Embed Size (px)
Citation preview

1
Post Partum Haemorrhage Record Type
Clinical Guideline
eLibrary ID Reference No: CG 971 Newly developed and approved Trust-wide Clinical Guidelines will be allocated an eLibrary reference number following
submission to relevant eLibrary administrator. Reviewed Clinical Guidelines must retain the original eLibrary reference id number.
Version: V4 Name of Approving Trust Committee / Forum / Body / Group
Obstetric and Gynaecology QPS Meeting
Date of Approval November 2015 Review Date September 2018 Expiry Date December 2018 Author’s Name, Title & email address: Maitrayee Maitra, Locum Consultant O&G
[email protected] Jacqueline Woodman, Consultant O&G [email protected]
Reviewer’s Name, Title & email address: Maitrayee Maitra, Locum Consultant O&G [email protected] Jacqueline Woodman, Consultant O&G, [email protected]
Responsible Director’s Name & Title: Stephen Keay, Clinical Director Department / Specialty: Obstetric and Gynaecology Target audience: Maternity Services
Purpose of Record
To prevent maternal morbidity and mortality from massive haemorrhage after delivery
Key search words for eLibrary Obstetric haemorrhage, postpartum To be read in conjunction with:
Placenta praevia guideline
Location of Clinical Guideline: (please state no more than 3 eLibrary directories / sub
directories to be saved in).
Clinical Guidelines, Obstetrics
Superseded Trust –wide Clinical Guideline (if applicable):
If printed, copied or otherwise transferred from eLibrary, Trust -wide Clinical Guidelines will be
considered ‘uncontrolled copies’. Staff must always consult the most up to date PDF version which is registered on eLibrary.
2
Version Title of Trust Committee/Forum/Body/Group consulted during the development stages of this Trust-wide
Clinical Guideline
Date
1.0 Obstetric and Gynaecology QPS Meeting

3
Table of Contents
Paragraph Number Description Page
Number 1.0 Scope 4 2.0 Introduction 4 3.0 Statement of Intent 4 4.0 Definitions 4 5.0 Duties/Responsibilities 4 6.0 Details of the Record 4-11 7.0 Dissemination and Implementation 11 8.0 Training 12 9.0 Monitoring Compliance
Monitoring Table 12-13
10.0 Staff Compliance Statement 13 11.0 Equality and Diversity Statement 13-14 12.0 UHCW Associated Records 14 13.0 References and Bibliography 14-15 14.0 Evidence based references
Reference table Evidence supporting recommendations
15-16
15.0 Appendices 17-18

4
1.0 SCOPE This guideline details actions to be taken by members of the maternity team in the event of postpartum haemorrhage. This covers postpartum haemorrhage, including intraoperative cell salvage and interventional radiology. This departmental guideline builds on the ‘Massive Haemorrhage Policy GOV/POL/004/11. Note this policy is the over-arching trust wide policy. 2.0 INTRODUCTION Postpartum haemorrhage remains a significant cause of maternal mortality. Active intervention in an appropriate sequence has been shown to reduce maternal mortality.
3.0 STATEMENT OF INTENT This document is produced in order to educate and guide members of the maternity team to give the highest standard of care to mothers who bleed.
