Embed Size (px)
Citation preview

8/10/2019 Presentation Gastroparesis
http://slidepdf.com/reader/full/presentation-gastroparesis 1/14
Bronx VA Longitudinal Clerkship 2014
Treatment of RefractoryGastroparesisSunjay Barton MS3

8/10/2019 Presentation Gastroparesis
http://slidepdf.com/reader/full/presentation-gastroparesis 2/14
Bronx VA Longitudinal Clerkship 2014
Case
• 49-year-old man with history of poorly controlleddiabetes and multiple hospitalizations for acute
exacerbations of gastroparesis
• Diagnosed with gastric scintigraphy, wireless
motility capsule
• Recurrent nausea, vomiting, severe crampy
abdominal pain

8/10/2019 Presentation Gastroparesis
http://slidepdf.com/reader/full/presentation-gastroparesis 3/14
Bronx VA Longitudinal Clerkship 2014
Failed medical treatments: diet modification
• Avoid fat (slows gastric emptying) and insolublefiber
• Small, frequent meals
• Blend food (liquid = rapid transit)
• Avoid alcohol/smoking (decreases motility)
• Optimize glycemic control

8/10/2019 Presentation Gastroparesis
http://slidepdf.com/reader/full/presentation-gastroparesis 4/14
Failed medical treatments: metoclopramide
• Patient developed legtwitching concerning
for extrapyramidal
symptoms vs tardive
dyskinesia
Bronx VA Longitudinal Clerkship 2014

8/10/2019 Presentation Gastroparesis
http://slidepdf.com/reader/full/presentation-gastroparesis 5/14
Bronx VA Longitudinal Clerkship 2014
Failed medical treatments: erythromycin
• Patient developed side effects of muscleweakness and blurred vision
• Patient discontinued medication after one week
• Interaction with statins (rhabdomyolysis, AKI)

8/10/2019 Presentation Gastroparesis
http://slidepdf.com/reader/full/presentation-gastroparesis 6/14
Bronx VA Longitudinal Clerkship 2014
Additional medical treatment options
• Domperidone (D2 antagonist; difficult to obtain inUS)
• Azithromycin
• Cisapride (5HT4 agonist; difficult to obtain in US)
• Anti-emetics: diphenhydramine, ondansetron,
prochlorperazine, TCAs
• Scopolamine, aprepitant, dronabinol have beenused, but no evidence for effectiveness

8/10/2019 Presentation Gastroparesis
http://slidepdf.com/reader/full/presentation-gastroparesis 7/14
Bronx VA Longitudinal Clerkship 2014
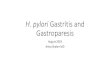
Previous surgical treatment: Botox pyloroplasty
• Temporarily relieved patient’s symptoms • No benefit in RCTs
• Not recommended in American College of
Gastroenterology guidelines for management ofgastroparesis [1]

8/10/2019 Presentation Gastroparesis
http://slidepdf.com/reader/full/presentation-gastroparesis 8/14

8/10/2019 Presentation Gastroparesis
http://slidepdf.com/reader/full/presentation-gastroparesis 9/14
Bronx VA Longitudinal Clerkship 2014
Additional treatments: G tube / J tube
• Gastrostomy tube placement for decompression• Jejunostomy tube placement for feeding in patients
with significant weight loss
• G tube +/- J tube reduced number ofhospitalizations 5-fold in prospective trial of 22
patients [3]

8/10/2019 Presentation Gastroparesis
http://slidepdf.com/reader/full/presentation-gastroparesis 10/14
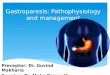
Gastric electrical stimulation: hardware
• Battery pack implantedin abdominal wall
• Electrodes deliver low
energy electrical
stimulation to stomach
at 12 cycles per
minute
• Physiologicoscillations are 3 cpm
Bronx VA Longitudinal Clerkship 2014

8/10/2019 Presentation Gastroparesis
http://slidepdf.com/reader/full/presentation-gastroparesis 11/14
Bronx VA Longitudinal Clerkship 2014
Gastric electrical stimulation: evidence
• Humanitarian device exemption for refractorydiabetic or idiopathic gastroparesis
• Double-blind, randomized crossover study of 33
patients in 2003 demonstrated reduction of weekly
vomiting frequency and improvement in quality of
life [4]
• Significant improvement seen in diabetic subgroup
as well as whole cohort

8/10/2019 Presentation Gastroparesis
http://slidepdf.com/reader/full/presentation-gastroparesis 12/14
Bronx VA Longitudinal Clerkship 2014
Gastric electrical stimulation: mechanism
• Unclear• No effect on gastric emptying
• Increases maximal tolerated gastric distention
• Research continues on devices that deliver
physiologic low frequency gastric pacing, currently
too large for implantation

8/10/2019 Presentation Gastroparesis
http://slidepdf.com/reader/full/presentation-gastroparesis 13/14
Summary
Bronx VA Longitudinal Clerkship 2014

8/10/2019 Presentation Gastroparesis
http://slidepdf.com/reader/full/presentation-gastroparesis 14/14
Bronx VA Longitudinal Clerkship 2014
Sources
1. Camilleri M, Parkman HP, Shafi MA, Abell TL, Gerson L. Clinical
guideline: management of gastroparesis. The American journal ofgastroenterology. 2013;108:18-37.
2. Hibbard ML, Dunst CM, Swanstrom LL. Laparoscopic and
endoscopic pyloroplasty for gastroparesis results in sustained symptom
improvement. Journal of gastrointestinal surgery: official journal of the
Society for Surgery of the Alimentary Tract. 2011;15:1513-9.
3. Borrazzo EC. Surgical management of gastroparesis:
gastrostomy/jejunostomy tubes, gastrectomy, pyloroplasty, gastric electrical
stimulation. Journal of gastrointestinal surgery: official journal of the Society
for Surgery of the Alimentary Tract. 2013;17:1559-61.4. Abell T, McCallum R, Hocking M, et al. Gastric electrical stimulation
for medically refractory gastroparesis. Gastroenterology. 2003;125:421-8.