Embed Size (px)
Citation preview

Physiological Changes:
Health Related Fitness
Chapter 8
1McGraw-Hill/Irwin © 2012 McGraw-Hill Companies. All Rights Reserved.

8-2
Maintaining an active lifestyle is linked to good
health.
2

8-3
Cardiovascular Fitness
A form of muscular enduranceEfficiency of the heart, lungs, and vascular system in delivering oxygen to working tissueYour ability to deliver oxygen to the muscle is affected by
Heart rateStroke volumeCardiac outputMaximal oxygen consumption
3

8-4
Cardiovascular Fitness: Heart Rate
The number of times the heart beats each minute (HR)Changes over the lifespan
Fetal HR is rapid and irregularBirth HR is below fetal level with periods of bradycardia (HR < 60 bpm)
120-140 bpm

8-5
Cardiovascular Fitness: Heart Rate
Children’s HR 1 year ~ 80-100 bpm HR will continue to decline at rest until adolescence
AdolescenceMale ~ 57-60 bpmFemale ~ 62-63 bpm

8-6
Cardiovascular Fitness: Heart Rate
Overall, resting HR declines by 50% from birth to maturityAdulthood
Average ~ 75-79 bpm
There is a decline in HR with ageResearchers believe the decline in HR with age is due to a decrease in sympathetic outflow and changes in the contractile properties of cardiac muscle

8-7
Cardiovascular Fitness: Heart Rate
To predict maximal HR220-age = HR maxHR max = 195-220 bpmDecline = 0.8 bpm/year of age
To predict maximal HR in the elderly HR max = 206 – 0.7(age in yr.)

8-8
Cardiovascular Fitness: Heart Rate
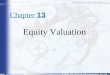
Work and HRLinear relationshipAs workload increases, HR increases
Workload
HR

8-9
Cardiovascular Fitness: Stroke Volume
The volume of blood ejected from the heart with each beat (SV)Size of SV affected by
Heart sizeContractile force of the heart muscleVascular resistance to blood flowVenous return

8-10
Cardiovascular Fitness: Stroke Volume
SV is lower in childrenDue to smaller heart
Lifespan changesBirth ~ 3-4 ml/beatAdolescence ~ 40 ml/beatMale adult ~ 70-90 ml/beatTrained male adult ~ 100-120 ml/beat

8-11
Cardiovascular Fitness: Stroke Volume
Maximal stroke volume is achieved during submaximal work
SV
Workload
40-60% (O2max)

8-12
Cardiovascular Fitness: Stroke Volume
Maximal SV during exerciseUntrained male ~ 100-120 ml/beatUntrained female ~ 80-100 ml/beatTrained male ~ 150-170 ml/beatTrained female ~ 100-120 ml/beat
Differences between male and female values due to smaller heart in female

8-13
Cardiovascular Fitness: Stroke Volume
Stroke volume and ageBetween the ages of 25-85 yr., SV can fall by 30%
Lifespan activity can minimize the SV decline with age

8-14
Cardiovascular Fitness: Cardiac Output
Amount of blood pumped in 1 minute (CO)HR x SV = COAt rest, CO5 liters/min
70 beats/min x 70 ml/beat = 4900 ml/min or 4.9 liters/min

8-15
Cardiovascular Fitness: Cardiac Output
CO and exerciseAffected by physical conditionAge
Untrained male ~ 20-25 liters/minTrained male ~ 30-35 liters/minBecause HR and SV decline with age, so does CO
Decline of 1 % / year after age 25 yr.