4.0 DEFINITIONS Obstetric blood loss of more than 500mL for a vaginal delivery and more than 1000mL for a Caesarean section will trigger an obstetric emergency call. A blood loss of more than 1500mL and ongoing will trigger a massive obstetric haemorrhage (MOH) call. PPH: postpartum haemorrhage 5.0 DUTIES / RESPONSIBILITIES All staff should familiarise themselves with this guideline, including: x Midwives x Obstetricians x Anaesthetists x Operating department practitioners x Theatre staff x Haematologists and biomedical scientists
x DETAILS OF THE DOCUMENT Postpartum Haemorrhage (PPH) Introduction: Postpartum haemorrhage is conventionally defined as a blood loss in excess of 500 ml after vaginal delivery or 1000 ml after caesarean section.
x PPH can be minor (500–1000 ml) or major (more than 1000 ml). x Major could be moderate (1000–2000 ml) or severe (more than 2000 ml).(RCOG,2009)
Successful outcome requires prompt action, effective communication and leadership.
5
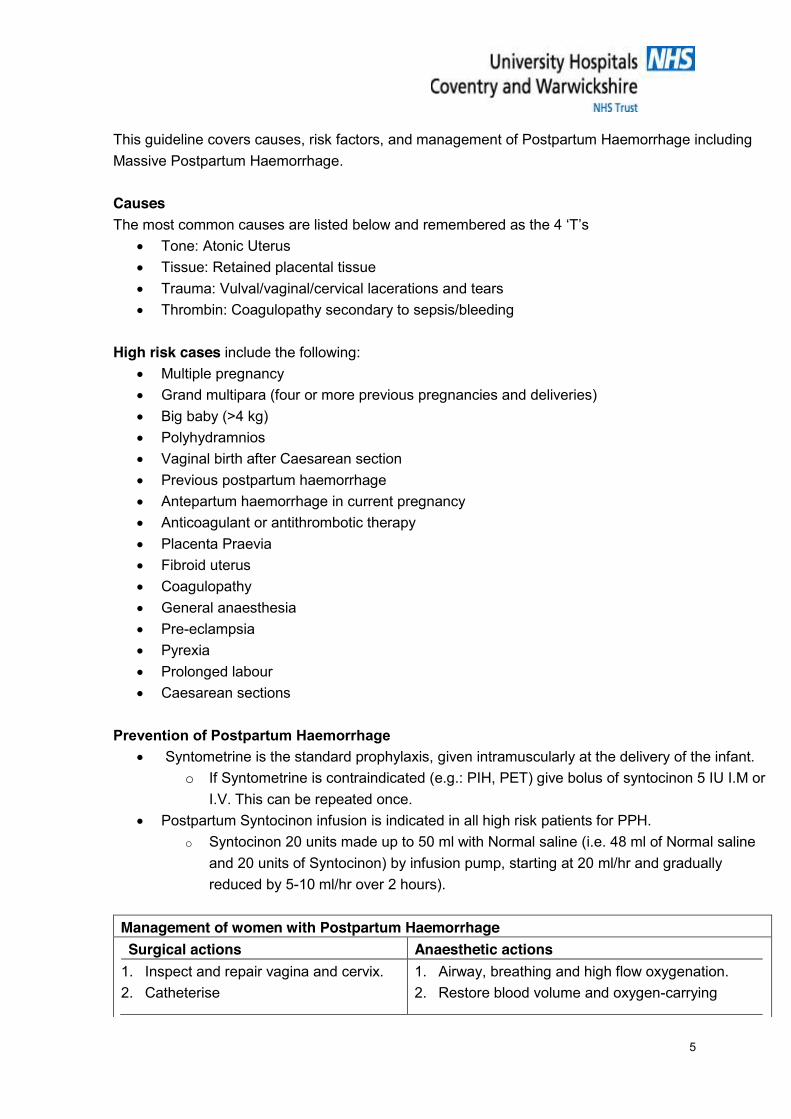
This guideline covers causes, risk factors, and management of Postpartum Haemorrhage including Massive Postpartum Haemorrhage. Causes The most common causes are listed below and remembered as the 4 ‘T’s
x Tone: Atonic Uterus x Tissue: Retained placental tissue x Trauma: Vulval/vaginal/cervical lacerations and tears x Thrombin: Coagulopathy secondary to sepsis/bleeding
High risk cases include the following:
x Multiple pregnancy x Grand multipara (four or more previous pregnancies and deliveries) x Big baby (>4 kg) x Polyhydramnios x Vaginal birth after Caesarean section x Previous postpartum haemorrhage x Antepartum haemorrhage in current pregnancy x Anticoagulant or antithrombotic therapy x Placenta Praevia x Fibroid uterus x Coagulopathy x General anaesthesia x Pre-eclampsia x Pyrexia x Prolonged labour x Caesarean sections
Prevention of Postpartum Haemorrhage
x Syntometrine is the standard prophylaxis, given intramuscularly at the delivery of the infant. o If Syntometrine is contraindicated (e.g.: PIH, PET) give bolus of syntocinon 5 IU I.M or
I.V. This can be repeated once. x Postpartum Syntocinon infusion is indicated in all high risk patients for PPH.
o Syntocinon 20 units made up to 50 ml with Normal saline (i.e. 48 ml of Normal saline and 20 units of Syntocinon) by infusion pump, starting at 20 ml/hr and gradually reduced by 5-10 ml/hr over 2 hours).
Management of women with Postpartum Haemorrhage Surgical actions Anaesthetic actions
1. Inspect and repair vagina and cervix. 2. Catheterise
1. Airway, breathing and high flow oxygenation. 2. Restore blood volume and oxygen-carrying
6
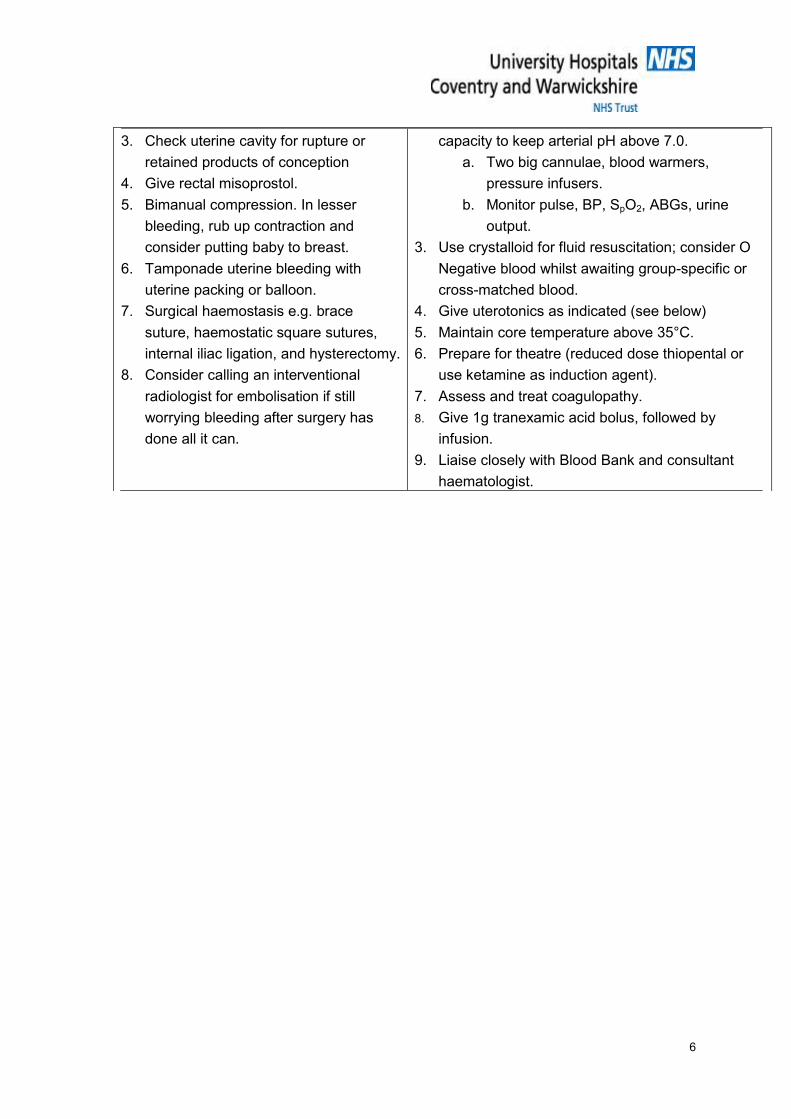
3. Check uterine cavity for rupture or retained products of conception
4. Give rectal misoprostol. 5. Bimanual compression. In lesser
bleeding, rub up contraction and consider putting baby to breast.
6. Tamponade uterine bleeding with uterine packing or balloon.
7. Surgical haemostasis e.g. brace suture, haemostatic square sutures, internal iliac ligation, and hysterectomy.
8. Consider calling an interventional radiologist for embolisation if still worrying bleeding after surgery has done all it can.
capacity to keep arterial pH above 7.0. a. Two big cannulae, blood warmers,
pressure infusers. b. Monitor pulse, BP, SpO2, ABGs, urine
output. 3. Use crystalloid for fluid resuscitation; consider O
Negative blood whilst awaiting group-specific or cross-matched blood.
