Embed Size (px)
Citation preview

1
Pediatric onset Multiple Sclerosis and related Disorders in minority
populations
Tanuja Chitnis M.D.
PARTNERS PEDIATRIC MULTIPLE SCLEROSIS CENTER
Massachusetts General Hospital for ChildrenHarvard Medical School
A TALE of TWO CHILDREN
• Rogier
• Justina
2
Rogier
• Age 10 – left facial droop with 3 T2 MRI lesions• Age 10.4 – right hemiparesis• Age 11 – bilateral leg weakness, requiring crutches
• Age 11.1 – diagnosed with pediatric MS and started on Beta-interferon-1a im
• Family history – no hx MS• Social: Grade 6, some prior learning difficulties, special Ed. • Parents Haitian. Divorced. Born in US. 2 older brothers.
Mother works in hospital
• Neuropsychological testing age 13:• IQ 82• 10-20% most areas on WISC – verbal comprehension, working memory,
processing speed
• IEP plan recommended, but never instituted
Rogier
• 12 years later… - age 23
• Continued Beta-interferon-1a im• 3 relapses mostly in the context of DMT non-adherence• Graduated high school• Completing Associates degree as an electrician in a
community college and working part-time as a security guard
• Girlfriend!
• Challenges:
• Non-adherence to medication• Lack of awareness in school, community• Communication
3
Justina
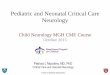
• Age 6 – frequent falls, leg weakness, shaking • Age 7 – regressed to “baby talk”; needed help dressing• Age 7.5 – Couldn’t feel warm water on left arm, MRI
demonstrated multiple brain and spine lesions c/w MS,5 OCB in CSF
• Age 7.5 – diagnosed pediatric MS. Started on beta-interferon-1a sc tiw – transaminitis, non-adherence
• Experienced 3 relapses in 1.5 years most with motor symptoms
• Age 9 – started on natalizumab 6mg/kg –allergic reaction, neutralizing antibodies
• Age 10 – started on rituximab – one moderate relapse with no new MRI lesions
Justina
