Embed Size (px)
Citation preview

1
Stroke IThe first 72 hours…
Michael R. Dobbs, M.D.Medical Director, Stroke Care
University of Kentucky Chandler Medical Center
Presenter Disclosure Information
Michael R. Dobbs, MDStroke: the first 72 hours
FINANCIAL DISCLOSURE:FINANCIAL DISCLOSURE:Speaking and teaching: Bristol-Myers-Squibb/Sanofi, Allergan
UNLABELED/UNAPPROVED USES DISCLOSURE:Intra-arterial tpa and most treatments for brain edema are investigational
The Stroke Pandemic
MHW = Ministry of Health, Labour and Welfare; WHO, Japanese MHW, Mattson Jack, American Heart Association; Available at: www.who.int. Accessed Sept. 11, 2006
Epidemiology
Stroke in the US
– 780,000 new or recurrent strokes each year
– 3rd leading cause of death
– 5 500 000 stroke survivors alive today5,500,000 stroke survivors alive today
– Leading cause of disability
What happens to a patient after a major stroke?
• Acute hospitalization
• Prolonged rehabilitation hospital stayg p y
• Neurological impairment that is permanent
• Disability
• Decreased quality of life
Impact of Stroke in the United States
• Stroke Survivors
– Return to normal 10%
– Hemiparetic 48%
– Unable to walk 22%
– Complete or partial
dependence 24‐53%
– Aphasic 12‐18%
– Clinically depressed 32%
Source: National Stroke Association. The Stroke/Brain Attack Report’s Handbook, 1997, p. 44.Source: National Stroke Association. The Stroke/Brain Attack Report’s Handbook, 1997, p. 44.US Department of Health & Human Services. PostUS Department of Health & Human Services. Post--Stroke Rehabilitation: Practical Clinical GuidelinesStroke Rehabilitation: Practical Clinical Guidelines..

2
Prevalence of Stroke by Age
6
8
10
12
14
po
pu
lati
on
MenWomen
American Heart Association. Heart Disease and Stroke Statistics—2003 Update.
0
2
4
6
20-24 25-34 35-44 45-54 55-64 65-74 75+
Age range (years)
% o
f p
Source: Unpublished data from NHANES III (1988-1994), CDC/NCHS.
UKMC Stroke Patient Demographics
165
188
176
101
120
140
160
180
200
ES
Median Age 64
8
4 2 5
38
85
101
17
0
20
40
60
80
100
0‐9 10‐19 20‐29 30‐39 40‐49 50‐59 60‐69 70‐79 80‐89 90‐100
CASE
AGE GROUP (YEARS)
Defining the Mechanism of a TIA or Cerebral Infarction: Four Major
Categories 1. Cardiac– Arrythmias
– Venous source with right‐to‐left shunt
– Intracardiac thrombus
– Cardiac mass lesions
– Valve disease
2. Large vessel disease– Atherosclerosis
– Dissection, fibromuscular dysplasia 1
2
Defining the Mechanism of a TIA or Cerebral Infarction: Four Major
Categories (cont’d)3. Small vessel disease
– Atherosclerosis, hypertension, smoking, diabetes
– Infectioni f i i i
34
– Non‐infectious arteritis
4. Hematologic – Lupus anticoagulant positivity, anticardiolipin antibodies, antiphospholipid antibodies
– Polycythemia, thrombocytosis, sickle cell disease
– Oral contraceptives
Cerebrovascular Disease:Pathogenesis
Ischemic Stroke (85%)Hemorrhagic Stroke (15%)
AtheroscleroticCerebrovascular
Cryptogenic (25%)IntracerebralHemorrhage (59%)
?
CerebrovascularDisease (25%)
Embolism (25%)Lacunar (25%)
SubarachnoidHemorrhage (41%)
Albers GW et al. Chest. 1998;114:683S-698S.Rosamond WD et al. Stroke. 1999;30:736-743.
TIA or Stroke
• True TIA are brief attacks lasting a few minutes‐hours
• Longer Attacks up to 24 hours with resolution of clinical symptoms are often ischemic strokeof clinical symptoms are often ischemic stroke
• MRI demonstrates abnormalities in 50‐70% cases

