Embed Size (px)
Citation preview

C H A P T E R
44
Thrombocytopenia in PregnancyKeith R. McCrae
Department of Hematologic Oncology and Blood Disorders, Lerner College of Medicine,
Cleveland Clinic, Cleveland, Ohio
I. INTRODUCTION
Thrombocytopenia in pregnant patients may resultfrom many causes, including “incidental” thrombo-cytopenia, immune thrombocytopenic purpura (ITP),hypertensive disorders such as preeclampsia, thesyndrome of hemolysis, elevated liver enzymes andlow platelets (HELLP), uncommon disorders such asthrombotic thrombocytopenic purpura (TTP) and thehemolytic-uremic syndrome (HUS), and acute fattyliver of pregnancy, among others (Table 44-1). Becauseeach of these disorders may have a distinct patho-genesis, the mechanisms by which thrombo-cytopenia develops may differ. The most commoncauses of thrombocytopenia in pregnancy are inci-dental thrombocytopenia and thrombocytopenia asso-ciated with hypertensive disorders. Though in eachof these the degree of thrombocytopenia is generallymild, this does not diminish the importance of accu-rate diagnosis in facilitating optimal patientmanagement.
The clinical manifestations of some causes of preg-nancy-associated thrombocytopenia may overlap soextensively that it may be difficult, if not impossible,to distinguish them from each other. However, sincethe management of these disorders is critically depen-dent upon defining the cause as accurately as possible,familiarity with the more common causes of thrombo-cytopenia in this population is essential for physicianswho care for pregnant patients. The goal of thischapter is to provide an overview of these disorders.For additional discussions of pregnancy-associatedthrombocytopenia, the reader is referred to recentreviews.1�4
II. SPECIFIC CAUSES OF PREGNANCY-ASSOCIATED THROMBOCYTOPENIA
A. Incidental Thrombocytopenia of Pregnancy
1. Definition and Clinical Characteristics
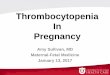
“Incidental” thrombocytopenia, referred to by someauthors as “gestational” thrombocytopenia, is the mostcommon cause of thrombocytopenia in pregnancy,affecting 6�7% of pregnant women and accounting formore than two thirds of all cases of pregnancy-associ-ated thrombocytopenia5�8 (Fig. 44-1). Women with thisdisorder usually develop mild thrombocytopenia in thelate second or third trimester, with platelet countsgenerally remaining above B1003 109/L. While thereis no absolute minimum platelet count below whichincidental thrombocytopenia may be excluded, the like-lihood of incidental thrombocytopenia diminishes as theplatelet count falls below this value, and most expertsconsider other diagnoses (e.g., immune thrombocytope-nic purpura [ITP]) equally if not more likely when plate-let counts fall below approximately 703 109/L.6
Patients with gestational thrombocytopenia are oth-erwise healthy, with no history of ITP or other autoim-mune disorders. Serologic studies such as antinuclearantibody tests and antiphospholipid antibodies aregenerally negative,6 and physical examination does notreveal hypertension or findings associated with othercauses of pregnancy-induced thrombocytopenia.
2. Platelet Counts in Normal Pregnancy:Implications for Incidental Thrombocytopenia
The pathogenesis of incidental thrombocytopeniais uncertain but may involve hemodilution and/or
909Platelets, 3rd edition © 2013 Elsevier Inc. All rights reserved.

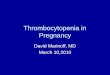
accelerated platelet clearance in the placental circula-tion.1,6,9 In at least some patients, the diagnosis of inci-dental thrombocytopenia likely reflects a “physiologic”decrease in the platelet count associated with preg-nancy. Several large, population-based studies havedemonstrated that in uncomplicated pregnancies, theplatelet count decreases by approximately 10% byterm; in one study,10 the mean platelet count in 6,770pregnant patients near term was 2133 109/L,
compared to 2483 109/L in nonpregnant controls. The2.5th percentile in the pregnant group, used to definethe lower limit of a “normal” platelet count, was1163 109/L.10 Similar results were obtained in anotherstudy involving 4,382 pregnant women, in which the5th percentile for the platelet count was 1233 109/L.11
These changes in mean platelet counts are shown by ashift to the left in the histogram of the platelet countdistribution (Fig. 44-2).10 In these studies, 7.3%11 and11.6%10 of pregnant women had platelet counts belowthe normal lower limit of 1503 109/L, as defined fornonpregnant populations, and were considered throm-bocytopenic. In another study of 2,263 pregnantwomen, the mean platelet count of the 1,357 womenconsidered normal was 2253 109/L, and 8.3% of theseindividuals had platelet counts below 1503 109/L.7
This high incidence of “thrombocytopenia” in preg-nant patients accounts for the fact that incidentalthrombocytopenia is the second most common hema-tologic complication of pregnancy, following anemia.
3. Management
Patients with incidental thrombocytopenia are notat increased risk for poor pregnancy outcomes ordelivery of thrombocytopenic offspring,5�7,12,13 and forthis reason evaluation of an otherwise healthy preg-nant woman with mild thrombocytopenia occurringbeyond the mid-second trimester may be limited tocareful assessment for the presence of hypertensionand/or proteinuria.6,14 However, offspring of womenwith suspected incidental thrombocytopenia shouldhave an umbilical cord platelet count determined, incase the maternal thrombocytopenia was a conse-quence of mild ITP (see following text). Incidentalthrombocytopenia remits after the pregnancy ends,often within several days, but almost always within2 months.1,6,11,15
B. Immune Thrombocytopenia Purpura
1. Incidence in Pregnancy
ITP is characterized by the presence of circulatingantiplatelet glycoprotein antibodies that cause acceler-ated clearance of platelets by the reticuloendothelialsystem, primarily the spleen (see Chapter 40 for fur-ther details).16�18 In some patients, these antibodiesmay also affect megakaryocytes, inhibiting plateletproduction.19�21 ITP affects approximately 0.1�1.0 ofevery 1,000 pregnancies and accounts for 3�5% ofcases of pregnancy-associated thrombocytopenia; thus,it is 50�100-fold less common than incidental throm-bocytopenia.17 However, ITP is the most commoncause of isolated thrombocytopenia occurring earlyin pregnancy, particularly in the first trimester.1,5,22,23
TABLE 44-1 Causes of Thrombocytopenia in Pregnancy
Pregnancy-Specific Not Pregnancy-Specific
Incidental thrombocytopenia ofpregnancy
Immune thrombocytopenicpurpura
Preeclampsia/eclampsia Thrombotic microangiopathies
HELLP syndrome Thrombotic thrombocytopenicpurpura
Acute fatty liver of pregnancy Hemolytic-uremic syndrome
Systemic lupus erythematosus
HIV infection
Other viral infections(e.g., CMV, EBV)
Antiphospholipid antibodies
Disseminated intravascularcoagulation (DIC)
Bone marrow dysfunction
Nutritional deficiencies
Drug-induced thrombocytopenia
Type IIB von Willebrand disease
Congenital hypersplenism
Abbreviations: CMV, cytomegalovirus; EBV, Epstein�Barr virus; HELLP,
hemolysis, elevated liver enzymes and low platelets; HIV, human
immunodeficiency virus.
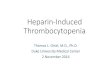
Other 13%
Incidental 66%
ITP-Immune 3%
Hypertension 18%
FIGURE 44-1 Frequency of causes of thrombocytopenia inpregnant women. Incidental refers to incidental thrombocytopeniaof pregnancy, also known as gestational thrombocytopenia.Hypertension includes preeclampsia, eclampsia, and HELLP.(Adapted with permission from Reference 7.)
910 44. THROMBOCYTOPENIA IN PREGNANCY
IV. DISORDERS OF PLATELET NUMBER AND FUNCTION

2. Clinical and Laboratory Diagnosis
Patients with ITP, whether pregnant or not, maypresent in a variety of ways. Those with more severethrombocytopenia may be symptomatic and experi-ence petechiae, purpura, or other bleeding manifesta-tions. Those with mild thrombocytopenia are mostoften asymptomatic. There are no “gold-standard” lab-oratory studies for ITP, and the diagnosis of this disor-der remains one of exclusion (Chapter 40).24�26
A history of thrombocytopenia preceding the preg-nancy is helpful in diagnosing ITP,27 as is a history ofautoimmune disease or the presence of more severethrombocytopenia (platelet count ,503 109/L).23,28
Increased levels of platelet surface-associated IgG arenonspecific and may be increased in incidental throm-bocytopenia as well as in other pregnancy-associatedthrombocytopenic disorders.29 Contemporary anti-platelet glycoprotein antibody assays, though less sen-sitive, are somewhat more specific but do not excludeITP if the tests are negative.6,11,16,18 Guidelines recentlypublished by an International Working Group considerantimaternal immunoglobulin to be of no value in rou-tine diagnosis of ITP during pregnancy.25
ITP associated with mild thrombocytopenia may beindistinguishable from incidental thrombocytopenia.1
Though ITP may occur at any time during pregnancy,a platelet count below 1003 109/L in the first trimes-ter, with continued decline as pregnancy progresses, ismost consistent with this disorder,23 while mildisolated thrombocytopenia first noted in the secondor third trimester that is not associated with
hypertension or proteinuria most often results fromincidental thrombocytopenia.
3. Management of the Pregnant Patient with ITP
Though patients with ITP who are contemplatingpregnancy should be counseled concerning potentialcomplications and neonatal thrombocytopenia, it isgenerally not necessary to advise these individualsagainst pregnancy.25 Though antiplatelet glycoproteinantibodies in patients with ITP may cross the placentaand in some cases induce neonatal thrombocytopenia(see Chapter 45), therapy for pregnant patients withITP should be dictated by the maternal platelet countand clinical manifestations. Throughout the first andsecond trimesters, patients with a platelet countabove approximately 20�303 109/L, who are notbleeding, do not require treatment.14,18,25�27,30 As termapproaches, closer monitoring of the platelet count isrequired, and more aggressive therapy may be indi-cated to raise the platelet count to a level that allows forsafe administration of epidural anesthesia and mini-mizes the risk of hemorrhage during delivery.31
Though there is no level 1 evidence defining the exactplatelet count at which such procedures are safe, mostexperts consider a platelet count of . 503 109/L ade-quate for either vaginal delivery or cesarean section.18,27
Although epidural anesthesia has been administeredsuccessfully in patients with very low plateletcounts,32,33 and most hematologists believe thatthis mode of anesthesia is safe at platelet counts. 503 109/L, current guidelines suggest that the
25%
Per
cent
age
of w
omen
20%
15%
10%
5%
0%
<50
50–7
4
75–9
9
100–
124
125–
149
150–
174
175–
199
200–
224
225–
249
250–
274
275–
299
300–
324
325–
349
350–
374
375–
399
400–
424
425–
449
450–
474
475–
499
>500
Platelet count (G/I)
Control womenPregnant women
FIGURE 44-2 Histogram of platelet counts of pregnant and nonpregnant women. (Reproduced with permission from Reference 10.)
911II. SPECIFIC CAUSES OF PREGNANCY-ASSOCIATED THROMBOCYTOPENIA
IV. DISORDERS OF PLATELET NUMBER AND FUNCTION