4. Give uterotonics as indicated (see below) 5. Maintain core temperature above 35°C. 6. Prepare for theatre (reduced dose thiopental or
use ketamine as induction agent). 7. Assess and treat coagulopathy. 8. Give 1g tranexamic acid bolus, followed by
infusion. 9. Liaise closely with Blood Bank and consultant
haematologist.
7
Drugs for Postpartum Haemorrhage 1. Natural oxytocics: rub up contraction and put baby to breast. 2. Repeat Syntometrine 1 ml i.m. 3. Ergometrine 500 µg i.m. (not if further Syntometrine given) or 100 µg i.v. repeated as needed.
Ensure that there are no contra-indications. 4. Carboprost (Hemabate) 250 µg i.m. every 15 minutes to a maximum of eight doses. 5. Misoprostol 1000 micrograms per rectal 6. Oxytocin (Syntocinon) post partum infusion for maintenance (not first line drug). 7. Consider systemic haemostatics like Tranexamic acid Massive Obstetric Haemorrhage – Labour Ward Emergency Management Definition: Blood loss exceeding 1500 ml and ongoing or more than 150 ml per minute. x Tachycardia, hypotension, and vasoconstriction in an obstetric patient represent severe
hypovolaemia: A young pregnant woman will typically maintain her vital signs relatively normally until more than 2 litres are lost, but thereafter decompensation might be very quick.
x Coagulopathy may cause haemorrhage. Haemorrhage causes coagulopathy. In the emergency situation, err on the side of caution: if the blood loss – especially the cumulative blood loss – looks alarming, then activate the massive haemorrhage pathway. Phase 1: If a woman in a labour ward room has bled > 1500ml, or if ongoing bleeding appears excessive to the attending midwife, pull the emergency knob (red triangle on the wall).
x This should bring a senior obstetrician, a senior anaesthetist, the labour midwife ward
coordinator. Please note, this will not include alerting the porter. If the woman is already in maternity theatre and begins to bleed excessively, proceed straight to Phase 2.
x On arrival, the senior obstetrician, or the most senior person present, should assess immediately if the massive haemorrhage protocol should be activated (Phase 2)
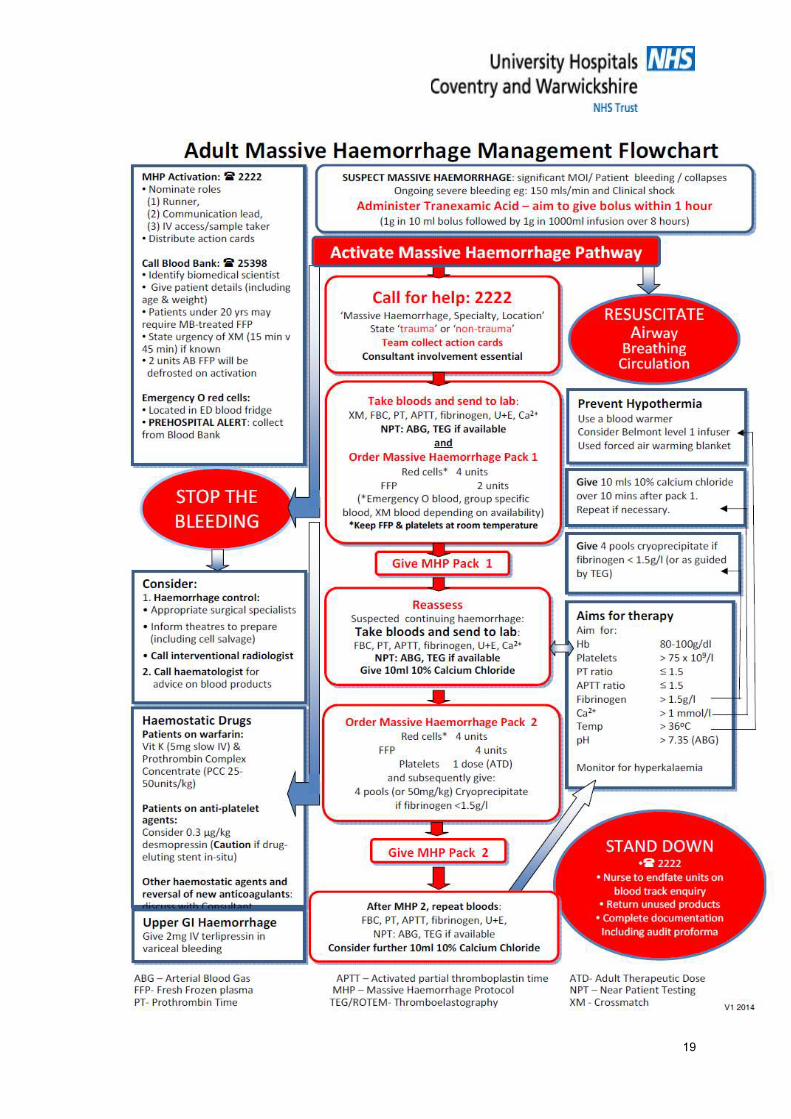
Phase 2: Activation of the Massive Obstetric Haemorrhage (MOH) protocol If blood loss exceeds 1500 mL and continuing, or is continuing at 150ml/min, activate the “MOH protocol”. (Appendix 1) 1. Activate Protocol
x Ring 2222 x State: Massive Obstetric Haemorrhage –Location e.g. ‘Massive haemorrhage, obstetrics, labour ward room 4.’ ‘Massive haemorrhage, obstetrics, maternity theatre 1.’
x After the MOH call has been activated, the Labour Ward Co-ordinator must immediately call
Blood Bank X 25398 to state which blood components are needed. When the co-ordinator contacts the blood lab immediately after the 2222 call they must give the patient name, hospital number, and ongoing situation. This needs to be regularly updated until the MOH is stood down.

