Embed Size (px)
Citation preview
8/11/2019 Peds33+34_Cyanotic and Acyanotic Heart Diseases
http://slidepdf.com/reader/full/peds3334cyanotic-and-acyanotic-heart-diseases 1/11
33-34
yanotic & Acyanotic
Heart Diseases
Eyad Amouri
Shakeeb & Sakher
21 / 12 / 2009
8/11/2019 Peds33+34_Cyanotic and Acyanotic Heart Diseases
http://slidepdf.com/reader/full/peds3334cyanotic-and-acyanotic-heart-diseases 2/11
8/11/2019 Peds33+34_Cyanotic and Acyanotic Heart Diseases
http://slidepdf.com/reader/full/peds3334cyanotic-and-acyanotic-heart-diseases 3/11
Page 2 of 10
Shunt lesions could also be classified to:
Left to right shunt.
Right to left shunt (Cyanotic heart disease).
Left to Right shunt:
- Types: ASD, VSD, PDA.
- Red blood goes to the lung.
-
Ineffective circulationbecause the blood is fully oxygenated, when it goes back
to the lungs, all what it will do is just volume overload at the lungs.
- Doesn’t cause cyanosis because there is Left to Right shunt not Right to Left,
so the shunt doesn’t affect the blood oxygenation.
-
VSD and PDA is the same story.
Aas we said, the amount of blood that goes to the lungs is called ineffective blood flow.
The effective blood flow is calculated by the ratio between the pulmonary blood flow (the amount that
goes to the lungs) and the systemic blood flow (the amount that goes to the body).
Physiology of ASD:
-
It’s usually asymptomatic. - Cardiac output is normal because the heart will do his best to compensate
normal Cardiac output, but it will increase the pulmonary flow.
- L. atrium, R. atrium, R. ventricle, and Pulmonary artery will complain of
dilation, while the L. ventricle will not.
- There will be fixed splitting of S2.
- There will be also R. ventricle heave because of dilation.
- There is also Ejection murmer.
- X- Ray will show R. artrial dilation lateral X- Ray will show R. ventricle against
the sternum because of dilation.- There will be no shifting of the apex.
- Some patients may present as “Failure to thrive”.
- If the patient has Asthma and ASD, it will make symptoms of Asthma become
worsen.
- Congestive Heart Failure will not happen.
- In older children they may complain of dyspnea on exercise
8/11/2019 Peds33+34_Cyanotic and Acyanotic Heart Diseases
http://slidepdf.com/reader/full/peds3334cyanotic-and-acyanotic-heart-diseases 4/11
Page 3 of 10
- Pulmonary Hypertension almost never happens because it is a low pressure
shunt.
- Some older children may present with SVT, Artrial or Ventricular tachycardia.
- Pneumonia presents with more sever symptoms because of increased
pulmonary blood flow, but there is no relation between ASD and Pneumoniaprogression.
- Upon ECG: () Signs of Right axis deviation.
() Signs of Right arterial dilation.
() Signs of Right ventricular dilation.
() Arrythmias.
- Upon X- Ray: () Plethoric lungs. (increase in vascular markings).
() Cardiomegaly due to Right atrial dilation.
- Echocardiogram is the diagnostic tool.
- There is no management except surgical methods (closure of the defect).
- There are no medications that could treat ASD, and there is no need for
Bacterial Endocarditis prophylaxis.
Physiology of VSD:
- Is the communication between Right and Left ventricles.
-
Red blood goes to the Right ventricle.
- Types: () Perimembranous (most common). We know from anatomy that
ventricle’s septum is mostly muscular except a small part underneath the
aortic valve is membranous.() Membranous (2
nd common), which is a muscular defect in any part
of ventricular septum.
() Anlet (3rd common), or AV canal. Its common in patients with
trisomy 21.
() Subpulmonary defect which is the rarest type.
- Newborns are asymptomatic because the pulmonary vascular resistance is
high when they are born and this takes about 4-8 weeks to become as adults,
So, the left to right shunt is minimal in the newborn age.
- If the VSD is large enough, then there will be an increase in the pulmonary
blood flow and this will cause left ventricular and left arterial dilation, and
eventually Heart Failure because when the left ventricle become dilated
according to “frank- starling law” when it becomes dilated to an extent the
heart contractility will drop down and the heart could not compensate
anymore, so the cardiac output will become aggressively low,,, as a result,
Heart Failure could occur.
8/11/2019 Peds33+34_Cyanotic and Acyanotic Heart Diseases
http://slidepdf.com/reader/full/peds3334cyanotic-and-acyanotic-heart-diseases 5/11
Page 4 of 10
- Babies with Heart Failure present with symptoms that differs from thes in
adults. Symptoms are : RS symptoms, Excessive sweating, and the most
important one is weight loss.
