Embed Size (px)
Citation preview

C
Pe
BS
a
AA
KOPTS
1
flSefi1ha2arm
eafii
isgf
1d
Joint Bone Spine 77 (2010) 78–80
ase report
osttraumatic psoriatic osteitis of the frontal bone successfully treated withtanercept. Report of a case
ernard Fournié ∗, Laurent Zabraniecki , Olivia Lemaire , Marie-Anne Plaut-Gaty , Elsa Poix-Joverervice de clinique de rhumatologie, CHU Purpan, place Baylac, TSA 40070, 31059 Toulouse cedex 9, France
r t i c l e i n f o
rticle history:
a b s t r a c t
We report a case of aseptic osteomyelitis of the frontal bone that developed after a local injury in an
ccepted 16 May 2009eywords:steitissoriasisrauma
8-year-old girl with psoriasis of the scalp as a predisposing factor. Follow-up was 36 years (1972 to2008). Enthesitis of the forehead muscles was a plausible pathophysiological mechanism. The symptomsresponded to anti-inflammatory medications and resolved immediately after the introduction of etan-ercept therapy. The most interesting feature of this case of psoriatic osteomyelitis is the involvement ofa skull bone.
ncais
kull © 2009 Société fra. Case report
The patient was 8 years old in 1972 when she was struck withull force by a ball on the left side of the forehead. She was in excel-ent health except for psoriasis of the scalp since early childhood.he had a family history of psoriasis (mother, sister, and broth-rs). After the head injury, she reported continuous pain in the leftrontal region with exacerbations marked by blepharitis and tear-ng of the left eye. She was in good general health, with no fever. In985, exophthalmos of the left eye developed gradually, as well asypertrophy of the lachrymal gland. The entire gland was removednd the histological study showed no evidence of malignancy. In007, she experienced a flare of palmoplantar pustular psoriasisnd in 2008 an episode of nongranulomatous anterior uveitis of theight eye. Over the 36 years since symptom onset, no other clinicalanifestations were recorded at any of the evaluations.The only meaningful laboratory test abnormality was repeated
levation of the erythrocyte sedimentation rate, which fluctu-ted between 20 and 50 mm/h. Findings were normal or negativerom the blood cell counts, platelet counts, serum protein stud-es, phosphate and calcium assays, standard biochemical tests, andmmunological tests.
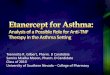
A radionuclide bone scan performed in 1976 (Fig. 1a) showed
ncreased uptake by the lower part of the left frontal bone. No hotpots were seen at any other skeletal sites. Sequential skull radio-raphs obtained starting in 1975 (Fig. 2) showed early osteolysisollowed by sclerosis of the left frontal bone: osteolysis was visible∗ Corresponding author. Tel.: +33 561 772 304; fax: +33 561 772 208.E-mail address: [email protected] (B. Fournié).
297-319X/$ – see front matter © 2009 Société francaise de rhumatologie. Published by Eoi:10.1016/j.jbspin.2009.11.006
e de rhumatologie. Published by Elsevier Masson SAS. All rights reserved.
initially in the lower part of the bone then spread gradually towardthe upper frontal bone and was finally replaced by hypertrophicsclerosis. Computed tomography of the brain performed in 1978showed no intracranial abnormalities. Two bone biopsies wereperformed, in 1975 and 1978, respectively; the results ruled outseptic osteitis (results were negative from microbiological studiesand tests for infection), osteosarcoma, and benign bone disease ofthe skull. Reactive bone marrow changes and marked blood vesseldilation were noted. There were no other remarkable histologicalfeatures.
Between 1975 and 1985, she was given a number of antimicro-bial agents (cyclines, penicillins, aminoglycosides, cephalosporins,and synergistins), to no avail. Nonsteroidal anti-inflammatorydrugs (tiaprofenic acid, ibuprofen, and flurbiprofen) produced someimprovement and were given in combination with acetaminophen.Prednisone was used as needed during the exacerbations.
When we first evaluated this patient in 2008, the clinical man-ifestations were unchanged, although the exacerbations were lessfrequent (about one per month), briefer (4–5 days), and less severethan previously. Both the frequency and the severity of the exac-erbations tended to increase in the winter. Irritation of the lefteye was a consistent feature. The exophthalmos of the left eyewas unchanged compared to 1985 when this manifestation firstdeveloped. A slight bulge was noted above the left orbit (Fig. 3a).There was no deformity of the forehead, which was neither warmnor tender to palpation. No evidence of psoriasis was found andthe patient reported spontaneous resolution of the psoriatic scalp
lesions 7 years earlier.Laboratory tests showed the following results: erythrocytesedimentation rate, 33 mm/h; C-reactive protein, 5 mg/L (N < 5);normal blood cell counts; �2 globulin, 9.2 g/L (N = 5–8); calcium,
lsevier Masson SAS. All rights reserved.

