Embed Size (px)
Citation preview

Pneumocystis Carinii Pneumonia
A Clinicopathologic Study of Twenty Patients
with Neoplastic Diseases
PETER ROSEN, M.D.
DONALD ARMSTRONG, M.D.
CORAZON RAMOS, M.D.
New York, New York
From the Department of Pathology, the Infec- tious Disease Service of the Department of Medicine, and the Department of Pediatrics, Memorial-Sloan Kettering Cancer Center, New York, New York. This study was pre- sented in part at, the meeting of the American Society of Clinical Pathologists, Boston, Mas- sachusetts, October . 28, 1971. Requests for reprints should be addressed to Dr. Peter Rosen, Department of Pathology, Memorial Hospital, 444 East 68th Street, New York, New York 10021. Manuscript received No- vember 11, 1971. revised November 22,197l.
A study of twenty patients proved to have Pneumocystis carinii pneumonia revealed that the clinical presentation of Pneumo- cystis infection may vary from fulminant to inapparent pneumo- nia and may be masked by preexistent pulmonary disease. Rapidly progressive Pneumocystis infections are characterized at an early stage by symptoms indicating more severe pulmo- nary compromise than suggested by either the physical exam- ination or chest roentgenogram. In these cases, particularly, an aggressive approach to make a specific diagnosis should be considered. Even when pentamidine therapy is initiated early in the course of proved infections, the survival of the patient may be jeopardized by other concomitant infectious or neoplastic pulmonary lesions. It is therefore important that thorough histo- pathologic and microbiologic studies be performed in order to identify the presence of any other potentially treatable pulmo- nary disease which may complicate Pneumocystis pneumonia.
Infections are an ever increasing problem in the care of pa- tients with neoplastic disease as more aggressive and pro; longed treatment regimens are used. Since specific therapy is not available for all opportunistic pathogens, it is important to identify those microorganisms which can be controlled by avaii- able drugs.
interest in the specific diagnosis of Pneumocystis carinii pneumonia has been heightened in recent years by the thera- peutic success with pentamidine isothionate [l-3]. Unfortu- nately, no reliable methods for isolation of Pneumocystis carinii or for serologic confirmation of infection are presently available [4]. Diagnosis rests on the clinical impression and microscopic demonstration of characteristic cysts either in pulmonary se- cretions [5] or in lung biopsy specimens [2]. Since lung biopsy is especially hazardous in patients with leukemia or lymphoma, caution must be exercised in the selection of patients for such operation.
We report our observations in a series of patients with neo- plastic disease who were proved to have Pneumocystis pneu- monia by pathologic examination. Analysis of this group of pa; tients suggested that they might be subdivided on the basis of morphologic alterations in the lungs for more detailed ciini- copathologic correlation.
428 October 1972 The American Journal of Medicine Volume 53

PNEUMOCYSTIS CARlNIl PNEUMONIA-ROSEN ET AL.
MATERIALS AND METHODS
Twenty patients were identified as having Pneumocystis pneumonia by a review of the laboratory and autopsy re- portsof Memorial Hospital from 1963 through June 1971. Pathologic and clinical material in each case was re- viewed, and the diagnosis was confirmed. When rele- vant information was unavailable, the number of items recorded under “Observations” was less than the total number of patients. Chest roentgenograms were reex- amined and correlated with histopathologic findings.
GENERAL OBSERVATIONS
Patients. Twelve of the patients were male and
eight female. All were white. The distribution of age at the time of death or diagnosis of infection ranged from four to fifty-six years. Two-thirds of the patients were thirty or more years of age. Epidemiology. More than half (twelve) of the cases occurred in the two and a half years after 1968. The others (eight) were distributed evenly over the six preceding years..Over the years, five patients either died or were found to have Pneu- mocystis pneumonia in the month of July. No more than three cases occurred in any other month. Six patients were urban residents, and twelve lived in suburban locations. Primary Disease and Therapy. Sixteen patients had either malignant lymphoma or leukemia: six had Hodgkin’s disease, four reticulum cell sar- coma, two lymphosarcoma, two chronic granulo- cytic leukemia and two acute lymphoblastic leu- kemia. Two women had breast cancer. One pa- tient had neuroblastoma, and one had multiple myeloma (Table I). In nineteen of twenty patients, the primary disease was widespread or in relapse at the time the pneumonia apparently developed. One patient with leukemia had a remission shortly after the diagnosis of Pneumocystis pneumonia was made and treatment begun.
Eighteen patients had been receiving adrenal corticosteroid therapy for at least one month, and fourteen of these were receiving other chemo- therapeutic agents concurrently. Three of four pa- tients not receiving adrenal steroids terminally had been under steroid treatment to within one or two months before death. The duration of corticoste- roid treatment ranged from one to over twenty- four months although the majority of patients were treated for less than twelve months. Cyclophos- phamide was combined with adrenal steroid ther- apy in four patients and vincristine in three. There
were instances of therapy with many other
chemotherapeutic agents in various combina- tions.