8
The following people should also be informed of the emergency if the clinical situation
warrants: x Transfusion laboratory biomedical scientist (BMS) who will inform the on duty coagulation
biomedical scientist (BMS) x Out of hours, the '2813' Senior Resident Anaesthetist will need to be fast bleeped. x Hospital bleep holder (modern matron / hospital at night coordinator) x Critical care – senior doctor on site
Critical care – nurse in charge
Allocation of team roles
x Team Leader. The most senior obstetrician present should assume this role, except when neither the consultant nor registrar has yet arrived, in which case it is the most senior person present. The team leader should then designate the following roles:
x Communication Lead. Usually a junior doctor – to liaise with Blood Bank, porters and other departments.
x Sample Taker / IV access establisher / documenter. Usually a junior doctor. x Runner. The porter, or in their absence a healthcare support worker, who should stay
designated to this incident until it is over. x Patient carer. The midwife caring for the woman should ensure that she is kept informed and
reassured as far as possible, and that the baby’s care is not forgotten.
Blood The Team Leader should decide on which red blood cell component should be transfused first. This will involve communication with Blood Bank via the communication lead, e.g. to ascertain suitability for electronic issue.
x Immediately available in blood fridge - If already cross matched for this patient x Immediately available - Emergency O Neg blood (available in Labour ward fridge) x 5-10 minutes - Electronic issue blood (if patient known to be suitable) x 15-20 minutes - Red Label blood (ABO RhD specific, but not cross-matched). x 45-60 minutes - Standard issue blood (fully cross-matched) x PLEASE NOTE: Some patients with red cell antibodies are not suitable for O-Neg flyers
(those in blood fridge) if the patient has been discussed at the MDT meeting that information is available in the hospital pregnancy record (it may not appear in PHR). Blood bank may have a suitable alternative in these cases i.e. antigen negative group O. Contact blood bank for advice.
Request immediate setting up of cell salvage if it is not already in action. Ensure warming of blood products. Consider use of Belmont Transfusion System (from Main Theatres)
9
x The Communication Lead should contact Blood Bank on x25398 or bleep 2169: x State “This is regarding the massive haemorrhage in obstetrics in (location).” x Give your name, location, extension number, and personal bleep number. x Obtain the name of the allocated Blood Bank biomedical scientist who will deal with this case x State the patient’s details: surname, forename hospital number, DOB. x State whether O Neg blood has been used and how many units x Ask if there is blood already cross-matched for this patient, and if so, where it is x Ask whether the patient is ‘suitable for electronic issue.’ (i.e. further fully compatible blood
can be issued rapidly) x Inform them of the team leader’s estimate of units of red cells likely to be required, and the
urgency for their issue x Request 2 units of FFP in Pack 1 unless DIC is suspected (e.g. APH, amniotic fluid
embolism), in which case request 4 units of FFP in Pack 1.
If the patient moves clinical area, communication lead should dial 2222 and request that a message goes out: ‘Massive haemorrhage, obstetrics, moving from (location) to (location)”.
x The Sample Taker should: x Complete request forms, take blood samples, and label samples correctly and fully at the
bedside, where possible BEFORE any blood components have been given. x Samples to be taken: FBC, coagulation screen, fibrinogen (to be decided by senior
obstetrician depending on the clinical picture), U&E’s, Crossmatch x The obstetrician to decide if Fibrinogen required – this is needed particularly in cases of
placental abruption and cases of intra-uterine death and ongoing bleeding x Give samples/forms to Runner to take to laboratory as quickly as possible. x Ensure IV access is adequate. x Document all actions, observations and fluids infused. x Ensure that all blood used is autofated (ask midwife to do this) x If O Neg emergency blood is used, complete documentation attached and return to blood
bank after the emergency is over. x Further samples (FBC, PT, aPTT, Fibrinogen, U&E’s) should be taken every 60 mins while
haemorrhage requires active management. x Use of TEG (located in Cardiac ITU or Cardiac theatres) should be considered to direct blood
product transfusion. 2. Team Leader will lead and coordinate obstetric management of the haemorrhage
(surgical and pharmacological), including discussion with an interventional radiologist if arterial embolisation is being considered.
3. The senior anaesthetist present will direct the resuscitation, and the fluid/blood product
management. He/she will also consult the on-call consultant haematologist for advice on blood product use, and especially if recombinant factor VIIa is being considered.
10
Resuscitation Priorities The priorities in resuscitation include in decreasing order of importance:
x Restoring blood volume to maintain tissue perfusion and oxygenation. x Restoration of oxygen-carrying capacity with adequate haemoglobin concentration. x Securing haemostasis through surgical treatment of the cause of bleeding or by correcting
coagulopathy. Delay in restoration of circulating volume (with warmed crystalloid fluids, then blood) may result in tissue hypoperfusion, organ failure and disseminated intravascular coagulopathy. Complications of resuscitation Iatrogenic complications of resuscitation are important and you should be alert for them.
x Pulmonary oedema, occurring as a result of over-vigorous crystalloid or colloid therapy (transfusion-associated circulatory overload, TACO), or when associated with transfusion-related acute lung injury (TRALI).
x Dilutional coagulopathy, occurring as a result of giving imbalanced or over-vigorous fluid therapy with insufficient blood components (fibrinogen/coagulation samples should be taken every 90 minutes).
x Blood component transfusion is associated with risk and adverse outcomes in its own right. It is positively correlated with increased risk of:
o Multi-organ failure (MOF). o Infection. o Mortality (it is a better predictor of mortality than the Injury Severity Score). o ICU admission. o Prolonged ICU and hospital stay.
x It is important to minimise transfusion by: o Controlling haemorrhage effectively. o Using cell salvage as much as possible. o Transfusing red cells for an indication, not just to improve a number. o Where red cell transfusion is indicated, giving the minimum number needed and
rechecking. For example, many patients who do need a postoperative blood transfusion will only need one unit.
Clotting disturbances
x If initial clotting studies are normal repeat after 1-2 hours. x If fibrinogen level is low patient must receive cryoprecipitate regardless of other parameters.
Talk to a haematologist. Aim for Fibrinogen >2 g/L in MOH. Deranged INR/APTT-R should be restored with FFP in the first instance.
x Platelet transfusion is rarely needed but should be considered if patient actively bleeding after delivery and platelets below 50 × 109 /L.