• Social history: Parents from Puerto Rico Spanish speaking. Patient born in US. ESL. 4th of 6 children. Pre-existing learning disorder and reading delay
• No family history of MS• Many missed appointments – social work involved
• Neuropsychological testing age 10 – IQ 75. WISC scores all areas in 5-15th percentile
• Individualized education plan (IEP) instituted
• Challenges:
• Communication – language, distance, scheduling, multiple providers
• Lack of awareness of MS
4
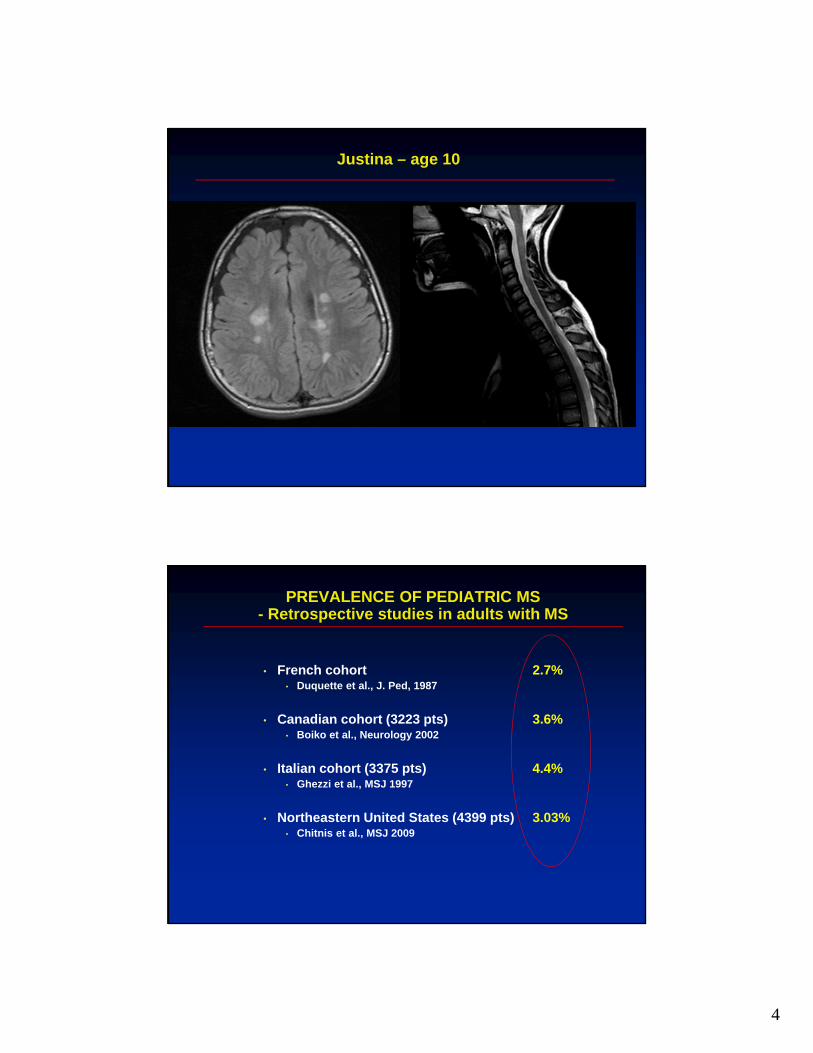
Justina – age 10
PREVALENCE OF PEDIATRIC MS - Retrospective studies in adults with MS
• French cohort 2.7%• Duquette et al., J. Ped, 1987
• Canadian cohort (3223 pts) 3.6%• Boiko et al., Neurology 2002
• Italian cohort (3375 pts) 4.4%• Ghezzi et al., MSJ 1997
• Northeastern United States (4399 pts) 3.03%• Chitnis et al., MSJ 2009

5
PROPORTION OF NON-CAUCASIAN PATIENTS FROM
ADULT AND PEDIATRIC MS CENTERS IN BOSTON
% Caucasian
Pediatric patients 66.7%
(currently under 18 years)
Pediatric onset patients 74%
(under 18y onset - now adults)
Adult onset patients 84.1%
(aged 25-35 years at onset)
Chitnis et al., MSJ 2009
Increased non-European ancestry in pediatric-onset vs. adult-onset MS in greater Toronto area
Kennedy, O’Connor, Sadovnick, Perara, Yee, Banwell - Neuroepidemiology, 2006
6
WORLD-WIDE DISTRIBUTION OF CASE REPORTS OF PEDIATRIC MS
• Argentina• Australia• Austria• Canada• Finland• France• Germany• Italy• India• Iran• Israel• Japan
• Hungary• Malaysia• Netherlands• Norway• Phillippines• Poland• Serbia• Russia• Thailand• Turkey• United States• United Kingdom• Venezuela
U.S. Network of Regional Pediatric MS Centers and the Data Coordinating and Analysis Center at the University of
Utah
Sponsored by the National MS Society
CHBMGH
Mayo ClinicLoma Linda
SUNY-StonybrookSUNY-Buffalo
Texas Childrens UAB
UCSF
7
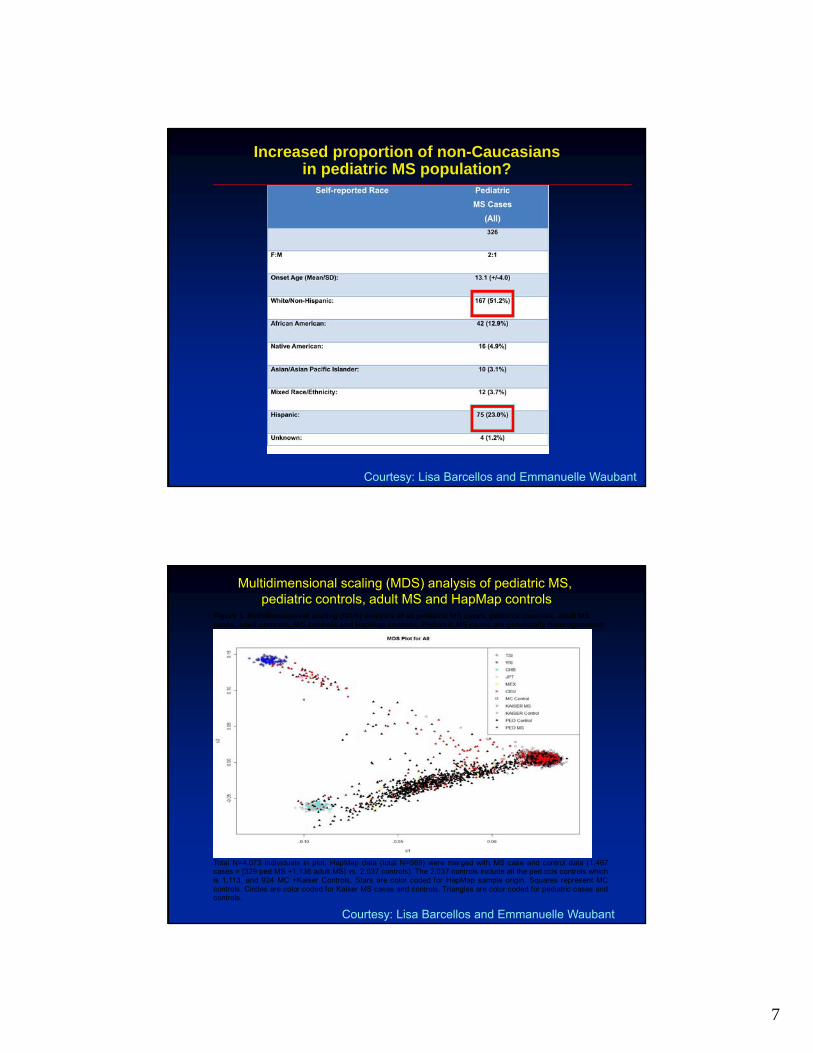
Increased proportion of non-Caucasians in pediatric MS population?