LABORATORY STUDIES
Peripheral Blood (Table I). Leukopenia (less than 5,000 leukocytes/cu mm) and severe thrombocy- topenia (less than 75,000 platelets/cu mm) were common coexistent problems among these pa- tients and represented the depressant effects on bone marrow function of the primary illness and therapy. Fifteen patients had prolonged (longer than one month) leukopenia before pneumonia developed. Of five patients who were not leuko- penic, two had leukemia in relapse. Serum Proteins (Table I). Eight of nineteen pa- tients whose serum proteins were studied had se- vere hypoalbuminemia (less than 3.0 gm/lOO ml, normal range 3.75 to 5.27 gm/lOO ml). Electro- phoresis was performed in six patients, and five had hypogammaglobulinemia (normal range 0.63 to 1.77 gm/lOO ml). Serology (Table I I). Complement-fixing (CF) antibody to cytomegalovirus (CMV) was mea- sured in six patients. Two had proved CMV infec- tion at necropsy but their titers were 1:8 and less than 1:8. Three patients with titers of less than 1:8 and one with a titer of 1: 16 had no demon- strable CMV infection at autopsy.
Cold agglutinins were determined in five pa- tients. In two patients studied four and fourteen months prior to death, no titers were present. The titer of one patient studied two months prior to death and terminally, decreased from 1:20 to zero. In the fourth and fifth patients studied within two weeks of death titers were nega- tive.
CLINICOPATHOLOGIC CORRELATIONS
The patients were subdivided into three groups (Table I) on the basis of histopathologic findings in the lungs. Group A consisted of those in whom the major lesion in the lungs was Pneumocystis pneumonia. Patients in group B had Pneumocystis pneumonia complicated by at least one other im- portant pathologic process. For those in group C, Pneumocystis was not a prominent aspect of the pulmonary pathology.
There were few differences with regard to basic clinical data among the three groups. The three children under ten years of age were in group A. Excluding them, the average age in each group was almost identical. There were only minor vari- ations in the distribution of the. month of death, in urban versus suburban residence, frequency of leukopenia or hypoalbuminemia and in therapy. With regard to primary disease, group C consisted
October 1972 The American Journal of Medicine Volume 53 429

TAB
LE
I S
um
mar
y o
f O
bse
rvat
ion
s in
Pat
ien
ts
Gro
up
ed
by
Ext
ent
of
Pn
eum
ocy
stis
P
neu
mo
nia
Leu
kocy
te
Th
erap
y at
Dia
gn
osi
s 01
Ter
min
ally
A
ge (y
r)
Co
un
t*
Ser
um
t S
ites
of
all
Pat
ien
t an
d S
ex
Pri
mar
y D
isea
se
(per
cu
mm
) Pr
otei
n R
adio
ther
apy
Ster
oids
C
hem
othe
rapy
O
ther
Lu
ng
Pat
ho
log
y at
Aut
opsy
and
Oth
er I
nfec
tions
Gro
up
A
Sku
ll N
on
e C
yclo
ph
osp
ham
ide
E.S
. R
F
J.D
u.
5,M
J.M
. 8,
M
J.P
. 4,
M
J.N
.
A.M
. 52
,M
J.P
r.
4&F
R.D
. 17
,M
Ho
dg
kin
’s
dis
ease
8,
100
M.S
. 39
,F
Ho
dg
kin
’s
dis
ease
2,
500
D.S
. 35
.F
Lym
ph
osa
rco
ma
Neu
rob
last
om
a
Lym
ph
osa
rco
ma
Acu
te
lym
ph
ob
last
ic
leu
kem
ia
Ch
ron
ic
gra
nu
locy
tic
leu
kem
ia
Ret
icu
lum
ce
ll sa
rco
ma
12,3
00
800
4,80
0
1.20
0
3.5
2.3
(0.7
3)
3.5
- 2.0
+
- + +
+
+ +
+ +
Rar
e p
ulm
on
ary
CM
V,
Can
did
a o
f m
ou
th
1 ?
Fo
cal
nec
roti
zin
g
pn
eum
on
ia,
up
per
lo
be
of
rig
ht
lun
g,
Can
did
a o
f m
ou
th
Ora
l C
and
ida,
n
o a
uto
psy
Sp
ine,
sk
ull
Th
iog
uan
ine,
cy
tosi
ne
arab
ino
sid
e
Th
iog
uan
ine,
vi
ncr
isti
ne,
L
-asp
arag
inas
e
Dau
no
myc
in
Cyc
lop
ho
sph
amid
e
4.0
= (0
.58)
Med
iast
inu
m,
bra
in
3.0
- 2.0
No
ne
12,0
00
2,60
0
2.6
- 1.6
(0.4
)
2.6
= (0
.6)
No
ne
Rar
e p
ulm
on
ary
CM
V,
term
inal
se
pti
cem
ia
Cit
rob
acte
r sp
.
Rar
e p
ulm
on
ary
CM
V,
cuta
neo
us
and
tr
ach
eal
her
pes
si
mp
lex,
o
ral
Can
did
a
Ble
om
ycin
P
leu
ral
fib
rosi
s
Su
pra
clav
icu
lar,
m
edia
stin
um
, ab
do
men
Ab
do
men
, m
edia
stin
um
. sk
ull
Gro
up
B
Sp
ine,
n
eck,
m
edia
stin
um
Ret
icu
lum
ce
ll sa
rco
ma
1,70
0 1.