11
x Calcium is depleted in massive transfusion: anaesthetist should check levels on ABG and replace as appropriate.
x Hypothermia and acidosis impair coagulation so should be actively managed. Disseminated Intravascular Coagulation Disorder (DIC) Abruption is a common cause of DIC but other obstetric causes must not be forgotten:
x Prolonged hypovolaemic shock x Amniotic fluid embolism x Septic abortion x Intrauterine infection x Retained dead fetus (after about three weeks) x Pre-eclampsia x Placenta accreta x Hydatidiform mole
Management x If there seems to be widespread haemostatic failure not responding to FFP, give
cryoprecipitate followed by one adult therapeutic dose of platelets if bleeding persists. x Please note: Single units of cryoprecipitate \re no longer stocked for adult use. Pooled
cryoprecipitate is stocked and each pooled pack contains the equivalent to 5 single doses. The standard adult dose is 2 packs of pooled cryoprecipitate (NB: the MHP states 4 if fibrinogen <1.5g/l; however in obstetric cases we would aim for a fibrinogen level of more than 2g/L)
x Suspected AFE will require larger volumes of cryoprecipitate. x Obtain fresh coagulation results and haematology advice. x Consider early use of Tranexamic acid, as below. x Fibrinogen levels and TEG is useful to guide blood product use. x Keep patient warm as hypothermia worsens coagulopathy.
Tranexamic acid (Cyklokapron) x This is an antifibrinolytic agent which stabilises the formation of blood clots, by inhibiting the
conversion of plasminogen to plasmin. It is indicated in massive obstetric haemorrhage as a first line measure.
x The dose is 15 mg kg-1 repeated every four hours as necessary – in practice a single intravenous injection of 1 g (2 u 5 mL) is a suitable dose when you declare massive obstetric haemorrhage. It can be repeated immediately if bleeding is out of control.
x Postoperative infusion of 1 g over 8 hours (usually diluted into 50 ml with normal saline) x Postoperative thromboprophylaxis with enoxaparin should be established in order to prevent
further fibrin deposition. x Tranexamic acid is indicated where the fibrinolytic system has been activated by acute severe
bleeding. It should not be used when disseminated intravascular coagulation results from

12
activation of the coagulation system. In pregnancy this might result from major placental abruption, retained dead fetus, severe pre-eclampsia or amniotic fluid embolism. If you are in doubt, discuss it with a haematologist.
Intraoperative cell salvage in Obstetrics (ICSO) See the separate procedure for ICSO.
x ICSO can be used in the management of obstetric haemorrhage. While it is usually indicated for anticipated haemorrhage and for anaemia, it can be set up in less than five minutes and is indicated in the emergency setting if bleeding continues and you expect there to be more to salvage and process.
x Always send for senior assistance if you are in this position – the patient is haemorrhaging. x Check with the ODP and consider sending for another ODP. x In ongoing massive haemorrhage, do not use the reinfusion filter. The filter will slow reinfusion
down so far that it cannot be used for reinfusion as part of intraoperative red cell therapy. In this case, the balance of risk, favours rapid return of salvaged red cells. Ensure volume infused is recorded.
Interventional Radiology
x This can be considered for elective cases where a MOH is anticipated e.g.; placenta accreta x Bilateral placement of catheters into the internal iliac arteries, with perioperative balloon
occlusion or transcatheter arterial embolisation have been used effectively to control massive obstetric haemorrhage.
x However, it is a prolonged procedure needing careful planning and taking place in the radiology department. It is very unlikely to be effectively employed in an acute situation if catheters are not already in place.
Heparin and diclofenac x Diclofenac is an important component of postoperative pain relief, which itself promotes
mobilisation – the mainstay of postoperative thromboprophylaxis. It does not usually need to be withheld as a precautionary measure. When the bleeding has resolved the anaesthetist and obstetrician should discuss its use. Refrain from using it if urine output is low. Please note: Diclofenac is contraindicated in patients with known bleeding disorders and women with severe PET &/or sepsis.
x Low molecular weight heparin is the main pharmacological agent in postoperative
thromboprophylaxis. It is unlikely to cause or exacerbate postpartum haemorrhage that has resolved. It does not usually need to be withheld as a precautionary measure. When the bleeding has resolved the anaesthetist and obstetrician should discuss its use.

13
Women who refuse blood transfusion – communication and management plan See also Trust wide Policy for the Transfusion of patients who refuse consent to the use of blood and blood products. CLIN-POL-003-10. Key points:
x Indicate risk in notes. x After full checking of the woman’s view, and appropriate counselling, the appropriate patient
disclaimer paperwork should be mutually completed between the woman and the consultant. This can be a consultant anaesthetist at the consultant anaesthetic clinic.
x Standard information leaflets on refusal of blood components should be given to patient and this action should be documented in notes.
x There should be a management plan in the hand-held record, (with key points transcribed to the hospital notes).
