Embed Size (px)
Citation preview
Ch 17
Physiology of
the Kidneys
Review Anatomy on your own
SLOs • List and describe the 4 major functions of the kidneys.
• List and explain the 4 processes of the urinary system.
• Diagram the filtration barriers a H2O molecule will pass as it travels from the blood into the nephron and illustrate the anatomical structures and mechanisms by which filtration can be controlled.
• Define GFR and give the average value for GFR.
• Describe the hydrostatic and osmotic pressures that contribute to glomerular filtration and indicate the direction of fluid movement favored by the net pressure.
• Diagram how GFR can be influenced by: – variable resistance in afferent and efferent renal arterioles. – myogenic and tubuloglomerular autoregulatory mechanisms. – hormonal control and neural control.
• Describe active and secondary active transport and passive reabsorption mechanisms used by the kidney to accomplish reabsorption of Na+ and glucose.
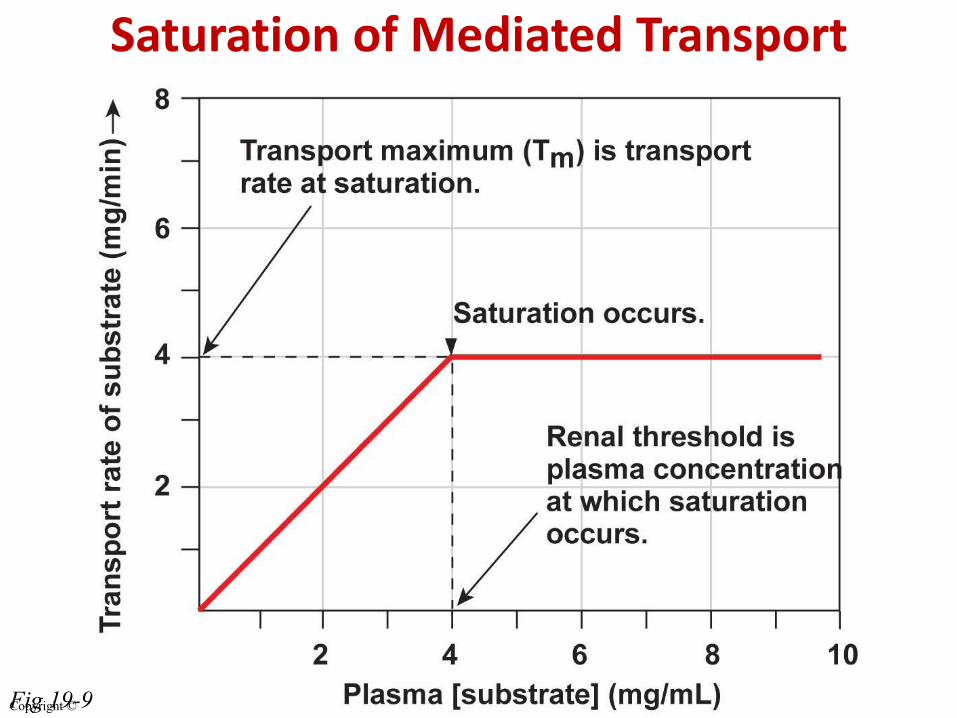
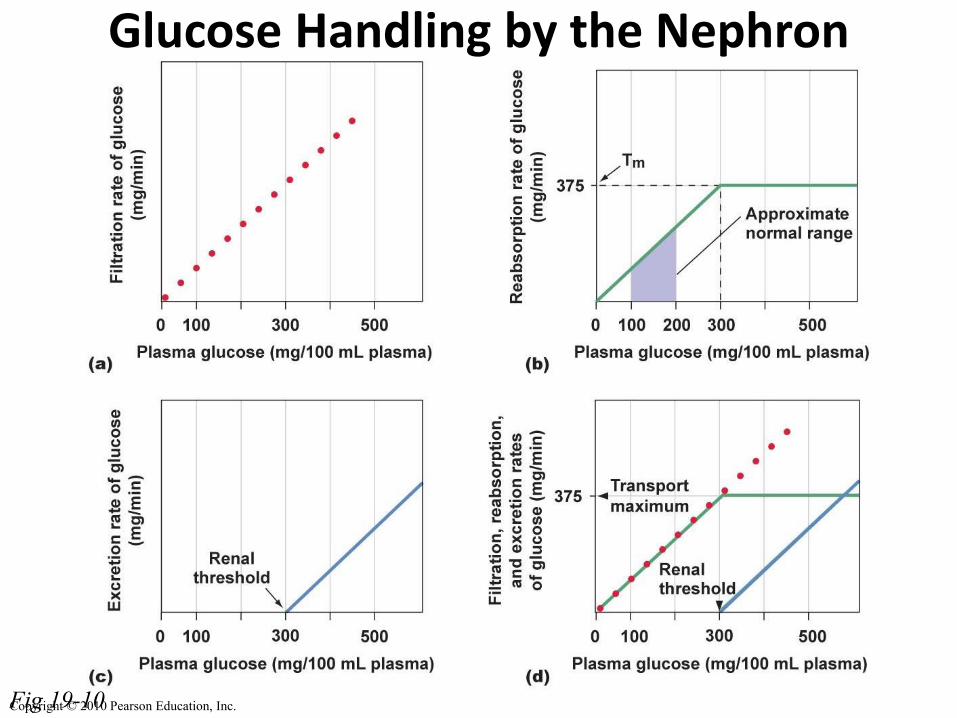
• Create a generalized graph of the reabsorption of glucose in order to demonstrate how protein-mediated renal transport can reach saturation. Mark on the graph where transport maximum and renal threshold occur.
• Explain the connection between GFR and Clearance rate and explain clinical significance of the clearance
• Apply the equation E = F – R + S to analyze renal handling of a substance.
• Diagram the involuntary micturition reflex and incorporate the voluntary control influence exerted by higher brain centers.
17.1 FUNCTION OF THE KIDNEYS
Kidneys function in …
H2O & solute concentration homeostasis
ECF volume ( BP)
osmolarity, electrolyte concentration
pH homeostasis (acid-base balance)
Excretion of wastes & foreign
substances
Hormone and enzyme production
Functional unit?