platelet count be raised to. 753 109/L prior to deliveryof epidural anesthesia.14,25,34 In many cases treatmentcan be deferred through the first and second trimestersof pregnancy but initiated during the late third trimes-ter 1�3 weeks prior to the expected date of delivery.
Though many physicians employ corticosteroidsas first-line therapy for ITP in pregnant patients,these agents are associated with unique pregnancy-associated toxicities such as gestational diabetes, accel-erated osteoporosis, pregnancy-induced hypertension,and perhaps premature rupture of the fetal mem-branes.18,27,35 These considerations have led some toadvocate the use of high dose (2 gm/kg) intravenousimmunoglobulin (IVIG) as initial therapy for pregnantwomen with ITP.22 Current guidelines recommendeither corticosteroids or IVIG as appropriate first-linetherapies during pregnancy.25,26 Although approxi-mately 70% of both pregnant and nonpregnantpatients with ITP respond to IVIG, these responses areoften of short duration, and multiple courses of ther-apy may be required to maintain an adequate plateletcount throughout pregnancy. Thus, although the opti-mal first-line therapy for ITP in pregnancy remainscontroversial, it is generally agreed that corticosteroidsshould be used judiciously, and IVIG considered ifpatients require prolonged therapy with an unaccept-ably high maintenance dose of corticosteroid.34 Oneapproach suggests that if treatment is not neededuntil the late third trimester, corticosteroids should beconsidered; however, if therapy must be initiated ear-lier in pregnancy and the expectation for prolongedtreatment exists, then therapy should be initiated withIVIG.27
Intravenous anti-D was used successfully and safelyin eight Rh(D)-positive pregnant patients with intactspleens and a median gestational age of 34 weeks.36
Six of these eight patients responded, with one com-plete and five partial responses (coincident therapywas administered in four patients). None of the neo-nates had hemolytic anemia. Thus, despite the positivedirect antiglobulin test results in a fraction of theseneonates, it is likely that the majority of the anti-Dimmunoglobulin is adsorbed to circulating maternalred cells, thus minimizing its transplacental passageand potential to cause hydrops in the fetus.25
Pregnant patients who are refractory to corticoster-oids and/or IVIG may either be treated medically orundergo splenectomy. Splenectomy is associated withan initial response rate of 75�85% in both pregnantand nonpregnant patients.25,26,34,37 The second trimes-ter is the optimal time for splenectomy, as proceduresearlier in pregnancy may be associated with a higherincidence of premature labor, and at later pointsin pregnancy the surgical field may be obscuredby the gravid uterus.34 Laparoscopic splenectomy
may be performed safely during pregnancy and associ-ated with a lower complication rate than openprocedures.37
Additional medical therapy may be used eitherprior to splenectomy or in patients in whom splenec-tomy is unsuccessful. Some individuals with refractoryITP may respond to high-dose “pulse” corticosteroids(methylprednisolone, 1 gm IV) with or without IVIG(2 gm/kg).14 For those who do not respond to thisapproach, additional immunosuppressive agents maybe considered.34 Most experts suggest the avoidance ofpotentially teratogenic agents such as danazol, cyclo-phosphamide, or vinca alkaloids.25,26 Azathioprine hasbeen used in pregnant patients without teratogenic-ity,25 although not specifically for ITP.26,38 Rituximabinduces complete or partial remissions in B50% ofnonpregnant patients with ITP.39�41 There havebeen several reports of the use of rituximab in preg-nancy, primarily for non-Hodgkin’s lymphoma,23,42
though a recent report demonstrated efficacy in preg-nancy-associated ITP.43 Rituximab delays neonatal B-cell maturation, which may not normalize for 4�9months.
4. Management of Thrombocytopenia in theNewborn of a Mother with ITP
Due to the transplacental passage of antiplateletantibodies, maternal ITP may cause neonatal thrombo-cytopenia. Approximately 10% of the offspring ofmothers with ITP will be born with a platelet count, 503 109/L, and 1�5% will be severely thrombocyto-penic with platelet counts , 203 109/L.44 However,although 25�50% of severely thrombocytopenic neo-nates experience bleeding during delivery, intracranialhemorrhage is rare (,1.0%).4,12,18 There is no noninva-sive means to determine which neonates will be bornthrombocytopenic, since neither the maternal plateletcount, results of platelet antibody tests, response ofmaternal ITP to therapy, or a number of other para-meters predict neonatal thrombocytopenia.23 The bestpredictor of neonatal thrombocytopenia appears to bea previous history of neonatal thrombocytopenia in asibling.35,45,46
The inability to determine the fetal platelet countnoninvasively has led to debate concerning the use ofpercutaneous umbilical cord blood sampling (PUBS) todetermine the fetal platelet count, with the aim ofdelivering neonates with platelet counts , 503 109/Lby cesarean section and avoiding potential cranialtrauma during traversal of the birth canal. PUBS isassociated with a neonatal morbidity (bleeding and/orfetal bradycardia requiring emergent cesarean section)of approximately 1%, which is equal to or greater thanthat of fetal intracranial hemorrhage during vaginaldelivery.44 Moreover, although a low risk of fetal
912 44. THROMBOCYTOPENIA IN PREGNANCY
IV. DISORDERS OF PLATELET NUMBER AND FUNCTION

intracranial hemorrhage exists with any deliverymethod, there is no evidence that this is reduced bycaesarean section.47 Based on these considerations,most perinatologists now advocate the use of cesareansection for maternal indications only.48 This opinionis advocated by recent International and AmericanSociety of Hematology guidelines.25,26
The risk of neonatal intracranial hemorrhage in theoffspring of patients with ITP may be greatest duringthe first few days after delivery, as platelet counts mayfall further over this period. Thus, all offspring ofmothers with ITP should have a cord platelet countobtained, as well as close monitoring of the plateletcount during the first postpartum week. A cranialsonogram should also be considered for severelythrombocytopenic infants.25,26,34 Treatment of severeneonatal thrombocytopenia with IVIG is generallyeffective, and life threatening bleeding should be trea-ted with platelet transfusion and IVIG (see alsoChapter 45).25
C. Preeclampsia and the HELLP Syndrome
1. Preeclampsia: Incidence and Definition
Preeclampsia affects approximately 6% of all preg-nancies, most often those of primigravidas less than 20or greater than 30 years of age,49 and accounts for17.6% of maternal deaths in the United States.50
National data indicate that a woman’s risk for devel-oping preeclampsia increases by 30% for each addi-tional year of age beyond 34.51
Diagnostic criteria for hypertensive disorders ofpregnancy have been defined by the NIH WorkingGroup on High Blood Pressure in Pregnancy (2000).52
This family of disorders consists of (1) chronic hyper-tension, which includes patients with hypertensionpreceding but exacerbated by pregnancy; (2) pre-eclampsia-eclampsia (discussed further later); (3) pre-eclampsia superimposed on chronic hypertension, thecategory that usually includes patients with the mostsevere illness; (4) gestational hypertension, defined ashypertension developing after 20 weeks of pregnancybut not associated with proteinuria; this classificationmay include transient cases, in which the hypertensionresolves by 12 weeks postpartum; and (5) chronichypertension, in which hypertension persists formore than 12 weeks postpartum.52,53
The diagnostic criteria for preeclampsia includehypertension (blood pressure $ 140/90 mm Hg) andproteinuria ($300 mg/24 hours, or at least 11 on adipstick urine analysis) developing after 20 weeks ofgestation and noted on at least two separate occasionsat least 6 hours apart. Patients with severe preeclamp-sia have a higher blood pressure ($160/110 mm Hg)
and more proteinuria ($5 gm/24 hours).54 Thesepatients have evidence of end organ damage and maydisplay a number of additional manifestations includ-ing headache, visual disturbances, pulmonary edema,right upper quadrant or epigastric pain, oligohydram-nios, and fetal intrauterine growth retardation.53
Eclampsia is defined by the occurrence of grand malseizures occurring antenatally or within 7 days ofdelivery in patients with preeclampsia, and compli-cates 1 in every 2,000�3,000 pregnancies in the UnitedStates.55
2. Preeclampsia: Genetic Associations
Women with a family history of preeclampsia pos-sess a three-fold greater risk of developing the disor-der than those that lack such a history and are morelikely to have a mother as opposed to a mother-in-law who has had preeclampsia.51 Interestingly, pater-nal genetic factors are also involved; both men andwomen who were the products of a pregnancy compli-cated by preeclampsia are significantly more likely tohave a child who is also the product of a pregnancyassociated with preeclampsia.56 Moreover, changedpaternity is a risk factor for the development of pre-eclampsia in multiparous women,57 although a morerecent study suggests that this association may reflecta longer duration between pregnancies.58 A history ofprolonged cohabitation between parents appears to beassociated with a decreased risk of preeclampsia.59,60
Recent studies have attributed approximately 35% ofthe susceptibility to preeclampsia to paternal factors,and large cohort studies are beginning to define singlenucleotide polymorphisms (SNPs) that associate withpreeclampsia.61
Despite these findings, several studies examininglikely candidate genes have been unrevealing. Onerecent study genotyped 657 women affected by pre-eclampsia and their families for SNPs in the genesencoding angiotensinogen, angiotensin receptors, fac-tor V Leiden, methylene tetrahydrofolate reductase(MTHFR), nitric oxide synthase, and tumor necrosis-alpha (TNF-α), but found that none of theseconferred an increased risk of disease.62 Additionalstudies failed to define relevant polymorphisms inthe genes for vascular endothelial cell growth factor(VEGF) or toll-like receptor 4 (TLR4).63,64 A system-atic review of the immunogenetics of preeclampsiaconcluded that the HLA-DR locus (particularly DR4)was a correlate of preeclampsia, though it has beenuncertain whether any specific HLA allele, haplotype,or susceptibility genes in linkage disequilibrium withthe HLA region were responsible.65 Polymorphismsof the 3’ untranslated region of the HLA-G generemain of interest.66
913II. SPECIFIC CAUSES OF PREGNANCY-ASSOCIATED THROMBOCYTOPENIA
IV. DISORDERS OF PLATELET NUMBER AND FUNCTION

3. Preeclampsia: Pathogenesis
Prominent risk factors for this disorder mayreflect underlying vascular disease, including preexist-ing hypertension, diabetes, and insulin resistance.Testosterone levels and African-American ethnicity areadditional risk factors.60 Obesity has also been recog-nized as an increasingly important risk factor for thedevelopment of preeclampsia.67
Several reports suggest that thrombophilic condi-tions may represent risk factors for preeclampsia. Ofthe acquired thrombophilic conditions, available evi-dence most strongly supports a role for antiphospholi-pid antibodies, which may be associated with asyndrome of early onset, severe preeclampsia.68�70 Anassociation of preeclampsia with inherited thrombophi-lia has been suggested by some studies,71�73 but notothers,74,75 and current dogma suggests that inheritedmaternal thrombophilias have a weak, if any, influenceon the development of preeclampsia.76,77 Fetal inheritedthrombophilias have also been suggested as contribut-ing to the pathogenesis of preeclampsia, but no relation-ship between common fetal inherited thrombophiliasand maternal preeclampsia has been convincinglydemonstrated.74,78,79
Though the clinical manifestations of preeclampsiausually do not appear until the third trimester, thepathophysiology of this disorder involves deficientremodeling of the maternal uterine vasculature earlyin pregnancy. In normal pregnancy, placental cytotro-phoblasts invade through the superficial decidualtissue and remodel the maternal uterine spiralarteries to the depth of the myometrium.80 In contrast,cytotrophoblast invasion is shallow in preeclampsia,often limited to the superficial decidua.81,82
Cytotrophoblast cells appear to modulate their pheno-type during uterine invasion, with the more invasivecells switching their pattern of adhesion moleculeexpression to one that more closely reflects a vascularphenotype (i.e., integrin αVβ3, VE-cadherin).82,83 In pre-eclampsia, invasive cytotrophoblasts may retain the“pro-adhesive” pattern of adhesion molecule expres-sion characteristic of less invasive trophoblast cells,leading to diminished remodeling of the uterine spiralarteries.82 Isolated trophoblasts from preeclampticpatients may also be deficient in their expression ofother invasion-related factors such as matrix metallo-proteases.84 A number of other hypotheses concerningthe role of the innate and adaptive systems in the patho-genesis of preeclampsia have emerged, primarily focus-ing on the role of deficient activation of uterine NK cellsand the elaboration of inflammatory cytokines thatimpair angiogenesis by decidual macrophages.85
Deficient trophoblast invasion and remodeling ofthe maternal uterine vasculature lead to placental
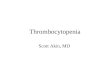
hypoperfusion.87�89 Indeed, the gene expressionprofiles of placentae from preeclamptic patients mayresemble those of placentae from high-altitude preg-nancies or from first-trimester placental explantscultured under hypoxic conditions.86 Placental hypo-perfusion may result in the release of placental factorsthat induce the systemic endothelial dysfunction char-acteristic of preeclampsia (Fig. 44-3).91 A factor ofsignificant pathogenic importance in preeclampsia issFLT1, a soluble form of VEGFR-1, which binds andneutralizes VEGF-A and placental growth factor(PLGF).92�97 VEGF-A and PLGF are essential to mainte-nance of endothelial homeostasis during pregnancy,and decreased levels of free VEGF and placental VEGFcontribute to the endotheliopathy, particularly in thekidney. Other factors generated in the preeclampticplacenta that mediate systemic manifestations of thedisorder include endoglin, endothelin 1, and reactiveoxygen species.92�95 Abnormalities in levels of sFLT1,PLGF, and endoglin have been identified in the firsttrimester of pregnancy, suggesting utility in predictingpreeclampsia, although the clinical value of thisapproach remains uncertain.96
A recent study identified mutations in three comple-ment regulatory proteins—membrane cofactor protein(MCP), factor I (CFI), and factor H (CFH)—in 7 of 40patients with SLE or antiphospholipid antibodies whodeveloped preeclampsia.97 Five of these patients hadrisk variants previously associated with the atypicalhemolytic uremic syndrome (aHUS, see Chapter 43).These findings suggest that a diminished ability to reg-ulate complement activation on cell surfaces may con-tribute to the pathogenesis of preeclampsia in somepatients with autoimmune disorders.
4. Preeclampsia: Thrombocytopenia andMicroangiopathic Hemolytic Anemia
Approximately 15�50% of patients with preeclamp-sia develop thrombocytopenia, the extent of which isgenerally proportional to the severity of disease.98 Thepathogenesis of preeclampsia-associated thrombocyto-penia is likely multifactorial. The elevated levels ofthromboxane A2 metabolites in the urine of preeclamp-tic patients, as well as the increased plasma levels ofthe platelet α-granule proteins β-thromboglobulin andplatelet factor 4 support the argument that plateletactivation is a cause of accelerated platelet clearance inthis disorder.53 Although only the most severe cases ofpreeclampsia are associated with a coagulation profilesuggestive of disseminated intravascular coagulation(DIC), the plasma of most patients with preeclampsiacontains increased levels of thrombin-antithrombincomplexes, and approximately 40% of these plasmascontain increased levels of fibrin D-dimers, suggesting
914 44. THROMBOCYTOPENIA IN PREGNANCY
IV. DISORDERS OF PLATELET NUMBER AND FUNCTION