Courtesy: Lisa Barcellos and Emmanuelle Waubant
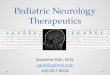
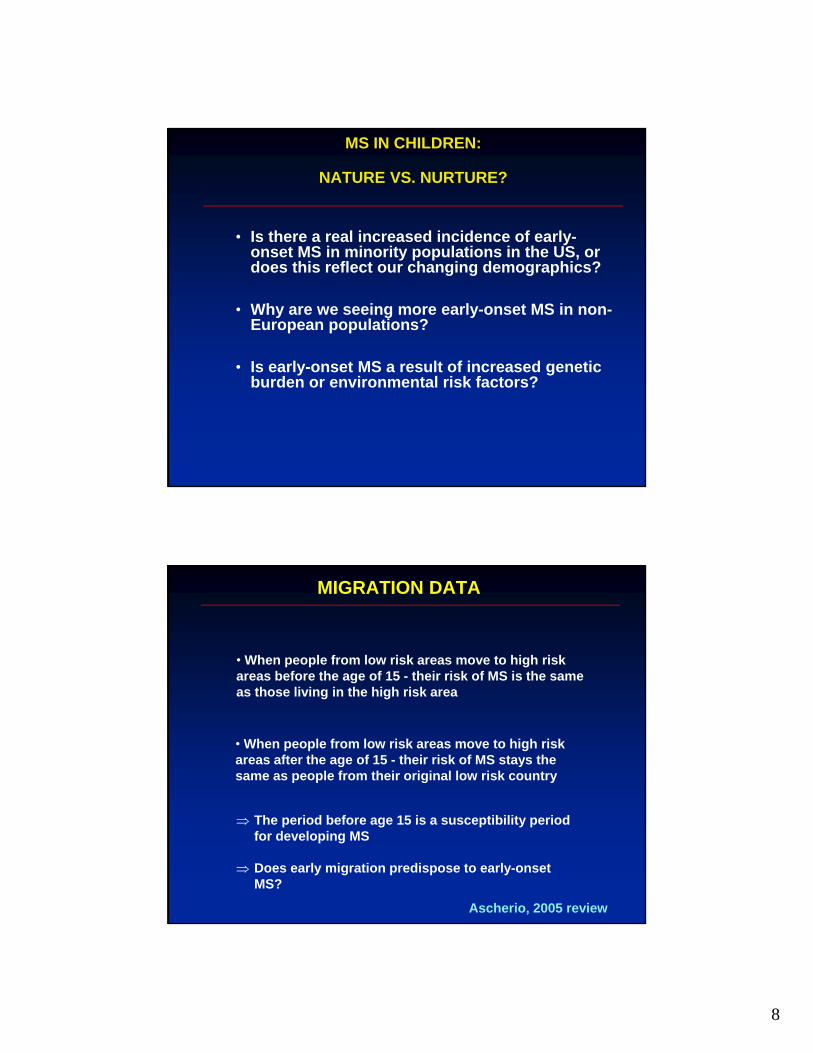
Figure 1. Multidimensional scaling (MDS) analysis of all pediatric MS cases, pediatric controls, adult MS cases, adult controls, MC controls and HapMap controls. Pediatric MS cases are genetically heterogeneous!
Total N=4.073 individuals in plot. HapMap data (total N=569) were merged with MS case and control data (1,467 cases = [329 ped MS +1,138 adult MS] vs. 2,037 controls). The 2,037 controls include all the ped ccls controls which is 1,113, and 924 MC +Kaiser Controls. Stars are color coded for HapMap sample origin. Squares represent MC controls. Circles are color coded for Kaiser MS cases and controls. Triangles are color coded for pediatric cases and controls.
Multidimensional scaling (MDS) analysis of pediatric MS, pediatric controls, adult MS and HapMap controls
Courtesy: Lisa Barcellos and Emmanuelle Waubant
8
MS IN CHILDREN:
NATURE VS. NURTURE?
• Is there a real increased incidence of early-onset MS in minority populations in the US, or does this reflect our changing demographics?
• Why are we seeing more early-onset MS in non-European populations?