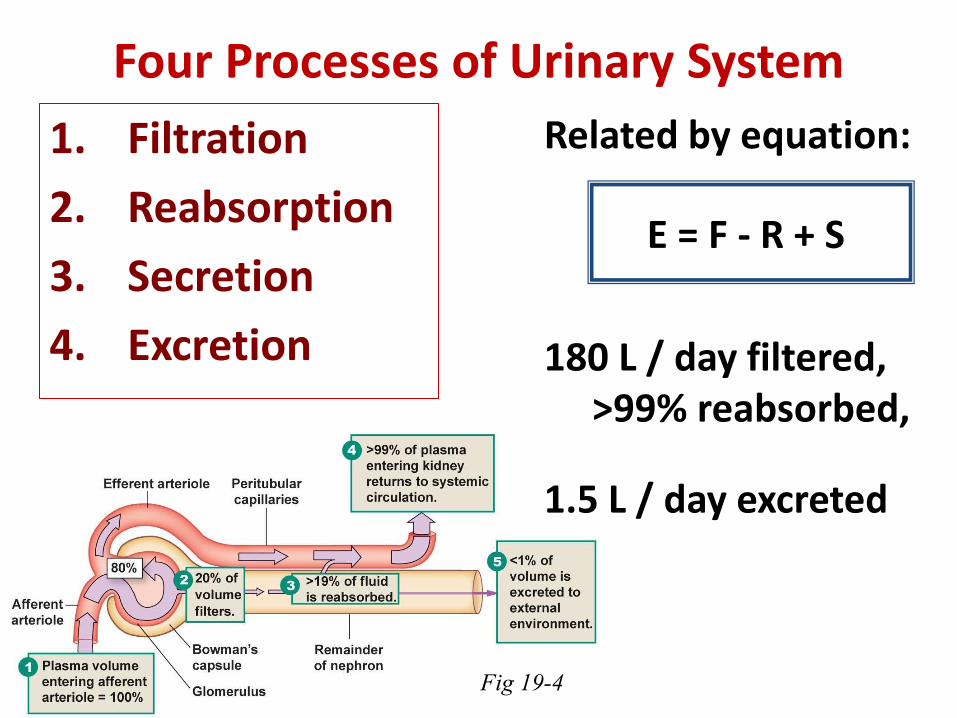
Four Processes of Urinary System
1. Filtration
2. Reabsorption
3. Secretion
4. Excretion
Related by equation:
E = F - R + S
180 L / day filtered, >99% reabsorbed,
1.5 L / day excreted
Fig 19-4
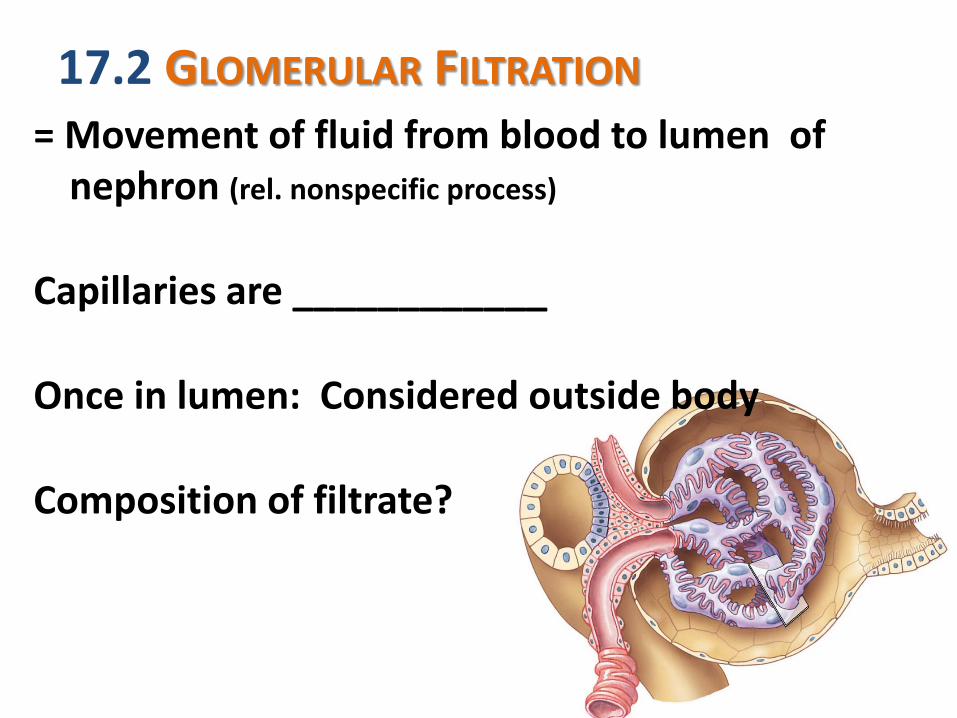
17.2 GLOMERULAR FILTRATION = Movement of fluid from blood to lumen of
nephron (rel. nonspecific process)
Capillaries are ____________
Once in lumen: Considered outside body
Composition of filtrate?
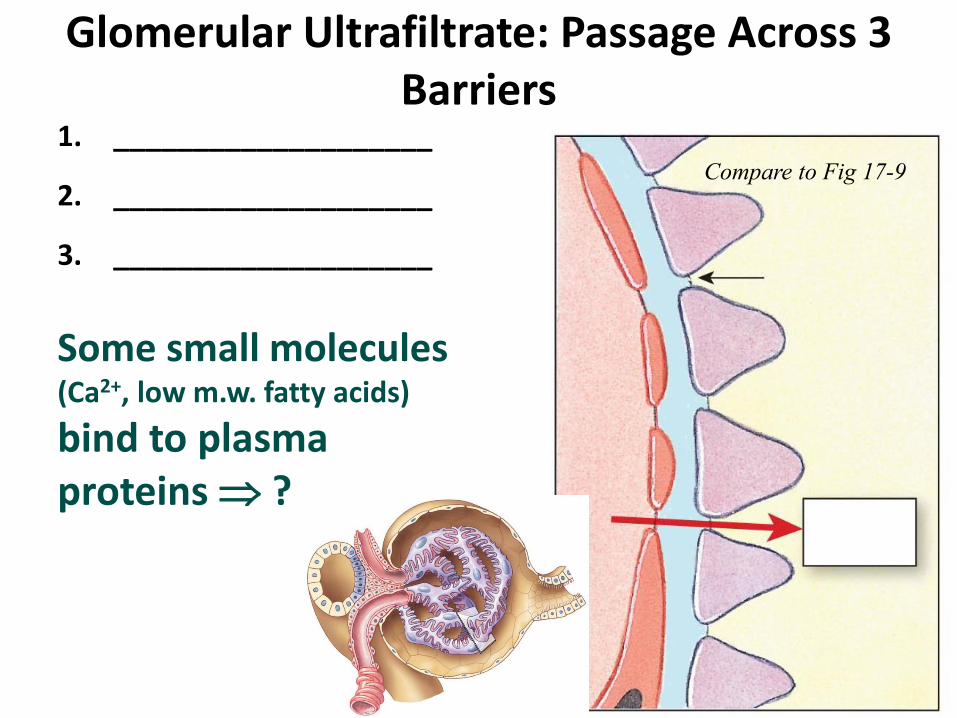
Glomerular Ultrafiltrate: Passage Across 3 Barriers
1. ____________________
2. ____________________
3. ____________________
Some small molecules (Ca2+, low m.w. fatty acids)
bind to plasma proteins ?
Compare to Fig 17-9
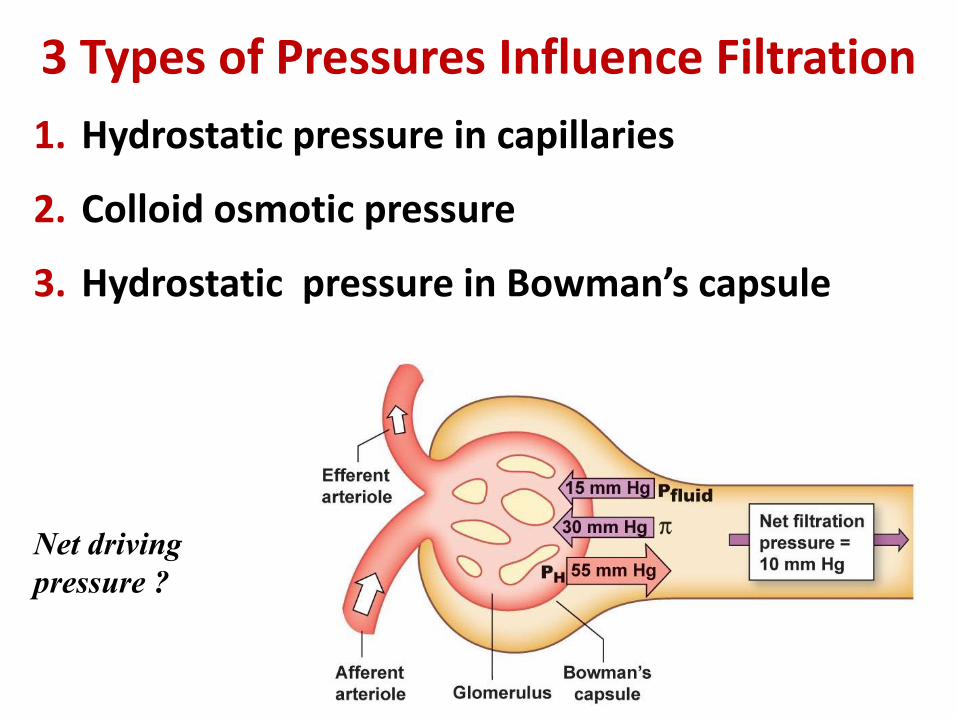
3 Types of Pressures Influence Filtration
1. Hydrostatic pressure in capillaries
2. Colloid osmotic pressure
3. Hydrostatic pressure in Bowman’s capsule
Net driving
pressure ?