x OPTIMISATION of patient’s haemoglobin
DISSEMINATION AND IMPLEMENTATION x On notification of upload to e-library (Document Management System), email cascade to
circulation lists. x Dissemination via newsletter TRAINING Training will be delivered as described in the Maternity Service Training Needs Analysis. Attendance and non-attendance will be managed in accordance with the Maternity Service Training Needs Analysis. See also Mandatory Training Policy. Midwives/MHCW’S x Maintaining normality and risk assessment: Induction x The sick pregnant woman: Induction and Annually x Basic life support and AED training: Induction and Annually x HDU care: Induction and Annually x Use of MEOWS chart : Induction and Annually x Recovery care: Induction and Annually Obstetricians x Critical care in obstetrics: Induction and as required thereafter, according to modular training x Basic life support and AED: Induction and Annually
14
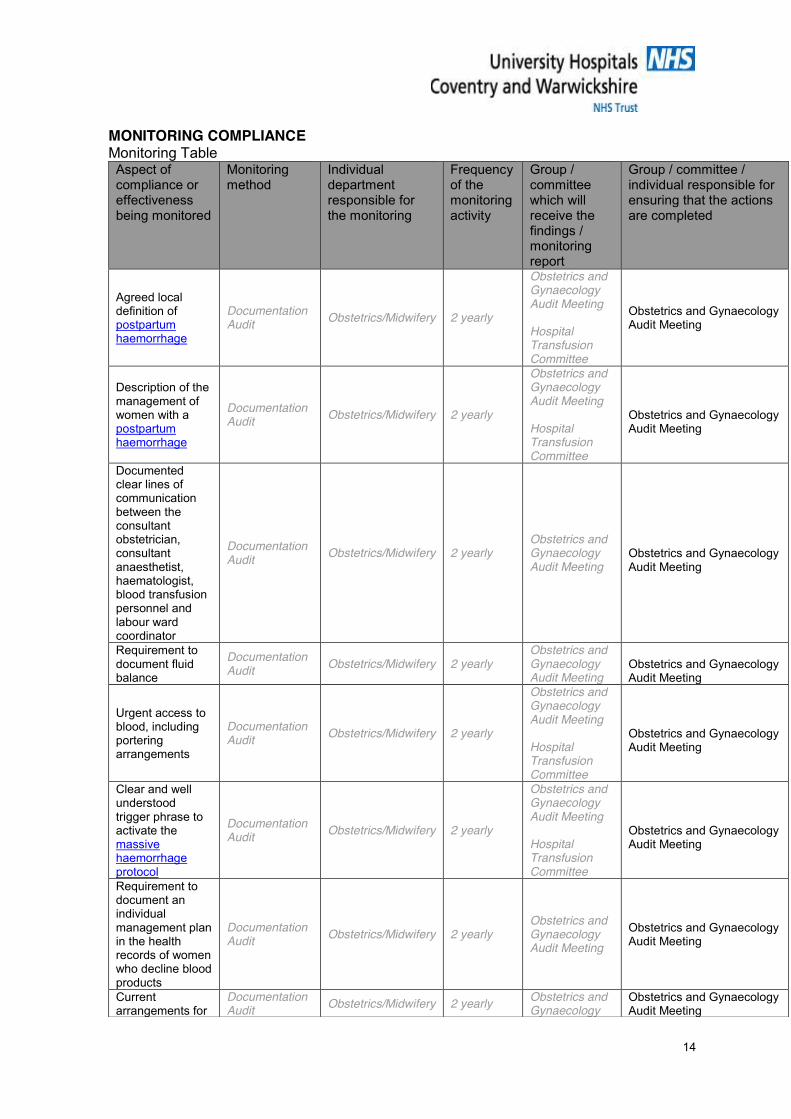
MONITORING COMPLIANCE Monitoring Table
Aspect of compliance or effectiveness being monitored
Monitoring method
Individual department responsible for the monitoring
Frequency of the monitoring activity
Group / committee which will receive the findings / monitoring report
Group / committee / individual responsible for ensuring that the actions are completed
Agreed local definition of postpartum haemorrhage
Documentation Audit Obstetrics/Midwifery 2 yearly
Obstetrics and Gynaecology Audit Meeting Hospital Transfusion Committee
Obstetrics and Gynaecology Audit Meeting
Description of the management of women with a postpartum haemorrhage
Documentation Audit Obstetrics/Midwifery 2 yearly
Obstetrics and Gynaecology Audit Meeting Hospital Transfusion Committee
Obstetrics and Gynaecology Audit Meeting
Documented clear lines of communication between the consultant obstetrician, consultant anaesthetist, haematologist, blood transfusion personnel and labour ward coordinator
Documentation Audit Obstetrics/Midwifery 2 yearly
Obstetrics and Gynaecology Audit Meeting
Obstetrics and Gynaecology Audit Meeting
Requirement to document fluid balance
Documentation Audit Obstetrics/Midwifery 2 yearly
Obstetrics and Gynaecology Audit Meeting
Obstetrics and Gynaecology Audit Meeting
Urgent access to blood, including portering arrangements
Documentation Audit Obstetrics/Midwifery 2 yearly
Obstetrics and Gynaecology Audit Meeting Hospital Transfusion Committee
Obstetrics and Gynaecology Audit Meeting
Clear and well understood trigger phrase to activate the massive haemorrhage protocol
Documentation Audit Obstetrics/Midwifery 2 yearly
Obstetrics and Gynaecology Audit Meeting Hospital Transfusion Committee
Obstetrics and Gynaecology Audit Meeting
Requirement to document an individual management plan in the health records of women who decline blood products
Documentation Audit Obstetrics/Midwifery 2 yearly
Obstetrics and Gynaecology Audit Meeting
Obstetrics and Gynaecology Audit Meeting
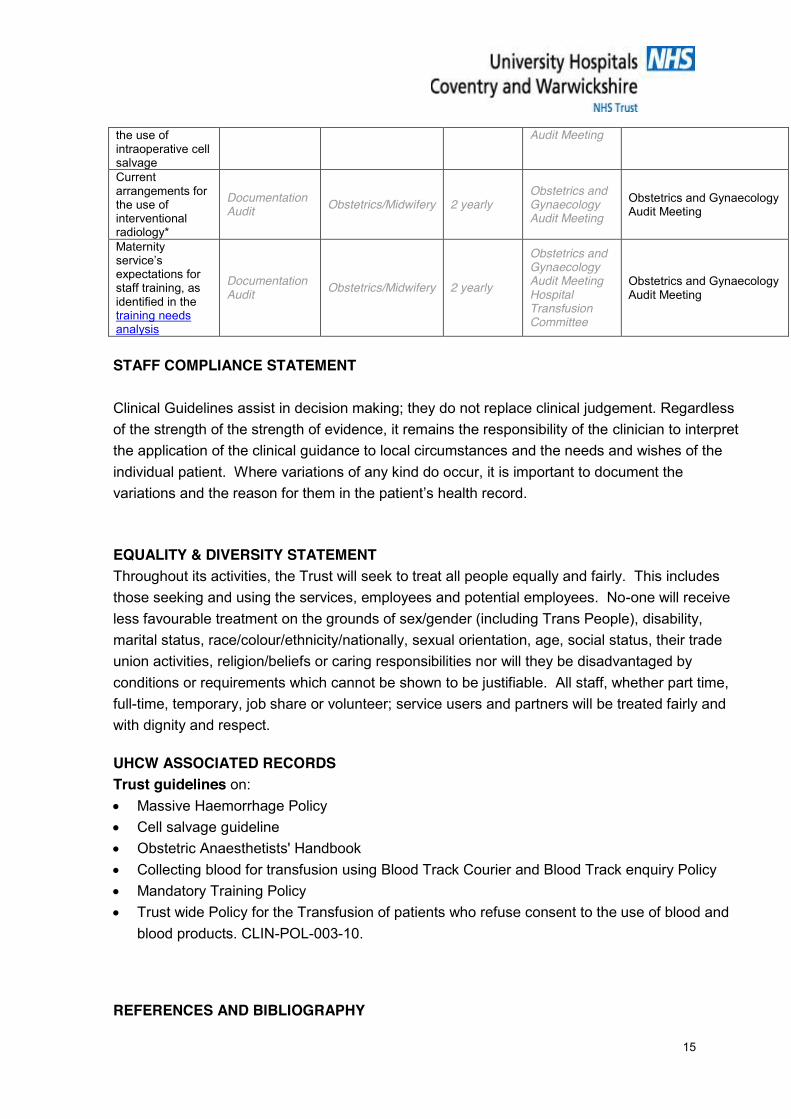
Current arrangements for
Documentation Audit Obstetrics/Midwifery 2 yearly Obstetrics and
Gynaecology Obstetrics and Gynaecology Audit Meeting
15
the use of intraoperative cell salvage
Audit Meeting
Current arrangements for the use of interventional radiology*
Documentation Audit Obstetrics/Midwifery 2 yearly
Obstetrics and Gynaecology Audit Meeting
Obstetrics and Gynaecology Audit Meeting
Maternity service’s expectations for staff training, as identified in the training needs analysis
Documentation Audit Obstetrics/Midwifery 2 yearly
Obstetrics and Gynaecology Audit Meeting Hospital Transfusion Committee
Obstetrics and Gynaecology Audit Meeting