• Is early-onset MS a result of increased genetic burden or environmental risk factors?
MIGRATION DATA
• When people from low risk areas move to high risk areas before the age of 15 - their risk of MS is the same as those living in the high risk area
• When people from low risk areas move to high risk areas after the age of 15 - their risk of MS stays the same as people from their original low risk country
The period before age 15 is a susceptibility period for developing MS
Does early migration predispose to early-onset MS?
Ascherio, 2005 review
9
ENVIRONMENTAL RISK FACTORS
• Pre-pubertal susceptibility factor to MS demonstrated by multiple migration studies
• Increased proportion of children of ethnic backgrounds with MS compared to adult cohort, suggesting place of residence is major risk factor
(Banwell, Neuroepidemiology, 2006)
• Serological evidence for remote EBV infection in pediatric MS patients vs. controls
• 83% MS, 42% controls (Aloitaibi et al., JAMA 2004)• 99% MS, 72% controls (Pohl et al, Neurology 2006) • 86% MS, 64% controls (Banwell et al., Lancet 2007) • 88% MS, 56% controls (Lunemann, Neurology 2008)
• Parental cigarette smoking increases MS risk in children (RR=2.12)(Mikaeloff et al. Brain 2007)
• Decreased Vitamin D levels in patients under 20 years of age correlated with MS susceptibility
(Munger and Ascherio, JAMA 2006)
• Vitamin D levels correlated with relapse rate in children with MS(Waubant et al, Annals of Neurology, 2010)
Obesity in MS
• Women who are obese (BMI>30kg/m2) at the age of 18 had a greater than two-fold increased risk of MS compared to those with normal BMI (Munger, Neurology 2009)
• Obese girls are twice as likely to develop MS as normal weight girls (Langer-Gould, Neurology 2013)
• Childhood obesity was associated with 2X risk of MS in females only (Munger, MSJ 2013)
• Obesity in women is associated with relapsing-onset MS (Marrie, Acta Scandivania 2011)
10
Risk factors for MS- are minorities increasingly susceptible?
Risk factor
� Smoking
� Vitamin D deficiency
� Epstein-Barr
virus exposure
� Obesity
Genetic/epigenetic interactions?
NIH-sponsored study –Environmental and Genetic risk factors in pediatric MS
• Target enrollment 500 children with MS from 15 pediatric MS Centers in US
• 1500 age and sex and center-matched controls
• Environmental and dietary exposures questionnaire
• DNA and serum sample
• www.clinicaltrials.gov
•
11