that subclinical activation of the coagulation systemoccurs.98,99 Thus, increased generation of thrombinmay be one mechanism that promotes platelet activa-tion.99 Platelets may also be stimulated through contactwith dysfunctional endothelium and/or exposed sub-endothelium underlying the injured placental vascula-ture. Platelet adhesion may be promoted by reducedlevels of ADAMTS-13100 as well as elevated levels ofvon Willebrand factor (VWF)101,102 and other adhesiveproteins such as cellular fibronectin.103
Preeclampsia-associated thrombocytopenia may pre-cede other clinical manifestations of the syndrome.104
Thus, preeclampsia must be included in the differentialdiagnosis of a falling platelet count in the third trimes-ter of pregnancy.98
Patients with preeclampsia also display microangio-pathic hemolytic anemia (MAHA). However, the extentof MAHA is relatively low compared to disorders suchas HELLP, TTP, or HUS.
5. HELLP: Definition and Association withPreeclampsia
The HELLP (hemolysis, elevated liver function tests,low platelets) syndrome complicates 20% of pre-eclampsia cases and is considered by some to be a pre-eclampsia variant. However, based on several featuresof HELLP not shared by preeclampsia, some haveargued that it may be a distinct disorder.105 The crite-ria for diagnosis of HELLP are not entirely consis-tent.106,107 In general, HELLP is defined by (1)hemolysis, (2) elevated liver enzymes, and (3) low
platelets. Hemolysis manifests as MAHA, which isgenerally more severe than that occurring in pre-eclampsia, and the serum haptoglobin is reduced in85�97% of cases.108 The extent of hepatic enzyme ele-vation required for a diagnosis of HELLP is an area ofdisagreement, but most experts accept an aspartateaminotransferase (AST) level $ 70 U/L (or appro-ximately two times the upper limit of the normallaboratory value).109 Likewise, disagreement exists con-cerning the degree of thrombocytopenia necessary fora diagnosis of HELLP, although the majority of reportsaccept a platelet count , 1003 109/L. Finally, mostauthors consider an LDH value of $ 600 U/L as a nec-essary part of the syndrome. One group has classifiedHELLP into three subcategories (referred to by someas the “Mississippi” classification) based on the sever-ity of thrombocytopenia. Patients with class 1 HELLPhave a platelet nadir below 503 109/L; patients withclass 2 HELLP, a nadir between 513 109/L and1003 109/L; and patients with class 3 HELLP, a nadirbetween 1013 109/L and 1503 109/L.110 This classifi-cation scheme is useful in predicting the rapidity ofpostpartum recovery of platelets and the need forplasma exchange. Some authors consider patients whohave some but not all manifestations of HELLP to have“partial” HELLP syndrome.107
The pathogenesis of HELLP remains poorly under-stood. The association with preeclampsia, increasedsFLT1, and decreased PLGF levels, and similar pla-cental pathology in patients with HELLP and pre-eclampsia suggests that similar mechanisms underlie
Genetic factors
↑ Oxidative stress
Immunological/InflammatoryNK cells/AT-1 receptor AA
Abnormal Placentation
Reduced Placental Perfusion
Other maternal factors
Systemic vascular dysfunctionCapillary leak/vasospasm
ProteinuriaGlomerular Endotheliosis
Hypertension Thrombocytopenia
?
Stage II(3rd trimester)
Stage I(1st and 2nd
trimesters)SGA infant
↑ sFlt-1 ↑ sEng↓ VEGF ↓ PlGF
Other maternal factors
Systemic vascular dysfunctionCapillary leak/vasospasm
FIGURE 44-3 Schematic representation of potential pathogenic pathways and their effects in preeclampsia. Abbreviations: AA, agonis-tic autoantibodies; AT-1, angiotensin 1; NK, natural killer; PlGF, placental growth factor; sEng, soluble endoglin; sFlt-1, soluble FMS-like tyro-sine kinase 1; SGA, small for gestational age; VEGF, vascular endothelial growth factor. (Adapted from Reference 90.)
915II. SPECIFIC CAUSES OF PREGNANCY-ASSOCIATED THROMBOCYTOPENIA
IV. DISORDERS OF PLATELET NUMBER AND FUNCTION

the development of both disorders. However, as inpregnancy-associated aHUS (see following text), recentstudies have identified mutations in genes encodingproteins that regulate the alternative complement path-way in patients with HELLP.111,112 The incidence ofthese mutations in HELLP and their correlation withclinical aspects of the disorder requires further study.
6. HELLP: Diagnosis and Clinical Characteristics
HELLP has been reported to affect 0.17�0.85% of alllive births, and occurs most commonly in a slightlyolder population than preeclampsia, with a mean ageof 25 years.108 In 70% of cases, HELLP is diagnosedantepartum, primarily between 27 and 37 weeks ofgestation; 30% of cases develop postpartum.113 Thepercentage of nulliparous patients ranges from 52% to81%, a lower proportion than those with preeclamp-sia.108,114 HELLP syndrome, particularly when it devel-ops early in pregnancy,115,116 may be associated withantiphospholipid antibodies in some patients.117,118
Patients with HELLP characteristically present withnonspecific complaints, including nausea, fatigue, andmalaise. Right upper quadrant and epigastric pain isthe most common symptom, occurring in 86�92% ofpatients; in occasional patients right upper quadrantpain may precede the onset of liver enzyme abnor-malities.108,114 Thus, patients with HELLP may be mis-takenly diagnosed with a primary gastrointestinaldisorder, particularly since only 50�70% of thesepatients have hypertension at the time of presentation;the differential diagnosis in a patient with such mani-festations is wide (Table 44-2). Patients may haveaccompanying edema, and 5�15% have no or minimalproteinuria; 15% may have neither hypertension norproteinuria.106,108 Patients who present with HELLPpostpartum usually do so within several days afterdelivery,119 with 6% of these individuals having noantepartum signs of preeclampsia.108
The classic liver lesion in HELLP syndrome consistsof periportal or focal parenchymal necrosis, with peri-portal hemorrhage and fibrin deposition in the liversinusoids.120,121 Necrosis may arise from liver ischemiaand may contribute to the characteristic right upperquadrant pain.122 Dissection of necrosis into the livercapsule may lead to the development of subcapsularhemorrhage and hepatic rupture.119
7. HELLP: Maternal Morbidity
Like preeclampsia, HELLP is associated with signifi-cant maternal and neonatal morbidity.123 It has beensuggested by some but not all studies that the maternaloutcomes of patients with HELLP are worse than thosewith severe preeclampsia.107 In many series, patientswith partial or full-blown HELLP are analyzedtogether, making the assessment of outcomes
problematic.107 Patients with class I HELLP have thegreatest morbidity, which, in addition to hepatic necro-sis, may include acute renal failure, pulmonary edema,abruptio placentae, intracerebral bleeding, and retinaldetachment.107 Fetal outcomes may be worse in off-spring of mothers with more severe thrombocytope-nia.124 Visual defects that develop in the course ofHELLP may in some cases be permanent.125
8. HELLP: Thrombocytopenia
The thrombocytopenia that accompanies HELLP isgenerally more severe than that of preeclampsia. It hasbeen reported that the rate of fall of the platelet countis a predictor of the eventual severity of HELLP, withpatients whose platelet counts decrease by.503 109/Lper day having a higher probability of developingclass 1 or 2 HELLP.126 There appears to be a correla-tion between the extent of thrombocytopenia and thedegree of liver dysfunction in patients with HELLP,as suggested by the HELLP classification schemedescribed previously. The platelet nadir is usuallyreached approximately 24 hours postpartum,108 withnormalization occurring within 6�11 days.127 As withpreeclampsia, the thrombocytopenia of the HELLP syn-drome likely reflects a multifactorial pathogenesis.Activation of platelets in contact with damagedendothelium is a likely scenario, as is consumptionof platelets secondary to thrombin generation.114
TABLE 44-2 Differential Diagnosis of the HELLP Syndrome
Gastrointestinal
Acute fatty liver of pregnancy
Cholelithiasis
Nephrolithiasis
Pancreatitis
Peptic ulcer disease
Appendicitis
Hepatitis
Gastroenteritis
Hematologic
Idiopathic thrombocytopenic purpura (ITP)
Thrombotic thrombocytopenic purpura (TTP)
Hemolytic-uremic syndrome (HUS)
Other
Hyperemesis gravidarum
Pyelonephritis
Diabetes insipidus
916 44. THROMBOCYTOPENIA IN PREGNANCY
IV. DISORDERS OF PLATELET NUMBER AND FUNCTION

Clinically apparent DIC complicates approximately 6%of cases of HELLP, as opposed to 1�2% of patients withpreeclampsia, although significant decreases in thefibrinogen level and elevated levels of fibrin degrada-tion products are not generally seen until the plateletcount is, 503 109/LL.119
9. HELLP: Neonatal Implications
HELLP is associated with a 10�20% fetal mortality,as well as substantial morbidity.128 Some neonatesmay have mild thrombocytopenia, although thismay not be apparent until after delivery. The patho-genesis of neonatal thrombocytopenia, though oftenattributable to routine causes such as sepsis and prema-turity, may also involve deficient platelet production.1
This may result, in part, from relatively low erythropoi-etin levels and/or impaired megakaryocyte responsesto erythropoietin.
10. Management of Preeclampsia and theHELLP Syndrome
The first step in the management of patients withpreeclampsia or HELLP is stabilization of the patient,with the goal of preparing the patient for definitivetreatment—delivery of the fetus. Intravenous magne-sium sulfate is administered as seizure prophylaxis,and acute hypertension is most commonly treatedwith hydralazine.129 While conservative managementof patients with evidence of mild preeclampsia may beattempted until fetal lung maturity is achieved or until38 weeks of gestation, emergent therapy is usuallyemployed for patients with severe preeclampsia, withor without superimposed HELLP.53,130 After maternalstabilization, the fetal status should be assessed, andpatients with severe preeclampsia or HELLP who arebeyond 34 weeks’ gestation should undergo urgentdelivery.119 If evidence of fetal lung maturity is notpresent, betamethasone should be administered anddelivery attempted after an additional 48 hours.50,119
While some have advocated more conservative man-agement, there is no evidence that fetal or maternaloutcomes have been improved by this approach.106
Most patients managed conservatively continue todeteriorate and may be exposed to additional compli-cations.106,107 The presence of HELLP or severe pre-eclampsia is not an absolute indication for cesareansection, and vaginal delivery may be employed in theabsence of obstetric contraindications.
Though platelet survival is reduced in patients withpreeclampsia or HELLP, platelet transfusion may beused to raise the platelet count in order to allow epidu-ral anesthesia and/or cesarean section. While there isno definitive study defining what is an adequate plate-let count for either of these procedures, most expertsconsider a platelet count of . 503 109/L to be
adequate for cesarean section, while a platelet countbetween 703 109/L to 1003 109/L has been recom-mended for epidural anesthesia.14,25,34 DIC should beconsidered in patients with bleeding, a prolonged pro-thrombin time, elevated levels of fibrin(ogen) degrada-tion products, and/or decreased fibrinogen.
Uncontrolled studies have suggested that antepar-tum or postpartum administration of corticosteroids,primarily dexamethasone, leads to a more rapid recov-ery of biochemical laboratory values and improvementof the platelet count in patients with HELLP131,132 andincreases the probability of successful labor inductionand candidacy for regional anesthesia.133,134 However,two prospective, randomized placebo-controlled trialsdemonstrated that postpartum administration of corti-costeroids did not benefit patients with severe pre-eclampsia who did not have HELLP,135 nor did theyreduce maternal morbidity or mortality in a group of105 women with HELLP randomized to receive pla-cebo or 20 mg of dexamethasone daily.136
11. Postpartum HELLP
Although the manifestations of preeclampsia or theHELLP syndrome generally remit within several daysafter delivery, occasional patients may experience pro-gressive disease after delivery. The management ofsuch individuals is not well defined. Though in a ret-rospective study, Martin et al.132 reported that steroidshastened the resolution of postpartum HELLP in43 women who received them in comparison to237 women who did not, these findings were not con-firmed in prospective studies.136 Plasma exchangewith fresh frozen plasma has also been employed inpatients with postpartum HELLP. In a study of7 patients with postpartum HELLP persisting for atleast 72 hours after delivery, Martin et al.137 reportedthat plasma exchange led to sustained increases in theplatelet count and a decrease in LDH. In a subsequentstudy, 18 patients with postpartum HELLP weredivided into two groups: group 1 included 9 womenwith persistent HELLP syndrome more than 72 hoursafter delivery, while group 2 included 9 women withworsening HELLP syndrome and evidence of organdysfunction at any time after delivery.138 While allgroup 1 patients responded to plasma exchange,responses in group 2 were inconsistent, and 2 deathsoccurred. A more recent study compared the outcomesof 29 patients with HELLP treated with plasmaexchange and found a decreased length of stay in theintensive care unit, a more rapid improvement in theplatelet count and biochemical abnormalities, anddecreased mortality in the patients treated with plasmaexchange compared to historical controls.139 Thus,although plasma exchange has not been subjected tocontrolled studies in HELLP, its use in progressive
917II. SPECIFIC CAUSES OF PREGNANCY-ASSOCIATED THROMBOCYTOPENIA
IV. DISORDERS OF PLATELET NUMBER AND FUNCTION