- Heart murmers may not be present in 1qst day of life because –as we said-
the pressure is almost equal in both ventricles because the pulmonarypressure is high. So, there is no turbulence in the blood flow across VSD, but
murmers usually appear after the age of 1 day, and its of pansystolic murmer
type.
- Definitely, the apex beat will be shifted due to Left ventricular hypertrophy.
- If we have a small VSD, we’ll have a pansystolic murmer, but we call it short
systolic murmer because it disappears before s2, .
- We’ll have also a loud S2, because there is pulmonary hypertension and that
will cause loud P2 not A2.
- We may hear also a disystolic murmer because of excessive flow across a
normal mitral valve.
- S3 gallop presents with patients with Heart Failure.
- Asymptomatic (small) VSD doesn’t need any intervention, it closes
spontaneously.
- For symptomatic VSD, we eliminate the symptoms or close it by surgical
intervention.
- In VSD also we don’t give patients SBE prophylaxis.
Coaroctation of the Aorta:
- Non- shunt obstructive lesions.
- The obstruction is in the distal part of the aortic arch just distal to the left
subclavian artery and because there is obstruction there, the heart starts to
pump at a high pressure in order to perfuse the lower extremities. So there
will be a hypertension in the upper extremities and normal or low pressure in
the lower extremity there will be left jugular hypertrophy.
- The apex beat will be dilatedand eventually there will be a collateral blood
flow across the area of obstruction.
Physiology of PDA:
- Communication between the aorta and the pulmonary artery.
- Causes some changes like VSD.
- The only difference between PDA and VSD is in the Blood pressure, it causes
wide pulse pressure.
8/11/2019 Peds33+34_Cyanotic and Acyanotic Heart Diseases
http://slidepdf.com/reader/full/peds3334cyanotic-and-acyanotic-heart-diseases 6/11
Page 5 of 10
CYANOTIC HEART DISEASES
Cyanosis: it’s bluish discoloration of the lips, it happens when there is clinically significant amount ofdeoxygenated hemoglobin and usually that’s about 3-4 g/dl in order to see the cyanosis by your eys, so
if the Hb of individual is 15, and you need 5g of deoxy Hb, so the saturation should be less than 70% in
order to see cyanosis.
Cyanosis is a clinical sign seen by your eyes.
Desaturation is not a clinical sign seen by your eyes, its actually calculated by saturation that you
measure, So not every hypoxemic patient may present with cyanosis.
Especially in children, they usually have Hb of 10, So they need to be 60% desaturated in order to seethe cyanosis.
The major cause of cyanosis in children is pulmonary causes.
Pulmonary causes:
1- Air way diseases: pneumonia, asthma, foreign body.(anything prevent the air getting
in).
2-
Hypoventilation: central causes.
3- Intrapulmonary circulation: the blue blood crosses to the red blood areas.
Cardiac causes of cyanosis is always secondary to intracardiac shunt which is the blue blood going to red
blood areas this is the cause of cardiac cyanosis.
The other rare causes like methmoglobinemia.
Cardiac causes:
1- Right to left shunt: blue blood going to the left side of circulation, so this is pure right
to left shunt. Eg: TOF.
2-
Mixing: both blue and red blood mix together in a chambers and there is distributedto the lungs and the body.
3- Recirculation: the whole red blood going to right side of circulation(pulmonary
artery), and the blue blood going to the left side of circulation(to the body). That
what happens in TGA. The left ventricle pumping blood to the lungs and the right
ventricle pumping blood to the body, so the pulmonary arterial circulation is 100%
saturated, and the systemic arterial circulation is 50%.
8/11/2019 Peds33+34_Cyanotic and Acyanotic Heart Diseases
http://slidepdf.com/reader/full/peds3334cyanotic-and-acyanotic-heart-diseases 7/11
Page 6 of 10
So Cyanotic Heart Diseases:
- To diagnose cyanotic heart diseases, approach should include full history to
rule in and out.- We do also physical examination, and some tests are used to help in diagnosis
as Chest radiograph, ECG, and Hyperoxygenation test, but non of them is a
diagnostic tool for the lesion itself. BUT the only test that is diagnostic is the
Echocardiogram.
- Hyperoxygenation test: is a test performed by giving the patient 100% o2 to
overcome the cyanosis, if the patient become well, then he has a respiratory
problem, but if not, he has a cardiac problem. Y3NI, we give the patient 100%
O2 and take an ABG, if PO2 is more than 250 then usually the cause is
respiratory, but if PO2 is less than 150 then the cause is cardiac.- Cyanotic Heart Diseases are: Tetralogy of Fallot, Transposition of great
vessels, Truncus Arteriosus, Total Anomalus, and Tricuspid Atresia.