9
2.8
4.1
1.1
Vin
bla
stin
e,
chlo
ram
bu
cil,
cycl
op
ho
sph
amid
e
Met
hyl
hyd
razi
ne
No
du
lar
pu
lmo
nar
y H
od
gki
n’s
d
isea
se
and
fi
bro
sis,
o
ral
her
pes
si
mp
lex
2.6
2.8
Su
pra
clav
icu
lar,
m
edia
stin
um
, ab
do
min
al
Med
iast
inu
m,
abd
om
en
Pu
lmo
nar
y H
od
gki
n’s
d
isea
se
and
fi
bro
sis,
ex
ten
sive
Ret
icu
lum
ce
ll sa
rco
ma
4,40
0 3.
7
2.5
Vin
cris
tin
e,
amet
ho
pte
rin
R
etic
ulu
m
cell
sarc
om
a p
leu
ra;
wid
esp
read
p
ulm
on
ary
hem
orr
hag
e an
d
hya
line
mem
bra
nes

W.S
. 39
,M
T.C
. 17
,F
F.B
. 53
,M
H.B
. 55
,M
E.H
. 56
,F
E.C
. 47
.M
E.J
. 44
,F
Z.W
. 38
,M
R.C
. 18
,M
M.C
. 37
,F
Ret
icu
lum
ce
lLsa
rco
ma
Acu
te
lym
ph
ob
last
ic
leu
kem
ia
Ch
ron
ic
gra
nu
locy
tic
leu
kem
ia
Mu
ltip
le
mye
lom
a
Mam
mar
y ca
rcin
om
a
Ho
dg
kin
’s
dis
ease
Mam
mar
y ca
rcin
om
a
Ho
dg
kin
’s
dis
ease
Ho
dg
kin
’s
dis
ease
Ho
dg
kin
’s
dis
ease
1,70
0
300
18,0
00
7,00
0
3,30
0
3,00
0
1,60
0
2,60
0
6,00
0
2,60
0
5.1
- 1.6
2.8
iii 2.7
-iZ
3.4
3.0 4.1
3.1
3.4
2.1
1.8
1.4
(0.1
5)
3.4
2.1
2.6
- 2.0
(0.3
8)
Fla
nk,
m
edia
stin
um
+
No
ne
No
ne
- +
Lu
mb
ar
spin
e +
Cyc
lop
ho
sph
amid
e
Sp
ine,
ri
bs
(rig
ht)
-
Bac
k,
retr
op
erit
on
eum
, +
abd
om
en,
nec
k,
axill
a
Gro
up
C
Sp
ine
+
Ch
est,
liv
er,
spin
e + +
Ch
est,
sp
ine,
ax
illas
+
Cyt
osi
ne
arab
ino
sid
e
L-A
spar
agin
ase
6.M
erca
pto
pu
rin
e
5-F
luo
rou
raci
l
Ble
om
ycin
-
Vin
cris
tin
e
Vin
cris
tin
e
No
du
lar
pu
lmo
nar
y re
ticu
lum
ce
ll sa
rco
ma,
o
ral
Can
did
a,
sep
sis
Sal
. ty
ph
imu
riu
m
Pse
ud
om
on
as
sep
tice
mia
an
d
pn
eum
on
ia;
pu
lmo
nar
y C
MV
CM
V
of
lun
gs
wit
h
foca
l n
ecro
sis,
se
vere
p
ulm
on
ary
fib
rosi
s,
Sta
ph
. au
reu
s se
psi
s
Fo
cal
her
pet
ic
pn
eum
on
ia,
seve
re
hya
line
mem
bra
nes
, o
ral
her
pes
si
mp
lex
Lym
ph
ang
itic
ca
rcin
om
ato
sis
of
lun
gs
Hya
line
mem
bra
nes
, in
ters
titi
al
fib
rosi
s,
pu
lmo
nar
y h
emo
rrh
age,
H
od
gki
n’s
d
isea
se
Pu
lmo
nar
y C
MV
, ly
mp
han
git
ic
carc
ino
mat
osi
s an
d
hem
orr
hag
ic
infa
rcts
Pu
lmo
nar
y C
MV
, ca
nd
idia
sis,
fi
bro
sis
and
H
od
gki
n’s
d
isea
se,
her
pes
sk
in
Pu
lmo
nar
y H
od
gki
n’s
d
isea
se,
fib
rosi
s an
d
nec
roti
zin
g
pn
eum
on
ia,
ora
l C
and
ida
s E
Dis
sem
inat
ed
her
pes
zo
ster
, o
ral
5 C
and
ida,
p
ulm
on
ary
CM
V
and
2
fib
rosi
s,
nec
roti
zin
g
Pse
ud
om
on
as
v)
i p
neu
mo
nia
f/
Y
0
NO
TE
: G
rou
p A
: P
red
om
inan
tly
Pn
eum
ocy
stis
p
neu
mo
nia
. G
rou
p
6: P
neu
mo
cyst
is
pn
eum
on
ia
maj
or
elem
ent
in p
ulm
on
ary
pat
ho
log
y,
bu
t co
mp
licat
ed
by
oth
er
lesi
on
s.