STAFF COMPLIANCE STATEMENT Clinical Guidelines assist in decision making; they do not replace clinical judgement. Regardless of the strength of the strength of evidence, it remains the responsibility of the clinician to interpret the application of the clinical guidance to local circumstances and the needs and wishes of the individual patient. Where variations of any kind do occur, it is important to document the variations and the reason for them in the patient’s health record.
EQUALITY & DIVERSITY STATEMENT Throughout its activities, the Trust will seek to treat all people equally and fairly. This includes those seeking and using the services, employees and potential employees. No-one will receive less favourable treatment on the grounds of sex/gender (including Trans People), disability, marital status, race/colour/ethnicity/nationally, sexual orientation, age, social status, their trade union activities, religion/beliefs or caring responsibilities nor will they be disadvantaged by conditions or requirements which cannot be shown to be justifiable. All staff, whether part time, full-time, temporary, job share or volunteer; service users and partners will be treated fairly and with dignity and respect. UHCW ASSOCIATED RECORDS Trust guidelines on: x Massive Haemorrhage Policy x Cell salvage guideline x Obstetric Anaesthetists' Handbook x Collecting blood for transfusion using Blood Track Courier and Blood Track enquiry Policy x Mandatory Training Policy x Trust wide Policy for the Transfusion of patients who refuse consent to the use of blood and
blood products. CLIN-POL-003-10. REFERENCES AND BIBLIOGRAPHY

16
1. National Institute for Health & Clinical Excellence. Intraoperative blood cell salvage in obstetrics. IPG 144. 2005. London: NICE. [online] available from http://www.nice.org.uk/nicemedia/pdf/ip/IPG144guidance.pdf
2. Royal College of Obstetricians and Gynaecologists. Postpartum Haemorrhage Prevention and
Management. Green Top Guideline 52. 2009 (revised April 2011). London: RCOG Press. [online] available from http://www.rcog.org.uk/files/rcog-corp/GT52PostpartumHaemorrhage0411.pdf
3. Royal College of Obstetricians and Gynaecologists. Responsibility of Consultant On-call. Good
Practice No. 8. 2009. London: RCOG Press. [online] available from http://www.rcog.org.uk/files/rcog-corp/uploaded-files/GoodPractice8ResponsibilityConsultant.pdf
4. Royal College of Obstetricians and Gynaecologists. Blood Transfusion in Obstetrics. Green top
Guideline 47.2008. London: RCOG Press. [online] available from http://www.aogm.org.mo/assets/Uploads/aogm/Guidelines/RCOG---UK/GT47-Blood-Transfusions-in-Obstetrics.pdf
5. Royal College of Obstetricians and Gynaecologists. The Role of Emergency and Elective
Interventional Radiology in Postpartum Haemorrhage Good Practice No. 6. 2007. London: RCOG Press. [online] available from http://www.rcog.org.uk/files/rcog-corp/uploaded-files/GoodPractice6RoleEmergency2007.pdf
6. NHS Litigation Authority. Clinical Negligence Scheme for Trusts: Maternity Clinical Risk
Management Standards. Version 1. 2012/13. London: NHS Litigation Authority. [online] available from http://www.nhsla.com/NR/rdonlyres/61B58996-CD88-4840-8203-53E886981CD3/0/CNSTMaternityStandards201213.doc (see standard 3 criterion 7 Postpartum Haemorrhage ; standard 1 criterion 10 Skills and Drills)
7. Mousa HA, Alfirevic Z. Treatment for primary postpartum haemorrhage. Cochrane Database of
Systematic Reviews 2007, Issue 1. Art. No.: CD003249. DOI: 10.1002/14651858.CD003249.pub2. [online] available from http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD003249.pub2/pdf
8. Oladapo OT, Fawole B, Blum J, Abalos E. Advance misoprostol distribution for preventing and treating
postpartum haemorrhage. Cochrane Database of Systematic Reviews 2012, Issue 2. Art. No.: CD009336. DOI: 10.1002/14651858.CD009336.pub2. [online] available from http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD009336.pub2/pdf
