Embed Size (px)
Citation preview

Problem Solving and DiabetesSelf-ManagementInvestigation in a large, multiracial sample
RUSSELL E. GLASGOW, PHD1
LAWRENCE FISHER, PHD2
MARILYN SKAFF, PHD2
JOE MULLAN, PHD2
DEBORAH J. TOOBERT, PHD3
OBJECTIVE — Problem solving is a core aspect of effective diabetes and chronic illnessself-management, yet there are relatively few objective evaluations of problem-solving skills,especially in large, multiracial samples.
RESEARCHDESIGNANDMETHODS — A multiracial sample of 506 adults who havetype 2 diabetes were assessed on a variety of patient characteristics, self-management behaviors,and biological and psychosocial measures. They also completed the Diabetes Problem-SolvingInterview (DPSI).
RESULTS — DPSI scores revealed significant variability across patients in problem-solvingskill and were related to a number of comorbid conditions and complications but not to severalother demographic factors, including race/ethnicity. Problem solving was also related to self-management behaviors (eating and exercise patterns), biological variables (A1C and lipids), andpsychosocial measures (Diabetes Distress Scale) in multivariable analyses controlling for a varietyof potential confounding factors.
CONCLUSIONS — Diabetes problem solving, as measured by the DPSI, is an importantpatient skill related to several key diabetes management variables that appears applicable acrossracial and ethnic groups. Future research is needed to identify the generality versus specificity ofdiabetes problem solving and practical interventions to enhance problem-solving skills.
Diabetes Care 30:33–37, 2007
S elf-management support is estab-lished as an evidence-based inter-vention for diabetes (1). A variety of
reviews and syntheses have concludedthat, at least in the short to medium term,diabetes self-management support is ef-fective (1–3). Further, almost all modelsor conceptualizations of the core aspectsof self-management support includeproblem-solving ability as a central fea-ture. This is true of the widely adoptedchronic disease self-management pro-gram of Lorig et al. (4), Chronic CareModel applications of self-management
support (5,6), the evidence-based five A’sapproach to health behavior change (7),and other well-controlled studies thathave been especially successful at longer-term maintenance of behavior change (8).
A substantial amount of research sup-ports the importance of effective problemsolving for successful adjustment andcoping. Much of this work has been basedupon the social problem-solving model ofD’Zurilla and colleagues (9,10). Thismodel has broad applicability to health-related conditions (11) and to regimenadherence (12). In diabetes, Hill-Briggs
(13) has applied problem-solving theoryto diabetes self-management and identi-fied problem-solving skill, along withproblem-solving orientation, disease-specific knowledge, and transfer of pastexperience as key components of effectiveself-management. Little is known, how-ever, about how patient characteristics in-cluding demographics, race, andpsychological distress are related to prob-lem solving.
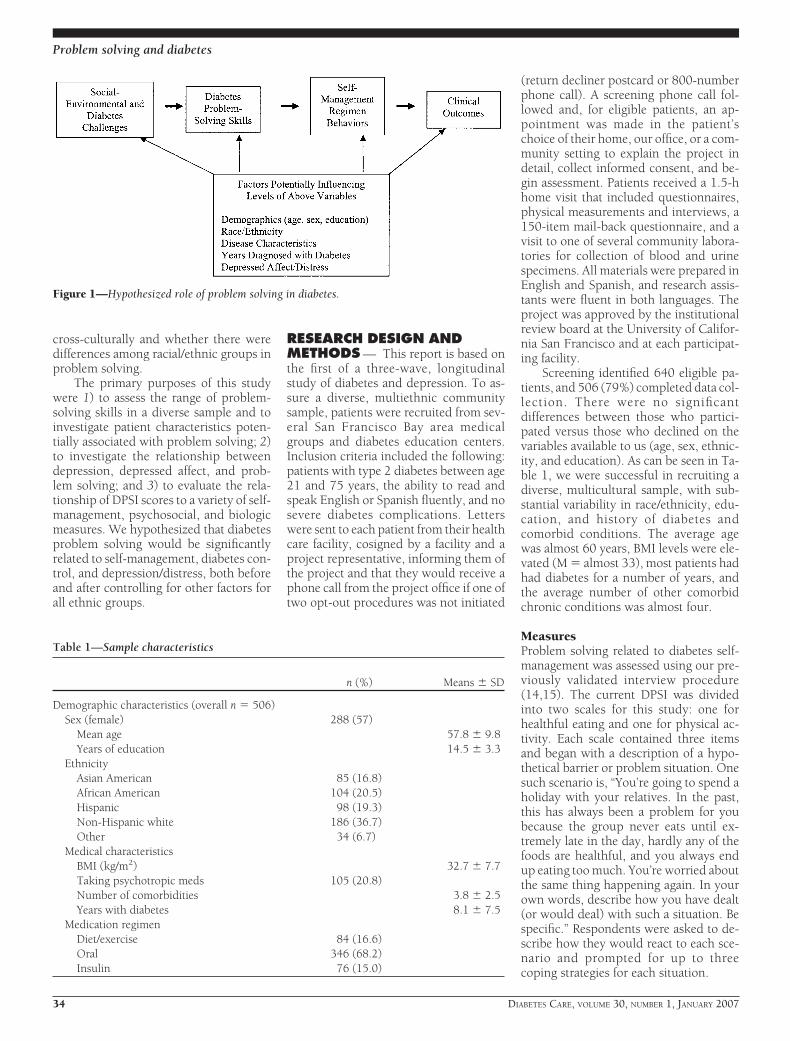