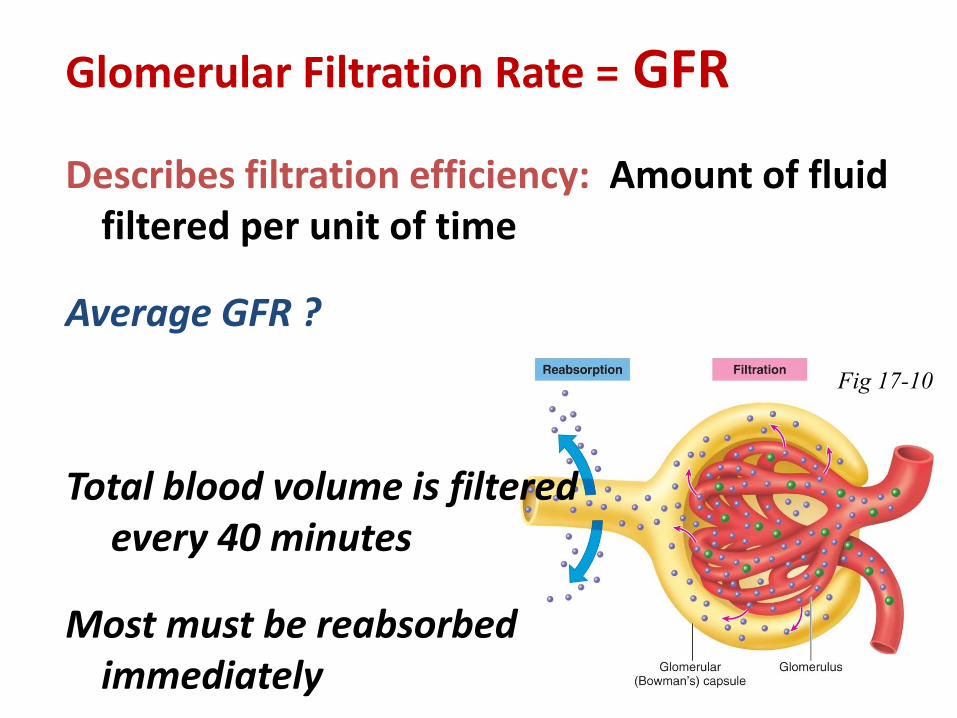
Glomerular Filtration Rate = GFR
Describes filtration efficiency: Amount of fluid filtered per unit of time
Average GFR ?
Total blood volume is filtered every 40 minutes
Most must be reabsorbed immediately
Fig 17-10
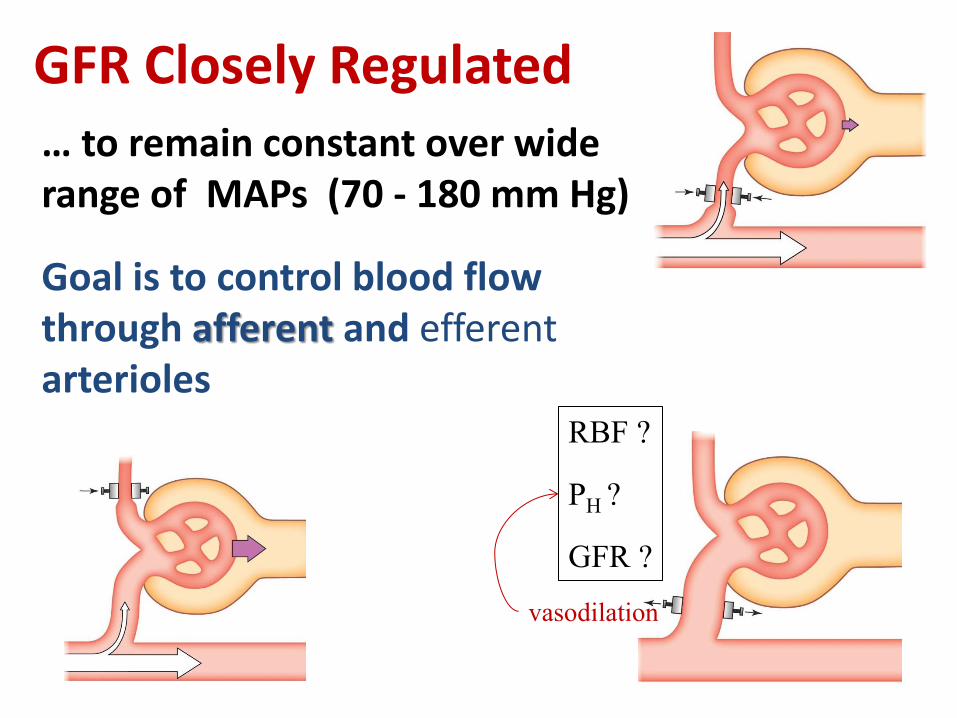
GFR Closely Regulated … to remain constant over wide range of MAPs (70 - 180 mm Hg)
Goal is to control blood flow through afferent and efferent arterioles
RBF ?
PH ?
GFR ?
vasodilation
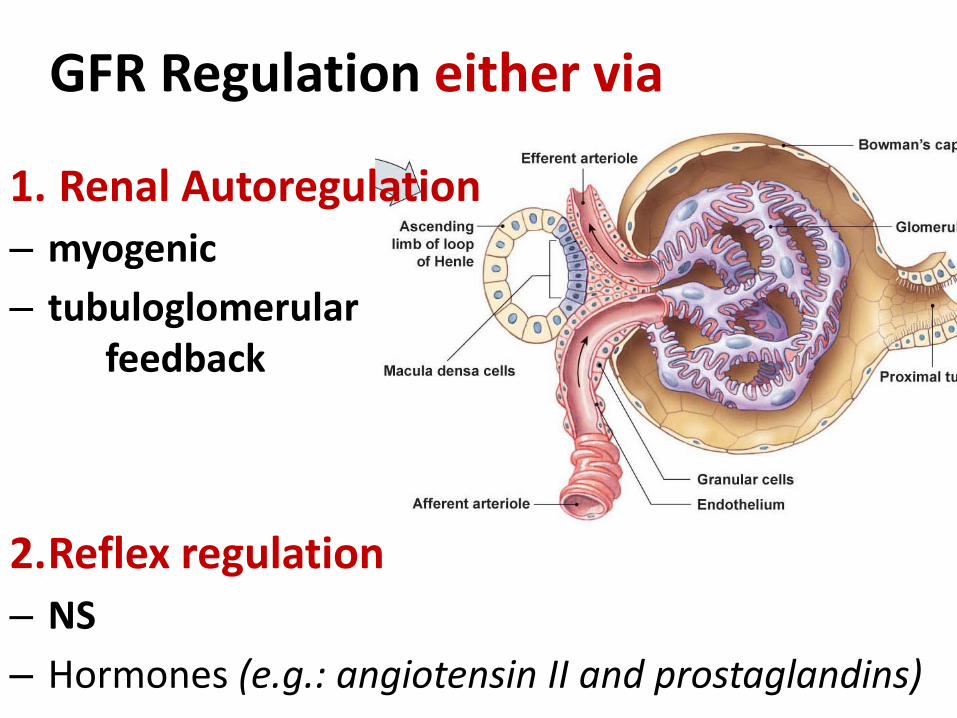
GFR Regulation either via
1. Renal Autoregulation
– myogenic
– tubuloglomerular feedback
2.Reflex regulation
– NS
– Hormones (e.g.: angiotensin II and prostaglandins)
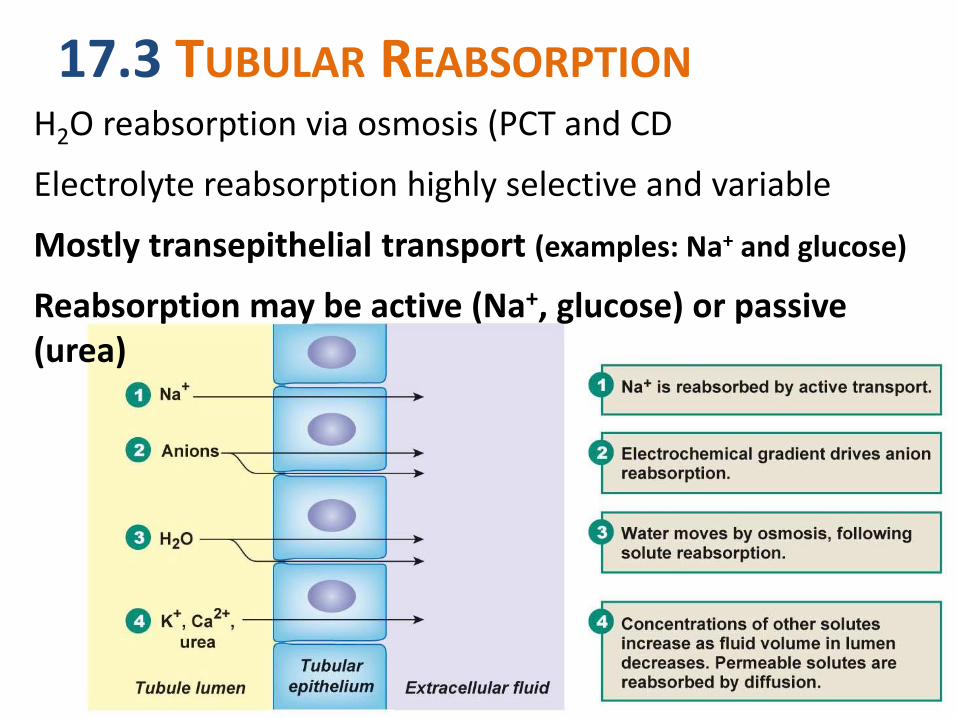
