Embed Size (px)
Citation preview

Journal of Neurology, Neurosurgery, and Psychiatry 1983;46:632-638
Physiologic and prognostic significance of''alpha coma"VICENTE J IRAGUI, CHARLOTTE B McCUTCHEN
From the Department ofNeurosciences, University of California, San Diego and the VeteransAdministration Medical Center, San Diego, California, USA
SUMMARY A patient with posthypoxic "alpha coma" is described whose EEGs were recordedbefore coma, within two hours following the onset of coma and after recovery. The differencesobserved between the alpha activity during coma and that seen before and after suggest that thealpha activity during coma and the physiologic alpha rhythm are different phenomena. This case,
as well as others reported, also suggests that "alpha coma" resolving in the first 24 hoursfollowing hypoxia may have a better prognosis than "alpha coma" detected after the first day,and stresses the need for EEG monitoring begun in the immediate period following hypoxia inorder to assess accurately the prognostic significance of this EEG pattern in the early stages ofpostanoxic encephalopathy. The aetiology of "alpha coma" also affects outcome. The survivalrate appears higher in patients with respiratory arrest than in those with combined cardiopulmo-nary arrest.
"Alpha coma" was first described in patients withbrainstem lesions'-'6 and later in patients with post-hypoxic coma'3-1S 17-27 and coma from drug over-dose.'4 28-31 With a few notable exceptions,2 12 28 theEEG prior to the onset of coma has not been avail-able, and it remains uncertain whether this patternrepresents a retained physiological alpha rhythm oris an abnormal pattern.'3 The prognosis of "alphacoma" has been generally considered to bepoor,132' 2227 although some patients have experi-enced partial or complete recovery.4 22-31 In mostinstances, however, EEGs with alpha patterncoma have been recorded several hours or daysafter the onset of coma, and recordings during thefirst few hours of coma are scarce. This is particu-larly relevant since the time of recording is critical inassessing the prognostic significance of EEG pat-terns following cerebral hypoxia.'2'4 The followingis a case report of a patient who recovered fromposthypoxic "alpha coma" on whom we had theopportunity to record EEGs prior to the hypoxicepisode, within two hours of the onset of coma, and
Address for reprint requests: Dr Iragui, Department of Neurosci-ences (M-008), University of California at San Diego, La Jolla,California 92093, USA.
Received 17 June 1982 and in revised form 20 December 1982.Accepted 7 February 1983
after recovery. The available literature is reviewedin the light of this observation.
Case report
A 64-year-old man with hypertension and severe wide-spread arteriosclerotic vascular disease suffered several2-3 minute episodes of transient loss of consciousness in1977. Two EEGs eight months apart were performed thatyear. The tracings (fig 1) showed well modulated 40-50,uv, 10 Hz activity confined to the occipital, parietal andposterior temporal regions of both hemispheres that wasattenuated by eye opening. Generalised rhythmic 30-40,uv beta activity was also noted, and was thought to berelated to 15 mg oral diazepam that the patient was receiv-ing daily. During Stage I of sleep, the alpha activity sub-sided and generalised rhythmic 20-30 v, 4-7 Hz activityappeared, most prominent over the fronto-central regions.During Stage II of sleep, physiological vertex waves as wellas symmetrical 14-15 Hz sleep spindles were present.Hyperventilation elicited no significant change, and photicstimulation resulted in no consistent photoentrainment.
During the ensuing years, he developed unstable anginaand suffered five myocardial infarctions. In December of1980, he had a new myocardial infarction accompanied bycongestive heart failure and acute pulmonary oedema. Hereceived immediate care and during attempts at endo-tracheal intubation he became unresponsive. Examinationone hour later showed him to be comatose, perspiring pro-fusely and agitated with a respiratory rate of 35/min, pulse90/min and blood pressure of 180/110 mm Hg. He did notfollow commands or open his eyes to auditory stimulation,
632
group.bmj.com on September 14, 2016 - Published by http://jnnp.bmj.com/Downloaded from

Physiologic and prognostic significance of "alpha coma" 633
S.'~~~~~~~~~~~~~~~r
1...~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~4,
77-50O9 Eyes opened Eyes cbosedFig 1 LEG performed prior to "alpha coma" showing a posteriorly distributed alpha rhythm that attenuates witheye opening. Time constant: 1 s. High frequency filter (-3 dB): 70Hz.