Finally, from a patient perspective,the challenges associated with having di-abetes and other chronic illnesses are notstatic. Rather, they are dynamic andchange over time, underscoring the needto have skills to cope with emerging is-sues, as opposed to simply “education”about standard responses or regimen be-haviors. Figure 1 depicts our conceptualmodel of how problem solving relates todiabetes. As can be seen, we conceptual-ize problem-solving skills as determininghow individuals will respond to chal-lenges and as strongly influencing theresulting levels of diabetes regimen self-management. Self-management regimenbehaviors, in turn, impact clinical out-comes. In addition, all of the above factorsare potentially influenced by the per-sonal, social, and medical characteristicsin the patients’ lives.
This study used a previously vali-dated assessment procedure, the DiabetesProblem-Solving Interview (DPSI), whichhas been found in prior research to be oneof the strongest predictors of diabetes self-management behaviors, to be sensitive toa self-management training interventionand to mediate behavior change in priorresearch (14,15). Use of both cognitiveand behavioral problem-solving strate-gies appeared to enable subjects to bemore successful in coping with the varietyof challenges posed by diabetes self-management behaviors. However, to ourknowledge, the DPSI has not been studiedwith large, multiracial samples or relatedto comprehensive measures of diabetescontrol and self-management. Given theimpact of health disparities, we felt itimportant to determine whether prob-lem-solving skills appear applicable
● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ●
From the 1Clinical Research Unit, Kaiser Permanente Colorado, Denver, Colorado; the 2Department ofFamily and Community Medicine, University of California, San Francisco, California; and the 3OregonResearch Institute, Eugene, Oregon.
Address correspondence and reprint requests to Russell E. Glasgow, PhD, Kaiser Permanente Colorado,P.O. Box 378066, Denver, CO 80237-8066; or 335 Road Runner Rd., Penrose, CO 81240. E-mail:[email protected].
Received for publication 3 July 2006 and accepted in revised form 29 September 2006.Abbreviations: DPSI, Diabetes Problem-Solving Interview.A table elsewhere in this issue shows conventional and Systeme International (SI) units and conversion
factors for many substances.DOI: 10.2337/dc06-1390© 2007 by the American Diabetes Association.The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby
marked “advertisement” in accordance with 18 U.S.C. Section 1734 solely to indicate this fact.
C l i n i c a l C a r e / E d u c a t i o n / N u t r i t i o nO R I G I N A L A R T I C L E
DIABETES CARE, VOLUME 30, NUMBER 1, JANUARY 2007 33
cross-culturally and whether there weredifferences among racial/ethnic groups inproblem solving.
The primary purposes of this studywere 1) to assess the range of problem-solving skills in a diverse sample and toinvestigate patient characteristics poten-tially associated with problem solving; 2)to investigate the relationship betweendepression, depressed affect, and prob-lem solving; and 3) to evaluate the rela-tionship of DPSI scores to a variety of self-management, psychosocial, and biologicmeasures. We hypothesized that diabetesproblem solving would be significantlyrelated to self-management, diabetes con-trol, and depression/distress, both beforeand after controlling for other factors forall ethnic groups.