B. Fournié et al. / Joint Bone Spine 77 (2010) 78–80 79
Fuu
22aac
sgosote
(400 mg tid), to which she added acetaminophen (500 mg every4 h) during minor exacerbations and prednisone (40 mg/day) dur-ing major exacerbations. Despite this regimen, the pain remainedincapacitating. Etanercept was therefore started, in a dosage of
ig. 1. Radionuclide bone scans of the skull (lateral views); (a) 1976: increasedptake in the lower part of the left frontal bone; (b) 2008: increased uptake in thepper part of the left frontal bone.
.44 mmol/L; phosphate, 1.27 mmol/L; alkaline phosphatase,10 IU/L (N = 100–280); IgA, 4.16 g/L (N = 0.86–2.74); normal IgGnd IgM levels; and nonsignificant titers of rheumatoid factors,nti-CCP antibodies, antinuclear antibodies, and antineutrophilytoplasmic antibodies. Her HLA genotype was A2 A23 B7 B14.
Radiographs of the skull demonstrated regular hypertrophy andclerosis of the entire left frontal bone (Fig. 2d), whose orbital mar-in was thickened (Fig. 3b). Findings were normal from radiographs
f the spine, pelvis, hands, feet, and chest. A radionuclide bonecan showed a single focus of increased uptake in the upper partf the left frontal bone (Fig. 1b). By magnetic resonance imaging,he diploe of the left frontal bone was seen to be markedly thick-ned, whereas the inner and outer tables were normal. GadoliniumFig. 2. Radiographs of the skull (left lateral views); (a) 1975: spotty osteolysis in thelower frontal bone; (b) 1978: spotty osteolysis in the upper frontal bone; (c) 1980:sclerotic hypertrophy in the lower frontal bone; (d) 2008: sclerotic hypertrophy inthe entire frontal bone.
injection was not followed by enhancement of the bone or adjacenttissues. No focal brain lesions were visible and the ventricular sys-tem was normal in size and position. Investigations to evaluate theleft exophthalmos found no intraorbital space-occupying lesion oroculomotor muscle alterations (Fig. 3c).
The patient had been taking the same treatment since1985, namely, the nonsteroidal anti-inflammatory drug ibuprofen
Fig. 3. Exophthalmos (2008); (a) clinical appearance: moderate exophthalmos onthe left with a slight supraorbital bulge; (b) radiograph: hypertrophy of the leftorbital margin, which narrows the orbital cavity; (c) magnetic resonance imaging: nospace-occupying lesion within the left orbital cavity or alterations of the oculomotormuscles.

8 Bone S
5t
2
alcssbaa1wtt
rdwoc[ealaAhsfoltie(
loonini
re
[
[
[
0 B. Fournié et al. / Joint
0 mg/week. She responded immediately to this drug and was ableo stop her usual symptomatic regimen.
. Discussion
The 36-year follow-up in our patient ruled out a malignancy,nd the imaging studies showed no evidence of an intracranialesion (e.g., meningioma). The clinical, laboratory, and histologi-al features were not suggestive of a benign bone disease of thekull (e.g., Paget’s disease, fibrous dysplasia, or frontal hyperosto-is). The most likely diagnosis was therefore osteitis of the frontalone. Septic osteitis was considered initially. However, the neg-tive tests for infection, negative biopsy specimen cultures, andbsence of a response to a variety of antimicrobials taken over a0-year period argued against septic osteitis. Aseptic osteomyelitisas a more likely diagnosis given the history of psoriasis, inciting
rauma, and good response to anti-inflammatory agents includinghe TNF antagonist etanercept.
Aseptic osteomyelitis is a well-recognized complication of pso-iasis that occurs chiefly in the palmoplantar pustular form of theisease [1]. Palmoplantar pustular psoriasis shows some overlapith psoriatic arthritis and with SAPHO syndrome [2]. Aseptic
steomyelitis chiefly targets the femur [3], pelvis [4,5], anteriorhest wall [6,7], and vertebras [8], and also probably the mandible9]. The course is obdurately chronic, with severe painful exac-rbations that respond variably to anti-inflammatory agents andnalgesics. Erythrocyte sedimentation rate elevation is the onlyaboratory test abnormality. Radiographs show osteolysis initiallynd a combination of hypertrophy and sclerosis later on (Fig. 2).
periosteal reaction may be visible. Bone scanning reveals aot spot. Imaging study findings and examination of a biopsypecimen show no evidence of malignancy or infection. Theseeatures of aseptic osteomyelitis match the clinical picture inur patient. The only unusual characteristic was the site of theesion in the frontal bone. The frontal bone contributes to formhe orbit (orbital margin and orbital cavity). The close proxim-ty of the bone inflammation and hypertrophy with the eye mayxplain the blepharitis, tearing, and exophthalmos in our patientFig. 3).
