definite signs of
improvement are observed. If there is rapid deterioration or
significant hypoxia, amphotericin B
is used more frequently. After clear evidence of improvement
emerges, therapy may be
changed to an oral azole to complete a prolonged course of
antifungal therapy. Because these
patients are often immunocompromised, the total duration of
therapy should be at least 1 year,
with secondary prophylaxis continuing indefinitely for subgroups
of patients who are severely
immunodeficient.
y Persons with asymptomatic pulmonary nodules or cavities often
do not warrant antifungaltherapy in the absence of
immunosuppression.
y Individuals with symptomatic or enlarging cavities may respond
to oral azole therapy or oral
antibacterial therapy, if bacterial superinfection of the cavity
is present. However, symptoms
may recur upon cessation of therapy and the cavities usually do
not resolve with antifungal
therapy.
y Antifungal therapy, often in conjunction with surgical
treatment, is recommended for patientswith ruptured coccidioidal
cavities.
y Individuals with chronic progressive fibrocavitary pneumonia
may be treated with prolongedazole therapy for at least 1 year.
Persons with progressive pulmonary disease not responding to
medical therapy with oral azoles may benefit from a higher dose
of azole, an alternative azole,
or amphotericin B and/or surgical resection.
y All patients with disseminated coccidioidomycosis warrant
prolonged antifungal treatment.Therapy for nonmeningeal
extrapulmonary disease can be initiated with oral azoles unless
the
disease is rapidly progressive or in a critical location (such
as the vertebral column); in such
situations, the alternative therapy is amphotericinB. Some
authors suggest initial therapy with
amphotericin B until significant clinical, radiographic, and
laboratory test (in particular, CF titers)
improvements are documented, followed by completion of the
antifungal regimen with an oral
azole. Fluconazole and itraconazole are the most commonly used
azoles, at doses from 400-
2000 mg/d for fluconazole, and up to 800 mg/d for
itraconazole.
y In patients who warrant amphotericin B therapy but have
drug-related toxicities, lipidamphotericin B formulations can be
considered and have been effective in animal models,
-
8/7/2019 Pediatric Coccidioidomycosis
13/20
although no human clinical trials have assessed their efficacy.
Combination therapy with
amphotericin B and an azole has been reported, but no clinical
trials have demonstrated its
superiority to single agent treatment, and antagonism with
combination therapy has been
reported for other fungal infections.
y The preferred regimen for individuals with meningeal disease
is administration of oralfluconazole, although itraconazole also
has been reported to be effective.Adult dosages of
fluconazole for meningitis range from 400-1000 mg/d and for
itraconazole from 400-600 mg/d.
Intrathecal amphotericin B23,28
has been used in conjunction with an oral azole, both initially
and
as an alternative regimen after failure with azole therapy
alone. The dose of intrathecal
amphotericin B ranges from 0.1-1.5 mg per dose.
y Lifelong antifungal therapy must be continued in patients with
CNS involvement23withCoccidioides species because of high relapse
rates (ie, up to 75%) with oral azoles.
y CNS vasculitis is a life-threatening complication of
coccidioidal meningitis. Short-term treatmentwith high-dose IV
corticosteroids has been reported with varying results in regards
to benefit.
Surgical Care
y Surgery is indicated for the following conditions:
asymptomatic persistent pulmonary cavities,especially if enlarging
or adjacent to the pleura; symptomatic localized or persistent
pulmonary
infections, including empyema and bronchopleural fistulae; and
cavities associated with rupture
or hemoptysis.
y In patients with chronic osteomyelitis, drainage of sequestrum
in bones and debridement ofadjacent purulent soft tissues often is
necessary. Joint involvement can be managed by incision
and drainage, although occasionally synovectomy and arthrodesis
are needed. Immobilization of
limbs affected by the disease may be necessary.
y The benefit of irrigation and local instillation of
amphotericin B to joints, cavities, or abscessesaffected by
coccidioidomycosis is controversial, and no clear data supporting
this practice are
available.