Z
Gro
up
C:
Pn
eum
ocy
stis
p
neu
mo
nia
an
in
con
spic
uo
us
asp
ect
of
lun
g p
ath
olo
gy.
C
MV
=
Cyt
om
egal
ovi
rus.
z =
* N
orm
al:
5,00
0 to
10,
600
wh
ite
blo
od
cel
ls/c
u
mm
. t
Alb
um
in:g
lob
ulin
(g
amm
a).
No
rmal
:A
lbu
min
3.
75 t
o 5
.27
gm
/lOO
m
l. G
lob
ulin
s:
gam
ma
glo
bu
lin
0.63
to
1.7
7 gm
/lO
O m
l, to
tal
glo
bu
lins
1.55
to
4.0
1 gm
/lO
O
ml.
P
!Z
h
PNEUMOCYSTIS CARlNIl PNEUMONIA-ROSEN ET AL
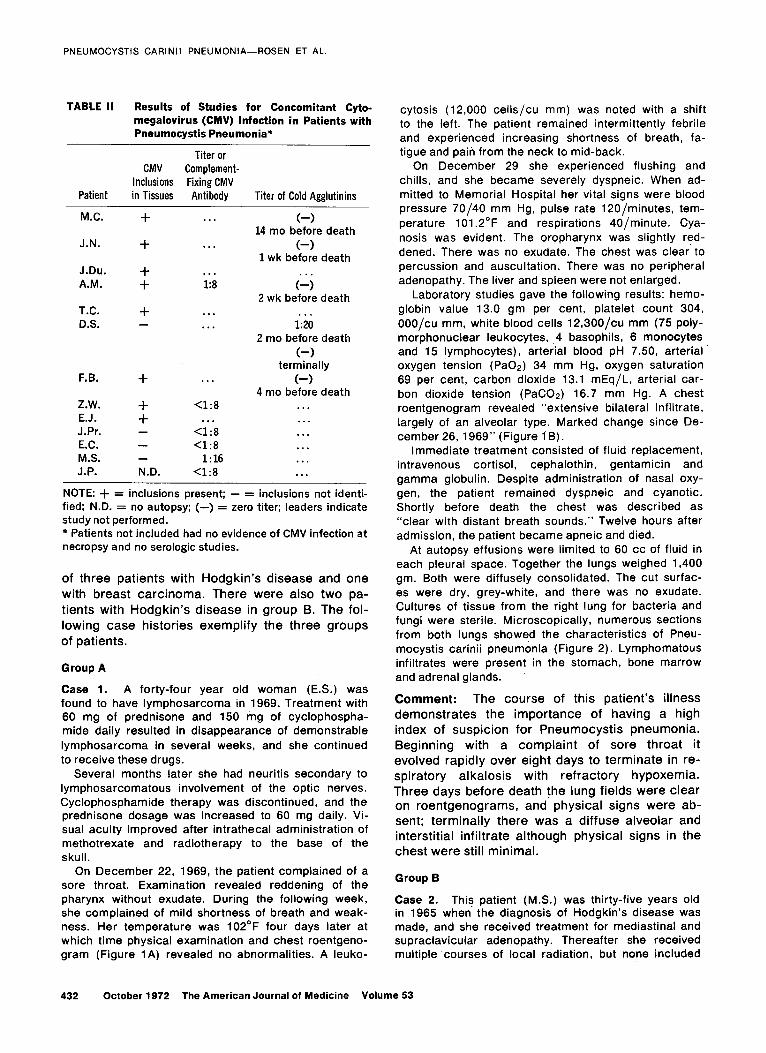
TABLE II Results of Studies for Concomitant Cyto- megalovirus (CMV) Infection in Patients with Pneumocystis Pneumonia*
Patient
Titer or CMV Complement-
Inclusions Fixing CMV
in Tissues Antibody Titer of Cold Agglutinins
M.C.
J.N.
J.Du.
A.M.
T.C.
D.S.
F.B.
Z.W. E.J.
J.Pr.
E.C.
M.S.
J.P.
+
+
+ +
+
+
+ +
N.D.
__
. . . C-1 14 mo before death
. . . (-) 1 wk before death
. . .
1:8 (Lj
2 wk before death . . .
. . . l-:20
2 mo before death
(-) terminally
. . .
<1:8 . . .
<1:8
X1:8 1:16
cl:8
(-) 4 mo before death
. . .
. . . . . . . . . . . . . . .
NOTE: + = inclusions present; - = inclusions not identi-
fied: N.D. = no autopsy: (-) = zero titer; leaders indicate
study not performed. * Patients not included had no evidence of CMV infection at
necropsy and no serologic studies.
of three patients with Hodgkin’s disease and one with breast carcinoma. There were also two pa- tients with Hodgkin’s disease in group B. The fol- lowing case histories exemplify the three groups of patients.
Group A
Case 1. A forty-four year old woman (E.S.) was found to have lymphosarcoma in 1969. Treatment with 60 mg of prednisone and 150 mg of cyclophospha- mide daily resulted in disappearance of demonstrable lymphosarcoma in several weeks, and she continued to receive these drugs.