postpartum disease is reasonable. Potential mechan-isms by which plasma exchange might improve thecourse of HELLP could include replenishment ofADAMTS13, which is decreased in some patients withthis disorder.140
12. Recurrent HELLP in Subsequent Pregnancies:Incidence and Prevention
The risk of recurrence of preeclampsia or HELLP insubsequent pregnancies is of major concern. In a studyof primigravid women whose pregnancies were com-plicated by severe preeclampsia or eclampsia, secondpregnancies were complicated by mild preeclampsia in19.5%, severe preeclampsia in 29.5%, and eclampsia in1.4%.128 The risk declined in subsequent pregnanciesyet remained significantly higher than control patientswho had never experienced preeclampsia. The risk ofrecurrent HELLP has been collated by Barton et al.107
and is summarized in Table 44-3. In patients whoexperienced a pregnancy complicated by HELLP, therisk of recurrent HELLP in subsequent pregnanciesranges from 3 to 19%, with a risk of preeclampsia ofapproximately 20%.141�144 In a recent cohort of 128patients with a history of HELLP, Habli et al. reportedthat in 53 subsequent pregnancies, HELLP recurred in24% and preeclampsia in 28%.145
Given the high incidence, significant recurrencerates, and morbidity associated with preeclampsia,extensive effort has been devoted to the identificationof strategies to prevent recurrent disease. Based on thepremise that platelets play a primary role in the patho-genesis of preeclampsia, the ability of aspirin to inhibitthe development of preeclampsia has been studied. Ina metaanalysis of 31 randomized trials, aspirin wasfound to reduce the incidence of preeclampsia byapproximately 10%.146 A recent study suggested thatthe addition of low molecular weight heparin mayincrease the efficacy of aspirin.147 Interest has alsofocused on the use of antioxidants.148 However,
vitamin C or E147,149 failed to inhibit the developmentof preeclampsia.150 While calcium has shown someefficacy in reducing the incidence of preeclamp-sia,151,152 other nutrients including zinc, selenium, folicacid, and magnesium have not been shown to beefficacious.150
D. Thrombotic Thrombocytopenic Purpuraand the Hemolytic-Uremic Syndrome
1. TTP: Incidence and Clinical Diagnosis
TTP (see also Chapter 43) is a rare disorder with anincidence of 6.5 cases per million annually153 and apeak incidence in the fourth decade. The disorder ismore common in females (female/male ratio 3:2).154
Other risk factors include African ancestry, obesity,and type O blood group.155�157
TTP is defined by a classic pentad of symptoms thatinclude MAHA, thrombocytopenia, neurologic symp-toms, fever, and renal dysfunction. However, whileonly 40% of patients display the entire pentad ofsymptoms, 75% present with the triad of MAHA,neurologic symptoms, and thrombocytopenia.158
Neurological symptoms generally predominate in TTPand may range from headache and confusion to sei-zures or coma.158�160 Thrombocytopenia is often severe,with platelet counts below 203 109/L.158,159 Renal dys-function is generally mild in patients with TTP.160
MAHA and compensatory reticulocytosis are centralfeatures of TTP. Markedly increased levels of LDHresult from hemolysis and tissue ischemia, and an ele-vated ratio of LDH to AST may be useful in distinguish-ing TTP from the HELLP syndrome.161 Thepathogenesis of TTP involves either inherited oracquired deficiencies of ADAMTS13, a critical enzymeinvolved in regulating cleavage of ultra-large vonWillebrand factor complexes into smaller multimers(see Chapter 43 for details).162,163
TABLE 44-3 Pregnancy Outcome after HELLP in Normotensive Women
Reference Number of
Women
Number of Subsequent
Pregnancies
Preeclampsia (% of Subsequent
Pregnancies)
HELLP (% of Subsequent
Pregnancies)
Sibai et al.143 139 192 19 3
Sullivan et al.144 122 161 23 19
Van Pampuset al.142
77 92 16 2
Chames et al.141 a 40 42 52 6
Habli et al.145 128 53 28 24.5
(Adapted from Reference 108.)aHELLP #28 weeks in previous pregnancy.
918 44. THROMBOCYTOPENIA IN PREGNANCY
IV. DISORDERS OF PLATELET NUMBER AND FUNCTION

2. HUS: Clinical Manifestations and Comparisonwith TTP
Patients with HUS (see also Chapter 43) may displaythe same pentad of symptoms as patients with TTP,although in contrast to TTP, renal failure generally pre-dominates and CNS symptoms are less pronounced.164
However, symptoms of TTP and HUS overlap substan-tially, and in some cases these disorders may be diffi-cult to distinguish.16,165 Pregnancy-specific thromboticmicroangiopathies may also be easily confused witheither of these disorders.1,2,167 However, although thereare no universally accepted classification schemes forthese thrombotic microangiopathies, better understand-ing of the pathogenesis of TTP and HUS has allowedproposals for pathophysiology-based classificationschemes. While there are three major subtypes of TTP—inherited, idiopathic, and nonidiopathic (bothacquired)163—there are two primary variants of HUS—diarrhea-associated (D)1 or “typical” HUS, which ismore common in childhood and is associated withgastroenteritis caused by shiga toxin-expressingbacteria,168�170 and inherited “atypical” HUS (aHUS),which is associated with deficiencies of or mutations incomplement regulatory proteins (see Chapter 43 fordetails). aHUS occurs sporadically, though pregnancyis a common precipitant.171
Thrombocytopenia in patients with aHUS is gener-ally less severe than in classic TTP, although upto 60% of patients require dialysis. From apractical perspective, the initial therapeutic approachto management of both disorders is similar.172
The incidence of both TTP and HUS is increased inpregnant patients.99,173 In some series 10�20% of allcases of TTP or HUS have occurred in pregnantindividuals.174
3. ADAMTS13 in Thrombotic Microangiopathiesduring Pregnancy
An inherited or acquired deficiency of ADAMTS13,a VWF-cleaving metalloprotease, underlies thedevelopment of TTP.175,176 Levels of ADAMTS13 aremarkedly decreased in most patients with TTP;ADAMTS13 levels of 5�10% of normal in the appro-priate clinical setting are considered diagnostic,although apparent cases of TTP occur even in theabsence of such severe deficiency.166,177 In patientswith acquired TTP, this deficiency results from antibo-dies against the protease,175,176 while patients withinherited forms of TTP harbor mutations in theADAMTS13 gene.162,163,178 In the absence of TTP, mildto moderately decreased levels of ADAMTS13 occur inseveral settings,179 including pregnancy.180 The level ofADAMTS13 drops progressively from the 12th throughthe 16th week of normal pregnancy to the puerperium,
and nulliparas have somewhat lower levels ofADAMTS13 than parous women. The mean level ofADAMTS13 measured at term was 52% in one study(range 22�89%).181
A severe deficiency of ADAMTS13 with impairedcleavage of ultra-large VWF multimers (ULVWF) leadsto increased levels of circulating ULVWF in the plasmaof patients with TTP.182 These ULVWF multimerscause agglutination of platelets in the microvascula-ture, particularly at areas of high shear stress whereULVWF may undergo conformational change.183
Whether the increased incidence of TTP in pregnantpatients reflects the pregnancy-related decrease inplasma ADAMTS13 is uncertain; while these levels donot decrease to the extent seen in patients with estab-lished TTP, pregnancy is also characterized byincreased levels of VWF.184,185 One study reported thatADAMTS13 levels in patients with HELLP were alsosignificantly lower than those in healthy pregnantpatients,140 although these individuals did not havesevere deficiency. Patients with HUS have not beenfound to have decreased levels of ADAMTS13.183
4. Time of Onset of TTP and HUS duringPregnancy
Pregnancy-associated HUS develops most com-monly in the postpartum period. In one series, themean time from delivery to the onset of symptomswas 26.6 days,186 a finding that helps to distinguishHUS from other causes of pregnancy-associatedMAHA and thrombocytopenia, such as preeclampsiaand HELLP. TTP appears to have a variable timeof onset. In the classic series of Weiner et al., 40 of45 cases of TTP developed antepartum with a meangestational age of 23.5 weeks.186 Similar findings werereported by Martin et al. in a retrospective analysis of166 patients; 55.5% of patients presented in the secondtrimester, 11.7% during the first, and 32.8% during thethird.187 In contrast, another retrospective reviewfound that the time of greatest risk for development ofTTP or HUS was at term or postpartum.2 Several casereports confirm the fact that TTP may develop as earlyas weeks 22�28 of pregnancy.174,188�190
5. Management of TTP and HUS
Unlike preeclampsia and HELLP, termination ofpregnancy does not lead to resolution of TTP orHUS.187,191,192 However, TTP responds equally wellto plasma-based therapy in pregnant and nonpregnantpatients.1 While the mortality of TTP exceeds 90%without treatment, survival exceeds 80% in patientswho receive plasma exchange (Chapter 43).172,193 Aprospective trial reported in 1991 demonstrated thatplasma exchange is superior to plasma infusion in thetreatment of patients with TTP,194 and thus in the
919II. SPECIFIC CAUSES OF PREGNANCY-ASSOCIATED THROMBOCYTOPENIA
IV. DISORDERS OF PLATELET NUMBER AND FUNCTION

absence of a known genetic deficiency of ADAMTS13,plasma exchange is the treatment of choice for this dis-order. Neurological improvement generally occursmost rapidly,160 although the platelet count may take5 days or more to improve, and weeks to return to nor-mal. Normalization of the LDH may require even lon-ger, lagging platelet normalization by a mean of 9 daysin a recent report.195 Daily plasma exchange should becontinued until symptoms have resolved and a normalplatelet count has been maintained for at least2 days.172,193 Corticosteroids are of little benefit ontheir own,196,197 and retrospective studies do not pro-vide compelling evidence that they improve theresponse to plasma exchange.197 Though their anti-inflammatory and immunosuppressive effects maymake them attractive adjunctive therapy for acquiredTTP associated with antibodies against ADAMTS13, theuse of corticosteroids in pregnancy is associated withunique toxicities.
The pathogenesis of aHUS has been linked to abnor-malities in complement regulation in approximately60% of cases (see Chapter 43 for details); these resultfrom mutations in functionally important regions ofcomplement inhibitory proteins, or with activatingmutations in Factor B or C3.198 Of the mutations thathave been identified, the most common are in comple-ment factor H (CFH; 15�30%), membrane cofactor pro-tein (MCP; 5�15%), Factor I (CFI; 3�13%), Factor B(CFB; 0�3%), and C3 (B10%).198 Additional mutationsin thrombomodulin have also been described in 3�5%of patients with HUS.199,200 A recent retrospectivestudy assessed the frequency of complement muta-tions in patients with pregnancy-associated HUS.201
Pregnancy-associated aHUS occurred in 21 of 100 adultfemale patients with aHUS; 79% of these cases occurredpostpartum. Complement abnormalities were detectedin 18 of the 21 patients. Outcomes were poor, with 62%of patients developing end stage renal disease within 1month.201
Classical therapy for pregnancy-associated aHUShas consisted of plasma exchange. Responses are rela-tively infrequent; however, they occur in occasionalindividuals. Thus, a trial of this therapy is indicated,particularly in light of the overlapping symptomsbetween TTP and aHUS.2,99,184 However, the prognosisof pregnancy-associated aHUS is poor, with a mortalityrate of 25% and chronic renal insufficiency in 50% ofsurvivors.202 In September 2011, the FDA approved theanti-C5 antibody, eculizumab, for treatment of aHUS,based on positive results in two single arm studiesof adult and pediatric patients with aHUS. Whilethere are no specific reports of the use of eculizu-mab in pregnancy-associated aHUS, these resultssuggest a new approach for treatment of thesepatients.203
6. Recurrence of TTP and HUS in SubsequentPregnancies
Patients who have experienced a pregnancy compli-cated by TTP or HUS should be counseled concerningthe risk of developing the disorder in a subsequentpregnancy. One review provided estimates of thisrisk.204 The incidence of recurrent TTP-HUS during asubsequent pregnancy in patients whose initial epi-sode of TTP-HUS had been idiopathic, and not preg-nancy-related, ranged from 43 to 91%. In patientswhose prior episode of TTP-HUS had been pregnancy-associated, the incidence of recurrent disease ina subsequent pregnancy ranged from 18 to 56%.204 Theincidence of aHUS in pregnant patients with docu-mented complement abnormalities is depicted inTable 44-4.201
In patients with a history of TTP responsive toplasma exchange, prophylactic plasma infusions havebeen effective in preventing recurrent disease in sub-sequent pregnancies.170,205
E. Other Causes of Pregnancy-AssociatedThrombocytopenia
Several other causes of pregnancy-associated throm-bocytopenia, though rare, should be noted (seeTable 44-1).
TABLE 44-4 Frequency of Pregnancy-Associated aHUSAccording to the Type of Complement Dysregulation
Patients Number of
Pregnancies
P-aHUS
(%)
CFH mutations (n5 23)a 49 10 (20%)
Mutations in SCR19-20 (n5 6) 10 1 (10%)
Mutations in other SCR(n5 17)
38 9 (24%)
CFI mutations (n5 8) 26 3 (11%)
MCP mutations (n5 4) 6 1 (17%)
C3 mutations (n5 3) 7 2 (28%)
CFB mutations (n5 2) 7 0 (0%)
More than one mutation(n5 4)b
5 3 (60%)
No mutation (n5 10) 15 3 (20%)
(From Reference 18 with permission.)aThree patients with two mutations in CFH (SCR 9 and 19)—in C3/CFH andin MCP/CFH—were excluded from the analysis.bPatients with two mutations in CFH (SCR 9 and 19)—in C3/CFH (patient 8),
in MCP/CFH (P3), and CFI/CFI (patient 4).Abbreviations: P-aHUS, pregnancy-associated aHUS; SCR, short consensus
repeat. Italicized text refers to the genes for factor H (CFH), complement C3
(C3), factor I (CFI), membrane cofactor protein (MCP), and factor B (CFB).
920 44. THROMBOCYTOPENIA IN PREGNANCY
IV. DISORDERS OF PLATELET NUMBER AND FUNCTION