8-16
Cardiovascular Fitness: Maximal Oxygen Consumption
The largest amount of oxygen that a human can utilize at the tissue level (VO2 max )This is the best measure of physical work capacity (ability to do work without fatigue)Very little data exist on children under 6 years of age

8-17
Cardiovascular Fitness: Maximal Oxygen Consumption
For boys ages 6 to 16 years, VO2 max 50 to 53 ml/kg/minFor girls at 8 yr., VO2 max = 50 ml/kg/min, on averageIf you do not correct for weight (kg), boys/men will always have higher absolute valuesTo compare males vs. females, correct for body weight (kg) (relative values)

8-18
Cardiovascular Fitness: Maximal Oxygen Consumption
There is a gradual decline in maximal oxygen consumption in young girls as maturity approaches due to
Increases in body fatLower blood hemoglobin concentrations A decline in large muscle development
Many girls become less active during adolescence

8-19
Cardiovascular Fitness: Maximal Oxygen Consumption
With age there is a decline in VO2 max and a concomitant decline in physical work capacityAn active lifestyle across the lifespan can alter this decline

8-20
Physical Activity and Cardiovascular
Fitness in ChildhoodInformation is fragmented and limitedAre changes in the cardiovascular values in children due to training or maturation?Some researchers question the value of endurance training in preadolescent children

8-21
Physical Activity and Cardiovascular
Fitness in ChildhoodVO2 max has been shown to improve in prepubertal children (10-11 yr.)Prepubertal children can follow the standard prescription used by adults
Frequency = 3 days per weekIntensity = 60%-80% HR maxTime = 30 min

8-22
Cardiovascular Endurance Field-Test Data
Field test data involve non-laboratory devices capable of testing large numbers of children
Practical Inexpensive
Most popular field test for childrenTimed distance run

8-23
Cardiovascular Endurance Field-Test Data
Boys’ run time peaks at 16 yr.Girls’ run time peaks at 14 yr.On average, boys run faster than girls at all ages

8-24
Physical Activity and Cardiovascular
Fitness in AdulthoodPrescription ~ FIT
Frequency = 3 to 5 days/weekIntensity = 60-90% HR maxTime = 20-60 min
Mode of activity is any large muscle group movement (walking, biking, running)A program of this sort will increase physical working capacity

8-25
Physical Activity and Cardiovascular
Fitness in AdulthoodIt has been suggested that as much as 50% of the functional declines in the factors affecting physical performance are due to disuse and not agingChildren’s Activity Pyramid

8-26

8-27
Muscular Strength
Strength is the ability to exert a muscular forceStatic or isometric force – muscular force exerted against a non-moveable objectDynamic force – muscular force exerted against a moveable object

8-28
Defining and Measuring Muscular Strength
Field testsPull-up test ~ upper body strength/enduranceChin-up test ~ upper arm strength/enduranceModified bent-knee sit-up test ~ abdominal strength/endurance

8-29
Age-related Changes in Muscular Strength: Laboratory Tests
Grip strength test is a common test among children
Easy to administerReliable
Changes in strength are tied to changes in body weight

8-30
Age-related Changes in Muscular Strength: Laboratory Tests
In boys, the strength “spurt” lags a year behind the height “spurt”
Boys tend to outgrow their strength just prior to pubertyMay explain why some boys experience a period of clumsiness
Boys’ fastest increase in muscular strength occurs 1 yr. after peak height

8-31
Age-related Changes in Muscular Strength: Laboratory Tests
In girls, the strength spurt occurs during the same year as peak heightIn general, boys are 10% stronger than girlsGender differences are most apparent after puberty
Total body strength in women is 63.5% of menAbsolute upper-body strength in women is 50% less than menAbsolute lower-body strength in women is 20-30% lower than men

8-32
Age-related Changes in Muscular Strength: Laboratory Tests
AgingBetween 25-50 yr. there is a slow loss in muscle mass of about 10%Between 50-80 yr. there is an accelerated loss of muscle mass of about 40%Therefore, one can lose approximately 50% of total muscle mass by the age of 80 yr.

8-33
Age-related Changes in Muscular Strength: Field Tests
Average scores for boys and girls on bent-knee sit-ups (60 sec) based on findings of the National Children and Youth Fitness Studies I and II

8-34
Age-related Changes in Muscular Strength: Field Tests
Average scores for boys and girls on modified pull-ups and chin-ups based on findings of the National Children and Youth Fitness Studies I and II

8-35
Age-related Changes in Muscular Strength: Field Tests
Abdominal strength/enduranceLittle differences exist between boys and girls ages 6 to 9 yr.After age 10 yr., boys outperform girlsPerformance for both boys and girls levels off between 16 to 18 yr.