Several months later she had neuritis secondary to lymphosarcomatous involvement of the optic nerves. Cyclophosphamide therapy was discontinued, and the prednisone dosage was increased to 60 mg daily. Vi- sual acuity improved after intrathecal administration of methotrexate and radiotherapy to the base of the skull.
On December 22, 1969, the patient complained of a sore throat. Examination revealed reddening of the pharynx without exudate. During the following week, she complained of mild shortness of breath and weak- ness. Her temperature was 102’F four days later at which time physical examination and chest roentgeno- gram (Figure 1A) revealed no abnormalities. A leuko-
cytosis (12,000 cells/cu mm) was noted with a shift to the left. The patient remained intermittently febrile and experienced increasing shortness of breath, fa- tigue and pain from the neck to mid-back.
On December 29 she experienced flushing and chills, and she became severely dyspneic. When ad- mitted to Memorial Hospital her vital signs were blood pressure 70/40 mm Hg, pulse rate 120/minutes, tem- perature 101.2”F and respirations 40/minute. Cya- nosis was evident. The oropharynx was slightly red- dened. There was no exudate. The chest was clear to percussion and auscultation. There was no peripheral adenopathy. The liver and spleen were not enlarged.
Laboratory studies gave the following results: hemo- globin value 13.0 gm per cent, platelet count 304, OOO/cu mm, white blood cells 12,3OO/cu mm (75 poly- morphonuclear leukocytes, 4 basophils, 6 monocytes and 15 lymphocytes), arterial blood pH 7.50, arterial oxygen tension (PaOs) 34 mm Hg, oxygen saturation 69 per cent, carbon dioxide 13.1 mEq/L, arterial car- bon dioxide tension (PaCOs) 16.7 mm Hg. A chest roentgenogram revealed “extensive bilateral infiltrate, largely of an alveolar type. Marked change since De- cember 26, 1969” (Figure 1 B).
Immediate treatment consisted of fluid replacement, intravenous cortisol, cephalothin, gentamicin and gamma globulin. Despite administration of nasal oxy- gen, the patient remained dyspneic and cyanotic. Shortly before death the chest was described as “clear with distant breath sounds.” Twelve hours after admission, the patient became apneic and died.
At autopsy effusions were limited to 60 cc of fluid in each pleural space. Together the lungs weighed 1,400 gm. Both were diffusely consolidated. The cut surfac- es were dry, grey-white, and there was no exudate. Cultures of tissue from the right lung for bacteria and fungi were sterile. Microscopically, numerous sections from both lungs showed the characteristics of Pneu- mocystis carinii pneumonia (Figure 2). Lymphomatous infiltrates were present in the stomach, bone marrow and adrenal glands.
Comment: The course of this patient’s illness demonstrates the importance of having a high index of suspicion for Pneumocystis pneumonia. Beginning with a complaint of sore throat it evolved rapidly over eight days to terminate in re- spiratory alkalosis with refractory hypoxemia. Three days before death the lung fields were clear on roentgenograms, and physical signs were ab- sent; terminally there was a diffuse alveolar and interstitial infiltrate although physical signs in the chest were still minimal.
Group B
Case 2. This patient (M.S.) was thirty-five years old in 1965 when the diagnosis of Hodgkin’s disease was made, and she received treatment for mediastinal and supraclavicular adenopathy. Thereafter she received multiple courses of local radiation, but none included
432 October 1972 The American Journal of Medicine Volume 53

PNEUMOCYSTIS CARlNIl PNEUMONIA-ROSEN ET AL.
Figure 1. Case 1. Chest roentgeno- grams showing the rapid progr@ssion over three days of a widespread Pneumocystis carinii pneumonia.
the lungs directly. A chest roentgenogram in July 1969 showed clear lung fields.
In August 1970 the accumulation of ascites resulted in shortness of breath. A nonproductive cough began in the first week of September, and the patient was admitted to Memorial Hospital. Bilateral pleural effu- sions and hilar adenopathy were seen on roentgeno- grams. Focal linear atelectasis and changes sugges- tive of an infiltrate were noted in the right lung. Breathing improved after bilateral thoracenteses. Ra- dioactive phosphorus (10 PC) was instilled into each pleural space. Chest tubes were left in place. Treat- ment with prednisone was instituted and maintained at 60 mg daily.
Loculated fluid persisted in the right major fissure,
and reaccumulation of effusions was noted on serial
chest films. In early November, treatment with meth- ylhydrazine, 200 mg daily, was begun. Although the patient was weak and had persistent exertional dysp- nea, these symptoms did not progress.
In mid-December 1970 a nonproductive cough de- veloped. No new changes were noted on a chest film. The patient was treated with ampicillin for presumed bronchitis. Because of progressing respiratory insuffi- ciency, she was readmitted to Memorial Hospital on December 26, 1970.
Vital signs were temperature 99.4”F, pulse rate 120/minute and regular, blood pressure 100/75 mm Hg, respirations 40/minute. There were signs of bi- lateral pleural effusion, and fine rales were heard inter- mittently in both lungs. A pleural rub was audible over the left lateral chest wall.