0 -
o 0
I,,+
77-5079Eeon50,ucV80-9128 Pinch left arm is
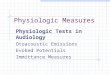
Fig 2 EEG performed within two hours after the onset ofcoma showing widespread unreactive alphaactivity, maximal anteriorly as well as theta and delta potentials, maximal on the left side. Prominent headmovement artifact from laboured respirations arising from the left occipito-parietal region obscured someportions of the tracing. The patient was perspiring profusely and sweat artifact is also present. Timeconstant: 1 s. High frequency fiter (-3 dB): 70 Hz.
group.bmj.com on September 14, 2016 - Published by http://jnnp.bmj.com/Downloaded from

4,D--o4,'
4 3
_ _ _ _ _ __ _ _
81 -460 X 6 Eyes opened Eyes closed isFig 3 EEG after recovery showing posteriorly distributed, reactive alpha rhythm. Irregular theta and delta activity is mostprominent in the left temporal area. Time constant: 1 s. High frequency filter (-3 dB): 70 Hz.
and he responded to pain only with incomprehensiblesounds and withdrawal. His Glasgow Coma Scale rating35was 6. Pupils were equal and reacted normally to light.Roving conjugate horizontal eye movements were presentand the oculocephalic responses were normal. Corneal andgag reflexes were present. The muscle tone was normal,and all extremities exhibited withdrawal to painful stimula-tion. Muscle stretch reflexes were normal, and there wereflexor plantar responses bilaterally. The EEG performedwithin two hours of the onset of coma (fig 2) showedrhythmic, 20-30 uv, 11-12 Hz activity with generaliseddistribution, but more prominent anteriorly and of slightlygreater amplitude on the right side. This activity was fairlyconstant in amplitude and frequency, and did not changewith painful stimulation, auditory stimulation or passiveeye opening. A moderate amount of irregular, 20-40 ,uv,2-5 Hz potentials were also seen that, although general-ised, had lower amplitude over the left centro-patietalregion. 20-60 gv, 0.5-1 Hz potentials were present maxi-mally over the left centro-parietal region. Shortly aftercompletion of the EEG, the patient underwent endo-tracheal intubation. He remained in coma for the next fourhours. Subsequently, he exhibited gradual improvement,and twelve hours after the onset of coma he was alert andable to open his eyes to command. He followed only simpleinstructions and did not talk. He also had a moderate righthemiparesis as well as a right extensor plantar response,and was believed to have suffered a left hemisphericinfarct. An EEG performed at that time showed general-ised fairly rhythmic 20-40 ,v, 6-7 Hz theta activity. Rarepotentials of 20-30 Av and 11-12 Hz were also presentdiffusely. In addition, polymorphic 20-40 ,uv, 1-3 Hz deltapotentials were prominent over the left temporal region.The patient showed progressive neurological improve-
ment, and six months later his residual deficit was anonfluent aphasia and he was moderately disabled accord-ing to the Glasgow Outcome Scale.36 EEGs performed twoand six months after the onset of coma (fig 3) showed analpha rhythm of 20-40 ,uv and 9-10 Hz confined to theoccipital, parietal and posterior temporal regions of bothsides. This activity was attenuated by eye opening, painfulstimulation and auditory stimulation. A small amount ofirregular low to medium voltage 6-7 Hz theta activity wasalso present diffusely. Low to medium voltage irregular1-3 Hz delta activity was detectable over the left hemi-sphere, particularly the left temporal region, more so in therecord performed two months after the onset of coma thanin the record performed six months afterwards. Nosignificant changes occurred with hyperventilation or pho-tic stimulation. Sleep records were not made.
Discussion
The present case is unique in that it demonstrates"alpha coma" in the immediate posthypoxic periodin a patient who recovered and had had prior EEGs.The data from this patient combined with the avail-able reports in the literature contribute to ourunderstanding of: (1) the relationship of the alphapattern in coma to the physiologic alpha rhythm,and (2) the prognostic value of early resolving"alpha pattern coma".