17.3 TUBULAR REABSORPTION H2O reabsorption via osmosis (PCT and CD
Electrolyte reabsorption highly selective and variable
Mostly transepithelial transport (examples: Na+ and glucose)
Reabsorption may be active (Na+, glucose) or passive (urea)
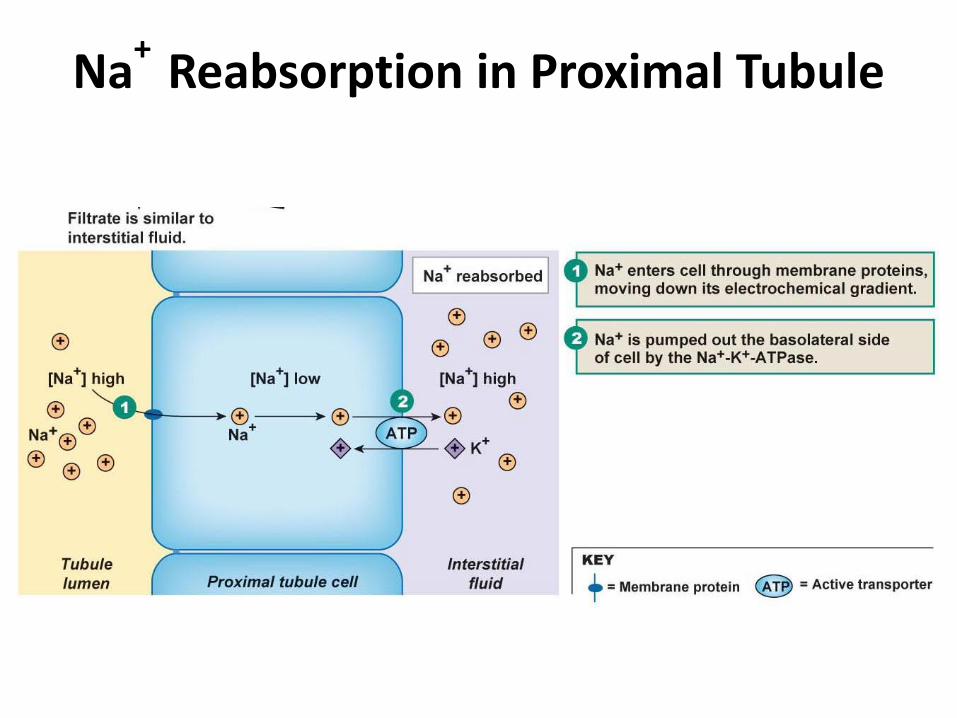
Na+
Reabsorption in Proximal Tubule
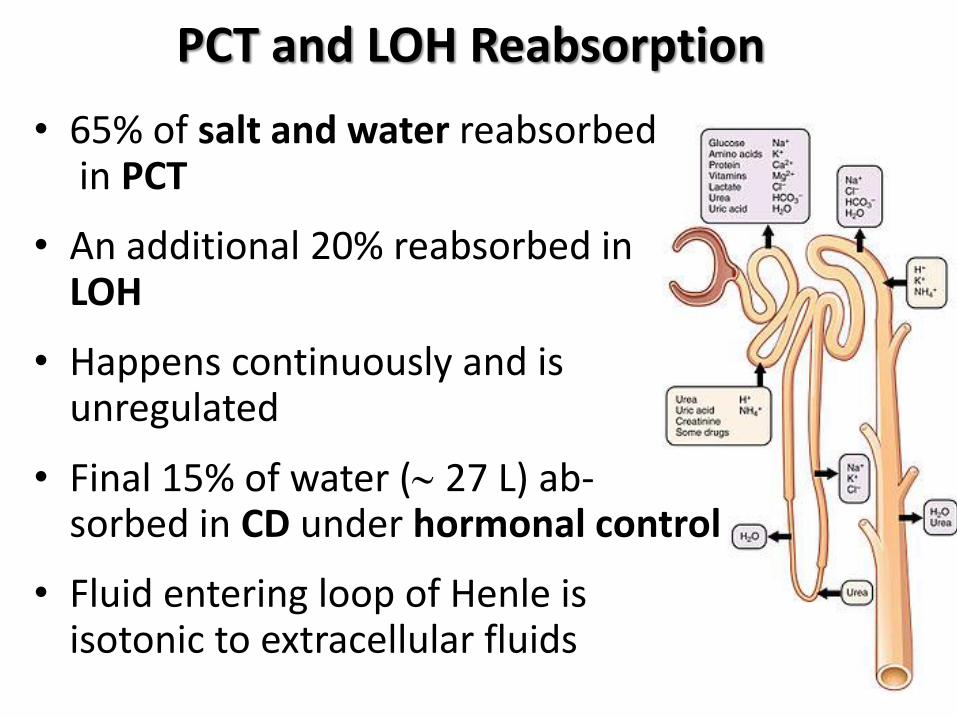
PCT and LOH Reabsorption
• 65% of salt and water reabsorbed in PCT
• An additional 20% reabsorbed in LOH
• Happens continuously and is unregulated
• Final 15% of water ( 27 L) ab- sorbed in CD under hormonal control
• Fluid entering loop of Henle is isotonic to extracellular fluids
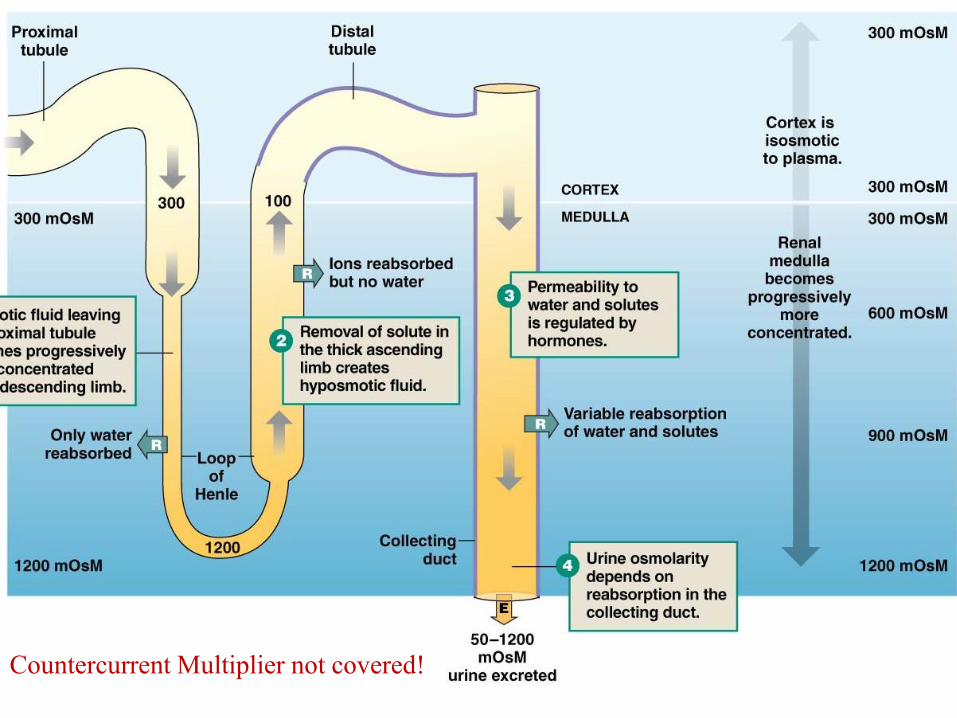
Countercurrent Multiplier not covered!