8-36
Age-related Changes in Muscular Strength: Field Tests
Upper-body strength/endurance30% of boys age 10-11 yr. failed to perform 1 chin-up during the NCYFS IModified chin-up test developed for the NCYFS II
Modified Chin-up Test

8-37
Age-related Changes in Muscular Strength: Field Tests
Upper-body strength/enduranceLittle differences exist between boys and girls ages 6 to 9 yr.After age 10 yr., boys outperform girlsAfter age 10 yr., girls are not capable of performing any chin-ups

8-38
Muscular Strength Training
PrepubescentControversy exists regarding strength training for this populationCan children increase strength through a resistance training program?Can these strength gains improve athletic performance?

8-39
Muscular Strength Training
PrepubescentSkills showing improvement
Long jumpVertical jumpRunning speedAgility
Specificity ~ greatest skill improvement was for those activities in which the children were involved

8-40
Muscular Strength Training
PrepubescentProfessional organizations publishing position statements for prepubescent strength training
American Academy of PediatricsNational Strength and Conditioning AssociationAmerican Orthopedic Society for Sports Medicine
All three recognize the value of weight training

8-41
Muscular Strength Training
PrepubescentWeight training involves the use of various resistance exercises to increase muscular strength, endurance, and power for fitness or sportWeight/power lifting is a sport incorporating maximal lifts (until physically mature)
Not recommended for youth

8-42
Muscular Strength Training
Adolescence/early and middle adulthoodPrograms of progressive resistance training will result in improved muscular strength/endurance
1 RM (repetition maximum) in boys and girls ages 6.2-12.3 yr. is safe when conducted in the presence of adult supervision

8-43
Muscular Strength Training
Minimal training standards (ACSM)Frequency ~ 2 times per weekIntensity ~ 60% of 1 repetition maximumAmount ~ 1 set
1 set of 8 to 12 exercises8-10 repetitions per exercise
Adolescence/early and middle adulthoodConcerns for these populations
Valsalva Maneuver ~ breath holding (straining) during a liftAnabolic steroid use

8-44
Muscular Strength Training
Late adulthoodCan strength training in late adulthood alter, delay, or allow one to avoid the physiological deterioration associated with aging?Even though decreases in muscular strength can be expected with age, the rate of decline can be significantly slowed

8-45
Muscular Strength Training
Late adulthoodIt is never too late to start a resistance-training program
1.9% to 132% improvements in strength
For the elderly, it is the intensity of the training and not the initial level of fitness that determines the response to training

8-46
Muscular Strength Training
Late adulthood Strength training also decreases the number of falls experienced by this populationStrength training positively influences activities of daily living

8-47
Muscular Strength Training
Mechanisms of strength increaseIn the early phase of training, neural adaptation predominates
Most training studies incorporate this phase
In intermediate and advanced training, progress is limited to the extent of muscular adaptation that can be achieved
HypertrophyAnabolic steroid use

8-48

8-49
Adverse Effects of Anabolic Steroids

8-50
Flexibility
Range of motion with a jointFlexibility is joint specific
There is no one good test for overall flexibility
A typical flexibility test Sit-and-reach test / back saver sit-and–reach testTests the hamstring, back and hip flexibility

8-51
Flexibility Sit and reach test
Back saver sit and reach test

8-52
Flexibility
Average sit-and-reach scores for boys and girls based on finding of the National Children and Youth Fitness Studies I and II
Performance Trends

8-53
Flexibility
Flexibility declines with age due to changes in
Connective tissue (tendons, ligaments) ~ less resilient and may crack or fraySynovial fluid ~ less viscousCartilage ~ may be damaged from injury or lifelong wear and tear

8-54
Flexibility
Declining flexibility and agingOsteoarthrosis is common in 80% of adults between the ages of 55 and 64 yr.
Regardless of process or causes, physical activity is necessary to maintain joint mobility