Trauma is an accepted inciting cause of inflammatory muscu-oskeletal lesions, particularly when the lesion develops at the sitef the injury [10,11]. In our patient, the bone lesion arose at the sitef a head injury. During the 36 years of follow-up, she experiencedo other osteoarticular manifestations of psoriasis. This isolated
nvolvement of the frontal bone may be ascribable to the combi-
ation of psoriasis of the scalp (predisposing factor) and of a headnjury (precipitating factor).Although most authors believe that osteomyelitis related to pso-
iasis reflects infection by Propionibacterium acnes, we suggest thatnthesitis may be the underlying mechanism. The inflammation at
[
[
pine 77 (2010) 78–80
the site of the affected enthesis may spread to the bone marrow[12,13].
At the skull, the fascia of the muscles of the head and face mergewith the galea aponeurotica, which is a vast layer of fibrous tissuethat covers the upper part of the skull and supplies each mus-cle with a complete sheath. At the frontal bone, the entheses arelocated along a transverse line that runs along the upper orbitalrims and glabella [14]. In our patient, the bone lesions started inthe lower part of the frontal bone then gradually spread upward(Figs. 1 and 2). This pattern is consistent with aseptic osteomyelitistriggered by forehead muscle enthesitis. Fusion of the two halvesof the frontal bone at the metopic suture starts during the secondyear of life and is complete at 8 years of age. Separate foreheadmuscles and entheses exist for the two sides of the forehead [14].The occurrence of the trauma at a young age (8 years) may explainthat the bone lesions remained confined to the half of the frontalbone located on the side of the injury.
We believe that forehead muscle enthesitis in response to a localinjury in a patient with a predisposing conditions (psoriasis of thescalp) explains the development of aseptic osteitis of the frontalbone in our patient. If our hypothesis is correct, then our case is thefirst reported instance of psoriatic osteomyelitis of a skull bone.
References
[1] Fournié B. Rhumatisme psoriasique. EMC (Elsevier Masson SAS, Paris). Appareillocomoteur, 14-246.A.10; 2007.
[2] Kahn MF. Frontières et confins du rhumatisme psoriasique. Rev Rhum (Ed Fr)2002;69:682–4.
[3] Fournié A, Bouvier M, Fournié B, et al. Hyperostose-ostéite-périostite, tri-ade radiologique des enthésopathies. Remarques à propos de 2 localisationsfémorales inhabituelles. Rev Rhum 1989;56:763–6.
[4] Belzunegui J, Onatibia A, Cancio J, et al. Aseptic osteomyelitis of the ilium in thepalmoplantar pustulosis. Clin Rheumatol 1995;14:382.
[5] Jurik AG, Helmig O, Graudal H. Skeletal disease, arthro-osteitis, in adult patientswith pustulosis palmoplantaris. Scand J Rheumatol 1988;70(Suppl.):3–15.
[6] Helliwell P. Anterior chest wall involvement in psoriatic arthritis. Rev Rhum(Eng Ed) 1997;64:436.
[7] Fournié B, Boutes A, Dromer C, et al. Étude prospective de l’atteinte du plas-tron sterno-costo-claviculaire dans la spondylarthrite ankylosante et dans lerhumatisme psoriasique. Rev Rhum (Ed Fr) 1997;64:23–6.
[8] Kotilainen P, Gullichsen RE, Saario R, et al. Aseptic spondylitis as the initialmanifestation of the SAPHO syndrome. Eur Spine J 1997;6:327–9.
[9] Kahn MF, Hayem F, Hayem G, et al. Is diffuse sclerosing osteomyelitis of themandible, part of the synovitis, acne, pustulosis, hyperostosis, osteitis (SAPHO)syndrome? Oral Surg Oral Med Oral Pathol 1994;78:594–8.
10] Punzi L, Pianon M, Rizzi E. Prévalence du rhumatisme psoriasique post-traumatique [lettre]. Presse Med 1997;26:420.
11] Sandorfi N, Freundlich B. Psoriatic and seronegative inflammatory arthropa-thy associated with a traumatic onset: 4 cases and review of the literature. JRheumatol 1997;24:187–92.
12] Fournié B. Le territoire enthésique et le syndrome d’hyperostose-ostéite-
périostite (HOP). Une approche nosologique radioclinique des spondy-larthropathies inflammatoires. Rev Rhum (Ed Fr) 1993;60:485–8.13] Fournié B. Anatomopathologie et anatomoclinique des spondylarthrites. RevRhum (Ed Fr) 2004;71:1130–5.
14] Poirier P, Charpy A, Nicolas A. Traité d’anatomie humaine, Ostéologie. Tome 1.Paris: Masson et Cie Ed; 1911.