1. Acute Fatty Liver of Pregnancy
Acute fatty liver of pregnancy (AFLP) is a rare dis-order with an incidence of 1 in every 7,000�16,000pregnancies.206 AFLP generally occurs in the third tri-mester, when patients present with nausea, vomiting,right upper quadrant pain, anorexia and malaise, jaun-dice and cholestatic liver dysfunction. Primiparas andwomen with twin gestations are more commonlyaffected.207�209 Decreased levels of antithrombin andfibrinogen accompanied by laboratory evidence of DICare present in most patients.209 The thrombocytopeniain patients with AFLP is characteristically mild, withan average nadir platelet count in one recent series of883 109/L, although the platelet count may occasion-ally fall to levels as low as 203 109/L.206 Maternalbleeding is common, reflecting thrombocytopeniaaccompanied by a severe coagulopathy secondary todiminished hepatic synthesis and a systemic consump-tive process.210 Some cases of AFLP and possiblyHELLP may result from fetal mitochondrial fatty acidoxidation disorders (FAODs),211 in which FAOD in thefetus induces disease in the heterozygous mother. Ofthese, the most common is a long chain 3-hydroxyacyl-CoA dehydrogenase (LCHAD) deficiency secondary toa 1528 G . C mutation.212,213 However, it is likelyFAOD accounts for only a minority of AFLP andHELLP cases.214 Therapy for AFLP involves intensesupportive care and management of the coagulopathy,followed by emergent delivery of the fetus.206,215,216
This approach has greatly improved outcomes, yetAFLP remains associated with a mortality rate ofapproximately 0.13 per 100,000 live births.217 In rarecases, maternal hepatic transplantation has beenemployed, with variable success.206 One group hasadvocated the use of plasma exchange as supportivecare following delivery.218
2. Type IIB von Willebrand Disease
Patients with type IIB von Willebrand diseaseexpress a mutant VWF molecule that causes agglutina-tion and enhanced clearance of circulating platelets.Most of the responsible mutations reside in the A1domain, resulting in a gain-of-function that leadsto increased binding of the mutant VWF to plateletglycoprotein (GP) Ibα.219 Levels of VWF in the GPIbα-binding conformation are increased at least six-fold inpatients with type IIb VWD.220 Due to the increasedlevels of VWF during pregnancy, affected patients dis-play enhanced platelet agglutination and progressivethrombocytopenia, and platelet counts may fall tolevels as low as 20�303 109/L at term.221 DDAVP(Chapter 60) is contraindicated in this disorder, as itleads to enhanced release of endogenous, mutantVWF, which can worsen thrombocytopenia.219 Patients
who require treatment usually receive VWF-rich factorVIII concentrates, which may stabilize the thrombocy-topenia. Platelet concentrates have been used with var-iable success.219
3. HIV and HCV Infection
Human immunodeficiency virus (HIV) infectionmay induce thrombocytopenia (Chapter 40) by enhanc-ing peripheral platelet destruction through the effectsof circulating immune complexes containing antibo-dies reactive with amino acids 49�66 of GPIIIa, whichmimics an epitope of the HIV nef protein.222,223
Antibodies with this reactivity may also impair mega-karyocyte differentiation,224 and the virus may directlyinfect megakaryocytes, leading to impaired thrombo-poiesis.225 Finally, patients with HIV infection developTTP with increased frequency, including duringpregnancy.190 Hepatitis C is another increasingly com-mon infectious cause of secondary immunethrombocytopenia.223,226
4. Miscellaneous Immune-MediatedThrombocytopenias
Antiphospholipid antibodies are associated with earlyonset HELLP118 and preeclampsia.51,70 Approximately10% of patients with ITP have coexisting antiphospholi-pid antibodies and comprise a subgroup of ITP patientsthat may be at increased risk for thrombotic events.227,228
Thrombocytopenia may complicate up to 25% of casesof systemic lupus erythematosus (SLE), and more thanhalf of patients with SLE may experience exacerbation oftheir disease during pregnancy.229 Drug-inducedthrombocytopenia (Chapters 41 and 42) must be consid-ered in any thrombocytopenic patient exposed to apotential offending medication.230�232
5. Congenital Thrombocytopenias
Though the majority of congenital thrombocytope-nias are diagnosed during childhood (Chapter 47),some disorders are relatively asymptomatic and cometo medical attention for the first time when thrombocy-topenia is noted during pregnancy.233 Perhaps themost common of these are the congenital macrothrom-bocytopenias characterized by mutations in the MYH9gene.234
6. Primary Hematologic Disorders
Primary hematologic disorders such as leukemias ormyelodysplastic syndromes, though uncommon inwomen of childbearing age, may occasionally presentwith isolated thrombocytopenia. Likewise, thoughchronic liver disease is uncommon in this population,patients with such disorders may develop portalhypertension leading to splenic sequestration. Finally,while uncommon in the United States, deficiencies of
921II. SPECIFIC CAUSES OF PREGNANCY-ASSOCIATED THROMBOCYTOPENIA
IV. DISORDERS OF PLATELET NUMBER AND FUNCTION

nutrients such as vitamin B12 and folic acid may leadto thrombocytopenia and/or pancytopenia in pregnantpatients.
III. SUMMARY AND CONCLUSIONS
Thrombocytopenia in the pregnant patient may havemany etiologies. The most common of these is inciden-tal thrombocytopenia of pregnancy, followed by thehypertensive disorders and the HELLP syndrome. ITPis less common, while TTP and HUS are rare.
In some cases, it may be difficult, if not impossible,to discern the cause of thrombocytopenia in a pregnantwoman. Nevertheless, it is important to make everyattempt to diagnose these disorders accurately becausemanagement strategies vary substantially for disordersthat appear clinically similar. For example, HELLP andTTP may share thrombocytopenia, MAHA, renal dys-function, and in some cases, neurologic symptoms, butthe optimal management of HELLP revolves arounddelivery of the fetus, while that for TTP is focused onplasma exchange.
Thrombocytopenia in pregnancy is best managed bya team of physicians that include high-risk obstetri-cians, hematologists, anesthesiologists, pediatricians,and transfusion medicine specialists. Inclusion of indi-viduals with expertise in these areas will ensure thatthe patient receives the complex care required toensure an optimal pregnancy outcome.
References
[1] McCrae KR. Thrombocytopenia in pregnancy. Hematology.Am Soc Hematol Educ Program 2010;2010:397�402.
[2] McMinn JR, George JN. Evaluation of women with clinicallysuspected thrombotic thrombocytopenic purpura-hemolyticuremic syndrome during pregnancy. J Clin Apheresis2001;16:202�9.
[3] Bockenstedt PL. Thrombocytopenia in pregnancy. HematolOncol Clin NA 2011;25(2):293�310 vii–viii.
[4] Kelton JG. Idiopathic thrombocytopenic purpura complicatingpregnancy. Blood Rev 2002;16:43�6.
[5] Crowther MA, Burrows RF, Ginsberg J, Kelton JG.Thrombocytopenia in pregnancy: diagnosis, pathogenesis andmanagement. Blood Rev 1996;10:8�18.
[6] Shehata N, Burrows RF, Kelton JG. Gestational thrombocytope-nia. Clin Obstet Gynecol 1999;42:327�34.
[7] Burrows RF, Kelton JG. Incidentally detected thrombocytope-nia in healthy mothers and their infants. N Engl J Med1988;319:142�5.
[8] Burrows RF, Andrew M. Neonatal thrombocytopenia in thehypertensive disorders of pregnancy. Obstet Gynecol1990;76:234�8.
[9] Valera MC, Parant O, Vayssiere C, Arnal JF, Payrastre B.Physiologic and pathologic changes of platelets in pregnancy.Platelets 2010;21:8587�95.
[10] Boehlen F, Hohlfeld H, Extermann P, Perneger TV, deMoerloose P. Platelet count at term pregnancy: a reappraisal ofthe threshold. Obstet Gynecol 2000;95:29�33.
[11] Sainio S, Kekomaki R, Riikonon S, Teramo K. Maternal throm-bocytopenia at term: a population-based study. Acta ObstetGynecol Scand 2000;79:744�9.
[12] Burrows RF, Kelton JG. Fetal thrombocytopenia and its rela-tion to maternal thrombocytopenia. N Engl J Med1993;329:1463�6.
[13] Burrows RF, Kelton JG. Thrombocytopenia at delivery: a pro-spective survey of 6715 deliveries. Am J Obstet Gynecol1990;162:731�4.
[14] Letsky EA, Greaves M. Guidelines on the investigation andmanagement of thrombocytopenia in pregnancy and neonatalalloimmune thrombocytopenia. Brit J Haematol 1996;95:21�36.
[15] Ruggeri M, Schiavotto C, Castaman G, Tosetto A. Gestationalthrombocytopenia: a prospective study. Haematologica 1997;82:341�2.
[16] Cines DB, Blanchette VS. Immune thrombocytopenic purpura.N Engl J Med 2002;346(13):995�1008.
[17] Provan D, Newland A. Idiopathic thrombocytopenic purpurain adults. J Ped Hematol Oncol 2003;25(Suppl.1):S34�8.
[18] Cines DB, McMillan R. Management of adult idiopathic throm-bocytopenic purpura. Ann Rev Med 2005;56:425�42.
[19] McMillan R, Wang L, Tomer A, Nichol J, Pistillo J. Suppressionof in vitro megakaryocyte production by antiplatelet autoanti-bodies from adult patients with chronic ITP. Blood 2004;103:1364�9.
[20] Semple JW, Provan D, Garvey MB, Freedman J. Recent prog-ress in understanding the pathogenesis of immune thrombocy-topenia. Curr Opin Hematol 2010;17(6):590�5.
[21] Cines DB, Bussel JB, Liebman HA, Luning Prak ET. The ITPsyndrome: pathogenic and clinical diversity. Blood 2009;113:6511�21.
[22] Gill KK, Kelton JG. Management of idiopathic thrombocytope-nic purpura in pregnancy. Sem Hematol 2000;37:275�83.
[23] Stavrou E, McCrae KR. Immune thrombocytopenia in preg-nancy. Hem Onc Clin NA 2009;23:1299�316.
[24] Karim R, Sacher RA. Thrombocytopenia in pregnancy. CurrHematol Rep 2004;3:128�33.
[25] Provan D, Stasi R, Newland AC, et al. International consensusreport on the investigation and management of primaryimmune thrombocytopenia. Blood 2010;115:168�86.
[26] Neunert C, Lim W, Crowther M, et al. The American Society ofHematology 2011 evidence-based practice guideline forimmune thrombocytopenia. Blood 2011;117(16):4190�207.
[27] British Committee for Standards in Haematology GeneralHaematology Task Force. Guidelines for the investigation andmanagement of idiopathic thrombocytopenic purpura inadults, children and in pregnancy. Brit J Haematol 2003;120:574�96.
[28] Webert KE, Mittal R, Siguoin C, Heddle NM, Kelton JG. A ret-rospective 11-year analysis of obstetric patients with idiopathicthrombocytopenic purpura. Blood 2003;102:4306�11.
[29] Samuels P, Main EK, Tomaski A, et al. Abnormalities in plate-let antiglobulin tests in preeclamptic mothers and their neo-nates. Am J Obstet Gynecol 1987;107:109�13.
[30] George JN, Woolf SH, Raskob GE, et al. Idiopathic thrombocy-topenic purpura: a practice guideline developed by explicitmethods for the American Society of Hematology. Blood1996;88:3�40.
[31] Veneri D, Franchini M, Raffaelli R, et al. Idiopathic thrombocy-topenic purpura in pregnancy: analysis of 43 consecutive casesfollowed at a single Italian institution. Ann Hematol 2006;85(8):552�4.
922 44. THROMBOCYTOPENIA IN PREGNANCY
IV. DISORDERS OF PLATELET NUMBER AND FUNCTION