Important differences were observed in ourpatient between the alpha activity during coma andthat recorded before or after coma. Distinguishingcharacteristics include the frequency, amplitude,
634 Iragui, McCutchen
group.bmj.com on September 14, 2016 - Published by http://jnnp.bmj.com/Downloaded from

Physiologic and prognostic significance of "alpha coma"
Table 1 Alpha coma patients who recovered consciousness
Reference Age (yr) Aetiology4 Length of Time from EEG during EEG after Outcome§Sex coma onset of coma coma coma
to EEG
Post hypoxic encephalopathy22 53 CA during diabetic 8 d
M coma
22 48 CA from not staM anaphylaxis
23 28 CA from electrical 3 wksM injury
23 26 CA from electrical 2 wksM injury
14 81 RA from vertebro- 4 wksF basilar insuff.
14 52 RA from food asp. 2 moF
14 28 Malpositioned Not staF endotracheal tube
24 56 CA -M
25 39 CA from myocardial 3 dM infarction
26 16 CA 5 dM
26 66 CA 6 dM
26 34 CA 15 dM
41 1'0/12 Strangulation 8 dM
37 12M
14 34F
14 38F
31 41M
t 64M
CA
RA from ElavilingestionRA frombarbiturateoverdoseRA fromtranquilizersCHFfrommyocardialinfarction
48 h
ted 48 h
19 h
24 h
ated *
24 h
18 h
24 h
4 d
1 d
3 d
19d 3d
24h *
Sd *
24 h 12 h
12h 2h
10-11 Hz, 20-40 Lv, 6-7 Hz diffusediffuse and fronto-cent, reactive9-10 Hz, 15-30 ,uv 5-7 Hz diffusediffuse unreactive7-9 Hz, low amp, 8-10 Hz Posteriorgen max fronto- reactivecent, unreactive9-11, med. amp, 7-8 Hz, very lowgen, max fronto- voltage reactivecentral
"alpha-coma"
8 Hz, max. fronto-temp. unreactiveAlpha, max. frontalreactiveAlpha
9-10 Hz and4-7 Hz, 30-50 lAv"Normal"
Not reported
Alpha, max. "Normal alpha"frontally unreactive10-11 Hz, 5 Hz, 40-150 tv50-120 yv, gen, post. reactive;max middle and widespread thetaPost. areas, and deltaunreactive; wide-spread theta anddelta11-5 Hz, widespread not reportedunreactive
Unreactive alpha
11-12 Hz,20-30 ,uv gen, max,frontal, unreactive
b
b
b
b
b
a
b, c
a
a
Normal reactive calpha9-10 Hz, 20-40 iLv bposterior reactive
Brain stem lesion12 63
F
14 68M
Vertebrobasilar 1 h 10 sec (comainsufficiency onset during
EEG)Midbrain infarction 6 wks *
12-14 and & Hz,20-30 MAvunreactive
10-12 Hz 20-35 Mv areactive
* b, c
Patients with alpha coma from drug overdose or head trauma are not included.*This study comprises 24 patients in 16 of whom the initial EEG was performed within 24 hrs after the onset of coma. The alpha activitywas diffuse in 9 patients, anteriorly predominant in 11 and posteriorly predominant in 4. Sensory stimulation was performed in 18 patients,and the EEG of only one patient considered to be "locked-in" showe a response. Follow-up EEGs in 5 of the 9 survivors demonstrated alow voltage alpha rhythm that responded to visual stimulation.tPresent report.tCA = cardiac arrest; RA = respiratory arrest; CHF = congestive heart failure.§a = full recovery; b = intellectual deficit, aphasia; c = motor disability, gait ataxia.