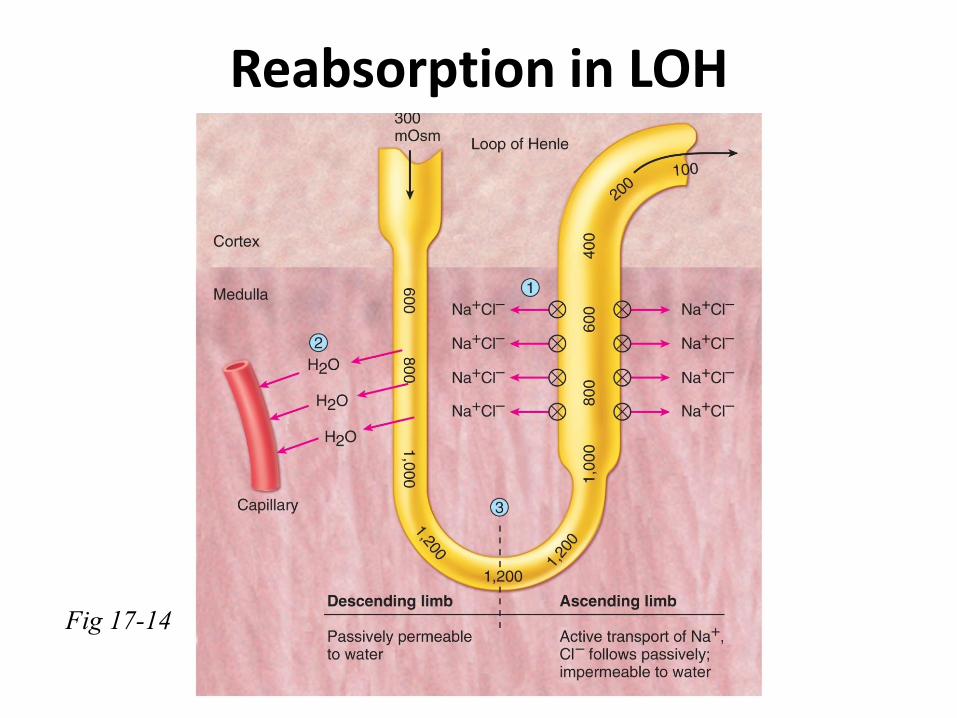
Reabsorption in LOH
Fig 17-14
Renal Medulla Creates Concentrated Urine
Reabsorption of varying amounts of H2O and Na+ established by LOH and CD
How is H2O absorbed? Only by _______________ due to the high medullary interstitial osmolarity
Key player: ADH = ____________, or________
• Body fluid osmolarity : ________? • Urine osmolarity can vary from 50 to 1200 mOsm.
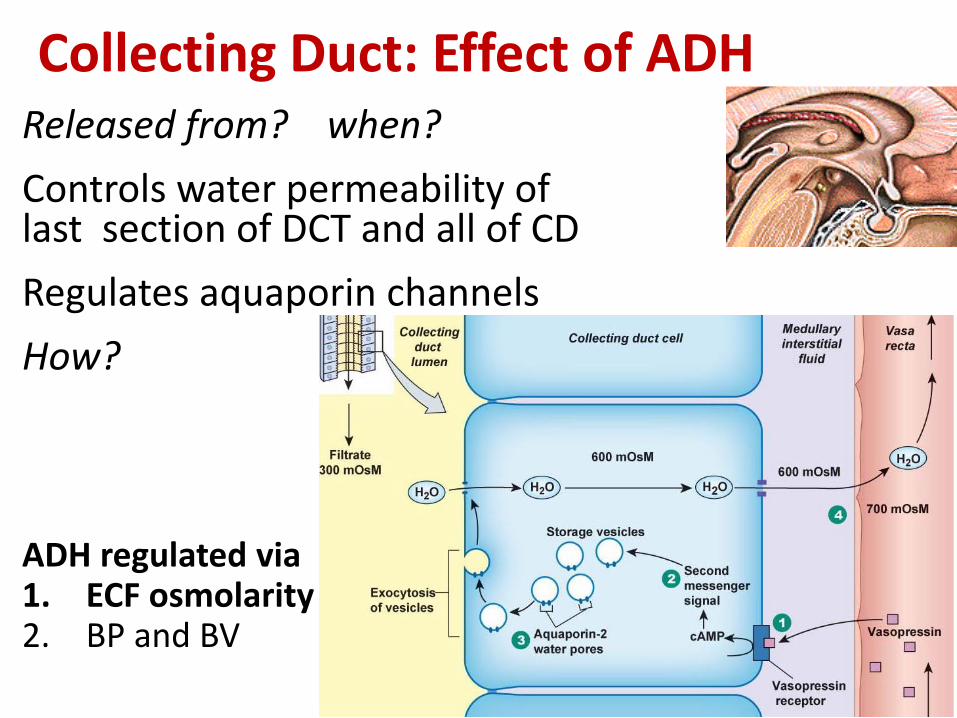
Released from? when?
Controls water permeability of last section of DCT and all of CD
Regulates aquaporin channels
How?
ADH regulated via 1. ECF osmolarity 2. BP and BV
Collecting Duct: Effect of ADH
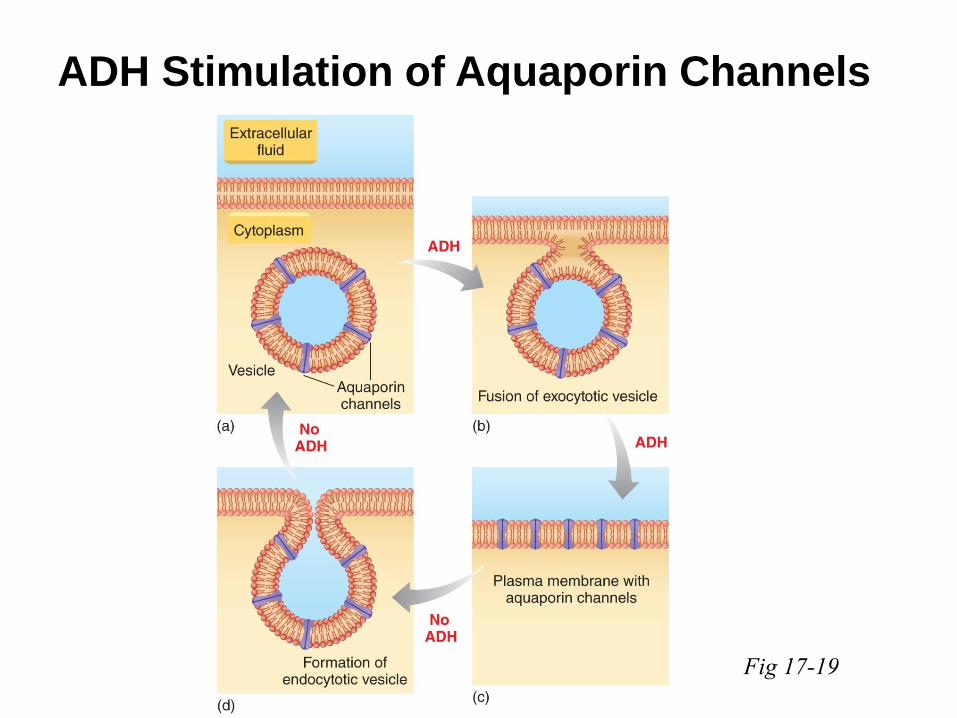
ADH Stimulation of Aquaporin Channels
Fig 17-19
Diabetes insipidus
Nocturnal enuresis
Clinical Application
A. Neurogenic / Central:
B. Nephrogenic:
C. Also: Dipsogenic and gestational
Desmopressin for A and C
Concentrated vs. Dilute Urine In presence of ADH:
Insertion of H2O pores
At maximal H2O permeability: Net H2O movement stops at equilibrium
Maximum osmolarity of urine?
