Embed Size (px)
Citation preview

Stelios Mantis, MD DuPage Medical Group
Pediatric Endocrinology4‐11‐13

Initial Presentation
Pt initially presented to pediatrician for school physical in
fall 2012.
Pt was found to be overweight (BMI: 27.4) and have signs
of insulin resistance (acanthosis) and hirsutism as well as thyromegally (no thyroid exam in notes).
Fasting labs: Glucose 103 mg/dl, normal CMP otherwise,
normal lipid panel, TSH: 0.95 mIU/ml, free testosterone: 2.7 pg/ml; thyroid US: 4 mm solid nodule, hypoechoic
hypovascular.
Sent to endocrine. Mom told it’s likely PCOS.

Initial PresentationCC: 13 11/12 yr old female presents to peds endo with
hirsutism, acanthosis, impaired fasting glucose, with the previous labs.
ROS: Has had hirsuitism and acanthosis for ~6 mo‐1yr, not bothered by it. No polyuria no polydipsia or
weight loss. No headaches, abdominal pain, or visual deficits. Deodorant use ~ 4 yr ago. Menarche ~8
months ago, periods irregular (perhaps every other month). LMP: 3 wks ago. Feels she is done growing.
No high blood pressure in the past

Initial PresentationPast medical history: Always been overweight, no meds
no allergies
Family History: Gestational DM (mom)
Mid Parental Height: 64 inches
Social Hx: no smoking, no alcohol, no illicit drug use, not sexually active

Initial Presentation
Physical Exam:
BP 118/84 Pulse 64 Ht 62.7 inches (40th%) Wt
155 lb 3.2 oz (90th%) BMI 27.7 (95th%)
Gen:
Pleasant, NAD, cooperative
HEENT:
hair along jawline, upper lip, anicteric sclera, MMM, Nl
visual field, no palpable nodules on thyroid, generous thryoid,
no lymphadenopathy, + acanthosis along neck
CV:
normal
Lungs:
CTAB
Abd:
soft obese, + hair in periumbilical region, no striae
Neuro:
nl reflexes, good strength in upper and lower extremities
Pubertal Exam:
no cliteromegally, Tanner 5 breast and pubic
hair, + hair on areola




Differential Diagnosis
Late onset CAH
PCOS
Androgen exposure
Hypercortisolemism
Adrenal Tumor
Virulizing Tumor
Glucocorticoid resitance

Tests Ordered (AM labs)
Free Testosterone: 3.5 pg/ml
Prolactin: 17.5 ng/ml (4.6‐23.3)
Estradiol: 19 pg/ml
LH: 19 mIU/ml
FSH: 9.2 mIU/ml
SMBG: 5.3 nmol/L (24.6‐122)
Androstenedione: 354 ng/dl (50‐224)
17 OH‐Progesterone: 108 ng/dl (20‐285)
Insulin: 32.4 uIU/ml (2.6‐24.9)
DHEA‐S: 314.7 ug/dl (33.9‐280)
CMP: nl except fasting glucose of 101 mg/dl
TSH: 0.929 uIU/ml
Free T4: 1.26 ng/dl
ACTH: 475.9 pg/ml ( 7.2‐63.3)
Cortisol: 24.4 (2.3‐19.4)
Bone age: ordered but not done

Tests Ordered (AM labs)
Free Testosterone: 3.5 pg/ml
Prolactin: 17.5 ng/ml (4.6‐23.3)
Estradiol: 19 pg/ml
LH: 19 mIU/ml
FSH: 9.2 mIU/ml
SMBG: 5.3 nmol/L (24.6‐122)
Androstenedione: 354 ng/dl (50‐224)
17 OH‐Progesterone: 108 ng/dl (20‐285)
Insulin: 32.4 uIU/ml (2.6‐24.9)
DHEA‐S: 314.7 ug/dl (33.9‐280)
CMP: nl except fasting glucose of 101 mg/dl
TSH: 0.929 uIU/ml
Free T4: 1.26 ng/dl ACTH: 475.9 pg/ml ( 7.2‐63.3) Cortisol: 24.4 (2.3‐19.4)
Bone age: ordered but not done

Phone call; 4 PM labs
ACTH: 71.8
Cortisol: 20.9
Midnight salivary cortisol: not sufficient sample X 2
MRI: Ordered
Dex suppression test: 8 mg at midnight
8 am cortisol: 1.3 ACTH: 3.6
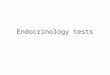
MRI: See following images

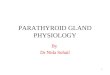
Elevated ACTH/cortisol at 1600;
loss of diurnal cortisol pattern
24 hr urine cortisol/mid
salivary cortisol
Low Intermediat
e High
obesitypseudocushing
Low dose dexSuppression testsuppressed
Unsuppressed
Hypercortisolem
ia
High dose dex
Suppressed = pituitary
source
No suppression =
Ectopic ACTH or
adrenal tumor



MRI Results
There is a sellar
mass with suprasellar
extension and
what appears to be indentation at the diaphragmatic sella
based on sagittal
image seven and demonstrating
enhancement, overall measuring approximately 10 x 11 x 12 mm in AP, transverse, and craniocaudal
dimensions, respectively, with involvement of the pituitary infundibulum.

Next Steps
Call placed to U of C neurosurgery
Informed pt and family of results
Went over possible course of action
Visual field testing ordered
Dr. Yamini has seen and evaluated patient
Surgery Scheduled for late April 2013
Pt currently in Philippines for a planned vacation

References‐Kappy et al. Pediatric Practice Endocrinology.Chapter 5 Adrenal Disorders pp 180‐181.
‐Jameson, LJ, De Groot,LJ. Endocrinology Adult and Pediatric Volume 1. 6th
edition pp308‐309.