[32] Moeller-Bertram T, Kuczkowski KM, Benumof JL. Uneventfulepidural labor analgesia in a parturient with immune throm-bocytopenic purpura and platelet count of 26,000/mm3 whichwas unknown preoperatively. J Clin Anesthesiol 2004;16:51�3.
[33] Beilin Y, Zahn J, Comerford M. Safe epidural analgesia inthirty parturients with platelet counts between 69,000 and98,000/μl. Anesthesia Analgesia 1997;85:385�90.
[34] Provan D, Newland A, Norfolk D, et al. Guidelines for theinvestigation and management of idiopathic thrombocytopenicpurpura in adults, children and in pregnancy. Brit J Haematol2003;120:574�96.
[35] Fujimura K, Harada Y, Fujimoto T, et al. Nationwide study ofidiopathic thrombocytopenic purpura in pregnant women andthe clinical influence on neonates. Int J Haematol2002;75:426�33.
[36] Michel M, Novoa MV, Bussel JB. Intravenous anti-D as a treat-ment for immune thrombocytopenic purpura (ITP) duringpregnancy. Brit J Haematol 2003;123:142�6.
[37] Kahn MJ, McCrae KR. Splenectomy in immune thrombocyto-penic purpura: recent controversies and long-term outcomes.Curr Hematol Rep 2004;3:317�23.
[38] Erkman J, Blythe JG. Azathioprine therapy complicated bypregnancy. Obstet Gynecol 1972;40:708�10.
[39] Stasi R, Pagano A, Stipa E, Amadori S. Rituximab chimericanti-CD20 monoclonal antibody treatment for adults withchronic idiopathic thrombocytopenic purpura. Blood2001;98:952�7.
[40] Stasi R. Rituximab in autoimmune hematologic diseases: notjust a matter of B cells. Semin Hematol 2010;47:170�9.
[41] Arnold DM, Dentali F, Crowther MA, et al. Systematicreview: efficacy and safety of rituximab for adults with idio-pathic thrombocytopenic purpura. Ann Int Med 2007;146(1):25�33.
[42] Kimby E, Sverrisdotter E, Elinder G. Safety of rituximab ther-apy during the first trimester of pregnancy: a case history. EurJ Haematol 2004;72:292�5.
[43] Gall B, Yee A, Berry B, et al. Rituximab for management ofrefractory pregnancy-associated immune thrombocytopenicpurpura. J Obstet Gynaecol Can 2010;32(12):1167�71.
[44] Burrows RF, Kelton JG. Pregnancy in patients with idiopathicthrombocytopenic purpura: assessing the risks for the infant atdelivery. Obstet Gynecol Surv 1993;48:781�8.
[45] Godelieve C, Christiaens ML, Nieuwenhuis HK, Bussel JB.Comparison of platelet counts in first and second newborns ofmothers with immune thrombocytopenic purpura. ObstetGynecol 1997;90:546�52.
[46] Koyama S, Tomimatsu T, Kanagawa T, et al. Reliable predic-tors of neonatal immune thrombocytopenia in pregnantwomen with idiopathic thrombocytopenic purpura. Am JHematol 2012;87:15�21.
[47] Payne SD, Resnik R, Moore TR, Hedriana HL, Kelly TF.Maternal characteristics and risk of severe neonatal thrombocy-topenia and intracranial hemorrhage in pregnancies compli-cated by autoimmune thrombocytopenia. Am J Obstet Gynecol1997;177:149�55.
[48] Peleg D, Hunter SK. Perinatal management of women withimmune thrombocytopenic purpura: survey of United Statesperinatologists. Am J Obstet Gynecol 1999;180:645�50.
[49] Zhang J, Meikle S, Trumble A. Severe maternal morbidity asso-ciated with hypertensive disorders in pregnancy in the UnitedStates. Hypertension Preg 2003;2003:203�12.
[50] Lain KY, Roberts JM. Contemporary concepts of the pathogen-esis and management of preeclampsia. J Am Med Assoc2002;287:3183�6.
[51] Duckitt K, Harrington D. Risk factors for preeclampsia at ante-natal booking: systemic review of controlled studies. Br Med J2005;330:595�601.
[52] Various. Working group report on high blood pressure inpregnancy (NIH Publication No. 00�3029). Bethesda, MD:National Institutes of Health, National Heart, Lung and BloodInstitute; 2000.
[53] Pridjian G, Puschett JB. Preeclampsia. Part 1: clinical andpathophysiological considerations. Obstet Gynecol Surv2002;57:598�618.
[54] American College of Obstet Gynecology. ACOG practice bulle-tin: diagnosis and management of preeclampsia in pregnancy[abstract]. Obstet Gynecol 2002;99:159�67.
[55] Mahmoudi N, Graves SW, Solomon CG. Eclampsia: a 13 yearexperience at a United States tertiary care center. J WomensHealth Gender Based Med 1999;8(4):495�500.
[56] Esplin MS, Fausett MB, Fraser A, et al. Paternal and maternalcomponents of the predisposition to preeclampsia. N Engl JMed 2001;344:867�72.
[57] Li DK, Wi S. Changing paternity and the risk of preeclampsia/eclampsia in the subsequent pregnancy. Am J Epidemiol2000;151:57�62.
[58] Skjærven R, Wilcox AJ, Lie RT. The interval between preg-nancies and the risk of preeclampsia. N Engl J Med2002;346:33�8.
[59] Robillard PY, Dekker GA, Hulsey TC. Revisiting the epidemio-logical standard of preeclampsia: primigravidity of primipater-nity. Eur J Obstet Gynecol Repro Biol 1999;84:37�41.
[60] Roberts JM, Cooper DW. Pathogenesis and genetics of pre-eclampsia. Lancet 2001;357:53�6.
[61] Dekker G, Robillard PY, Roberts C. The etiology of pre-eclampsia: the role of the father. J Reprod Immunol2011;89:2126�32.
[62] GOPEC consortium. Disentangling fetal and maternal suscepti-bility for preeclampsia: a British multicenter candidate genestudy. Am J Hum Genetics 2005;77:127�31.
[63] Garza-Veloz I, Castruita-De la Rosa C, Cortes-Flores R, et al.No association between polymorphisms/haplotypes of the vas-cular endothelial growth factor gene and preeclampsia. BMCPregnancy Childbirth 2011;11:35.
[64] Molvarec A, Jermendy A, Kovacs M, Prohaszka Z, Rigo Jr. J.Toll-like receptor 4 gene polymorphisms and preeclampsia:lack of association in a Caucasian population. HypertensionRes 2008;31:5859�64.
[65] Saftlas AF, Beydoun H, Triche E. Immunogenetic determinantsof preeclampsia and related pregnancy disorders. A systematicreview. Obstet Gynecol 2005;106:162�72.
[66] Larsen MH, Hylenius S, Andersen AM, Hviid TV. The 3’-untranslated region of the HLA-G gene in relation to pre-eclampsia: revisited. Tissue Antigens 2010;75(3):253�61.
[67] Sohlberg S, Stephansson O, Cnattingius S, Wikstrom AK.Maternal body mass index, height, and risks of preeclampsia.Am J Hypertens 2012;25(1):120�5.
[68] Wilson WA, Gharavi AE, Koike T, et al. International consen-sus statement on preliminary classification criteria for definiteantiphospholipid syndrome. Arth Rheum 1999;42:1309�11.
[69] Shehata HA, Nelson-Piercy C, Khamashta MA. Management ofpregnancy in the antiphospholipid syndrome. Rheum Dis ClinNA 2001;27:643�9.
[70] Branch W. Report of the Obstetric APS Task Force: 13th inter-national congress on antiphospholipid antibodies, 13th April2010. Lupus 2011;20(2):158�64.
[71] Dizon-Townson DS, Nelson LM, Easton K, Ward K. The factorV Leiden mutation may predispose women to severe pre-eclampsia. Am J Obstet Gynecol 1996;175:902�5.
923REFERENCES
IV. DISORDERS OF PLATELET NUMBER AND FUNCTION

[72] Grandone E, Margaglione M, Colaizzo D, et al. Factor VLeiden, C.T MTHFR polymorphism and genetic susceptibil-ity to preeclampsia. Thromb Haemost 1997;77:1052�4.
[73] Kupferminc MJ, Eldor A, Steinman M, et al. Increased fre-quency of genetic thrombophilia in women with complica-tions of pregnancy. N Engl J Med 1999;1999:340�9.
[74] Livingston JC, Barton JR, Park V, et al. Maternal and fetalinherited thrombophilias are not related to the developmentof severe preeclampsia. Am J Obstet Gynecol 2001;185:153�7.
[75] Alfirevic Z, Roberts D, Martlew V. How strong is the associa-tion between maternal thrombophilia and adverse pregnancyoutcome? A systematic review. Eur J Obstet Gynecol ReproBiol 2002;101:6�14.
[76] de Maat MP, de Groot CJ. Thrombophilia and pre-eclampsia.Semin Thromb Hemost 2011;37(2):106�10.
[77] Rodger MA. Anticoagulant prophylaxis for placenta mediatedpregnancy complications. Thromb Res 2011;127(Suppl.3):S76�80.
[78] Stanley-Christian H, Ghidini A, Sacher R, Shimerani M.Fetal genotype for specific thrombophilias is not associatedwith severe preeclampsia. J Soc Gynecol Invest 2005;12:198�201.
[79] Battinelli EM, Bauer KA. Thrombophilias in pregnancy.Hematol Oncol Clin NA 2011;25(2):323�33 viii
[80] Brosens IO. The utero-placental vessels at term—the distribu-tion and extent of physiological changes. Troph Res1988;3:61�7.
[81] Khong TY, De Wolf F, Robertson WB, Brosens I. Inadequatematernal vascular response to placentation in pregnanciescomplicated by preeclampsia and by small for gestational ageinfants. Am J Obstet Gynecol 1987;157:360�3.
[82] Zhou Y, Damsky CH, Fisher SJ. Preeclampsia is associatedwith failure of human cytotrophoblasts to mimic a vascularadhesion phenotype. J Clin Invest 1997;99:2152�64.
[83] Zhou Y, Fisher SJ, Janatpour M, et al. Human cytotropho-blasts adopt a vascular phenotype as they differentiate. Astrategy for successful endovascular invasion? J Clin Invest1997;99:2139�51.
[84] Graham CH, McCrae KR. Expression of gelatinase and plas-minogen activator activity by trophoblast cells isolated fromthe placentae of normal and preeclamptic women. Am JObstet Gynecol 1996;175:555�62.
[85] Ahn H, Park J, Gilman-Sachs A, Kwak-Kim J. Immunologiccharacteristics of preeclampsia, a comprehensive review. AmJ Reprod Immunol 2011;65(4):377�94.
[86] Soleymanlou N, Jurisica I, Nevo O, et al. Molecular evidenceof placental hypoxia in preeclampsia. J Clin Endo Metab2005;90:4299�308.
[87] Levine RJ, Maynard SE, Qian C, et al. Circulating angiogenicfactors and the risk of preeclampsia. N Engl J Med2004;350:672�83.
[88] Maynard SE, Venkatesha S, Thadhani R, Karumanchi SA.Soluble Fms-like tyrosine kinase 1 and endothelial dysfunc-tion in the pathogenesis of preeclampsia. Pediatr Res2005;57:1R�7R.
[89] Steinberg G, Khankin EV, Karumanchi SA. Angiogenic fac-tors and preeclampsia. Thromb Res 2009;123(Suppl.2):S93�9.
[90] Young BC, Levine RJ, Karumanchi SA. Pathogenesis of pre-eclampsia. Ann Rev Pathology 2010;5:173�92.
[91] Agarwal I, Karumanchi SA. Preeclampsia and the anti-angio-genic state. Preg Hypertension 2011;1:117�21.
[92] Aggarwal PK, Chandel N, Jain V, Jha V. The relationshipbetween circulating endothelin-1, soluble fms-like tyrosine
kinase-1 and soluble endoglin in preeclampsia. J HumHypertension 2012;26(4):236�41.
[93] Dekker GA, Kraayenbrink AA, Zeeman GG, van Kamp GJ.Increased plasma levels of the novel vasoconstrictor peptideendothelin in severe preeclampsia. Eur J Obstet GynecolRepro Biol 1991;40:215�20.
[94] Myatt L, Cui X. Oxidative stress in the placenta. HistochemCell Biology 2004;122:369�82.
[95] Maynard SE, Karumanchi SA. Angiogenic factors and pre-eclampsia. Semin Nephrol. 2011;31(1):33�46.
[96] Powers RW, Jeyabalan A, Clifton RG, et al. Soluble fms-Liketyrosine kinase 1 (sFlt1), endoglin and placental growth factor(PlGF) in preeclampsia among high risk pregnancies. PLoSOne 2010;5:10e13263.
[97] Salmon JE, Heuser C, Triebwasser M, et al. Mutations in com-plement regulatory proteins predispose to preeclampsia: agenetic analysis of the PROMISSE cohort. PLoS Med2011;8:3e1001013.
[98] McCrae KR. Thrombocytopenia in pregnancy: differentialdiagnosis, pathogenesis and management. Blood Rev 2003;17:7�14.
[99] McCrae KR, Cines DB. Thrombotic microangiopathy duringpregnancy. Sem Hematol 1997;34:148�58.
[100] Stepanian A, Cohen-Moatti M, Sanglier T, et al. VonWillebrand factor and ADAMTS13: a candidate couple forpreeclampsia pathophysiology. Arterioscl Thromb Vasc Biol2011;31(7):1703�9.
[101] Brenner B, Zwang E, Bronshtein M, Seligsohn U. VonWillebrand factor multimer patterns in pregnancy-inducedhypertension. Thromb Haemost 1989;62:715�7.
[102] Thorp JM, White GC, Moake JL, Bowes WA. von Willebrandfactor multimeric levels and patterns in patients with severepreeclampsia. Obstet Gynecol 1990;75:163�7.
[103] Lockwood CJ, Peters JH. Increased plasma levels of ED11 cel-lular fibronectin precede the clinical signs of preeclampsia.Am J Obstet Gynecol 1990;162:358�62.
[104] Redman CWG, Beilin LJ, Denson KWE, Bolton FG, StirratGM. Factor VIII consumption in pre-eclampsia. Lancet1977;:1249�52 ii
[105] Benedetto C, Marozio L, Tancredi A, et al. Biochemistry ofHELLP syndrome. Adv Clin Chem. 2011;53:85�104.
[106] O’Brien JM, Barton JR. Controversies with the diagnosis andmanagement of HELLP syndrome. Clin Obstet Gynecol2005;48:460�77.
[107] Barton JR, Sibai BM. Diagnosis and management of hemoly-sis, elevated liver enzymes and low platelets syndrome. ClinPerinatol 2004;31:807�33.
[108] Rath W, Faridi A, Dudenhausen JW. HELLP syndrome.J Perinatal Med 2000;28:249�60.
[109] Sibai BM. The HELLP syndrome (hemolysis, elevated liverenzymes, and low platelets): much ado about nothing? Am JObstet Gynecol 1990;162:311�6.
[110] Martin JN, Blake PG, Lowry SL, et al. Pregnancy compli-cated by preeclampsia—with the syndrome of hemolysis,elevated liver enzymes, and low platelet counts: howrapid is postpartum recovery. Obstet Gynecol 1990;76:737�41.
[111] Fakhouri F, Jablonski M, Lepercq J, et al. Factor H, membranecofactor protein, and factor I mutations in patients withhemolysis, elevated liver enzymes, and low platelet countsyndrome. Blood 2008;112(12):4542�5.
[112] Fang CJ, Fremeaux-Bacchi V, Liszewski MK, et al. Membranecofactor protein mutations in atypical hemolytic uremic syn-drome (aHUS), fatal Stx-HUS, C3 glomerulonephritis, and theHELLP syndrome. Blood 2008;111:624�32.
924 44. THROMBOCYTOPENIA IN PREGNANCY
IV. DISORDERS OF PLATELET NUMBER AND FUNCTION