y Hydrocephalus from CNS involvement often requires shunt
placement for management.Medication
Historically, amphotericin B has been the drug of choice to
treat disseminatedcoccidioidomycosis. More recently, oral azoles
have provided a desirable alternative for bothinitial therapy and
completion of courses after amphotericin therapy. The benefits of
azolesinclude oral formulations and fewer adverse effects. Large,
multicenter, nonrandomized clinicaltrials have studied the response
of chronic pulmonary and disseminated coccidioidal infections
tooral azoles (eg, fluconazole, itraconazole, ketoconazole) and
have found adequate treatmentefficacy but high relapse rates upon
cessation of therapy. Other azoles (eg, voriconazole) may
also be effective against Coccidioides species. Research on the
use of immunomodulators toimprove T-cell response to coccidioidal
infection is still underway. A new triazole antifungal,posaconazole
(Noxafil), was recently approved by the US Food and Drug
Administration(FDA).3,29,30
-
8/7/2019 Pediatric Coccidioidomycosis
14/20
Polyene antifungal
These agents are used for rapidly progressing coccidioidal
infection and disease unresponsive tooral azole therapy.
Amphotericin B (Fungizone, AmBisome,Abelcet)
Polyene antibiotic produced by a strain ofStreptomyces nodosus;
can be fungistatic orfungicidal. Binds to sterols, such as
ergosterol, in the fungal cell membrane, causing
intracellularcomponents to leak with subsequent fungal cell
death.DOC for rapidly progressing coccidioidal infection and
disease nonresponsive to PO azoletherapy. Liposomal amphotericin
should be used when significant nephrotoxicity is a risk
withconventional amphotericin B therapy. Intrathecal amphotericin B
has been used for coccidioidalmeningitis.
y DosingAdult
Primary pulmonary (amphotericin B lipid complex or liposomal): 5
mg/kg/day IV; infuse IV atrate of 2.5 mg/hMeningitis (amphotericin
B deoxycholate [conventional]): 0.1-1.5 mg/dose IT; administered
atintervals from daily to weekly, increasing dose to patient's
tolerance
Pediatric
Administer as in adults
y InteractionsAntineoplastic agents may enhance potential of
amphotericinB for renal toxicity,
bronchospasm, and hypotension; corticosteroids, digitalis, and
thiazides may potentiate
hypokalemia; risk of renal toxicity is increased with
cyclosporine
y ContraindicationsDocumented hypersensitivity
y PrecautionsPregnancy
B - Fetal risk not confirmed in studies in humans but has been
shown in some studies in animals
-
8/7/2019 Pediatric Coccidioidomycosis
15/20
Precautions
Severe renal dysfunction can result; administer NS bolus or PO
sodium chloride before eachdose; monitor serum electrolytes (eg,
magnesium, potassium), liver function, CBC count, andhemoglobin
concentrations; resume therapy at lowest level when therapy is
interrupted for more
than 7 d; hypoxemia, acute dyspnea, and interstitial infiltrates
may occur in neutropenic patientsreceiving leukocyte transfusions
(separate time of amphotericin infusion from time of
leukocytetransfusion); IT administration may cause pain with
administration, headache, paresthesias,nerve palsies, and
arachnoiditisPremedication with acetaminophen and/or
diphenhydramine may reduce infusion-relatedsymptoms and may be
repeated at appropriate dosing interval if infusion is
prolonged;hydrocortisone (mixed with amphotericin solution) has
also been used to reduce infusion-relatedsymptoms
Azole antifungals
Oral azoles have been used in the treatment of disseminated
coccidioidomycosis and primarypulmonary infections in high-risk
groups. Overall, the initial response rate is 50-60% with
azoletherapy, although relapse rates may be as high as 50%. A
preliminary report from the MycosesStudy Group found no
statistically significant difference in efficacy between
fluconazole anditraconazole. How well azoles perform in rapidly
progressive disease is not clear.
Fluconazole (Diflucan)
Fungistatic activity. Synthetic PO antifungal (broad-spectrum
bistriazole) that selectively inhibits
fungal CYP450 and sterol C-14 alpha-demethylation, which
prevents conversion of lanosterol toergosterol, thereby disrupting
cellular membranes.Used in treatment of primary pulmonary
infections in high-risk groups and of
disseminatedcoccidioidomycosis. Preferred over ketoconazole because
of better response rates and less GIand endocrine adverse effects.