3
Event Risk Within 3 MonthsAfter TIA
12.7%
10.5% • Age > 60 years
• Diabetes mellitus
• Duration of episode greater than 10 min
• Weakness
Independent risk factors for stroke within 90 days after TIA:
Johnston SC, et al. JAMA. 2000;284:2901-2906.
RecurrentTIA
Cardiac Event
Stroke Death
2.6% 2.6%5% in
48 h
• Weakness
• Language impairment with the episode
Acute Care of Stroke PatientsStroke Patients
General Considerations
• Airway and breathing should be maintained.
• Supplemental Oxygen should be provided to keep O2 saturation at 92% or above.
• Fever is harmful in acute stroke. Ascertaining and addressing the cause, while lowering elevated temperature, is strongly advised.
• Pneumatic compression devices (or pharmacologic means) should be applied to help prevent deep venous thromboses.
• Avoid any and all oral intake until a swallowing is clearly unimpaired.
– This helps to avoid aspiration pneumonia.
• DON’T DROP BP UNLESS ABSOLUTELY NECESSARY
• Consider neurosurgical intervention for craniectomy in select cases.
– Typical cases where craniectomy might be performed would include a) cerebellar ischemia with compression of brainstem or 4th ventricle, and b) large right middle cerebral artery ischemia.
Intravenous thrombolysis
• IV‐tpa is the only medical therapy which is FDA‐approved for treatment of ischemic stroke.
• The time window is within 3 hours of symptom onset.
• There are strict criteria for administration of IV‐tpap
• The protocol is weight‐based with 90mg being the maximum dose.
• Some new data suggest that IV‐tpa can be administered safely and with benefit in select patients up to 4.5 hours from symptom onset. There are additional exclusion criteria if IV‐tpa is given beyond the 3 hour window.

4
Overall Benefits and Risks of IV tPA for Stroke
• Benefit: neurologically normal at 3 months
– 55% relative increase– 12% absolute increase
Ver rob st effect NNT 8• Very robust effect: NNT = 8
• Risk of symptomatic ICH was 6.4%
• The overall benefits include the ICHs
• Risk of ICH can be reduced by closely following the tPA protocol
NINDS rt-PA Stroke Study Group. N Engl J Med. 1995;333:1581-1587. Guidelines in Adams HP Jr, et al. Stroke. 2003;34:1056-1083.
Efficacy of tPA by Stroke Subtype
50
60
70
80
d o
utc
om
e
tPA
Placebo
0
10
20
30
40
% w
ith
go
od
Small vessel Large vessel Cardioembolic
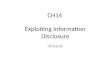
Time Is Brain: Effects of tPA vs Time
8
7
6
5
4or
favo
rab
le
t 3
mo
nth
s
60 70 80 90 100 110 120 130 140 150 160 170 180
4
3
2
1
0
Benefit for rt-PANo benefit for rt-PA
Minutes from stroke onset to start of treatment
Od
ds
rati
o f
oo
utc
om
eat
μ
Using tPA in Routine Clinical Practice
• Overall only about 3%‐4% of stroke patients receive tPA—mostly due to time delays
• Efficacy similar to NINDS trial
• Rate of ICH: 4%‐6%
Ri k f ICH i ith t l i l ti• Risk of ICH increases with protocol violations– Poor blood pressure control– Using prohibited agents– Wrong dose
• 0.9 mg/kg• Maximum dose: 90 mg
– Elevated blood sugar also increases risk
IV‐tPA at 4 and ½ hours—2010
Additional warnings for patients treated between 3‐ 4.5 hours
– Age > 80
– History of prior stroke AND diabetesy p
– Any anticoagulant use prior to admission (even if INR <1.7)
– NIHSS >25
– CT findings involving more than 1/3 of the MCA territory (as evidenced byhypodensity, sulcal effacement or mass effect estimated by visual inspection orABC/2>100 cc)
Key Elements of a Primary Stroke Center
• Director
• Stroke team 24/7
• Stroke unit
• Care mapsp
• Rapid CT and lab testing
• Neurosurgery within 2 hours
• Track outcomes
• Education – public and private