No ADH:
DCT & CD impermeable to H2O
Osmolarity can plunge to ~ 50 mOsm
Review:
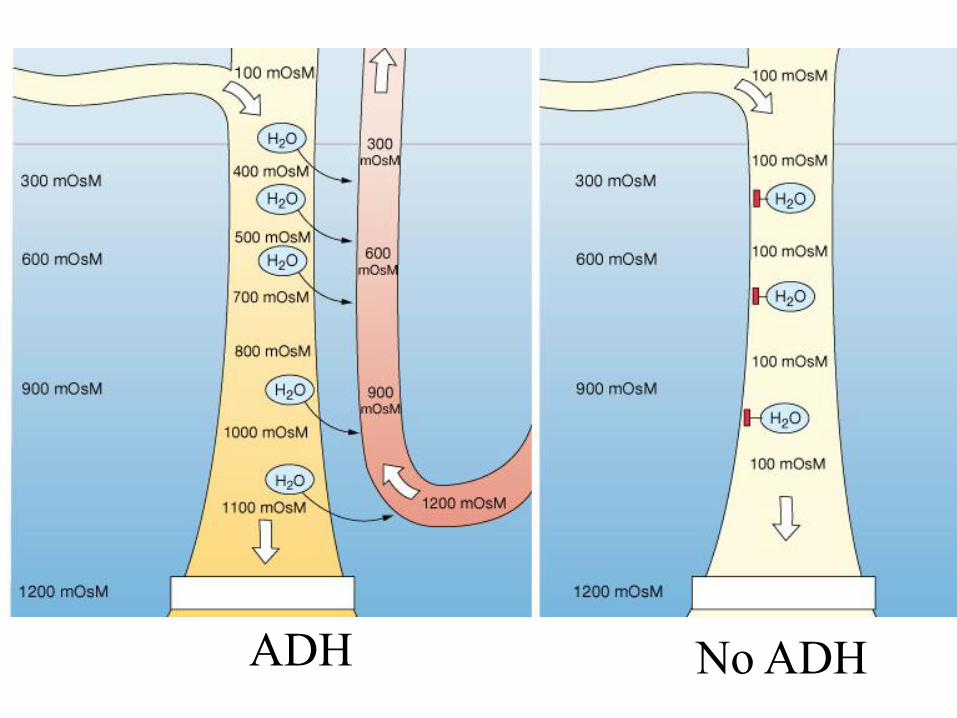
ADH No ADH
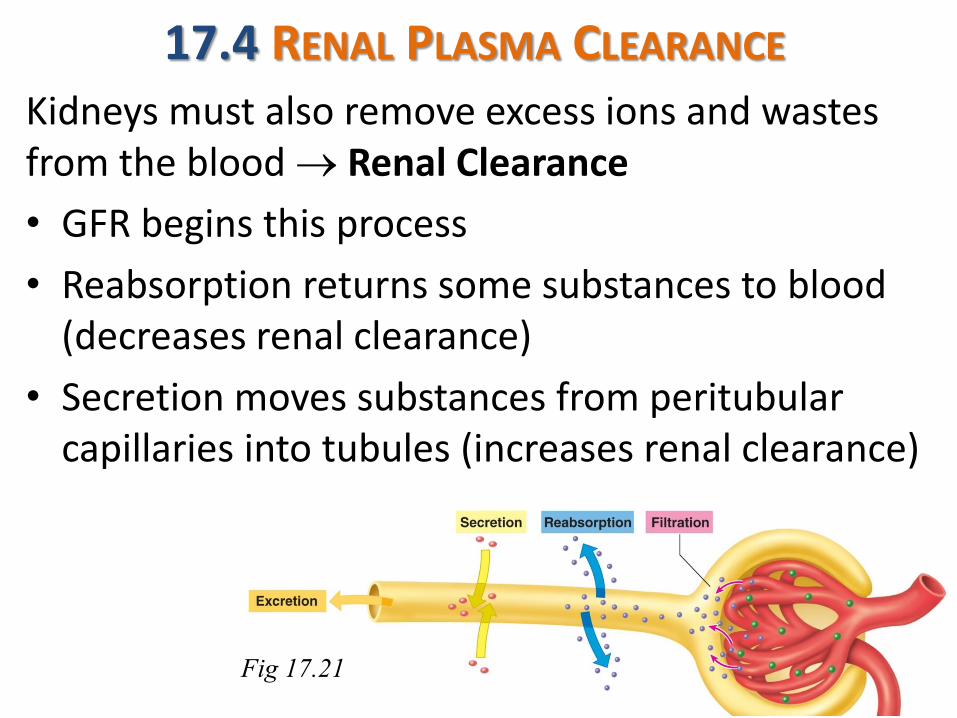
17.4 RENAL PLASMA CLEARANCE Kidneys must also remove excess ions and wastes from the blood Renal Clearance
• GFR begins this process
• Reabsorption returns some substances to blood (decreases renal clearance)
• Secretion moves substances from peritubular capillaries into tubules (increases renal clearance)
Fig 17.21
Clinical Importance of GFR and Clearance
GFR is indicator for overall kidney function
Clearance → non-invasive way to measure/estimate GFR (creatinine and inulin)
If substance is filtered and reabsorbed but not secreted clearance rate > or ?< GFR
If substance is filtered and secreted but not reabsorbed clearance rate > or ?< GFR
Inulin used as markers of glomerular filtration rate because it is filtered but not reabsorbed or secreted
Easier to use Creatinine
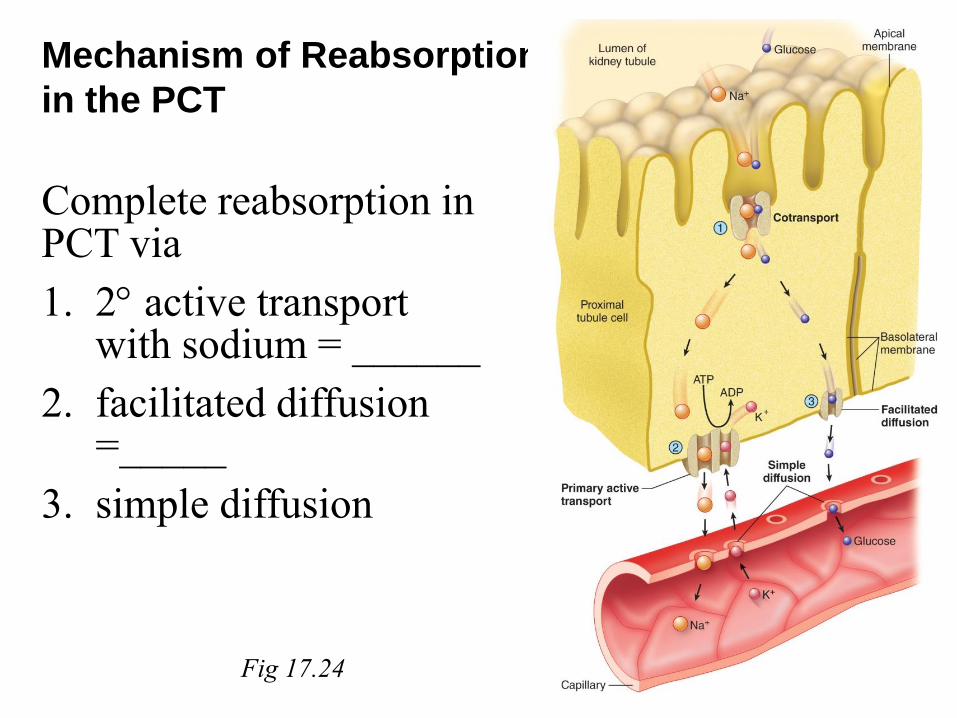
Mechanism of Reabsorption
in the PCT
Complete reabsorption in PCT via
1. 2 active transport with sodium = ______
2. facilitated diffusion =_____
3. simple diffusion
Fig 17.24
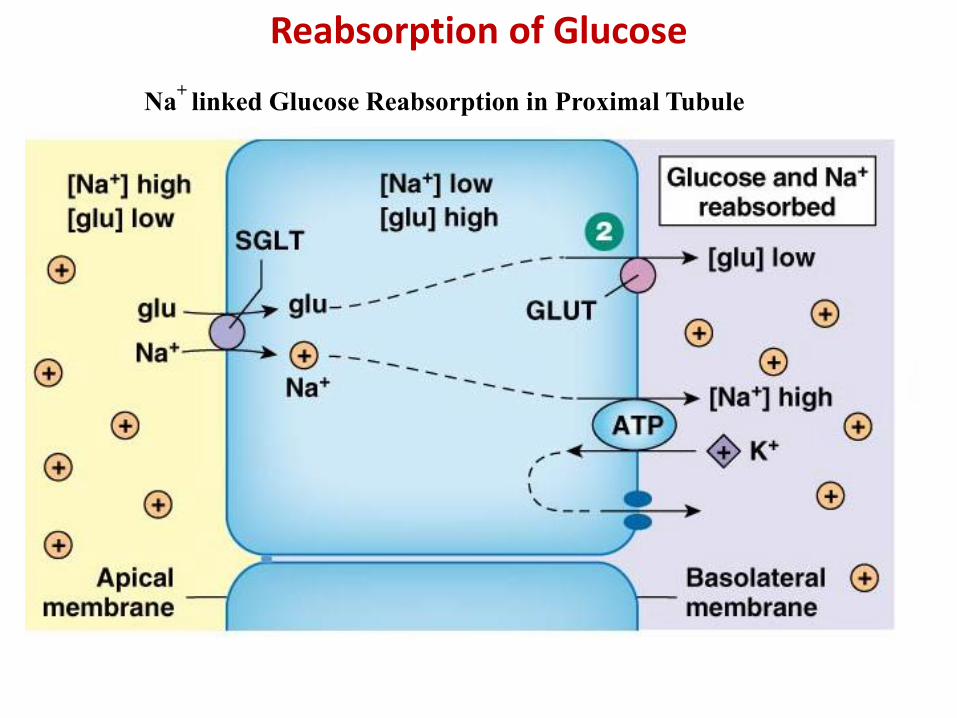
Reabsorption of Glucose
Na+
linked Glucose Reabsorption in Proximal Tubule
Characteristics of Renal Transport
As in all mediated transport
Transport maximum determined by
1. Specificity
2. Competition
3. Saturation Renal threshold, determines transport maximum.
Copyright © 2010 Pearson Education, Inc.