Laboratory studies disclosed the following: hemo- globin value 9.3 gm/lOO ml, white blood cell count 2, 7OO/cu mm, platelet count 31,OOO/cu mm, total pro- tein 6.0 gm/lOO ml, albumin 2.6 gm per cent, alpha, globulin 0.44 gm per cent (normal 0.08 to 0.30 gm per cent), alphas globulin 1.54 gm per cent (normal 0.28 to 1.04 gm per cent), beta globulin 0.87 gm per cent (normal 0.46 to 1.02 gm per cent), gamma globulin 0.55 gm per cent (normal 0.93 to 1.93 gm per cent). Chest roentgenogram showed, in addition to long- standing changes, “bilateral diffuse alveolar infiltrates” (Figure 3).
Treatment with cephalothin and nasal oxygen was begun. Dyspnea persisted after a right thoracentesis. The patient remained afebrile. Roentgenographically, the parenchymal infiltrates appeared denser on the second hospital day.
Over the subsequent twenty-four hours she became increasingly dyspneic and cyanotic. Shortly before death on December 29, the following arterial blood
Figure 2. Pneumocystis in alveolar space. Methenamine silver stain.
October 1972 The American Journal of Medicine Volume 53 433

PNEUMOCYSTIS CARlNIl PNEUMONIA-ROSEN ET AL.
Figure 3. Case 2. Chest roentgenogram showing an unusual ground glass appearance due to a combina- tion of Pneumocystis carinii infection and lung infiltra- tion with Hodgkin’s disease.
gas results were obtained: pH 7.51, PaC02 27 mm Hg, carbon dioxide 21 mEq/L, Pa02 51 mm Hg, oxygen saturation 89 per cent.
Autopsy was limited to the thorax. Diffuse fibrous pleural adhesions were present bilaterally. A total of 1,000 cc of fluid were present in the pleural spaces. The lungs were diffusely congested and consolidated. A grey-white infiltrate was present in the upper lobe of the right lung. Microscopically, sections from both lungs revealed a vacuolated intra-alveolar exudate in which Pneumocystis carinii was demonstrated. The in- terstitial infiltrate of plasma cells and lymphocytes var- ied from scanty to moderately cellular in different por- tions of both lungs. Reactive hyperplasia of alveolar lining cells and focal hyaline membranes were present throughout the lungs. The pleura was fibrotic and there was an organizing pleural exudate. No Hodgkin’s dis- ease could be identified in the lungs.
Comment: Hodgkin’s disease in this patient was
complicated by recurrent pleural effusions which
were treated by chest tube drainage and instilla-
tion of radioactive phosphorus. The final illness represents a marked acceleration of preexisting respiratory compromise. The clinical findings dur- ing hospitalization were highly suggestive of Pneu- mocystis carinii pneumonia. Although this was the major pathologic process seen in the lungs at au- topsy, the effects of chronic pleural effusion, ra- diation and respirator support were also apparent.
Group C
Case 3. A thirty-six year old white woman (M.C.) was found to have Hodgkin’s disease in a left cervical
lymph node in January 1963. Radiation was given to multiple sites for local disease. An episode of dissemi- nated cutaneous herpes zoster developed two years later and healed slowly with supportive treatment in- cluding gamma globulin injections. Treatment with prednisone, 20 mg daily, and vincristine was begun in October 1966. In January 1967 it was necessary to raise the steroid gosage to control fever, and she was maintained on 60 mg daily. Because of pancytopenia, other therapy was discontinued.
The following month she was hospitalized in a ter- minal state with fever, vomiting and abdominal pain. Severe esophagitis thought to represent a combined fungal and viral infection did not respond to treatment with mycostatin, amphotericin B or intravenously ad- ministered cytosine arabinoside.
Cyanosis was first noted a week before death, and rales were heard at the base of the right lung. Chest roentgenogram showed haziness of both lung fields consistent with a lymphangitic infiltrate or pulmonary edema. Respiratory insufficiency progressed, persist- ent intestinal hemorrhage developed, and the patient died (Figure 4).
At autopsy Hodgkin’s disease was present in multi- ple lymph nodes, spleen and gallbladder, and there was severe atrophy of bone marrow. The esophagus and larynx were the site of diffuse, severe ulcerative herpetic infection with bacterial overgrowth consisting of mixed flora including Pseudomonas aeruginosa and Enterobacter species.
The lungs were the site of a widespread hemorrhag- ic necrotizing pneumonia with multiple foci of abscess formation. Nuclear cytomegalovirus inclusions oc- curred throughout the areas of hemorrhagic pneumo- nia. Gram-negative bacilli were demonstrable in re- gions of purulent pneumonia. In microscopic fields which lacked features of either cytomegalovirus or bacterial infection there was a distinct interstitial pneumonia in which Pneumocystis carinii was demon- strated.
Figure 4. Case 3. Chest roentgenogram that is high- ly suggestive of Pneumocystis carinii pneumonia. The major pathologic processes are, in fact, due to Pseudomonas aeruginosa and cytomegalovirus.