5
Mechanical Clot Disruption
• PT Angioplasty +/‐ stent
• Endovascular Thrombectomy– Merci clot retrieval device
• 43% complete recanalization
• 21% more when intraarterial rt‐PA added%
– Merci2: 150 patients 53.3 recanalization with embolectomy
– SICH 7.8%
– Improved outcome in recanalized patients
• Penumbra device
*
IA Reperfusion Therapy
• IA tpa is an option for selected, severe patients < 6 h or < 3 not candidates for IV tPA (Class I; B)
• Treatment requires SC and qualified INR (Class I; C)C)
• Contraindications for IV tPA (surgery) Class IIa; C)
• Should not preclude IV tPA (Class III; C)
• 68 y/o female with history of peripheral vascular disease, hypertension, and atrial fibrillation.
• While watching TV with husband, patient began having a left facial droop and left sided weakness. Her husband noticed this and called 911.
• Patient presented to ER with left‐sided weakness, left facial droop, and no movement of left upper extremity, Neurologic exam also revealed right gaze deviation; the patient could not move her eyes past midline.
• Pre NIHSS = 13• A non‐contrast CT of the brain was obtained on arrival at the ER and it
identified a dense right middle cerebral artery sign, without significant loss of gray matter differentiation an indication that this patient was angray‐matter differentiation an indication that this patient was an interventional candidate.
• She was not a candidate for IV tPA because she was on Coumadin with INR>1.7.
• Angiography revealed a complete occlusion of the right M1 middle cerebral artery and the distal branches.

6
• Immediately after the procedure, the patient was identified to have increased movement of the left lower and upper extremities.
• Patient didn’t qualify for acute rehab and is• Patient didn t qualify for acute rehab and is home doing well
• (outpt therapy)
Who is (really) a candidate?
• Ischemic stroke with significant deficit
• Large vessel occlusion– MCA trunk or main branch, ICA, basilar, vertebral, ACA or PCA origin
May want CTA– May want CTA
• Can be performed after IV‐tpa
• We don’t know how long the time window is– CT or MRI perfusion
– Typically thought of as 8hrs
Pearls and pitfalls—acute stroke intervention
• After IV‐tpa, risk of symptomatic ICH is about 5%
• BP guidelines might not apply if the vessels are open (a successful recanalization procedure)
• Risk of ICH with IA therapy is comparable to IVRisk of ICH with IA therapy is comparable to IV
• May see extravasation of contrast that mimics ICH, esp in the basal ganglia

7
Stroke Unit: The Ideal
• Acute stroke patients should be admitted to a stroke unit
• Tools in a stroke unit– Telemetry– Care maps– Experienced nurses– Prevent aspiration pneumonia, DVT, infection– Multidisciplinary team
• All TIA patients admitted if they present within 48 hours or have multiple TIAs
Stroke Unit Care • Meta‐analysis of 23 trials comparing organized stroke unit care
with general ward care
Outcome Odds P value ratio(Stroke Unit/Ward)
Death (1 year) 0.86 .005
Death or institutionalized care 0.8 .0002
Death or dependency 0.78 .0003
• No increase in length of stay
• Conclusion: Stroke unit care associated with lower odds of death or dependency
Stroke Unit Trialists’ Collaboration. Cochrane Database Syst Rev. 2002;(1):CD000197.
Results of Anticoagulation: Meta‐analysis
• No significant difference in 2‐week mortality (8.5% in AC group vs 8.7% in controls)
T l k3.50%
4.00%
4.50%
ICH Ischemic Stroke
• Total new strokes identical between 2 treatment groups: 4.1%
• No evidence of heterogeneity among various studies or agents 0.00%
0.50%
1.00%
1.50%
2.00%
2.50%
3.00%
No AC AC
Sandercock P, et al. Stroke. 1999;30:248.
Blood Pressure in Ischemic Stroke
Acute elevations of BP are common in stroke Seen in 85% of patients Often declines spontaneously in first
24‐48 hours
Cerebral autoregulation is defective in most strokeCerebral autoregulation is defective in most stroke patients
Acutely lowering BP can expand area of ischemia Supported by PET studies Supported by clinical experience Supported by ASA guidelines
BP Recommendations for Ischemic Stroke Patients Not Eligible for Thrombolysis
Systolic <220 or diastolic <120 Observe unless other end‐organ involvement
Systolic >220 or diastolic <121‐140 Labetalol 10‐20 mg IV over 1‐2 min (may repeat or g ( y p
double every 10 min); or Nicardipine
Aim for 10%‐15% reduction in BP
Diastolic >140 Nitroprusside
Adams HP Jr, et al. ASA Guidelines. Stroke. 2003;34:1056-1083.
BP Recommendations for Ischemic Stroke Patients Eligible for Thrombolysis
Before tPA treatment Systolic >185 or diastolic >110
– Labetalol
During and after tPA treatment Monitor BP Monitor BP Diastolic >140
– Nitroprusside Systolic >230 or diastolic 121‐140
– Labetalol or nicardipine Systolic 180‐230 or diastolic 105‐120
– Labetalol
Adams HP Jr, et al. ASA Guidelines. Stroke. 2003;34:1056-1083.