Available in PO susp.
y DosingAdult
400 mg/d PO/IV; doses as high as 800-1000 mg/d have been
reported
Pediatric
10-12 mg/kg/d PO/IV; not to exceed 400 mg/d
y Interactions
-
8/7/2019 Pediatric Coccidioidomycosis
16/20
Levels may increase with hydrochlorothiazide; levels may
decrease with long-term
coadministration of rifampin; coadministration of fluconazole
may decrease phenytoin
clearance; may increase concentrations of theophylline,
tolbutamide, glyburide, and glipizide;
effects of anticoagulants may increase with fluconazole
coadministration; increases in
cyclosporine concentrations may occur when administered
concurrently
y ContraindicationsDocumented hypersensitivity, pregnancy,
concurrent QT-prolonging drugs, congenital long QT
pts or conditions that incur QT prolongation risk
y PrecautionsPregnancy
C - Fetal risk revealed in studies in animals but not
established or not studied in humans; mayuse if benefits outweigh
risk to fetus
Precautions
Monitor closely if rashes develop and discontinue drug if
lesions progress; may cause clinicalhepatitis, cholestasis, and
fulminant hepatic failure (including death) in patients with
underlyingmedical conditions (eg, AIDS, malignancy) and in those
taking multiple concomitantmedications; not recommended for mothers
who are breastfeeding
Itraconazole (Sporanox)
Fungistatic activity. Synthetic triazole antifungal agent that
slows fungal cell growth byinhibiting CYP450-dependent synthesis of
ergosterol, a vital component of fungal cellmembranes.Used to treat
primary pulmonary infections in high-risk groups and
disseminatedcoccidioidomycosis. Preferred over ketoconazole because
of better response rates and less GIand endocrine adverse effects.
IV form available, but long-term usage is not established.
Alsoavailable in PO solution. The PO solution provides better, more
consistent absorption than thecapsule. Take capsules with full meal
to improve absorption, but take oral solution on emptystomach, if
possible.
y DosingAdult
400 mg/day PO
Pediatric
5-10 mg/kg/day PO; not to exceed 400 mg/day
-
8/7/2019 Pediatric Coccidioidomycosis
17/20
y InteractionsStrong CYP3A4 inhibitor; antacids may reduce
absorption; edema may occur with
coadministration of calcium channel blockers (eg, amlodipine,
nifedipine); hypoglycemia may
occur with sulfonylureas; may increase tacrolimus and
cyclosporine plasma concentrations
when high doses are used; rhabdomyolysis may occur with
coadministration of HMG-CoA
reductase inhibitors (ie, lovastatin, simvastatin);
coadministration with cisapride can cause
cardiac rhythm abnormalities and death; may increase digoxin
levels; coadministration may
increase plasma levels of midazolam or triazolam; phenytoin and
rifampin may reduce
itraconazole levels (phenytoin metabolism may be altered)
y ContraindicationsDocumented hypersensitivity; pregnancy;
concurrent QT-prolonging drugs or congenital long QT
y PrecautionsPregnancy
C - Fetal risk revealed in studies in animals but not
established or not studied in humans; mayuse if benefits outweigh
risk to fetus
Precautions
BlackBox WarningsCongestive heart failure (CHF): Negative
inotropic effects reported with IV administration;reassess therapy
if signs or symptoms of CHF occur during
administrationContraindicated drug interactions: Potent CYP450 3A4
inhibitor; serious cardiovascular events,including QT prolongation,
torsades de pointes, ventricular tachycardia, cardiac arrest,
and/orsudden death reported when administered with drugs
metabolized by this isoenzyme system,including cisapride, pimozide,
quinidine, dofetilide, or levomethadyl acetateOther
precautionsCaution in hepatic insufficiencies; level can be checked
after 2 wk of therapy to documentadequate absorption; GI distress,
headache, dizziness, rash, and hypokalemia
Ketoconazole (Nizoral)
Fungistatic activity. Imidazole broad-spectrum antifungal agent;
inhibits synthesis of ergosterol,causing cellular components to
leak, resulting in fungal cell death.Has been used in treatment of
coccidioidomycosis, although fluconazole and itraconazole
arepreferred because of low response rates (
-
8/7/2019 Pediatric Coccidioidomycosis
18/20
Adult
400-800 mg/day PO; if 800 mg/day needed, administer in divided
doses bid
Pediatric
>2 years: 3.3-6.6 mg/kg/day PO; not to exceed adult dose
y InteractionsStrong CYP3A4 inhibitor; isoniazid may decrease