morphology, topography and/or reactivity. Thepremorbid alpha rhythm was of lower frequency andhigher amplitude than the alpha activity duringcoma. It also displayed typical spindling while thealpha activity during coma was sustained and dis-played little voltage modulation. The "normal"
alpha rhythm was most prominent over the posteriorhead regions and Was reactive to sensory stimula-tion, whereas the alpha activity during coma waswidespread and unreactive. Similar differences be-tween alpha activity during coma and that followingcoma have been reported in a number of cases who
3
635
group.bmj.com on September 14, 2016 - Published by http://jnnp.bmj.com/Downloaded from

636
recovered from "alpha coma" (table 1). However,few reports contain an EEG taken prior to the onsetof coma. Carroll and Mastaglia28 reported fourpatients with "alpha coma" caused by drug intoxica-tion apparently uncomplicated by cerebral hypoxia.An EEG prior to the onset of coma, available in oneof the patients, showed "reactive and symmetrical10 c/s alpha activity in a posterior distribution". AnEEG during coma showed "symmetrical 10 c/salpha activity in, a fronto-central distribution-whichdid not react to manual eye opening or to vigorousauditory or painful stimuli". An EEG followingrecovery was similar to the one prior to the onset ofcoma. The authors suggested that pharmacological.depression of the brain stem reticular formationplayed an important role in the pathogenesis ofdrug-induced "alpha coma", its genesis thereforebeing similar to that of "alpha coma" in structuralbrain stem disease. Jones et al'2 reported a patientwith vertebro-basilar insufficiency due to cervicalosteochondrosis, in whom transient ischaemia of thebrainstem resulted in coma lasting about one hour.Prior to the onset of coma, the EEG showed "apartially responsive and symmetrical alpha rhythmat 10-12 c/s of 20-35 ,uv". During coma, "thedominant activity was within the alpha frequencyrange, chiefly at 12-14 c/s, but intermixed at timeswith waves of about 8 c/s; the amplitude was usually20-30 ,uv peak to peak. Auditory or painful stimuliand passive opening of the eyes were without appar-ent effect on the EEG." Topography was. notreported. An EEG following recovery from coma
was similar to the first EEG. Lundervold2 studied a
patient who did not recover from coma followingvertebral angiography in whom post mortem exami-nation showed a pontine lesion involving the reticu-lar formation. The alpha activity during coma hadthe same amplitude, frequency and distribution as
the alpha rhythm recorded before coma, but it didnot react to sensory stimulation. Molofsky3'reported "alpha coma" in a 12-year-old boy whoseEEG at age 10 "was normal showing a well-developed 50-60 luv 10 Hz alpha rhythm whichattenuated with eye opening". An EEG on day 1 ofposthypoxic coma showed "diffuse slowing com-
prised of low voltage polymorphic 1-2 Hz waves andsmall amounts of intermixed 7-8 Hz activity". Onday 3, "the EEG was characterised by widespread11*5 Hz rhythmic activity unreactive to auditory,visual or noxious stimuli". On day 10, the EEGshowed "continuous polymorphic and rhythmic 5-7Hz activity, residual 1-3 Hz waves and abnormalsleep patterns". "Alpha coma" has also beenreported in three children of 2, 22 and 30 months ofage though a posterior dominant rhythm in thealpha range is not typical of this age group.40o42
Iragui, McCutchen
These observations and the findings in our patientsupport the interpretation that the alpha activity incomatose patients is an abnormally generated pat-tern different from the physiologic alpha rhythm.
Unlike our case and the paediatric case ofMolofsky,3 the other reports containing an EEGprior to the onset of coma are of patients whose"alpha coma" was thought secondary to drug orvascular insult to the brain stem. Apparently, thereare some differences between the alpha activity inthis clinical circumstance and the alpha activity inposthypoxic coma.13 In patients rendered comatoseby cardiac or respiratory failure, the alpha activity iseither generalised or most prominent over theanterior head regions, and is usually unreactive tosensory stimulation, as in our patient.13 14 2122 Mod-erate amounts of theta and delta potentials are alsoseen21 27 (fig 2). In patients with brainstem lesions,on the contrary, the alpha activity is typically maxi-mal over the posterior head regions and may beattenuated by sensory stimulation,913 although insome patients, stimulation failed to alter theEEG.231214 This emphasises the fact that patientswith "alpha coma" have to be distinguished fromthose with the "locked-in syndrome". The latterpatients usually have an alpha rhythm with normaltopography and reactivity and are conscious, thoughthey may appear to be in coma because they aremute and quadriplegic.'4 22 3839 In these cases a reac-tive alpha rhythm suggests that the patient may beawake and "locked-in" rather than comatose,. aspointed out by Grindal et al. 14The prognosis of "alpha coma" has generally