8
Ischemic Stroke• Cerebral autoregulation may be lost
• Chronic hypertensive patients are accustomed to higher BP— curve shifted to the right
• Patients may have concomitant cardiac disease
• Hypertension may resolve spontaneously1
– May be important to maintain adequate perfusion pressures
– Usually not treated unless:• SBP >220, DBP >120 or MAP >130 mmHg2
• Or concomitant medical conditions—acute MI, aortic dissection, hypertensive encephalopathy, severe LV failure
• Or if thrombolytic Rx to avoid hemorrhage
References: 1. Krieger D. The intensive care of the stroke patient. In: Barnett HJM. Stroke: Pathophysiology, Diagnosis, and Management. 3rd ed. Churchill Livingstone; 1998:1138. 2. Marx. Rosen's Emergency Medicine: Concepts and Clinical Practice. 5th ed. Mosby, Inc.; 2002:1440.
Hemorrhagic Stroke
• Cerebral autoregulation may be lost
• Hypertension may cause deterioration1:– Due to increased ICP
– Due to further bleeding
• Goal is controlled reduction of hypertension (SBP >160–180 orDBP >105)1
– If BP too low, risk of ischemia
– If BP too high, increased risk of hemorrhage
Reference: 1. Marx. Rosen's Emergency Medicine: Concepts and Clinical Practice.5th ed. Mosby, Inc.; 2002:1442.
Benefits of ASA in Acute Stroke
• Absolute reduction of 5 recurrent strokes (all types) per 1,000 treated
• Absolute reduction of 4 deaths (all causes) per 1 000 treated1,000 treated
• Overall benefit of 9‐10/1,000 fewer strokes and deaths using 100‐300 mg ASA started within 48 hours of acute stroke, continued for at least 2 weeks
IST Collaborative Group. Lancet. 1997;349:1569-1581. CAST Collaborative Group. Lancet. 1997;349:1641-1649.
Other Keys in Acute Stroke
• Hypoglycemia: hypoglycemia can mimic stroke. Prompt assessment of serum [glucose] and replacement as necessary is important.
• Hyperglycemia: the presence of hyperglycemia worsens ischemic stroke outcome. Hyperglycemia should be managed aggressively.
• Hypotension: the presence of systemic hypotension in acute ischemic stroke portends a poor outcome. The cause should be sought, and volume depletion should be corrected with normal saline. Cardiac arrhythmias should be treated. Induced hypertension with vasopressor agents may be useful in select cases with an ischemic penumbra at risk, but caution is strongly advised.
Acute Therapy: Conclusions
• Acute therapy of stroke patients requires a coordinated and focused approach
• IV tPA within 3 hours is a safe and effective therapy if the protocol is carefully followedtherapy if the protocol is carefully followed
• The workup should determine the cause and mechanism of the stroke
• Steps to prevent peri‐stroke complications can improve outcomes
Goals of the Workup• Stabilize patient/reverse stroke
– tPA, unit care
• Prevent peri‐stroke complications– DVT pneumonia cerebral edemaDVT, pneumonia, cerebral edema
• Determine location of stroke
• Define mechanism of stroke
• Take steps for secondary prevention