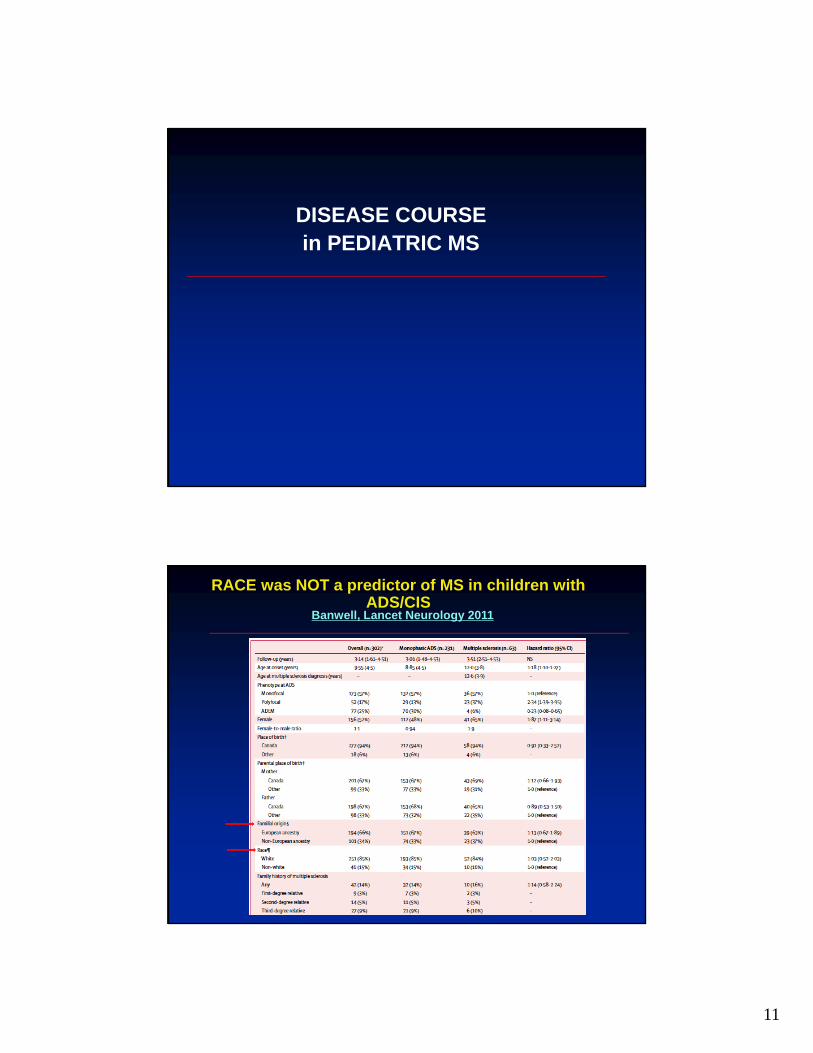
DISEASE COURSE in PEDIATRIC MS
Banwell, Lancet Neurology 2011
RACE was NOT a predictor of MS in children with ADS/CIS
12
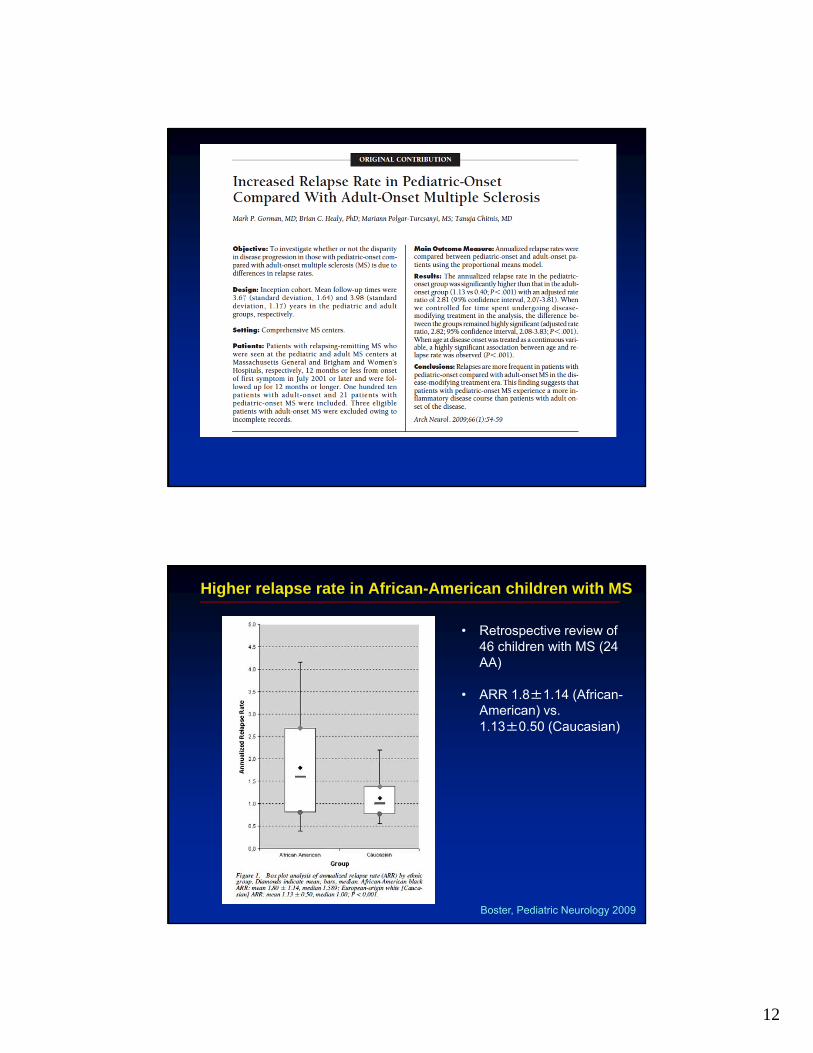
Higher relapse rate in African-American children with MS
• Retrospective review of 46 children with MS (24 AA)
• ARR 1.8±1.14 (African-American) vs. 1.13±0.50 (Caucasian)
Boster, Pediatric Neurology 2009
13
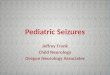
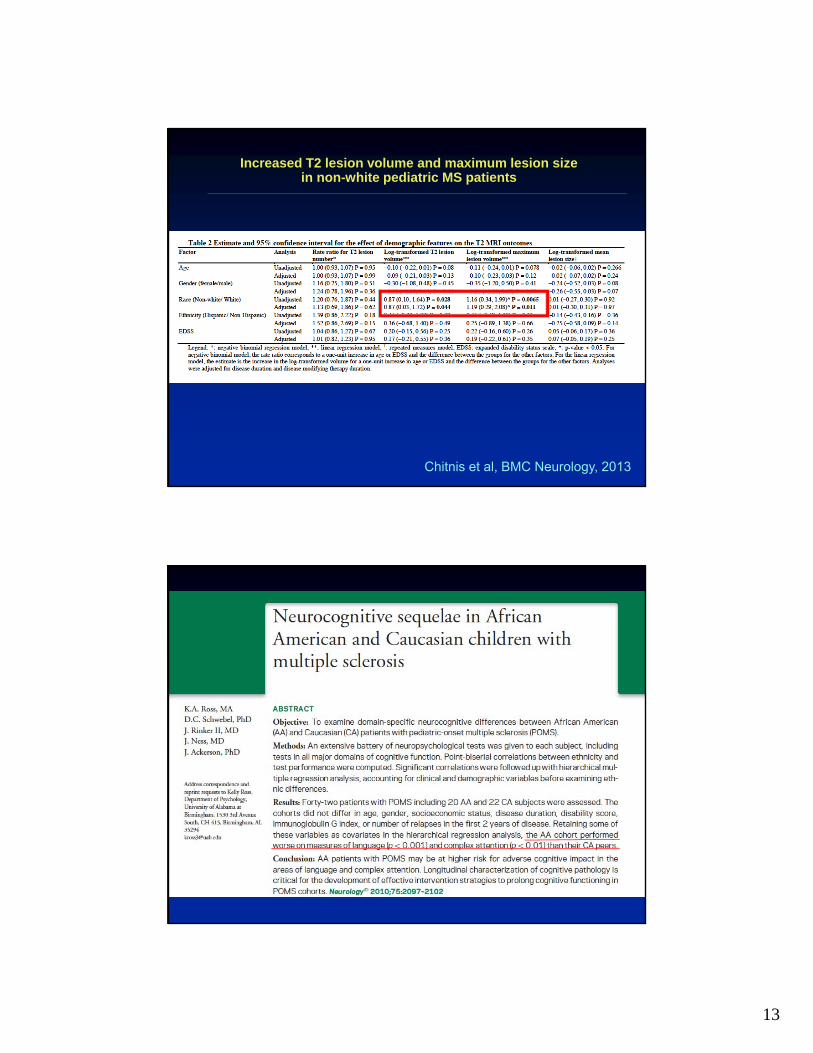
Increased T2 lesion volume and maximum lesion size in non-white pediatric MS patients
Chitnis et al, BMC Neurology, 2013
14
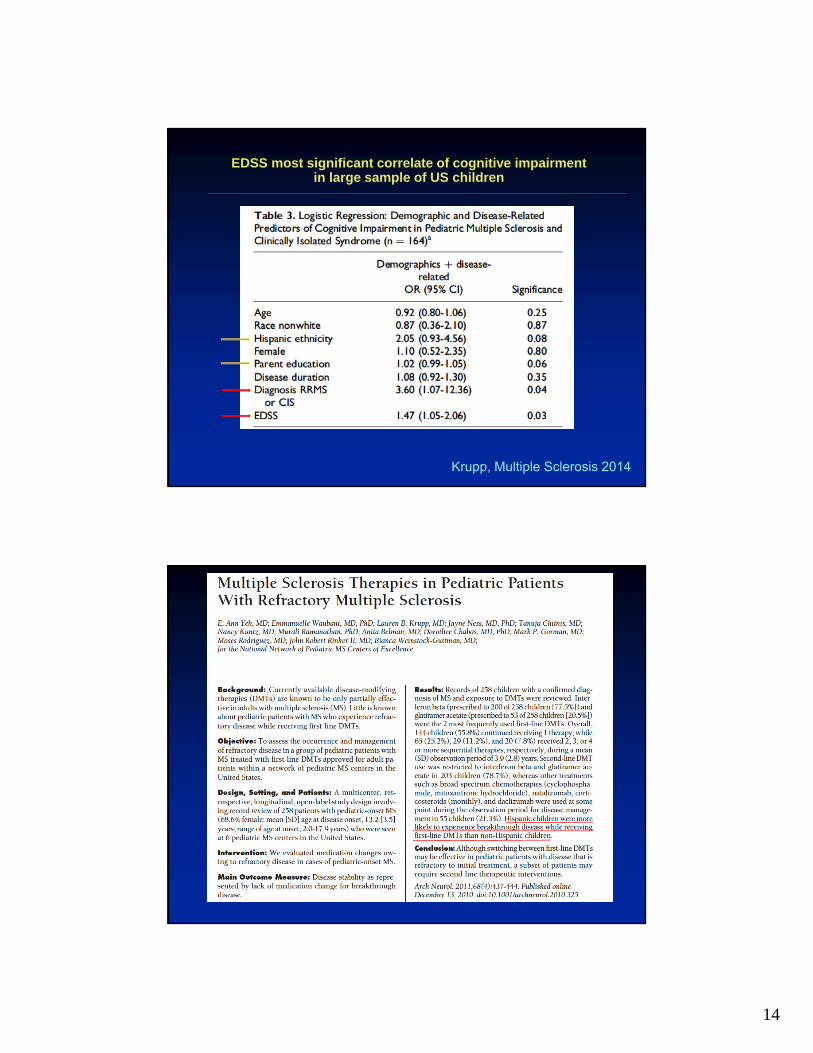
EDSS most significant correlate of cognitive impairment in large sample of US children
Krupp, Multiple Sclerosis 2014
15
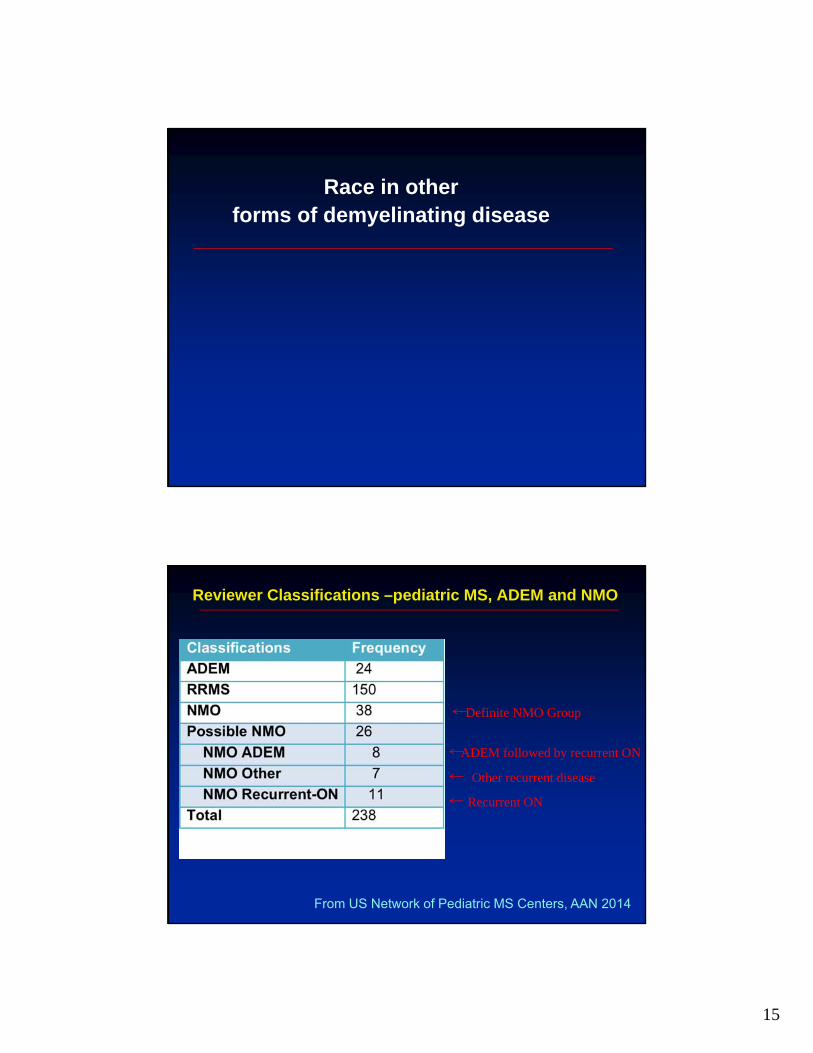
Race in other forms of demyelinating disease
Reviewer Classifications –pediatric MS, ADEM and NMO
Definite NMO Group
ADEM followed by recurrent ON
Recurrent ON
Other recurrent disease
From US Network of Pediatric MS Centers, AAN 2014
16
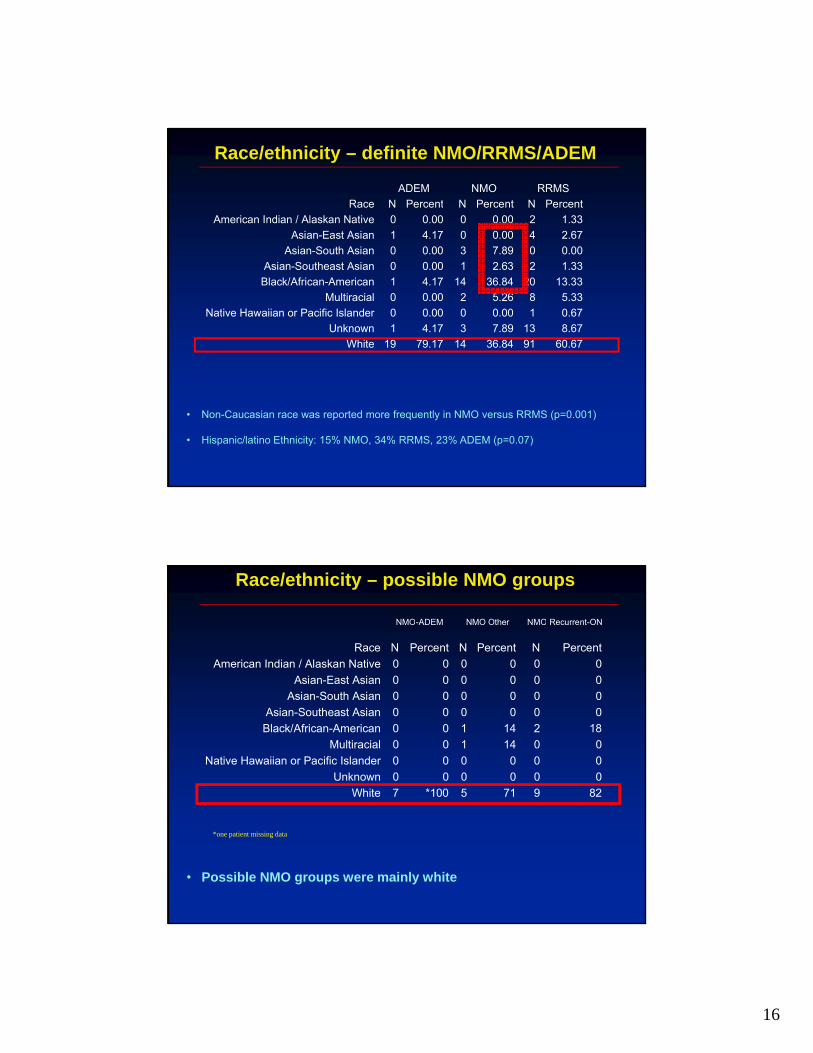
Race/ethnicity – definite NMO/RRMS/ADEM
• Non-Caucasian race was reported more frequently in NMO versus RRMS (p=0.001)