Saturation of Mediated Transport
Fig 19-9
Copyright © 2010 Pearson Education, Inc.
Glucose Handling by the Nephron
Fig 19-10
Glycosuria
Diabetes mellitus Untreated DM → high blood glucose levels → …
→ Osmotic Diuresis
→ Polyuria and polydipsia
Similarities and
differences to
diabetes insipidus ?
Secretion
2nd route of entry into tubules for selected molecules
Mostly transepithelial transport (analogous to reabsorption). Depends mostly on membrane transport systems (usually 2o active transport)
Provides mechanism for rapid removal of substances . Most important for H+, K+, foreign organic ions and drugs such as penicillin etc.)
Excretion = Urine Output Excretion of H2O, excess ions, nitrogenous waste,
toxins, and other foreign molecules
Depends on F, R, S (formula ?)
Direct measurement of F, R, S impossible infer from blood & urine analysis
Kidneys clean or “clear” plasma of certain substances
For any substance: Clearance = plasma volume completely cleared of that substance per minute
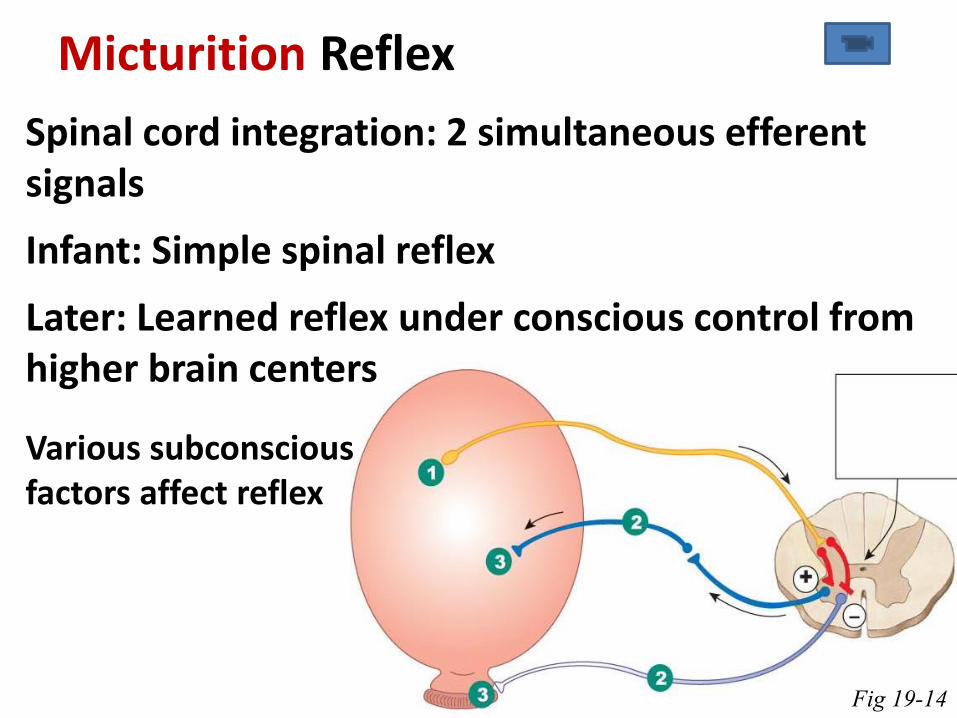
Micturition Reflex
Spinal cord integration: 2 simultaneous efferent signals
Infant: Simple spinal reflex
Later: Learned reflex under conscious control from higher brain centers
Various subconscious factors affect reflex
Fig 19-14
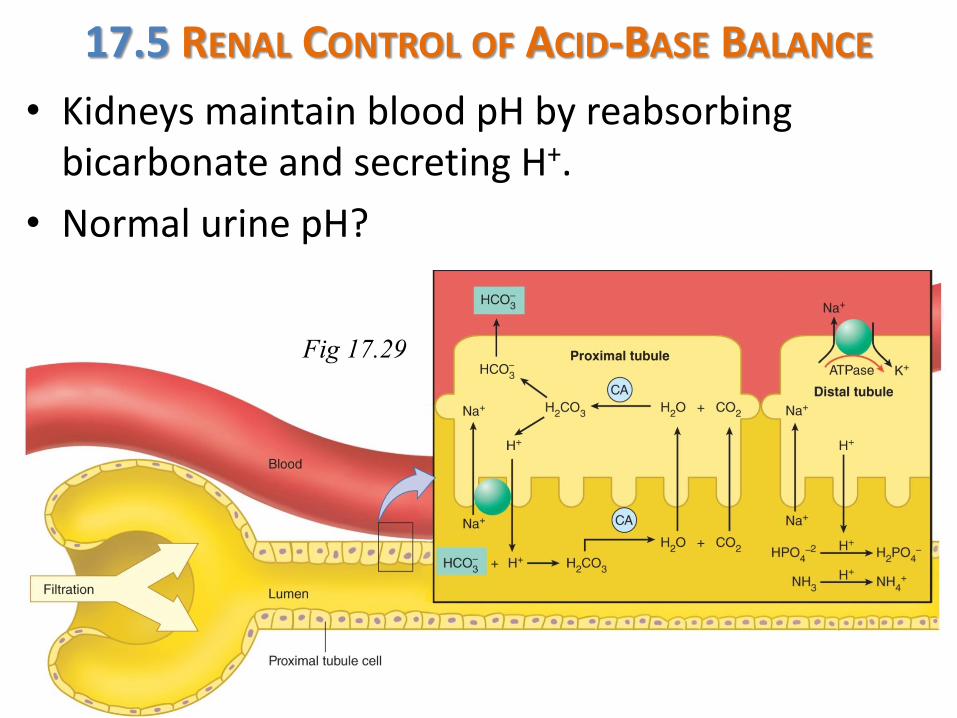
17.5 RENAL CONTROL OF ACID-BASE BALANCE
• Kidneys maintain blood pH by reabsorbing bicarbonate and secreting H+.
• Normal urine pH?
Fig 17.29
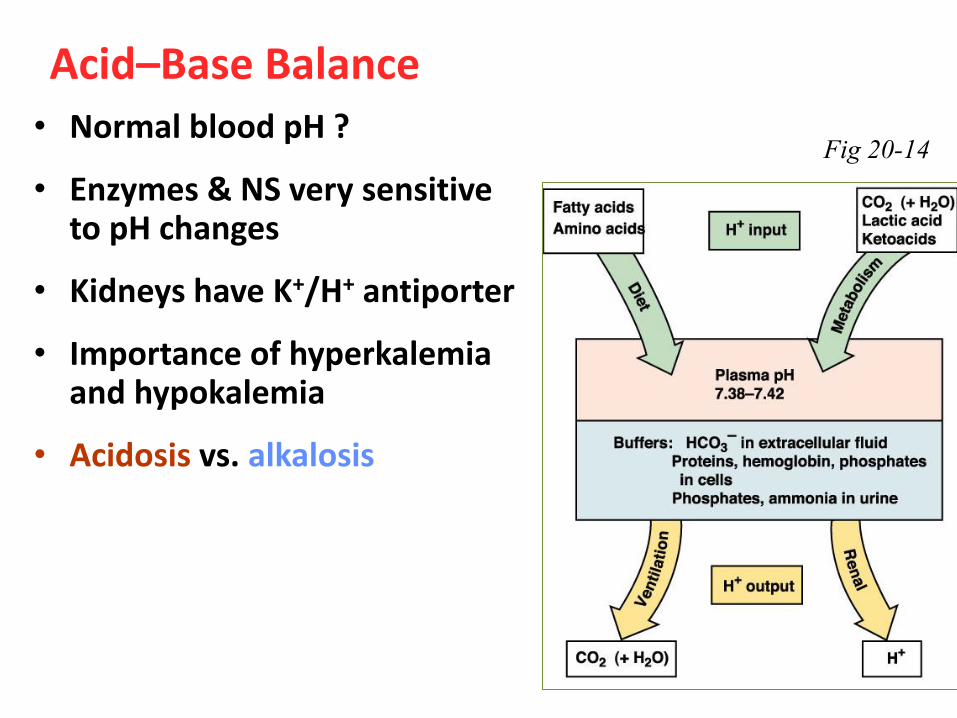
Acid–Base Balance • Normal blood pH ?