9
Evaluation of Stroke
• Blood• Blood
• Brain parenchyma
• Vascular system
Evaluation of Brain Parenchyma
MRI
CT
Blood Tests—general
• CBC
• Sedimentation rate
• Blood chemistries
• Blood sugar
• Hb A1c
• PT, PTT
• Lipids (total cholesterol, LDL, HDL, triglycerides)
Blood Tests—specific
• FACTOR V LEIDEN
• LUPUS ANTICOAGULANT
• ANTICARDIOLIPIN PANEL
• ANTI THROMBIN III ACTIVITY
• PROTEIN S ACTIVITY
• ACTIVATED PROTEIN C RESISTANCE
• PROTHROMBIN G20210A MUTATION
Evaluation of the Vascular System
Penetrating arterydisease
Flow-reducingCarotid plaque with
Intracranialatherosclerosis
Albers GW, et al. Chest. 1998;114:683S-698S.
carotid stenosis
Atrial fibrillation
Valve disease
Left ventricularthrombi
Cardiogenicemboli
Aortic archplaque
arteriogenic emboli
Vascular Tests
Noninvasive MR angiography (MRA)
Intracranial, extracranial
CT angiography (CTA)Intracranial, extracranial
Carotid ultrasound
Invasive Conventional cerebral
angiography Risks (should be <1% risk of stroke or
death)
Measurement of lesions

10
Heart Tests
• ECG
• EchocardiographyEchocardiography–TTE–TEE
• Holter monitor
Aortic Arch
Transesophageal echocardiography
TEE in Stroke WorkupTEE in 824 patients with strokes
LA thrombus in 7%
Complex aortic plaque in 13%
Septal abnormalities in 15%
These lesions are often missed on TTE These lesions are often missed on TTE
Recommendations
OK to start with TTE in patients with cardiac disease
If patient is young and has no cardiac disease, consider TEE first
Leung DY, et al. Stroke. 1995;26:1820-1824. Rauh R, et al. Stroke. 1996;27:691-694.
Cardioembolic Sources: Risk Stratification
Major risk sources Atrial fibrillation
Mitral stenosis
Prosthetic valves
Minor risk sources Mitral valve prolapse
Mitral calcification
Patent foramen ovale Prosthetic valves
Recent MI
Left ventricular thrombus
Atrial myxoma
Dilating cardiomyopathies
Marantic endocarditis
Patent foramen ovale
Atrial septal aneurysm
Calcific aortic stenosis
Left ventricular regional wall motion abnormalities
Atrial Fibrillation in the US:Future Projections
5.615.425.164.784.34
3.84
5
6
Millions of adults with AF projected over time
3.332.94
2.662.442.262.08
0
1
2
3
4
1995 2000 2005 2010 2015 2020 2025 2030 2035 2040 2045 2050
Go AS, et al. JAMA. 2001;285:2370-2375.
Stroke Prevention in AF Meta‐analysis of 16 Randomized Trials
62% [48 72]29006Warfarin vs placebo
RRR [95% CI]
No. of patients
No. of trials
36% [14-52]28375Warfarin vs aspirin
22% [2-38]31196Aspirin vs placebo
62% [48-72]29006Warfarin vs placebo
Hart RG, et al. Ann Intern Med. 1999;131:492-501.

