Embed Size (px)
Citation preview

Pediatric Neurology Quick Talks
AtaxiaMichael Babcock
Summer 2013

Scenario
• 2 yo girl
• Acute onset of not walking – every since waking this morning
• Crying and trying to be carried
• No fever
• No recent witnessed trauma
• No erythema, no pain with palpation of extremities
• Hx of normal development, walking for 8 months.
• Awake and alert, but fussy

Refusal to Walk (or abnormal gait/limp)
• Infections – septic arthritis, osteomyelitis, discitis, myositis
• Inflammatory – transient synovitis
• Trauma – toddler's fractures, foot fracture, child abuse, contusions/bruises
• Bony deformity/problem – slipped epiphysis, hip dysplasia, asceptic necrosis (legg-calve-perthes), vaso-occlusive crisis, osteochondrosis, tumors.
• Abdominal pain – appendicitis, PID, abscess
• Neurologic – weakness (muscular dystrophy, NMJ, GBS, TM), ataxia, infections – meningitis, spinal abscess.
• Psychogenic - conversion

History
• When was walking last normal; onset of symptoms?
• Any trauma?
• Vitals? Fever?
• Any LOC or abnormal movements?
• nausea/vertigo/posterior fossa symptoms?
• Why is walking altered? - pain, weakness, numbness, imbalance, can't say?

Neurologic Exam – walk refusal/abnormal walk
• MS
• CN – pupils, eye movements (abnormal movements, opsoclonus), CN 8 (ear exam, tinnitus, hearing loss) – peripheral vestibular neuropathy/labrynthitis
• Motor – strength – weakness –> myopathy/NMJ/peripheral nerve/UMN
• Reflexes – absent? -->GBS, increased?->UMN
• Sensory – uncommon reason in kids – B12, tabes dorsalis, diabetic peripheral neuropathy
• Cerebellar – Rapid alternating movements (finger-tapping/alligator chomp, toe-tapping), Finger-nose-finger, heel-knee-shin, other rhythmic movements-clapping, also listen to speech.
• Gait – romberg, tandem – think of different abnormal gait types.

This lecture is on Ataxia
• Children can present with wide-based, ataxic gait OR with refusal to walk due to sense of imbalance.
• Static ataxia – present in resting state
• Kinetic ataxia – present only with movement
• Dystaxia
– Dysmetria – can't control distance/speed/power – leads to past-pointing
– Dysdiadochokinesia – can't rapidly switch/alternate movements – leads to poor rhythm (hand/foot tapping), leads to poor rapid alternating movements.

Cerebellum
• Midline – vermis– Dysarthia– Truncal titubation– Gait abnormalities
• Hemispheres– Double-crossed tracts,
ipsilateral findings– Limb dysmetria– Ipsilateral veering
while walking– Tremor– hypotonia

Abnormal Gait
• Spastic gait
• Sensory ataxic gait – wide-based, high-stepping, romberg +
• Cerebellar ataxic gait – titubation, wide-based
• LMN – distal weakness, foot drop, high-stepping, but narrow-based
• Myopathic – proximal weakness, difficulty rising from chair, Gower's
• Movement disorder gaits – adventitial movements, lurching gait
• Psychogenic – Astasia-abasia – wide variation with complex movements, often wide movement off vertical axis without falling.

Romberg test
-Sensory ataxia
-Pt can stand with feet together with eyes open, but not eyes closed.
-Cerebellar ataxia
-Pt can not stand with feet together even with eyes open.
-Positive romberg – imbalance with eyes closed
-Testing for sensory ataxia.

Causes of ataxia
• ACUTE
– Brain tumor
– Neuroblastoma
– Head-trauma
– Vertebrobasilar dissection/stroke
– ADEM
– Opsoclonus-Myoclonus-Ataxia
– Acute Cerebellar Ataxia
– GBS
– Tick paralysis
– Infections – encephalitis, cerebellar abscess, ccute labrynthitis
– Toxicities – alcohol, lead, AED
– Conversion reaction
• Intermittent
– Benign paroxysmal vertigo
– Seizure
– Inborn Error of Metabolism
– Basilar migraine
• Chronic
– Congenital anomaly of posterior fossa
• Dandy-walker, chiari, cerebellar dysplasias
– Hereditary ataxias
• Freidrich ataxia, ataxia-telangectasia, Roussy-Levy, spinocerebellar ataxia, episodic ataxias
– Neurodegenerative
• abetaliproteinemia, vitamin E deficiency, Refsum, Niemann-Pick,

Work-up for acute ataxia
• Head imaging – if AMS, focal neurologic signs, cranial neuropathies, marked asymmetric ataxia, trauma, other concerns for mass lesion – posterior fossa symptoms/ elevated ICP symptoms
– MRI is best, especially for posterior fossa lesions, demyelinating
– CT if concern for hydrocephalus, trauma, mass lesions, unstable
• Labs – UDS, alcohol level, BMP (glucose), CSF if concern for infection or GBS. Metabolic evaluation for IEM if needed

Acute Cerebellar Ataxia
• Age 2-5 yo
• Preceded by febrile illness – 4 days to 3 weeks
• Symptoms – acute, maximal at onset – gait disturbance is most common, can also have motor symptoms/fine tremor, dysarthria, 50% have nystagmus
– Some with vomiting and headache in older children
– Should NOT have fever, meningismus, seizure, AMS, focal neurologic signs, insiduous onset
• Differential – toxic/metabolic, infectious—meningitis, encephalitis, ADEM, labrynthitis, structural, metabolic, neurodegenerative, episodic ataxic syndrome.
• Work-up: CSF if fever, meningitic signs, AMS; imaging if trauma, ICP signs, posterior fossa signs, asymetric focal findings, ADEM
• Usually resolves within 2-3 weeks; if worsening or relapse than reconsider diagnosis
• Tx – sometimes steroids, IVIG in severe/refractory cases
• 10% will have some long-term effects, but most recover completely
– older age and EBV associated with worse prognosis.