[113] Mihu D, Costin N, Mihu CM, Seicean A, Ciortea R. HELLPsyndrome—a multisystemic disorder. J Gastro Liver Dis2007;16(4):419�24.
[114] Kirkpatrick CA. The HELLP syndrome. Acta Clin Belg2010;65(2):91�7.
[115] McMahon LP, Smith J. The HELLP syndrome at 16 weeksgestation: possible association with the antiphospholipid syn-drome. Aust N Z J Obstet Gynaecol 1997;37:313�4.
[116] Haram K, Trovik J, Sanset PM, Hordnes K. Severe syndromeof hemolysis, elevated liver enzymes and low platelets(HELLP) in the 18th week of pregnancy associated with theantiphospholipid-antibody syndrome. Acta Obstet GynecolScand 2003;82:679�80.
[117] Li Thi Thoung D, Tieulie N, Costedoat N, et al. The HELLPsyndrome in the antiphospholipid syndrome: retrospectivestudy of 16 cases in 15 women. Ann Rheum Dis2005;64:273�8.
[118] Appenzeller S, Souza FH, Wagner Silva de SA, Shoenfeld Y,de Carvalho JF. HELLP syndrome and its relationship withantiphospholipid syndrome and antiphospholipid antibodies.Semin Arthritis Rheum 2011;41:517�23.
[119] Magann EF, Martin JR. Twelve steps to optimal managementof HELLP syndrome. Clin Obstet Gynecol 1999;42:532�50.
[120] Pan C, Perumalswami PV. Pregnancy-related liver diseases.Clin Liver Dis 2011;15(1):199�208.
[121] Joshi D, James A, Quaglia A, Westbrook RH, HeneghanMA. Liver disease in pregnancy. Lancet 2010;375(9714):594�605.
[122] Nasr A, Nafeh H. Decreased hepatic perfusion inpatients with HELLP syndrome. J Obstet Gynaecol 2009;29(7):624�7.
[123] Sibai BM. Diagnosis, controversies and management of thesyndrome of hemolysis, elevated liver enzymes, and lowplatelet count. Obstet Gynecol 2004;103:981�91.
[124] Yucesoy G, Cakiroglu Y, Bodur H, Ozkan S, Tan T. An analy-sis of HELLP syndrome cases: does platelet count predictadverse maternal and fetal outcomes in women with HELLPsyndrome? Arch Gynecol Obstet 2011;283(5):941�5.
[125] Murphy MA, Ayazifar M. Permanent visual defects second-ary to the HELLP syndrome. J Neuro-Ophthalmol 2005;25:122�7.
[126] Rinehart BK, Terrone DA, May WL, et al. Change in plateletcount predicts eventual maternal outcome with syndrome ofhemolysis, elevated liver enzymes and low platelet count. JMaternal-Fetal Med 2001;10:28�34.
[127] Martin JN, Blake PG, Perry KG, et al. The natural history ofHELLP syndrome: patterns of disease progression and regres-sion. Am J Obstet Gynecol 1991;164:1500�13.
[128] Sibai BM, Taslimi MM, El-Nazer A, et al. Maternal-perinataloutcome associated with the syndrome of hemolysis, elevatedliver enzymes, and low platelets in severe preeclampsia-eclampsia. Am J Obstet Gynecol 1986;155:501�9.
[129] Coppage KH, Sibai BM. Treatment of hypertensive complica-tions of pregnancy. Curr Pharm Des 2005;11:749�57.
[130] Pridjian G, Puschett JB. Preeclampsia. Part 2: experimentaland genetic considerations. Obstet Gynecol Surv 2002;57:619�40.
[131] van Runnard Heimel PJ, Franx A, Schobben AF, et al.Corticosteroids, pregnancy, and HELLP syndrome: a review.Obstet Gynecol Surv 2004;60:57�70.
[132] Martin JN, Perry KG, Blake PG, et al. Better maternal out-comes are achieved with dexamethasone therapy for postpar-tum HELLP (hemolysis, elevated liver enzymes, andthrombocytopenia) syndrome. Am J Obstet Gynecol 1997;177:1011�7.
[133] Rose CH, Thigpen BD, Bofill JA, et al. Obstetric implicationsof antepartum corticosteroid therapy for HELLP syndrome.Obstet Gynecol 2004;104:1011�4.
[134] O’Brien JM, Milligan DA, Barton JR. Impact of high-dose cor-ticosteroid therapy for patients with HELLP (hemolysis, ele-vated liver enzymes, and low platelet count) syndrome. Am JObstet Gynecol 2000;183:304�9.
[135] Barilleaux PS, Martin JN, Klauser CK, Bufkin L, May WL.Postpartum intravenous dexamethasone for severely pre-eclamptic patients without hemolysis, elevated liver enzymes,low platelets (HELLP) syndrome: a randomized trial. ObstetGynecol 2005;105:843�8.
[136] Katz L, de Amorim MM, Figueiroa JN, Pinto e Silva JL.Postpartum dexamethasone for women with hemolysis, ele-vated liver enzymes, and low platelets (HELLP) syndrome: adouble-blind, placebo-controlled, randomized clinical trial.Am J Obstet Gynecol 2008;198(3):283�8.
[137] Martin Jr. JN, Files JC, Blake PG, et al. Plasma exchange forpreeclampsia. I. Postpartum use for persistently severe pre-eclampsia-eclampsia with HELLP syndrome. Am J ObstetGynecol 1990;162:126�37.
[138] Martin Jr JN, Files JC, Blake PG, et al. Postpartum plasmaexchange for atypical preeclampsia-eclampsia as HELLP(hemolysis, elevated liver enzymes and low platelets syn-drome). Am J Obstet Gynecol 1995;172:1107�12.
[139] Eser B, Guven M, Unal A, et al. The role of plasma exchangein HELLP syndrome. Clin Applied Thromb/Hemost2005;11:211�7.
[140] Lattuada A, Rossi E, Calzarossa C, Candolfi R, MannucciPM. Mild to moderate reduction of a von Willebrand factorcleaving protease (ADAMTS-13) in pregnant women withHELLP microangiopathic syndrome. Haematologica 2003;88:1029�34.
[141] Chames MC, Haddad B, Barton JR, Livingston C, Sibai BM.Subsequent pregnancy outcome in women with a history ofHELLP syndrome at , 28 weeks of gestation. Am J ObstetGynecol 2003;188:1504�8.
[142] van Pampus MG, Wolf H, Mayruu G, Treffers PE, Bleker OP.Long-term follow-up in patients with a history of (H)ELLPsyndrome. Hypertens Preg 2001;20:15�23.
[143] Sibai BM, VRamadan MK, Chari RS, Friedman SA.Pregnancies complicated by HELLP syndrome (hemolysis,elevated liver enzymes, and low platelets): subsequent preg-nancy outcome and long term prognosis. Am J ObstetGynecol 1995;172:125�9.
[144] Sullivan CA, Magann EF, Perry Jr KG, Blake PG, Martin Jr JN.The recurrence risk of the syndrome of hemolysis, elevatedliver enzymes and low platelets (HELLP) in subsequent gesta-tions. Am J Obstet Gynecol 1994;171:940�3.
[145] Habli M, Eftekhari N, Wiebracht E, et al. Long-term maternaland subsequent pregnancy outcomes 5 years after hemolysis,elevated liver enzymes, and low platelets (HELLP) syndrome.Am J Obstet Gynecol 2009;201(4):385.
[146] Askie LM, Duley L, Henderson-Smart DJ, Stewart LA.Antiplatelet agents for prevention of pre-eclampsia: a meta-analysis of individual patient data. Lancet 2007;369(9575):1791�8.
[147] Gris JC, Chauleur C, Molinari N, et al. Addition of enoxaparinto aspirin for the secondary prevention of placental vascularcomplications in women with severe pre-eclampsia. The pilotrandomised controlled NOH-PE trial. Thromb Haemost2011;106:5.
[148] Roberts JM, Pearson G, Cutler J, Lindheimer MD. Summaryof the NHLBI working group on research on hypertensionduring pregnancy. Hypertension 2003;41:437�45.
925REFERENCES
IV. DISORDERS OF PLATELET NUMBER AND FUNCTION