• Enzymes & NS very sensitive to pH changes
• Kidneys have K+/H+ antiporter
• Importance of hyperkalemia and hypokalemia
• Acidosis vs. alkalosis
Fig 20-14
Acidosis Respiratory acidosis due to alveolar hypoventilation
→ accumulation of ______
Possible causes: Respiratory depression, increased airway resistance (___________), impaired gas exchange (___________, ______________, _____________ ____________, _______________________________)
Metabolic acidosis due to gain of fixed acid or loss of bicarbonate
Possible causes: lactic acidosis, ketoacidosis, diarrhea
Buffer capabilities exceeded once pH change appears in plasma. Options for compensation?
3 Mechanisms to Deal with pH Changes
Buffers 1st defense, immediate response
Ventilation 2nd line of defense, can handle ~ 75% of most pH disturbances
Renal regulation of H+ & HCO3-
final defense, slow but very effective
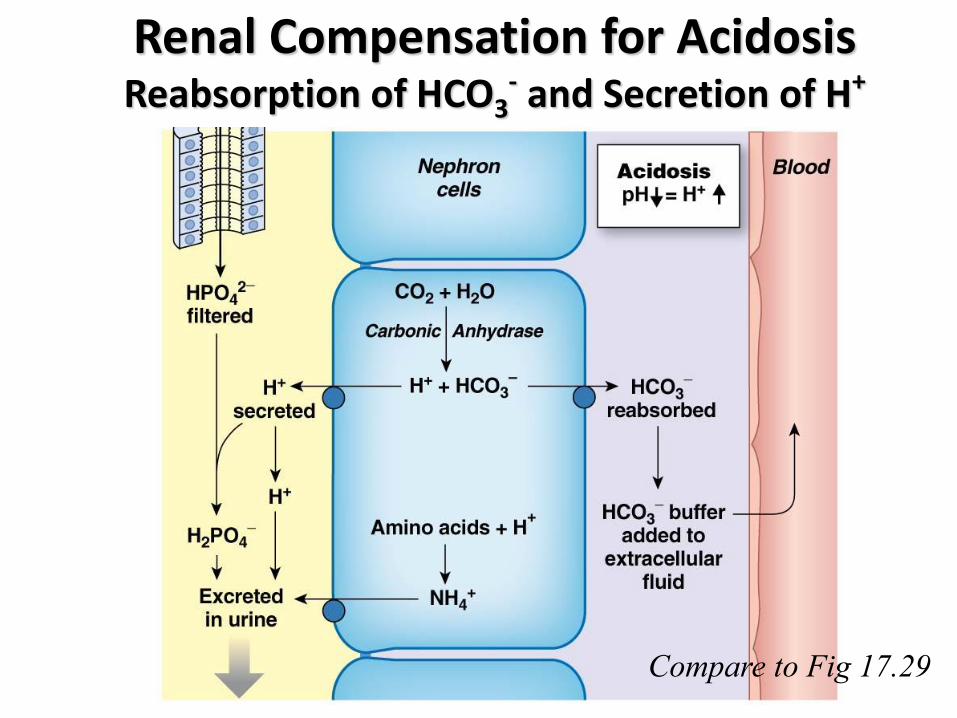
Renal Compensation for Acidosis Reabsorption of HCO3
- and Secretion of H+
Compare to Fig 17.29
Alkalosis much rarer
Respiratory alkalosis due to alveolar hyperventilation in the absence of increased metabolic CO2 production
Possible causes: Anxiety with hysterical hyperventilation, excessive artificial ventilation, aspirin toxicity, fever, high altitude
Compensation?
Metabolic alkalosis due to loss of H+ ions or shift of H+ into the intracellular space.
Possible causes: Vomiting or nasogastric (NG) suction; antacid overdose
Compensation?
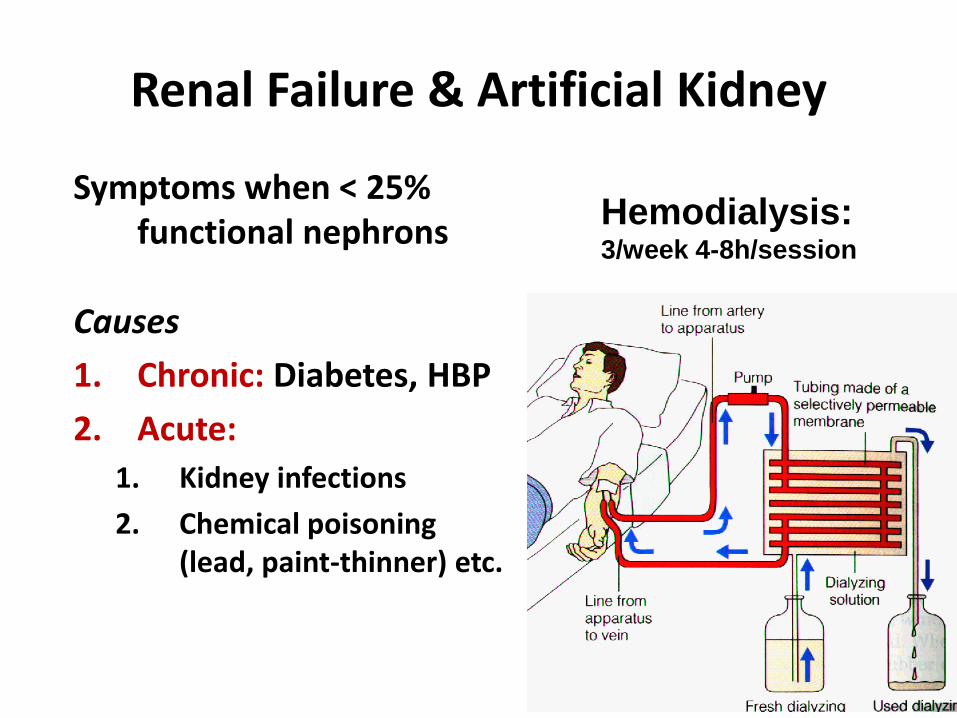
Renal Failure & Artificial Kidney
Symptoms when < 25% functional nephrons
Causes
1. Chronic: Diabetes, HBP
2. Acute:
1. Kidney infections
2. Chemical poisoning (lead, paint-thinner) etc.
Hemodialysis:
3/week 4-8h/session
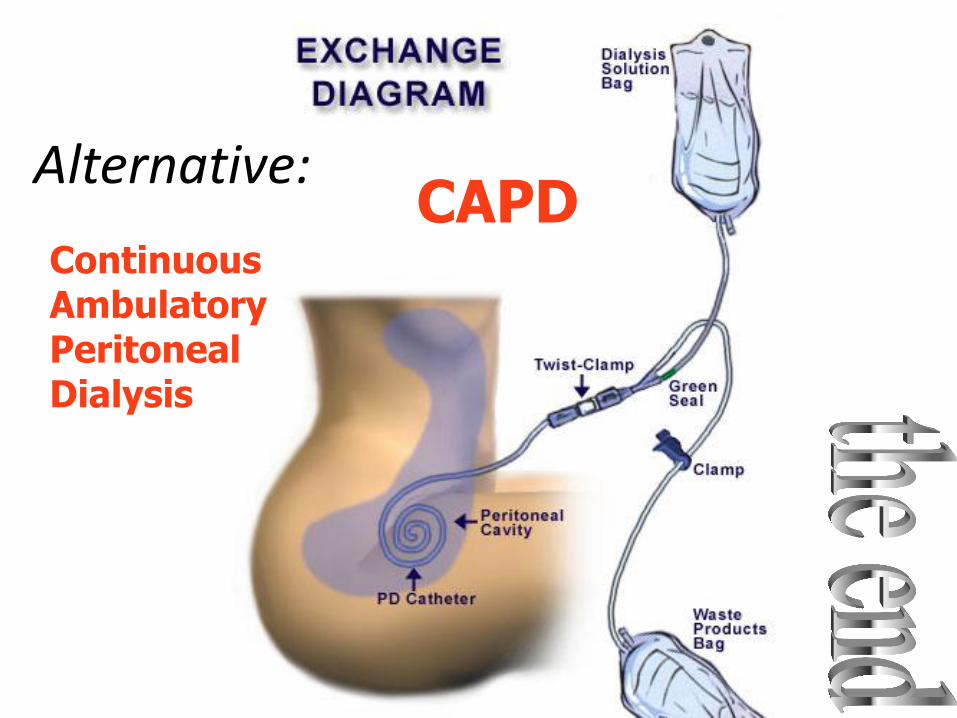
CAPD Alternative:
Continuous Ambulatory Peritoneal Dialysis







![Lew Cirne, FS16 Keynote [FutureStack16]](https://img.pdfslide.net/doc/110x75/5870d95b1a28ab64768b7441/lew-cirne-fs16-keynote-futurestack16.jpg)