Opsoclonus-Myoclonus-Ataxia Syndrome
• Dancing eyes – dancing feet
• Mean age – 2 yo.
• Opsoclonus – uncontrolled, frequent, conjugate, saccidic movement of eyes in all directions.
• irritability, sleep problems
• Auto-immune: Paraneoplastic – neuroblastoma (unknown Ab); parainfectious
• Differential: other causes of myoclonus, ataxia; toxic/metabolic dz, structural
• Work-up – Look for neuroblastoma – CAP MRI, VMA/HVA, MIBG scan. If no neuroblastoma, then MRI brain to look for structural, toxic/metabolic, med review, infections – viral (hep C, Lyme, EBV, HIV, coxsackie, rota, mycoplasma, GAS).
• Tx - Treat movements with immunosuppression- steroids, IVIG, rituximab.

Freidrich Ataxia
• AR
• Most common hereditary ataxia – 1:50,000 Caucasian
• Frataxin gene – 9q13 – trinculeotide repeat
• Affects brain, heart, pancreas. Slow onset and progressive.
• Onset before age 25 (often by age 5), ataxia of all 4 limbs, cerebellar dysarthria, absence of LE reflexes, pyramidal signs (weakness, extensor plantars), optic atrophy, brainstem involvement (swallowing dysfunction), early loss of position/vibration without pain/temperature loss, sensineuronal hearing loss
• Cardiomyopathy – 66% of patients – hypertrophic – main cause of death is arrhythmia and heart failure
• Diabetes Mellitus – 33% of patients

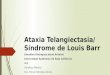
Ataxia-telangectasia
• AR; ATM gene; 11q22.3
• 1:20-100,000
• ATM gene involved in detecting DNA damage, plays role in cell cycle progression
• Neurologic effects
– Progressive cerebellar ataxia (earliest feature; children usual begin walking, then have problems with fluid walking); articulation problems
– abnormal eye movements – oculmotor apraxia is earliest
– Can also have dystonia, chorea, peripheral axonal neuropathy
• Oculocutaneous telangectasias – oculobulbar, nose, face, ear, neck. Appear age 3-5 yo. Also can have cafe-au-lait macules.
• Immune deficiency – recurrent sinopulmonary infections
• Pulmonary disease – major cause of death – recurrent infections, interstitial lung disease, neuromuscular abnormalities (dysphagia, aspiration, resp muscle weakness)
• Malignancy – 10-20% will develop cancer.

PREP QuestionA 4 year old boy presents to the emergency department with balance problems. He had been previously
healthy, but his walking has worsened progressively for the past 2 days, with staggering and lurching.
On PE, the boy is cooperative and alert. His muscles are not tender, and his joints are not red, swollen or tender. His vision seems functionally normal, but there is end-gaze nystagmus in all directions. When sitting independently, his head and trunk bob. His strength appears normal, and his reflexes are normal. When asked to stand with his hands outstretched, a symmetric tremor is evident, and worsens as he approaches this target on finger-to-nose testing. His gait is broad-based. A urine toxicology screen reveals normal results. Brain magnetic resonance imaging shows no tumors or other gray or white matter lesions. Lumbar puncture shows 3 WBCs, 2 RBCs, protein 20, glucose 50.
Of the following, you are MOST likely to advise the child's mother that:
A. Intravenous steroids significantly reduce recurrence risk
B. Neuroblastoma is a common cause of these symptoms
C. Repeat lumbar puncture is needed in 2 days
D. Symptoms may resolve in weeks to months
E. Symptoms usually resolve after antibiotic treatment

D. Symptoms may resolve in weeks to months
-Cerebellar ataxia
-Cerebellar findings on exam: Lateral end gaze nystagmus, dysmetria, ataxia, titubation.
-Subacute onset with normal mental status suggests acute cerebellar ataxia
-Usually acquired after infection or immunization
-MRI shows lesion
-Regarding other choices:
A. Intravenous steroids significantly reduce recurrence risk: They don't
B. Neuroblastoma is a common cause of these symptoms: not as common
C. Repeat lumbar puncture is needed in 2 days: no new information
E. Symptoms usually resolve after antibiotic treatment: Not a primary infectious process

References
-Uptodate articles
http://www.studyblue.com/notes/note/n/pnb-exam-3/deck/107773
http://www.medicinenet.com/image-collection/ataxia_telangiectasia_ear_picture/picture.htm
-maria, b. current management in child neurology.2009
-http://www.78steps.com/examination-sequence/arm-drift.html