been though to be poor13212227 although recoverywith little or no neurological deficit has beenreported in some patients'4 22-31 37 41 including two ofthe four reported paediatric cases.374' The aetiologyof the coma has bearing on the outcome (table 1).Only two of approximately 40 patients with "alphacoma" from brainstem lesions reported in the Engl-ish literature survived, one of whom had significantmental and motor disability.'214 All patients withdrug overdose, with or without respiratory arrest,survived without sequelae.'42823' Though the sam-ple is small, the survival rate of patients with post-hypoxic "alpha coma" seems to be higher withrespiratory arrest than with cardiopulmonary arrest(table 2),.In our case, significant but incomplete clin-ical recovery occurred with the most important disa-bility being a nonfluent aphasia secondary to lefthemispheric infarct. Although an alpha rhythmdeveloped wvith characteristic physiologic distribu-tion and reactivity, polymorphic delta activityremained in the left temporal region as a consequ-ence of the stroke.The timing of electroencephalography following
group.bmj.com on September 14, 2016 - Published by http://jnnp.bmj.com/Downloaded from

Physiologic and prognostic significance of "alpha coma"
Table 2 Outcome ofpatients with post hypoxic alpha coma
Author No ofpts. Cardiopulm arrest Respiratory arrestpts/survivors ptslsurvivors
Lindgren et al'7 1 1/0 0/0Brierley et a1'9 1 1/0 0/0Vignaendra et al2' 8 8/0 0/0Westmoreland et al" 5 5/0 0/0Chokroverty22 9 9/2 0/0Grindal et al'4 23 20 14/2* 6/5tSnyder et al2' 2 2/1 0/0Sorensen et a!26 13 13/3 0/0Alvin et al27 30 30/1 0/0Obeso et al" 2 2/0 0/0Kuroiwa and Furukawa3' 1 0/0 1/1*Collins and Chatrian4' 1 0/0 1/1Molofsky37 1 1/1 0/0Total 94 86/10 8/7
'Cardiac arrest was secondary to electrical injury in both survivors.tIn two of the survivors, respiratory arrest was secondary to drug intoxication.tRespiratory arrest was secondary to drug intoxication.
hypoxia seems critical for accurate assessment of theprognostic significance of EEG patterns in post-hypoxic coma.3234 Since early onset continuousEEG monitoring in comatose patients has not beenstandard, the actual incidence and evolution of"alpha coma" is unknown. However, it appearsfrom our case and from those in the litera-ture'3-1517-27 that patients with an alpha patterndetected and resolved within 24 hours after theonset of posthypoxic coma have a more favourableoutcome than patients with alpha pattern disco-vered on or after the second day of coma (table 1).Alpha pattern not present in the initial EEGs afterhypoxia but appearing in later recordings usuallyindicates a poor prognosis13 14 192022 and when it isfollowed after several hours by electrocerebral sil-ence has been called "transitional alpha".43 In con-trast, the time at which the alpha pattern appears inpatients rendered comatose by brain stem lesionsdoes not seem to have prognostic implications.'1'6Our case is of particular interest because the alpha
pattern was recorded within 2 hours of theonset of posthypoxic coma in a patient that subse-quently recovered. Although EEGs during the firsttwo hours following cardiac arrest are now seldomperformed, aggressive therapy for posthypoxicencephalopathy such as the use of barbiturates mayrequire earlier prediction of potential for recovery."Under this circumstance, the prognostic value of theEEG pattern immediately following hypoxia may be.important in selecting patients for such treatment.Transient early "alpha coma" may not be uncom-mon and, as our case and others'2 suggest, may notindicate a poor prognosis. EEG monitoring begun inthe immediate period following hypoxia is needed toadequately assess the incidence of this pattern andits prognostic significance.
We thank Mr Hilary Lawrence for technicalassistance and Ms Marlene Brindell and Ms EmilyMaheu for assistance in the preparation of themanuscript.
AddendumJanati and Erbae recently reported "alpha coma" in threechildren with near-drowning accompanied bycardiorespiratory arrest that required resuscitation. TheEEGs recorded within 72 hours after the accident, "pre-sented widespread delta activity superimposed by 8-13c/sec rhythms which were either diffuse or maximal in thefrontal regions. Although largely unreactive, this alpha-like activity was at times attenuated by painful stimula-tion". Two male children ages 3-5 and 5 years, died daysafter the accident. The third one, a 22-month-old girl, sur-vived with severe neurological deficits.
References
'Loeb C, Poggio G. Electroencephalograms in a casewith ponto-mesencephalic hemorrhage. Electro-encephalogr Clin Neurophysiol 1953;5:295-6.
2Lundervold A, Hauge T, Loken AC. Unusual EEG inunconscious patient with brain stem atrophy. Elec-troencephalogr Clin Neurophysiol 1956;8:665-70.