• Hispanic/latino Ethnicity: 15% NMO, 34% RRMS, 23% ADEM (p=0.07)
ADEM NMO RRMS
Race N Percent N Percent N Percent
American Indian / Alaskan Native 0 0.00 0 0.00 2 1.33
Asian-East Asian 1 4.17 0 0.00 4 2.67
Asian-South Asian 0 0.00 3 7.89 0 0.00
Asian-Southeast Asian 0 0.00 1 2.63 2 1.33
Black/African-American 1 4.17 14 36.84 20 13.33
Multiracial 0 0.00 2 5.26 8 5.33
Native Hawaiian or Pacific Islander 0 0.00 0 0.00 1 0.67
Unknown 1 4.17 3 7.89 13 8.67
White 19 79.17 14 36.84 91 60.67
NMO-ADEM NMO Other NMO Recurrent-ON
Race N Percent N Percent N Percent
American Indian / Alaskan Native 0 0 0 0 0 0
Asian-East Asian 0 0 0 0 0 0
Asian-South Asian 0 0 0 0 0 0
Asian-Southeast Asian 0 0 0 0 0 0
Black/African-American 0 0 1 14 2 18
Multiracial 0 0 1 14 0 0
Native Hawaiian or Pacific Islander 0 0 0 0 0 0
Unknown 0 0 0 0 0 0
White 7 *100 5 71 9 82
Race/ethnicity – possible NMO groups
• Possible NMO groups were mainly white
*one patient missing data
17
SUMMARY
•Pediatric MS in minorities may pose unique challenges – language, cultural, awareness, educational
•There is mounting evidence suggesting an increased proportion of non-Caucasian representation amongst pediatric MS patients compared to adult MS
• Definitive epidemiological studies need to be conducted (referral bias, immigration trends)
• Does this reflect an increased incidence of MS amongst non-Caucasians in general?
• Nature vs. nurture?
SUMMARY
• Some evidence of increased severity of MS (relapses, MRI lesion volume) amongst non-Caucasian pediatric MS patients
• Poorer response to first line DMT in hispanicpediatric MS patients
• Does this reflect the observations that non-Caucasians experience a more severe course of MS in general (including earlier onset?)
• Referral bias?
• Cognitive impairment linked to disease severity

18
SUMMARY
• Race was not associated with conversion of CIS to MS
• However differences in race/ethnicity proportions in pediatric MS, NMO and other forms of recurrent demyelinating disease
WAY FORWARD
• Increase awareness of demyelinating diseases in non-Caucasian patients and communities
• Increased availability of literature in non-English languages
• National and international collaborative studies on environmental/genetic influences which include race
• Harmonization of terminology of race (international)
• Participation of all patient groups in research studies, especially genetic research
19
THANK YOUPatients and their families