434 October 1972 The American Journal of Medicine Volume 53

Comment: It was clear in this case that Pneumo- cystis carinii was responsible only in part for the patient’s respiratory signs and symptoms. Various microbial infections and infiltrative neoplastic dis- ease seem to have played a more important role in causing respiratory insufficiency in this third
group of patients.
DIAGNOSIS AND TREATMENT OF P. CARlNIl PNEUMONIA
A diagnosis of Pneumocystis pneumonia was con- sidered clinically in six patients. Aspirated trache- al secretions were studied in each, but the orga- nisms were not identified. Lung biopsy was per- formed in five patients. In four this led to identifi- cation of Pneumocystis carinii. Biopsy of the left lung in the fifth patient (D.S.) revealed only mild inflammation. Treatment with pentamidine isothio- nate (4 mg/kg/day) was begun, but she died three days later. At autopsy Pneumocystis carinii was present in the lungs.
Three of the four patients in whom the diagno- sis was established by biopsy were treated with pentamidine isothionate. One child (J.P.) re- sponded [6] coincident with remission of his leu- kemia. He died five months later with uncontrolled leukemia and gastrointestinal hemorrhage. Respi- ratory symptoms prior to death suggested recur- rence of Pneumocystis pneumonia. Although a definite diagnosis could not be established by ex- amination of tracheal secretions, he was treated terminally with pentamidine. No autopsy was per- formed. The second patient (A.M.) treated with pentamidine died a week after a ten day course of therapy without evidence of improvement. Autopsy revealed persistent Pneumocystis organisms throughout both lungs and an organizing pneumo- nia. The third patient (E.C.) died after six days of treatment. Although inflammatory changes and an alveolar exudate were present, the cysts were no longer demonstrable.
A fourth patient (F.B.) proved to have Pneumo- cystis pneumonia by lung biopsy in 1963 is the subject of a previous case report [7]. The patient was seen prior to the availability of pentamidine and because of pulmonary fibrosis was treated with adrenal steroids. He survived four months after diagnosis. Autopsy revealed extensive inter- stitial fibrosis and organizing pneumonia, particu- larly in the lower lobes. In addition to the evi-
dence of widespread Pneumocystis pneumonia, foci of cytomegalovirus infection were present.
COMMENTS
The increase in the number of cases of Pneumo- cystis carinii pneumonia over the past two years
PNEUMOCYSTIS CARlNIl PNEUMONIA-ROSEN ET AL.
apparently reflects an increased incidence since the number of patients admitted to this hospital, including those with lymphoma and leukemia, has remained nearly constant. Greater interest in the disease in recent years may have prompted more careful search for less obvious infections.
Our findings coincide with prior observations [8,9] that among patients with neoplastic disease Pneumocystis carinii pneumonia has been ob- served most often in those with malignant lympho- ma or leukemia. The predilection for lymphomas and leukemia6 is possibly as much related to ef- fects of the therapeutic agents employed as it is a direct consequence of the primary disease. Leukopenia, hypoalbuminemia and hypogamma- globulinemia may be contributing factors but were not of exceptional severity or duration in these pa- tients under treatment for primary neoplastic dis- eases.
A number of studies have demonstrated that the evolution of experimentally induced Pneumo- cystis pneumonia in laboratory animals can be in- fluenced by certain drugs. The pneumonia fol- lowing administration of cortisone in rabbits shows a diminished interstitial and alveolar exudate [lo] and is less symptomatic. After termination of ste- roid treatment, the characteristic interstitial and intra-alveolar reaction develops, and the animals become increasingly symptomatic. The adminis- tration of chlorambucil and aminopterin potentiates the capacity of cortisone to induce pneumonia in rats [ll], and active infection can be induced ex- perimentally by the administration of cyclophos- phamide alone.
Virtually every patient in this study was under treatment with cortisone. The abundance of cellu- lar reaction in different parts of a given lung as well as between individual patients did not appear to correlate with type, duration or dosage of chemotherapy. The cellular reaction was not more prominent in patients in whom steroid therapy was discontinued in the two months before death. It remains possible, however, that the influence of chemotherapy on the exudative reaction may in part explain the discrepancy between intensity of symptoms and the findings on physical examina- tion or chest roentgenogram as exemplified by Case 1.
The development of interstitial fibrosis in asso- ciation with Pneumocystis pneumonia was recent- ly reported in a patient with mycosis fungoides [12]. Details of therapy in the early part of that patient’s illness are not given. We have seen four examples of pulmonary interstitial fibrosis and ex- tensive Pneumocystis pneumonia. Three of these are included in this study.
October 1972 The American Journal of Medicine Volume 53 435
PNEUMOCYSTIS CARlNIl PNEUMONIA-ROSEN ET AL
Pulmonary fibrosis does not seem to follow un- complicated Pneumocystis pneumonia in experi-
mental animals [ll]. In our experience interstitial fibrosis has been found in patients under treat- ment with chemotherapeutic agents known to cause such pulmonary changes. Consequently, al- though interstitial fibrosis might be a result of Pneumocystis pneumonia, we believe the evi- dence to substantiate this is still inconclusive.