3Loeb C, Rosadini G, Poggio GF. Electro-encephalograms during coma. Normal and borderlinerecords in five patients. Neurology A(Mnneap)1959;9:610-8.
4Kaada BR, Harkmark W, Stokke D. Deep coma associ-ated with desynchronization in EEG. Electro-encephalogr Clin Neurophysiol 1961;13:785-9.
5Chatrian GE, White LE, Shaw CM. EEG patternresembling wakefulness in unresponsive descerebratestate following traumatic brain-stem infarct. Electro-encephalogr Clin Neurophysiol 1964;16:285-9.
6Marquardsen I, Harvald B. The electroencephalogramin acute vascular lesions of the brain stem and cerebel-lum. Acta Neurol Scand 1964;40:58-69.
637
group.bmj.com on September 14, 2016 - Published by http://jnnp.bmj.com/Downloaded from

638
Rohmer F, Jurtz D, Kiffer A. Etude critique de L'acti-vite E.E.G. dans les syndromes vasculaires de tronccerebral. Rev Neurol (Paris) 1965;113:279-84.
Radermecker J. Severe acute necrosis of the pons withlong survival. Electro-clinical symptoms and absenceof cerebral lesions. Electroencephalogr ClinNeurophysiol 1967;23:281.
9 Chase TN, Moretti L, Prensky AL. Clinical and elec-troencephalographic manifestations of vascularlesions of the pons. Neurology (Minneap) 1968;18:357-68.
10 Wilkus RJ, Harvey F, Ojeman LM, Lettich E. Elec-troencephalogram and sensory evoked potentials.Finding in an unresponsive patient with pontineinfarct. Arch Neurol 1971;24:538-44.
" Hughes JR, Cayaffa J, Leetsma J, Mizuna Y. Alternating"waking" and "sleep" EEG patterns in a deeply com-atose patient. Clin Electroencephalogr 1972;3:86-93.
12 Jones BN, Binnie CD, Fung D, Hamblin JJ. Reversiblecoma with an EEG pattern normally associated withwakefulness. Electroencephalogr Clin Neurophysiol1972;33: 107-9.
13 Westmoreland BF, Klass DW, Sharbrough FY, ReaganTJ. Alpha-coma. Electrographic, clinical, pathologicand etiologic correlations. Arch Neurol 1975;32:713-8.
14 Grindal AB, Suter C, Martinez AJ. Alpha-pattern coma:24 cases with 9 survivors. Ann Neurol 1977;1:371-7.
.s Obeso JA, Iragui MI, Marti-Masso JF, Maravi E, Tei-jeira JM, Carrera N, Teijeira J. Neurophysiologicalassessment of alpha-pattern coma. J NeurolNeurosurg Psychiatry 1980;43:63-7.
16 Dias A, Scott DF. Alpha coma: a case report. Clin Elec-troencephalogr 1981;12:130-2.
17 Lindgren S, Petersen I, Zwetnow N. Prediction of deathin serious brain damage. Acta Chir Scand 1968;134:405-16.
1 Binnie CD, Prior PF, Lloyd DSL, Scott DF, MargerisonJH. Electroencephalographic prediction of fatalanoxic brain damage after resuscitation from cardiacarrest. Br Med J 1970;4:265-8.
19 Brierley JB, Adams JH, Graham DI, Simpson JA.Neocortical death after cardiac arrest. A clinical,neurophysiological and neuropathological report oftwo cases. Lancet 1971;2:560-5.
20 Lemmi H, Hubbart CH, Faris AA. The electro-encephalogram after resuscitation of cardiocirculatoryarrest. J Neurol Neurosurg Psychiatry 1973;36:997-1002.
21 Vignaendra V, Wilkus RJ, Copass MK, Chatrian GE.Electroencephalographic rhythms of alpha frequencyin comatose patients after cardiopulmonary arrest.Neurology (Minneap) 1974;24:582-8.
22 Chokroverty S. "Alpha-like" rhythms in electro-encephalograms in coma after cardiac arrest.Neurology (Minneap) 1975;25:655-63.
23 Grindal AB, Suter C. "Alpha-pattern coma" in high vol-tage electrical injury. Electroencephalogr ClinNeurophysiol 1975;38:521-6.