11
Warfarin for the Prevention of Cardioembolic Stroke
• Atrial fibrillation is the leading cause of cardiac embolism, responsible for 50% of cardiogenic emboli
• Oral anticoagulation is effective for primary and• Oral anticoagulation is effective for primary and secondary prevention of stroke in patients with atrial fibrillation
• Warfarin (INR of 2.5) is effective for the prevention of cardioembolic stroke in high risk patients
INR = international normalized ratio
Albers GW, et al. Chest. 2001;119:300S-320S.
AHA Recommendations for Patients With AF
Age
<65
65–75
Risk factors*
AbsentPresent
AbsentPresent
Treatment
AspirinWarfarin†
Aspirin or warfarinWarfarin†
>75
Present
Absent or present
Warfarin†
Warfarin†
*Hypertension, diabetes mellitus, poor left ventricular function, rheumatic mitral valve disease, prior TIA/stroke, systemic embolism or stroke, prosthetic heart valve (may require higher target INR).†Target INR = 2.5.
Goldstein LB, et al. Circulation. 2001;103:163-182.
Cardiac Catheterization
• Cerebral ischemic events: 0.1‐1.0 % of patients– Vertebrobasilar Circulation: 60‐70%
– Anterior Circulation: 30‐40%
• Presumed mechanism: Embolism ofPresumed mechanism: Embolism of atherosclerotic plaque from manipulation of the guide wire or clot released during catheter flushing
• Outcome generally favorable– Resolution of focal defects within 48 hrs
Percutaneous Transluminal Coronary Intervention
• Focal Ischemic Complications: 0.2 ‐ 0.3%
• Similar Sx and Mechanism as Cardiac Cath strokes
i id d difi i i• Lower incidence due to modifications in catheters and use of heparin and ASA
Acute MI and stroke
• 2.5% have stroke within 2 weeks
• More common with anterior wall than inferior
• Patients who keep low EF post MI have 8.1% k i kstroke risk over 5 years
• Warfarin plus ASA in MI survivors may decrease long‐term risk, but dramatically increases bleeding over ASA alone
Left ventricle thrombus
– LV thrombus in up to 40% of ant wall
– Within 2 weeks, coinciding with highest stroke risk
– Anticoagulate 3‐6 months (poor evidence)

12
fComplications of stroke
Acute (within 72hrs) complications of stroke
• cerebral edema
• increased ICP and possible herniation
• hemorrhagic transformation
• aspiration pneumonia• aspiration pneumonia
• seizures
• Post‐thrombolytic bleeding
– intracerebral hemorrhage
– Other potential sites of bleeding
Hemorrhagic infarction Complications Of Restoration of Blood Flow: Hemorrhage and Edema
• Arterial occlusion causes ischemia to capillaries, arterioles and vascular walls in addition to the deleterious effects on neuronsdeleterious effects on neurons
• Hemorrhage (red infarcts) result when the fragile “ischemic” or “injured” vessels rupture after sudden restoration of blood flow
• Vasogenic edema can also occur following a massive stroke or sudden restoration of blood flow to an ischemic area
Factors Associated With Red Infarcts (Hemorrhagic Transformation)
• Size of the infarct ‐ bigger infarcts have a higher chance of becoming hemorrhagic
• Richness of collateral circulation
• Use of anti‐coagulants
• Treatment with thrombolytic agents

13
Aspiration pneumonia
• Bacterial pneumonia causes 15‐25% of stroke‐related deaths
• High risk– Reduced consciousness
I i d ll i bl– Impaired gag or swallowing problems
• May assume aspiration if found unconscious, vomiting, or “down” for long time
• Broad antibiotic coverage
• May happen in subacute phase– NG feeding, frequent movement, pulmonary PT may help
Seizures
• May occur in acute phase
– Slightly more common in hemorrhages
• Focal or generalized
• May manifest as non‐convulsive delirium
• Standard therapies
• Some patients may benefit from continuous EEG monitoring
Post‐thrombolytic hemorrhage
• greatest concern is intracerebral hemorrhage,
– typically within the first 12 hours after treatment
– More likely if protocol not followed closely
• Other potential sites of bleedingp g
– GI tract
– genitourinary tract (associated with Foley catheters)
– Skin—typically at sites of intravenous lines
Subacute complications of stroke
• pneumonia
• deep venous thrombosis and pulmonary emboli
• urinary tract infections
• decubitus ulcers• decubitus ulcers
• contractures
• spasticity
• Malnutrition
• Depression
deep venous thrombosis and pulmonary emboli
• PE is a common cause of death in stroke patients– Tachypnea, chest pain, oxygen desaturation
• Low threshold for ultrasound of legs
• Risk of DVT/PE reduced by– Early mobilization
– SQ heparin, LMW heparin• Must weigh against risk of hemorrhagic complications
– Other alternatives• PT
• Compression stockings
Urinary tract infection
• Very common complication
• Urinary retention in early phase after stroke
• Need indwelling catheter
– Suprapubic may be less prone to UTI than FoleySuprapubic may be less prone to UTI than Foley
– Acidification may further lower risk of UTI
– Intermittent cath not shown to be safer
• Prophylactic anitbiotics are not recommended