[149] Xu H, Perez-Cuevas R, Xiong X, et al. An international trial ofantioxidants in the prevention of preeclampsia (INTAPP). AmJ Obstet Gynecol 2010;202(3):239.e1�239.e10.
[150] Steegers EA, von DP, Duvekot JJ, Pijnenborg R. Pre-eclampsia.Lancet 2010;376(9741):631�44.
[151] Astrup A. Calcium reduces risk of pre-eclampsia. Lancet2010;376(9757):1986�7.
[152] Hofmeyr GJ, Lawrie TA, Atallah AN, Duley L. Calcium sup-plementation during pregnancy for preventing hypertensivedisorders and related problems. Cochrane Database Syst Rev2010;(8):CD001059.
[153] Miller DP, Kaye JA, Ziyadeh N, et al. Incidence of thromboticthrombocytopenic purpura/hemolytic uremic syndrome.Epidemiology 2004;15:208�15.
[154] Torok TJ, Holman RC, Chorba TL. Increasing mortality fromthrombotic thrombocytopenic purpura in the United States—analysis of national mortality data, 1968�1961. Am J Hematol1995;50(2):84�90.
[155] Vesely SK, George JN, Lammle B, et al. ADAMTS13 activityin thrombotic thrombocytopenic purpura-hemolytic uremicsyndrome: relation to presenting features and clinical out-comes in a prospective cohort of 142 patients. Blood2003;102:60�8.
[156] Nicol KK, Shelton BJ, Knovich MS, Owen J. Overweight indi-viduals are at increased risk for thrombotic thrombocytopenicpurpura. Am J Hematol 2003;74:170�4.
[157] Terrell DR, Motto DG, Kremer Hovinga JA, et al. Bloodgroup O and black race are independent risk factors forthrombotic thrombocytopenic purpura associated withsevere ADAMTS13 deficiency. Transfusion 2011;51(10):2237�43.
[158] Ridolfi RL, Bell WR. Thrombotic thrombocytopenia purpura:report of 25 cases and a review of the literature. Medicine1981;60:413�28.
[159] Nabhan C, Kwaan HC. Current concepts in the diagnosis andmanagement of thrombotic thrombocytopenic purpura.Hematol Oncol Clin NA 2003;17:177�99.
[160] Thompson CE, Damon LE, Ries CA, Linker CA. Thromboticmicroangiopathies in the 1980s: clinical features, response totreatment, and the impact of the human immunodeficiencyvirus epidemic. Blood 1992;80:1890�5.
[161] Keiser SD, Boyd KW, Rehberg JF, et al. A high LDH to ASTratio helps to differentiate pregnancy-associated thromboticthrombocytopenic purpura (TTP) from HELLP syndrome.J Maternal Fetal Neonatal Med 2011.
[162] Sadler JE. von Willebrand factor, ADAMTS13, and thromboticthrombocytopenic purpura. Blood 2008;112:11�8.
[163] Zheng XL, Sadler JE. Pathogenesis of thrombotic microangio-pathies. Annu Rev Pathol Mech Dis 2008;3:249�77.
[164] Berns JS, Kaplan BS, Mackow RC, Hefter LG. Inherited hemo-lytic uremic syndrome in adults. Am J Kidney Dis 1992;:331�4 XIX
[165] George JN. Evaluation and management of patients withthrombotic thrombocytopenic purpura. J Intensive Care Med2007;22:82�91.
[166] George JN. How I treat patients with thrombotic thrombocy-topenic purpura: 2010. Blood 2010;116(20):4060�9.
[167] McCrae KR, Sadler JE, Cines DB. Thrombotic thrombocy-topenic purpura and the hemolytic uremic syndrome.In: Hoffman R, Benz Jr E, Shattil SJ, et al., editors.Hematology: Basic Principles and Practice. Philadelphia:Churchill Livingstone; 2009. p. 2099�112.
[168] Proulx F, Siefdman EG, Karpman D. Pathogenesis of shigatoxin-associated hemolytic uremic syndrome. Ped Res2001;50:163�71.
[169] Kavanagh D, Goodship TH. Atypical hemolytic uremic syn-drome, genetic basis, and clinical manifestations. Hematology.Am Soc Hematol Educ Program 2011;2011:15�20.
[170] Boyer O, Niaudet P. Hemolytic uremic syndrome: new devel-opments in pathogenesis and treatment. Int J Nephrol2011;2011:908407.
[171] Kavanagh D, Goodship T. Haemolytic uraemic syndrome.Nephron Clin Practice 2011;118(1):c37�42.
[172] George JN. How I treat patients with thrombotic thrombocy-topenic purpura-hemolytic uremic syndrome. Blood2000;96:1223�9.
[173] Esplin MS, Branch DW. Diagnosis and management of throm-botic microangiopathies during pregnancy. Clin ObstetGynecol 1999;42:360�8.
[174] Castella M, Pujol M, Massague I, et al. Thrombotic thrombo-cytopenic purpura and pregnancy: a review of ten cases. VoxSang 2004;87:287�90.
[175] Furlan M, Robles R, Galbusera M, et al. von Willebrand fac-tor-cleaving protease in thrombotic thrombocytopenic pur-pura and the hemolytic-uremic syndrome. N Engl J Med1998;339:1578�84.
[176] Tsai H-M, Lian ECY. Antibodies to von Willebrand factor-cleaving protease in acute thrombotic thrombocytopenic pur-pura. N Engl J Med 1998;339:1585�94.
[177] George JN. The thrombotic thrombocytopenic purpura andhemolytic uremic syndromes: evaluation, management,and long-term outcomes experience of the OklahomaTTP-HUS Registry, 1989�2007. Kidney Int Suppl 2009;112:S52�4.
[178] Levy GG, Nichols WC, Lian EC, et al. Mutations in a memberof the ADAMTS gene family cause thrombotic thrombocyto-penic purpura. Nature 2001;413:488�94.
[179] Mannucci PM, Vanoli M, Forza I, Canciani MT, Scorz R. vonWillebrand factor cleaving protease (ADAMTS-13) in 123patients with connective tissue diseases (systemic lupuserythematosus and systemic sclerosis). Haematologica2003;88:914�8.
[180] Mannucci PM, Canciani T, Forza I, et al. Changes in healthand disease of the metalloprotease that cleaves vonWillebrand factor. Blood 2001;98:2730�5.
[181] Sanchez-Luceros A, Farias CE, Amaral MM, et al. vonWillebrand factor-cleaving protease (ADAMTS13) activity innormal non-pregnant women, pregnant and post-deliverywomen. Thromb Haemost 2004;92:1320�6.
[182] Moake JL. Thrombotic microangiopathies. N Engl J Med2002;347:589�600.
[183] Tsai H-M. Current concepts in thrombotic thrombocytopenicpurpura. Ann Rev Med 2006;57:419�36.
[184] George JN. The association of pregnancy with thromboticthrombocytopenic purpura-hemolytic uremic syndrome. CurrOpin Hematol 2003;10:339�44.
[185] Reiter RA, Varadi K, Turecek PL, Jilma B, Knobl P. Changesin ADAMTS13 (von-Willebrand-factor-cleaving protease)activity after induced release of von Willebrand factor duringacute systemic inflammation. Thromb Haemost 2005;93:554�8.
[186] Weiner CP. Thrombotic microangiopathy in pregnancy andthe postpartum period. Sem Hematol 1987;24:119�29.
[187] Martin Jr. JN, Bailey AP, Rehberg JF, et al. Thrombotic throm-bocytopenic purpura in 166 pregnancies: 1955�2006. Am JObstet Gynecol 2008;199(2):98�104.
[188] Ducloy-Bouthors AS, Caron C, Subtil D, et al. Thromboticthrombocytopenic purpura: medical and biological monitor-ing of six pregnancies. Eur J Obstet Gynecol Repro Biol2003;111:146�52.
926 44. THROMBOCYTOPENIA IN PREGNANCY
IV. DISORDERS OF PLATELET NUMBER AND FUNCTION

[189] Clark K. TTP and me. Pract Midwife 2004;7:13�7.[190] Sherer DM, Sanmugarajah J, Dalloul M, et al. Thrombotic
thrombocytopenic purpura in a patient with acquired immu-nodeficiency syndrome at 28 weeks gestation. Am J Perinatol2005;22:223�5.
[191] Ganesan C, Maynard SE. Acute kidney injury in pregnancy:the thrombotic microangiopathies. J Nephrol 2011;24(5):554�63.
[192] Sibai BM. Imitators of severe pre-eclampsia. Semin Perinatol2009;33(3):196�205.
[193] Allford SL, Hunt BJ, Rose P, Machin SJ. Haemostasis andThrombosis Task Force of the British Committee forStandards in Haematology. Guidelines on the diagnosis andmanagement of the thrombotic microangiopathic haemolyticanaemias. Brit J Haematol 2003;120:556�73.
[194] Rock GA, Shumak KH, Buskard NA, et al. Comparison ofplasma exchange with plasma infusion in the treatment ofthrombotic thrombocytopenic purpura. N Engl J Med1991;325:393�7.
[195] Zhan H, Streiff MB, King KE, Segal JB. Thrombotic thrombo-cytopenic purpura at the Johns Hopkins Hospital from 1992to 2008: clinical outcomes and risk factors for relapse.Transfusion 2010;50(4):868�74.
[196] Ruggenenti P, Remuzzi G. The pathophysiology and manage-ment of thrombotic thrombocytopenic purpura. Eur JHaematol 1996;56:191�207.
[197] Kwaan HC, Soff GA. Management of thrombotic thrombocy-topenic purpura and hemolytic uremic syndrome. SemHematol 1997;34:159�66.
[198] Fang CJ, Richards A, Liszewski MK, Kavanagh D, AtkinsonJP. Advances in understanding of pathogenesis of aHUS andHELLP. Brit J Haematol 2008;143:336�48.
[199] Delvaeye M, Noris M, De VA, et al. Thrombomodulin muta-tions in atypical hemolytic-uremic syndrome. N Engl J Med2009;361:345�57.
[200] Loirat C, Fremeaux-Bacchi V. Atypical hemolytic uremic syn-drome. Orphanet J Rare Dis 2011;6:60.
[201] Fakhouri F, Roumenina L, Provot F, et al. Pregnancy-associ-ated hemolytic uremic syndrome revisited in the era ofcomplement gene mutations. J Am Soc Nephrol 2010;21:859�67.
[202] Remuzzi G. The hemolytic uremic syndrome. Kidney Int1995;47:2�19.
[203] Kose O, Zimmerhackl LB, Jungraithmayr T, Mache C,Nurnberger J. New treatment options for atypical hemolyticuremic syndrome with the complement inhibitor eculizumab.Sem Thromb Hemost 2010;36(6):669�72.
[204] Vesely SK, Li X, McMinn JR, Terrell DR, George JN.Pregnancy outcomes after recovery from thrombotic thrombo-cytopenic purpura-hemolytic uremic syndrome. Transfusion2004;44:1149�58.
[205] Kerr H, Richards A. Complement-mediated injury andprotection of endothelium: lessons from atypicalhaemolytic uraemic syndrome. Immunobiology 2012;217(2):195�203.
[206] Fesenmeir MF, Coppage KH, Lambers DS, Barton JR, SibaiBM. Acute fatty liver of pregnancy in 3 tertiary care centers.Am J Obstet Gynecol 2005;192:1416�9.
[207] Burroughs AK, Seong NH, Dojcinov DM, Scheur PH,Sherlock SV. Idiopathic acute fatty liver of pregnancy in 12patients. Quart J Med 1982;51:481�97.
[208] Usta IM, Barton JR, Amon EA, Gonzalez A, Sibai BM. Acutefatty liver of pregnancy: an experience in the diagnosis andmanagement of fourteen cases. Am J Obstet Gynecol1994;171:1342�7.
[209] Vigil-De Gracia P. Acute fatty liver and HELLP syndrome:two distinct pregnancy disorders. Int J Gynaecol Obstet2001;73:215�21.
[210] Bacq Y. Acute fatty liver of pregnancy. Sem Perinatol1998;22:134�40.
[211] Ibdah JA, Yang Z, Bennett MJ. Liver disease in pregnancyand fetal fatty acid oxidation defects. Mol Genetics Metab2000;71:182�7.
[212] Ibdah JA, Bennett MJ, Rinaldo P, et al. A fetal fatty-acid oxi-dation disorder as a cause of liver disease in pregnantwomen. N Engl J Med 1999;340:1723�31.
[213] Gutierrez JC, Balmaseda E, Gil E, et al. Acute fatty liver ofpregnancy and neonatal long-chain 3-hydroxyacyl-coenzymeA dehydrogenase (LCHAD) deficiency. Eur J Pediatr 2009;168(1):103�6.
[214] Holub M, Bodamer OA, Item C, et al. Lack of correlationbetween fatty acid oxidation disorders and haemolysis, ele-vated liver enzymes, low platelets (HELLP) syndrome? ActaPaeds Scand 2005;94:48�52.
[215] Knox TA, Olans LB. Liver disease in pregnancy. N Engl JMed 1996;335:569�76.
[216] Tan AC, van Krieken JH, Peters WH, Steegers EA. Acute fattyliver in pregnancy. Netherlands J Med 2002;60:370�3.
[217] Dekker RR, Schutte JM, Stekelenburg J, Zwart JJ, van RJ.Maternal mortality and severe maternal morbidity from acutefatty liver of pregnancy in the Netherlands. Eur J ObstetGynecol Reprod Biol 2011;157(1):27�31.
[218] Martin Jr. JN, Briery CM, Rose CH, et al. Postpartum plasmaexchange as adjunctive therapy for severe acute fatty liver ofpregnancy. J Clin Apheresis 2008;23(4):138�43.
[219] Hepner DL, Tsen LC. Severe thrombocytopenia, type 2B vonWillebrand disease and pregnancy. Anesthesiology2004;101:1465�7.
[220] Federici AB, Mannucci PM, Castaman G, et al. Clinical andmolecular predictors of thrombocytopenia and risk of bleed-ing in patients with von Willebrand disease type 2B: a cohortstudy of 67 patients. Blood 2009;113(3):526�34.
[221] Casonato A, Sartori MT, Bertomoro A, et al. Pregnancy-induced worsening of thrombocytopenia in a patient withtype IIB von Willebrand’s disease. Blood Coag Fibrinolysis1991;2:33�40.
[222] Li Z, Nardi MA, Karpatkin S. Role of molecular mimicry toHIV-1 peptides in HIV-1 related immunologic thrombocyto-penia. Blood 2005;106:572�6.
[223] Cines DB, Liebman H, Stasi R. Pathobiology ofsecondary immune thrombocytopenia. Semin Hematol 2009;46:S2�14.
[224] Pan R, Wang J, Nardi MA, Li Z. The inhibition effect of anti-GPIIIa49�66 antibody on megakaryocyte differentiation.Thromb Haemost 2011;106(3):484�90.
[225] Chelucci C, Federico M, Guerriero R, et al. Productive humanimmunodeficiency virus-1 infection of purified megakaryo-cytic progenitors/precursors and maturing megakaryocytes.Blood 1999;91:1225�34.
[226] Zhang W, Nardi MA, Borkowsky W, Li Z, Karpatkin S. Roleof molecular mimicry of hepatitis C virus protein with plateletGPIIIa in hepatitis C-related immunologic thrombocytopenia.Blood 2009;113(17):4086�93.
[227] Diz-Kucukkaya R, Hacehanefioglu A, Yenerel M, et al.Antiphospholipid antibodies and antiphospholipid syn-drome in patients presenting with immune thrombocytope-nic purpura: a prospective cohort study. Blood 2001;98:1760�4.
[228] Nagayama K, Izumi N, Miyasaka Y, et al. Hemolysis, elevatedliver enzymes, and low platelets syndrome associated with
927REFERENCES
IV. DISORDERS OF PLATELET NUMBER AND FUNCTION

primary anti-phospholipid antibody syndrome. Int Med1997;36:661�7.
[229] Chakravarty EF, Colon I, Langen ES, et al. Factors that predictprematurity and preeclampsia in pregnancies that are compli-cated by systemic lupus erythematosus. Am J Obstet Gynecol2005;192:1897�904.
[230] Aster RH. Drug-induced immune cytopenias. Toxicology2005;209:149�53.
[231] George JN, Aster RH. Drug-induced thrombocytopenia: path-ogenesis, evaluation, and management. Hematology. Am SocHematol Educ Program 2009;:153�8.
[232] Aster RH, Curtis BR, McFarland JG, Bougie DW. Drug-induced immune thrombocytopenia: pathogenesis, diag-nosis, and management. J Thromb Haemost 2009;7(6):911�8.
[233] Cox K, Price V, Kahr WH. Inherited platelet disorders: a clini-cal approach to diagnosis and management. Expert RevHematol 2011;4(4):455�72.
[234] Balduini CL, Pecci A, Savoia A. Recent advances inthe understanding and management of MYH9-related in-herited thrombocytopenias. Brit J Haematol 2011;154(2):161�74.
928 44. THROMBOCYTOPENIA IN PREGNANCY
IV. DISORDERS OF PLATELET NUMBER AND FUNCTION