Tetrology of Fallot
- Components are: 1- VSD. 2- Pulmonary Atresia. 3- Aortic override. 4- Right
Ventricular hypertrophy.
- Most common cyanotic heart disease.
- 3rd
most common overall.
- 10% of congenital heart diseases.
- Etiology: There is no certain cause of TOF, but it usually presents with some
syndromes as: Down’s, De Lange, Klippel- Feil, and others.
- Physiology: () Depends in 2 factors; VSD and Pulmonary artery
obstruction. So if the patient doesn’t have Pulmonary stenosis, then its VSD
not TOF. Y3ni TOF without pulmonary stenosis IS VSD.
() Pulmonary stenosis differs from a patient to another, and
its progressive with time, Y3ni, at one month of age, it will
be moderate, at six months it become severe, Y3ni thepatient becomes more cyanotic with time.
() There is equal pressure in both ventricles.
() Flow depends on the difference between systemic and
pulmonic outflow resistance.
8/11/2019 Peds33+34_Cyanotic and Acyanotic Heart Diseases
http://slidepdf.com/reader/full/peds3334cyanotic-and-acyanotic-heart-diseases 8/11
8/11/2019 Peds33+34_Cyanotic and Acyanotic Heart Diseases
http://slidepdf.com/reader/full/peds3334cyanotic-and-acyanotic-heart-diseases 9/11
Page 8 of 10
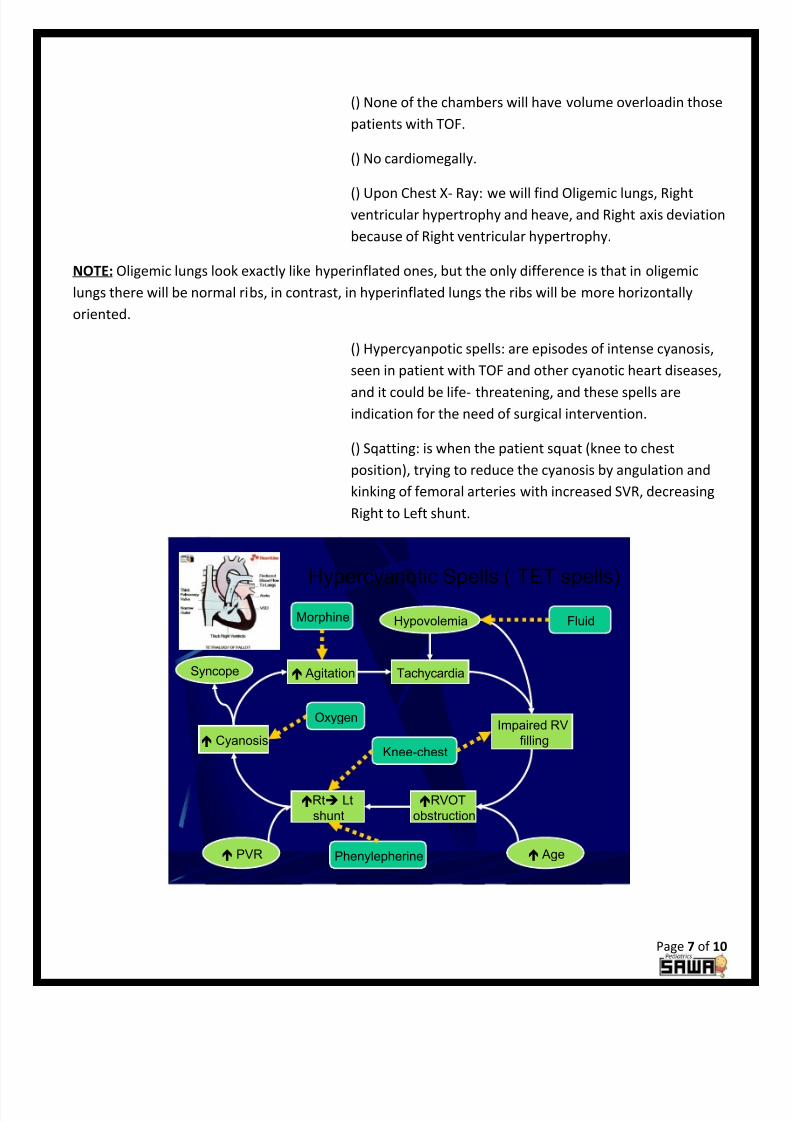
- Chest X- Ray: reveals normal heart size, but an abnormal shape, y3ni the
patients will have what is called “boat shaped” heart, and upturned apex, and
there is a concavity in the area of the pulmonary artery.