24 Snyder BD, Ramirez-Lassepas M, Lippert DM.Neurologic status and prognosis after cardio-pulmonary arrest: I. A retrospective study. Neurology(Minneap) 1977;27:807-1 1.
25 M0ller M. "Alpha-pattern coma" and survival after car-
Iragui, McCutchen
diac arrest. Electroencephalogr Clin Neurophysiol1978;44:518-22.
26 Sorensen K, Thomassen A, Wernberg M. Prognosticsignificance of alpha frequency EEG rhythm in comaafter cardiac arrest. J Neurol Neurosurg Psychiatry1978;41:840-2.
27 Alvin J, M0ller M, Sindrup E, Nielsen BL. "Alpha pat-tern coma" following cerebral anoxia. Electro-encephalogr Clin Neurophysiol 1979;47:95-101.
28 Carroll WM, Mastaglia FL. Alpha and beta coma in drugintoxication uncomplicated by cerebral hypoxia. Elec-troencephalogr Clin Neurophysiol 1979;46:95-105.
29 Endo M, Hirano M, Nakamura I, Kawai Y. The twosurvival cases of alpha-pattern coma caused by largeamounts of hypnotica and neuroleptica. Folia PsychiatNeurol Jap 1980;34:451-8.
30 Guterman B, Sebastian P, Sodha N. Recovery from thealpha coma after lorazepam overdose. Clin Elec-troencephalogr 1981 ;12:205-8.
31 Kuroiwa Y, Furukawa T. EEG prognostication in drug-related alpha coma. Arch Neurol 1981;38:200.
32 Prior PF. The EEG in Acute Cerebral Anoxia. Amster-dam: Excerpta Medica, 1973.
33 Pampiglione G. Electroencephalographic studies aftercardiorespiratory resuscitation. Proc Roy Soc Med1962;55:653-62.
34 Pampiglione G, Harden A. Resuscitation after cardiocir-culatory arrest. Prognostic evaluation of early elec-troencephalographic findings. Lancet 1968;1:1261-5.
35 Teasdale G, Jennett B. Assessment of coma andimpaired consciousness: A pratical scale. Lancet1974;2:81-4.
36 Jennett B, Bond M. Assessment of outcome after severebrain damage: A practical scale. Lancet 1975;1:480-4.
31 Molofsky WJ. Alpha coma in a child. J NeurolNeurosurg Psychiatry 1982;45:95.
3 Hawkes CH, Bryan-Smyth L. The electro-encephalogram in the "locked-in" syndrome. Neurol-ogy (Minneap) 1974;24:1015-8.
39 Plum F, Posner JB. The Diagnosis ofStupor and Coma.Philadelphia: FA Davis Co, 1980:159-60.
10 Yamada T, Stevland N, Kimura J. Alpha-pattern comain a 2-year-old child. Arch Neurol 1979;36:225-7.
41 Collins AT, Chatrian GE. EEG rhythm of alpha fre-quency in a 22-month-old child after strangulation.Neurology (Minneap) 1980;30: 1316-9.
42 Homan RW, Jones MG. Alpha-pattern coma in a2-month-old child. Ann Neurol 1981;9:611-3.
43 Arfel G. Introduction to clinical and EEG studies incoma. In: Remond A, ed. Handbook of Electro-encephalography and Clinical Neurophysiology. Vol-ume 12. Altered states ofconciousness, coma and cere-bral death. Amsterdam: Elsevier Scientific PublishingCompany, 1975:5-23.
4Allen N. Life or death of the brain after cardiac arrest.Neurology (Minneap) 1977;27:805-6.
4S Janati A, Erba G. Electroencephalographic correlates ofnear-drowning encephalopathy in children.Electroencephalogr Clin Neurophysiol 1982;53:182-91.
group.bmj.com on September 14, 2016 - Published by http://jnnp.bmj.com/Downloaded from

significance of "alpha coma".Physiologic and prognostic
V J Iragui and C B McCutchen
doi: 10.1136/jnnp.46.7.6321983 46: 632-638 J Neurol Neurosurg Psychiatry
http://jnnp.bmj.com/content/46/7/632Updated information and services can be found at:
These include:
serviceEmail alerting
online article. article. Sign up in the box at the top right corner of the Receive free email alerts when new articles cite this
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on September 14, 2016 - Published by http://jnnp.bmj.com/Downloaded from