Three different subgroups of disease due to Pneumocystis carinii were established on the basis of pathologic findings. These could not be distinguished clinically. Since group 6 includes one and group C includes more than one other pulmonary disease, some potentially treatable, it is important to ascertain exactly how many pro- cesses are producing the clinical picture pre- sumed to be due to Pneumocystis carinii. Requi- site studies include cultures for bacteria, fungi and viruses as well as histopathologic studies with special stains. It seems inappropriate to treat in- terstitial pneumonia empirically with pentamidine [13] until an attempt has been made to identify all the pathologic processes responsible for it.
Study of smears of aspirated tracheal secre- tions has not been of assistance in identifying Pneumocystis carinii in this hospital. Although an attempt at diagnosis by this method may be made, a negative result is inconclusive. When the clinical situation is strongly suggestive of Pneumo- cystis pneumonia, a lung biopsy should be per- formed promptly unless contraindicated by the status of the patient. The decision between a needle or surgical biopsy will depend on individual circumstances, but the latter seems preferable
because it offers better control of potential bleed- ing and more material is obtained for study not only for Pneumocystis carinii but also for other potential pathogens.
Staining technics which may be employed to identify the Pneumocystis cysts have been de- scribed in detail elsewhere [6]. It is helpful if im- prints or touch preparations are made from a bi- opsy specimen immediately after it is obtained. These may be stained immediately, thus avoiding the delay necessitated by tissue processing. Char- acteristically, the cysts are observed in groups, usually embedded in a proteinaceous matrix. Touch preparation smears should be interpreted with caution by the inexperienced. Erythrocytes may mimic the cysts in improperly stained slides and some fungi (Cryptococcus and Candida species) may be mistaken for Pneumocystis.
An elevation in serum cold agglutinin titers has been noted in some patients with Pneumocystis pneumonia [14]. The data from our patients are limited (Table I I), but in none of the five studied was the cold agglutinin titer greater than 1:20. Cold agglutinins, along with other serologic abnor- malities, have been noted in infection due to cytomegalovirus [15]; the patients with elevated cold agglutinins in the study mentioned [14] all had concomitant cytomegalovirus infections. It is probable that this serologic reaction was due to the viral infection rather than to Pneumocystis.
ACKNOWLEDGMENT
We express our appreciation for the assistance of Miss Donna Nager in the preparation of this manuscript.
REFERENCES
1. lvady G, Paldy L. Unger G: Further experiences in the treatment of interstitial plasma cell pneumonia with pentamidine. Mschr Kinderheilk 111: 297. 1963.
2. De Vita VT, Emmer M. Levine A. Jacobs A, Berard C: Pneumocystis carinii pneumonia. Successful diag- nosis and treatment of two patients with associated malignant processes. New Eng J Med 280:287, 1969.
3. Western KA, Perera DR. Schultz MG: Pentamidine isothionate in the treatment of Pneumocvstis carinii pneumonia. Ann Intern Med 73:695, 1970. .
4. Robbins JB: Immunological and clinicopathological as- pects of Pneumocystis carinii pneumonitis. Birth De- fects: Immunologic Deficiency Diseases in Man, vol 4, National Foundation, March of Dimes, 1969, p 219.
5. Tan-Vinh L. Cochard AM. Dong VT, Solonar W: Diag- nostic in vivo de la pneumonie a Pneumocystis. Arch Franc Pediat 20: 773. 1963.
8. Hendry WS, Patrick R: Observation on thirteen cases of Pneumocystis carinii pneumonia. Amer J Clin Path 38: 401, 1962.
9. Hamfin WB: Pneumocystis carinii. JAMA 204: 173.1968. 10. Sheldon WH: Experimental pulmonary Pneumocystis
carinii infection in rabbits. J Exp Med 110: 147, 1959.
11. Frenkel JK, Good JT, Schultz JA: Latent Pneumocystis infection of rats, relapse and chemotherapy. Lab In- vest 15: 1559,1966.
12. Whitcomb MD, Schwarz MI. Charles MA. Larson PH: Interstitial fibrosis after Pneumocystis carinii pneu- monia. Ann Intern Med 73: 761, 1970.
13. Goode11 B, Jacobs JB, Powell RD, De Vita VT: Pneumo- cystis carinii. The spectrum of diffuse interstitial pneumonia in patients with neoplastic diseases. Ann Intern Med 72: 337, 1970.
6. Exelby PR, Murphy LM, Armstrong D, Rosen PP, Ramos 14. Rifkind D, Faris TD, Hill RB: Pneumocystis carinii C. Rosen G, Fish B: Pneumocystis carinii. Memorial pneumonia. Studies on the diagnosis and treatment. Hosp Bull 1: 23.1971. Ann Intern Med 65: 943, 1966.
7. Nicastri A. Hutter RVP, Collins HS: Pneumocystis carinii 15. Kantor GL. Goldberg LS. Johnson L et al: Immunologic pneumonia in an adult. New York J Med 65: 2149, abnormalities induced by post-perfusion Cytomegalo-
1965. virus infection. Ann Intern Med 73: 553, 1970.
436 October 1972 The American Journal of Medicine Volume 53





