- Patients are polycythemic , and it is a secondary mechanism to hypoxia.
-
If the Hct more than 60% might have symptoms of hyper viscosity syndromes.- Surgical management is required by closure of VSD.
Transposition of Great Vessels
- The Aorta originates from the R ventricle, and the Pulmonary artery originates
from the Left one.
- So the blue and the red blood keep going to the same area. Now, in able to
the patient to survive, there must be a comminucation between the two
“bloods” at the arterial level. Y3ni usually its essential to these patients to
have ASD or Foramen ovale to survive.
- Presents in about 5-7% of all cyanotic heart diseases.
- 50% of the patients may present with VSD but this doesn’t contribute in the
pathology of the disease.
- Usually the symptoms appear at the 1st
few hours of life, so cyanosis at the 1st
few hours of life indicates TGV rather than TOF.
- Chest X- Ray shows “egg on sting” heart shape, and there will be also narrow
mediastinum because the pulmonary artery and the aorta are “front and
back” not “side by side”. 6ab3an these findings appear when it the patient left
untreated.
- So if the patient presents with profound cyanosis at birth, there are number
of things that we can do before surgical intervention. One thing is to ensure
that is a Right to Left shunt (mixing at the arterial level) and also to ensure
that there is a pulmonary blood flow that is blue, so we need blue blood to go
to the lungs, and what we do is to keep PDA because the PDA will allow blood
from the Aorta to the pulmonary artery and this blood is blue, so that blue
blood will go to the lungs and this is the effect of circulation. So when more
blood goes to th lungs, more blood is coming to the atrium fully saturated, so
the pressure will be more than in the right atrium, and ASD now will function
as effective systemic opening, So the blood will cross from the left atrium to
the right atrium which has red blood that goes to the body. So one is we have
to keep the PDA opening by using PGE-@ infusion, if that doesn’t work then
we have to do an opening at the arterial septum by a Ballonatrial septostomy.

8/11/2019 Peds33+34_Cyanotic and Acyanotic Heart Diseases
http://slidepdf.com/reader/full/peds3334cyanotic-and-acyanotic-heart-diseases 10/11
Page 9 of 10
Truncus Arteriosus- Is a common trunk arises from both ventricles. An important point that there
is no TA without VSD, but we don’t call it VSD.
- 1.2-2.5% of all congenital heart disease
-
Generally patients have increased pulmonary blood flow
- Degree of cyanosis is mild and may not be evident clinically until late stage
with pulmonary vascular disease
- Upon examination we find Single S2, Ejection click of the abnormal truncal
valve , Systolic murmur of truncal valve stenosis if present, Diaastolic murmur
of truncal valve insufficiency, and Gallop.
- Upon Chest X-Ray we find: Cardiomegally, increased pulmonary circulation.
-
Acute management of TA: is not to give the patient O2 in order to minimize
pulmonary blood flow, Give diruitics.
-
Surgical management: complete repair with VSD closure and conduit
placement between the right ventricle and pulmonary arteries.
Tricuspid Atresia- Here there is no tricuspid valve, so there is no communication between the
right atriem and the right ventricle.
- About 3 % of congenital heart disease
- Usually associated with VSD
-
The pulmonary blood flow is dependent on the size of the VSD- Pulmonary blood flow can be increased or decreased causing variable
presenting symptoms
- If there is no VSD ( also called Hypoplastic right ventricle) the pulmonary
blood flow is dependent on the PDA
-
The presentation of the disease depends on the amount of pulmonary blood
flow; if it decreased, then the main presenting symptom is cyanosis. BUT if it
increased, the presentation is that of congestive heart failure.
- Chest X-Ray reflects the amount of pulmonary blood flow.
-
ECG reveals LEFT AXIS DEVIATION. (V. IMPORTANT).
8/11/2019 Peds33+34_Cyanotic and Acyanotic Heart Diseases
http://slidepdf.com/reader/full/peds3334cyanotic-and-acyanotic-heart-diseases 11/11
Page 10 of 10
Management
PBF
Decreased Increased
PGE-1, and minimal
supplemental O2 to
maintain ductal
patency
No O2
Afterload
reduction
Diuretics
Total Anomalous Pulmonary Venous Return
(TAPVR)- Rarest cyanotic heart disease.
-
Pulmonary veins coming to the left atrium missed the left atrium, the go to
the right one to communicate either with abnormal vein or directly to theright atrium, So the pulmonary veins which has red blood goes to the superior
vena cava and to right atrium or Inferior vena cava to the right atrium. So all
the blood will be mixed in the right atrium, so again this is a complete mixing.
The blood can’t go to the left ventricle except through an ASD. So the blood
will be distributed to the circulation through ASD.
---THE END---
www.sawa2006.com