8-55
Body Composition ~ Obesity
Defining obesityMany define obesity based upon appearance alone or the number of pounds one is “overweight”Body composition
Amount of lean body tissue vs. fat tissue

8-56
Body Composition ~ Obesity
Growth trends in adipose tissueBirth ~ 11% fat in boys and 14% in girlsFat at birth is stored in ~5 billion adipocytesThe number of fat cells continues to increase in childhood

8-57
Body Composition ~ Obesity
Two growth spurts in fat tissue1 yr. ~ fat % in boys 26%; in girls 28%Puberty for boys; prepuberty and puberty for girls
Greater fat mass in girls during the second growth spurt
With age, fat’s contribution to overall body composition depends upon the size of fat cells, not the number of cells

8-58
Body Composition ~ Obesity
General growth trendsBody weight reaches its peak at about 45 years of age
Body weight is not a good indicator of body composition
A sedentary lifestyle lends to the observed decrease in lean body mass and an increase in fat mass

8-59
Body Composition ~ Obesity
Prevalence of obesity among children and adults

8-60
Body Composition ~ Obesity

8-61
Trends in Obesity

8-62
Body Composition ~ Obesity
Prevalence of obesity in the US ~ raceMexican American and black non-Hispanic women exhibit higher rates of overweight and obesity compared non-Hispanic white womenMexican American men exhibit higher rates of overweight and obesity compared to non-Hispanic blacks and non-Hispanic whites

8-63
Obesity in Selected Groups

8-64
Body Composition ~ Obesity
Prevalence of obesity in the US ~ incomeLow socioeconomic status (income < 130% of the poverty levelHigh socioeconomic status (income > 130% of the poverty level

8-65
Body Composition ~ Obesity
Prevalence of obesity in the US ~ incomeMen in both groups are likely to become overweight and obeseWomen in low socioeconomic groups are more likely to become overweight or obese compared to women in high socioeconomic groups

8-66
Body Composition ~ Obesity
Health consequencesHigh blood lipid levelsElevated blood pressureDiabetesCardiovascular disease

8-67
Body Composition ~ Obesity
Association between childhood and adulthood obesity
Children with a BMI value at the 95th tile for their age and gender have a greater than 60% chance of being obese at age 35 yr.

8-68
Body Composition ~ Obesity
Selected percentiles for BMI in males from the Second National Health and Nutrition Examination Survey

8-69
Body Composition ~ ObesitySelected percentiles for BMI in females from the Second National Health and Nutrition Examination Survey

8-70
Body Composition ~ Obesity
Field test measures of body fatHydrostatic weighingBod PodDual energy X-ray absorptiometry (DEXA)Skinfold calipers

8-71
Body Composition ~ Hydrostatic Weighing
Hydrostatic weighing has been the preferred method for determining percent body fatThis test is not practical as a field-test measureCalculations based upon water displacement

8-72
Body Composition ~ Bod Pod
The Bod Pod is fast becoming the new standard in body composition measurementCalculations are based upon air displacementEveryone can be tested ~ disabled, children, elderly

8-73
Body Composition ~ Skinfolds
Average sum of triceps and subscapular skinfold thicknesses in boys and girls

8-74
Body Composition ~ Obesity
Relationship of obesity to motor development and performance
In general, greater amounts of fat are negatively related to activities where the body has to be projected or lifted (tests of vertical jumping, running/walking, running)

8-75
Gender Differences in Health-Related Physical Fitness
During the ages of 4-18 yrs.Strong negative correlation between BMI and endurance performanceBoys outperform girls in the distance run, chin-up, and sit-up testsGirls outperform boys in the sit-and-reach test

8-76
Factors Associated with Physiological Fitness in Children and
AdolescentsChildren who perform well on tests
of physiological fitness tend to participate
in more community-based activities,
watch less television, receive their
physical education from a specialist,
experience more activities over the
course of a year, and come from
families where physical activity is valued

8-77
We are living longer. What is the best way to live a long and
high quality life?

8-78
Key Terms