9. Novikova N, Hofmeyr GJ. Tranexamic acid for preventing postpartum haemorrhage. Cochrane Database of Systematic Reviews 2010, Issue 7. Art. No.: CD007872. DOI: 10.1002/14651858.CD007872.pub2. [online] available from http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD007872.pub2/pdf
10. Hofmeyr GJ, Abdel-Aleem H, Abdel-Aleem MA. Uterine massage for preventing postpartum
haemorrhage. Cochrane Database of Systematic Reviews 2008, Issue 3. Art. No.: CD006431. DOI: 10.1002/14651858.CD006431.pub2. [online] available from http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD006431.pub2/pdf
11. Gülmezoglu AM, Forna F, Villar J, Hofmeyr GJ. Prostaglandins for preventing postpartum
haemorrhage. Cochrane Database of Systematic Reviews 2007, Issue 3. Art. No.: CD000494. DOI: 10.1002/14651858.CD000494.pub3. [online] available from http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD000494.pub3/pdf
Bibliography 12. Royal College of Obstetricians and Gynaecologists. Antepartum Haemorrhage. Green Top Guideline
63. 2011. London: RCOG Press. [online] available from http://www.rcog.org.uk/files/rcog-corp/GTG63_05122011APH.pdf
17
13. National Institute for Health & Clinical Excellence. Intrapartum care: management and delivery of care to women in labour. NICE Clinical Guideline CG55 September 2007 (currently under review 2011) London: NICE. [online] available from http://www.nice.org.uk/nicemedia/pdf/IPCNICEGuidance.pdf
14. Royal College of Obstetricians and Gynaecologists, Royal College of Anaesthetists, Royal College of
Midwives, Royal College of Paediatrics and Child Health. Standards for Maternity Care: Report of a Working Party. 2008 London: RCOG Press. [online] available from http://www.rcog.org.uk/files/rcog-corp/uploaded-files/WPRMaternityStandards2008.pdf
15. Association of Anaesthetists of Great Britain and Ireland. AAGBI Safety Guideline. Blood
Transfusion and the Anaesthetist: Management of Massive Haemorrhage. Anaesthesia 2010; 65: 1153-1161 [online] available from http://www.aagbi.org/sites/default/files/massive_haemorrhage_2010_0.pdf
16. Association of Anaesthetists of Great Britain and Ireland. Blood Transfusion and the Anaesthetist
Intra-operative Cell Salvage. 2009. London: AAGBI. [online] available from http://www.aagbi.org/sites/default/files/cell%20_salvage_2009_amended.pdf
Further reading 17. British Committee for Standards in Haematology. Guidelines on the management of massive blood
loss. British Journal of Haematology, 2006, 135, 634–641 [online] available from http://www.bcshguidelines.com/documents/massive_bloodloss_bjh_2006.pdf
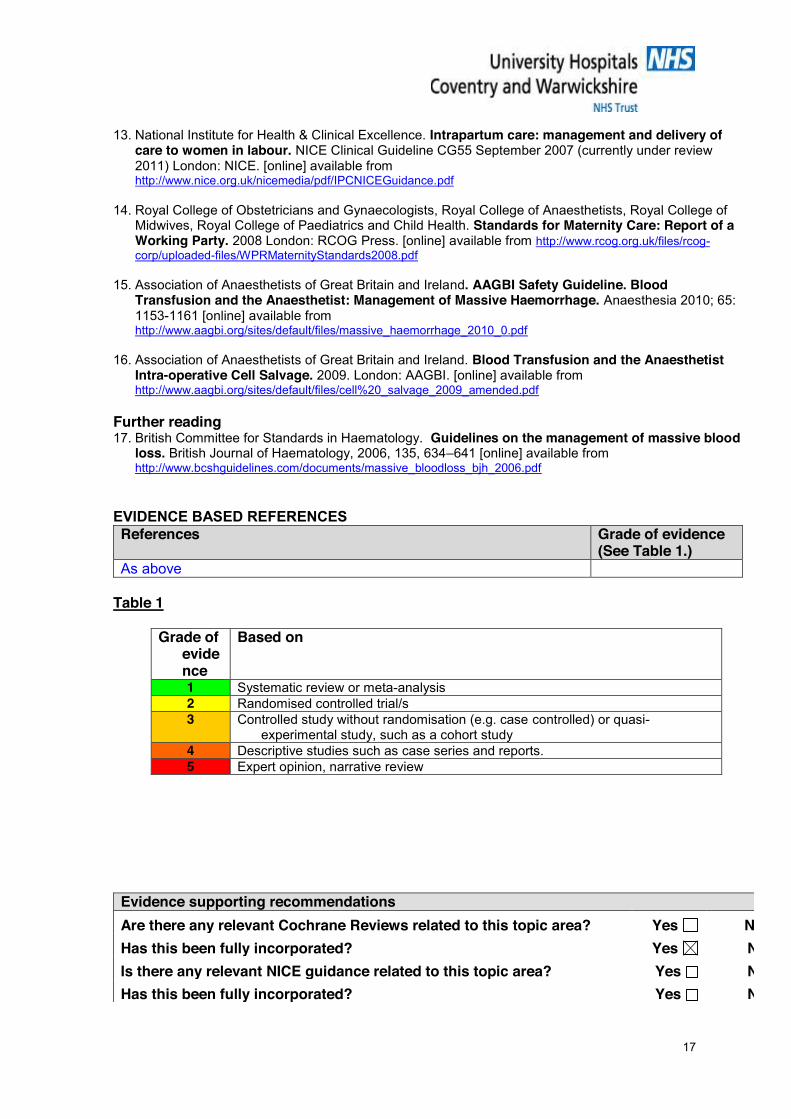
EVIDENCE BASED REFERENCES References
Grade of evidence (See Table 1.)
As above Table 1
Grade of evidence
Based on
1 Systematic review or meta-analysis 2 Randomised controlled trial/s 3 Controlled study without randomisation (e.g. case controlled) or quasi-
experimental study, such as a cohort study 4 Descriptive studies such as case series and reports. 5 Expert opinion, narrative review
Evidence supporting recommendations Are there any relevant Cochrane Reviews related to this topic area? Yes No Has this been fully incorporated? Yes No Is there any relevant NICE guidance related to this topic area? Yes No Has this been fully incorporated? Yes No

18
Is there any relevant RCOG guidance related to this topic area? Yes No Has this been fully incorporated? Yes No Is there any relevant RCM guidance literature related to this topic area? Yes No Has this been fully incorporated? Yes No Is there any other relevant national guidance related to this topic area? Yes No
Has this been fully incorporated? Yes No
19