14
Decubiti prevention
• Keep skin dry if incontinent
– Indwelling catheter
• Frequent turning
/• Air/fluid mattress if high risk
• Antibiotic therapy before debridement is justified
Post‐stroke depression
• 30‐50% of stroke survivors
• Left anterior, right posterior infarcts may predispose
d f i l i l i i k• Dependence for ADLs, social isolation are risks
• Tricyclics, SSRIs, methylphenidate, citalopram are all reasonable choices
Seizures after stroke
• 10% of patients some time after stroke
• #1 cause of acquired epilepsy in the elderly
• Higher risk
– Cardiac embolismCardiac embolism
– Cortical infarct
– EEG findings
• PLEDs
• Focal spikes
• 75% of new seizures occur within the first year
Strategies for managing acute ICP related complications of large
l li t t kvessel malignant stroke
Surgery for cerebellar infarct
• Rapidly progressive deterioration of consciousness
• Edematous changes on imaging
• Suboccipital craniectomy and duroplasty is accepted
– May need IVC if HCP presentMay need IVC if HCP present
• May need to incise dura first if very tense
– May need to resect cerebellar tissue if highly edematous
Surgery for cerebellar infarct

15
Surgery for ICH
• Controversial—who should get operation?
• Sometimes clear
– Young patient doing well, sudden deterioration with non dominant lobar hemorrhagewith non‐dominant lobar hemorrhage
– Dependent patient dominant ICH c thalamic extension, IVH and coma
• CPP > 70 desired post‐op
Class I evidence
• Supratentorial ICH 2ary ruptured aneurysm
– 27% mortality vs 80% for conservative treatment
• No class I evidence for cerebellar ICH
– Generally accepted patients may benefity p p y
Class II and III evidence
• Lots of studies
• Standard craniotomy, stereotaxic aspiration, ultrasonic aspiration
fli i• Conflicting reports
• Patients in deep coma may fare poorly
– Clot >50ml may favor craniotomy
– Small clots may do better with aspiration
• Must consider hydrocephalus
• Treating HCP may d i ll
Management of cerebellar hematom
dramatically restore consciousness
• Usually traumatic patients do better than spontaneous hemorrhages—age?
Recommendations Regarding Restarting Antithrombotic Therapy
• Class II– The decision to restart antithrombotic therapy after ICH related to
antithrombotic therapy depends on the risk of subsequent arterial or venous thromboembolism, the risk of recurrent ICH, and the overall state of the patient.
– For patients with a comparatively lower risk of cerebral infarction (e.g., AF without prior ischemic stroke) and a higher risk of amyloidAF without prior ischemic stroke) and a higher risk of amyloid angiopathy (e.g., elderly patients with lobar ICH) or with very poor overall neurological function, an antiplatelet agent may be an overall better choice for prevention of ischemic stroke than warfarin.
– In patients with a very high risk of thromboembolism in whom restarting warfarin is considered, warfarin therapy may be restarted after 7 to 10 days after onset of the original ICH
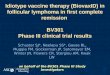
Cumulative Mortality Over 5 YearsAfter Ischemic Stroke
40
50
60
41
% 29
Hartmann A, et al. Neurology. 2001;57:2000-2005.
0
10
20
30
30 Days 5 Years
5
16
1 Year 3 Years
29

16
Cause of death
First stroke
Recurrent stroke
Cardiovascular disease
Long‐Term Cause of Stroke Mortality Risk at 5 Years
60
70
80
90
100
nt
Nonvascular disease
Unknown
Hankey GJ et al. Stroke. 2000;31:2080-2086.
Time since first–ever stroke
0
10
20
30
40
50
60
< 30d 30d–6m 6m–1yr 1-3yr 3-5yr
Per
cen
Cause of Death in Stroke Patients
“...survivors of atherosclerotic stroke are more likely to die from coronary events
than from a recurrent stroke.”
Wilterdink JL et al. Neurology. 1998:51(suppl 3):S23-S26.