bioavailability; coadministration with rifampin
decreases effects of either drug; may increase effect of
anticoagulants; may increase toxicity of
corticosteroids and cyclosporine (cyclosporine dosage can be
adjusted); may decrease theophylline
levels; ventricular arrhythmias reported when ketoconazole was
coadministered with cisapride
(restricted distribution in the US), terfenadine, or astemizole
(no longer on US market) due to
accumulation of these drugs
y ContraindicationsD
ocumented hypersensitivity
y Precautions
Pregnancy
C - Fetal risk revealed in studies in animals but not
established or not studied in humans; mayuse if benefits outweigh
risk to fetus
Precautions
Caution in hepatic insufficiencies; has been associated with
fatal hepatotoxicity; high doses maysuppress adrenocortical
function; jaundice, GI distress, rash, alopecia,
adrenocorticalinsufficiency, diminished libido, impotence,
menstrual irregularities, and gynecomastia
Follow-up
Further Outpatient Care
y Treatment of patients with primary pulmonary
coccidioidomycosis relies on periodic monitoringof symptoms and
radiographic studies to assess residual disease (eg, nodules,
cavities) and
identify signs of early dissemination.
y Continue follow-up care for at least 1-2 years or until
resolution of all coccidioidal diseaseoccurs. The identification of
progressive pulmonary disease or dissemination warrants
initiationof antifungal therapy as outlined in Medication.
y Follow-up care of patients with disseminated
coccidioidomycosis includes periodic monitoring ofthe complement
fixation (CF) titer until it is less than 1:8. Also, monitor other
abnormal
laboratory or radiographic studies at regular intervals.
y Initially, monitor CF titers at monthly intervals until a
consistent decrease has beendocumented. Relapses of
coccidioidomycosis can be predicted by recurrence of symptoms,
-
8/7/2019 Pediatric Coccidioidomycosis
19/20
physical findings, and increases in the CF titer. Cerebrospinal
fluid (CSF) abnormalities and CF
titers may persist for months despite therapy.
y Development of hydrocephalus in a patient with coccidioidal
meningitis who is otherwise stableand improving does not imply
failure of antifungal therapy.
y Monitor routine health maintenance as well as reviews of all
medications for potential druginteractions with the prescribed
antifungal therapy. Periodically evaluate adverse effects of
antifungal medications by history and laboratory testing.
Deterrence/Prevention
y Infection with Coccidioides species can be minimized with dust
control measures at constructionor archaeological sites and in
areas with large amounts of soil disruption.
y Within the hospital, isolation precautions are not necessary
because person-to-persontransmission of the disease does not occur;
however, draining wounds may pose an infectious
risk from aerosolization of organisms growing in the dressing or
cast material. Enforce proper
disposal of contaminated materials.2
y Primary prophylaxis for patients with HIV in endemic areas is
not recommended routinely.However, indefinitely continue
suppressive therapy after active disease (ie, secondary
prophylaxis) with oral itraconazole (200 mg twice a day) or
fluconazole (400 mg each day). For
patients with organ transplants and a history of
coccidioidomycosis, antifungal treatment at the
time of engraftment has been proposed, although no formal
recommendations exist.
y No vaccines to prevent coccidioidomycosis currently are used
in humans. A killed spherule-derived vaccine was found to be
efficacious in experimental animals but not protective in
humans. Multiple Coccidioides species cell-surface antigens have
been investigated for their
ability to stimulate protective T-cell mediated immune
responses.Currently, recombinantDNA
techniques to develop vaccines using the proline-rich31
and other antigens from the Coccidioides
spherule appear promising.
Miscellaneous
MedicolegalPitfalls
y Delay in diagnosis of disseminated coccidioidomycosis may
occur, given the insidious nature ofthe disease; however, no
medicolegal issues specific to the diagnosis or management of
coccidioidomycosis exist.
Acknowledgments
The authors and editors of eMedicine gratefully acknowledge the
contributions of previousauthors Michele M Cheung, MD and Peggy
Weintrub, MD to the development and writing ofthis article.
-
8/7/2019 Pediatric Coccidioidomycosis
20/20