RESEARCH DESIGN ANDMETHODS — This report is based onthe first of a three-wave, longitudinalstudy of diabetes and depression. To as-sure a diverse, multiethnic communitysample, patients were recruited from sev-eral San Francisco Bay area medicalgroups and diabetes education centers.Inclusion criteria included the following:patients with type 2 diabetes between age21 and 75 years, the ability to read andspeak English or Spanish fluently, and nosevere diabetes complications. Letterswere sent to each patient from their healthcare facility, cosigned by a facility and aproject representative, informing them ofthe project and that they would receive aphone call from the project office if one oftwo opt-out procedures was not initiated
(return decliner postcard or 800-numberphone call). A screening phone call fol-lowed and, for eligible patients, an ap-pointment was made in the patient’schoice of their home, our office, or a com-munity setting to explain the project indetail, collect informed consent, and be-gin assessment. Patients received a 1.5-hhome visit that included questionnaires,physical measurements and interviews, a150-item mail-back questionnaire, and avisit to one of several community labora-tories for collection of blood and urinespecimens. All materials were prepared inEnglish and Spanish, and research assis-tants were fluent in both languages. Theproject was approved by the institutionalreview board at the University of Califor-nia San Francisco and at each participat-ing facility.
Screening identified 640 eligible pa-tients, and 506 (79%) completed data col-lection. There were no significantdifferences between those who partici-pated versus those who declined on thevariables available to us (age, sex, ethnic-ity, and education). As can be seen in Ta-ble 1, we were successful in recruiting adiverse, multicultural sample, with sub-stantial variability in race/ethnicity, edu-cation, and history of diabetes andcomorbid conditions. The average agewas almost 60 years, BMI levels were ele-vated (M � almost 33), most patients hadhad diabetes for a number of years, andthe average number of other comorbidchronic conditions was almost four.
MeasuresProblem solving related to diabetes self-management was assessed using our pre-viously validated interview procedure(14,15). The current DPSI was dividedinto two scales for this study: one forhealthful eating and one for physical ac-tivity. Each scale contained three itemsand began with a description of a hypo-thetical barrier or problem situation. Onesuch scenario is, “You’re going to spend aholiday with your relatives. In the past,this has always been a problem for youbecause the group never eats until ex-tremely late in the day, hardly any of thefoods are healthful, and you always endup eating too much. You’re worried aboutthe same thing happening again. In yourown words, describe how you have dealt(or would deal) with such a situation. Bespecific.” Respondents were asked to de-scribe how they would react to each sce-nario and prompted for up to threecoping strategies for each situation.
Figure 1—Hypothesized role of problem solving in diabetes.
Table 1—Sample characteristics
n (%) Means � SD
Demographic characteristics (overall n � 506)Sex (female) 288 (57)
Mean age 57.8 � 9.8Years of education 14.5 � 3.3
EthnicityAsian American 85 (16.8)African American 104 (20.5)Hispanic 98 (19.3)Non-Hispanic white 186 (36.7)Other 34 (6.7)
Medical characteristicsBMI (kg/m2) 32.7 � 7.7Taking psychotropic meds 105 (20.8)Number of comorbidities 3.8 � 2.5Years with diabetes 8.1 � 7.5
Medication regimenDiet/exercise 84 (16.6)Oral 346 (68.2)Insulin 76 (15.0)
Problem solving and diabetes
34 DIABETES CARE, VOLUME 30, NUMBER 1, JANUARY 2007
Following the initial hypothetical sit-uation within each regimen area, partici-pants were asked to provide a personallyrelevant situation that made it difficult forthem to engage in that lifestyle practice(eating a healthful diet, engaging in phys-ical activity). Then they were asked to de-scribe strategies they would use forovercoming each obstacle to diabetes self-care. Prompts were provided to encour-age participants to list multiple strategies.Finally, respondents were asked to de-scribe the strategies they generally use tohelp them adhere to that aspect of theirregimen.
Coders provided an overall problem-solving rating for each situation on a5-point scale (from 1 � very poor strategyto 5 � excellent strategy). A rating of 1 or2 points was assigned if nothing was doneto improve the problem situation or if astrategy would produce a detrimental ef-fect (for instance, “If I have a stressful day,I skip exercise and watch television.”). Ascore of 4 or 5 points was assigned if strat-egies included planning ahead and flexi-bility in carrying out the regimen activity(for instance, “In case my first strategy didnot work, I would then . . .”; “I wouldeither walk before work if the weather wasgood or meet my neighbor at the mall if
the weather was bad.”). Coders were re-search assistants who read and discussedthe detailed coding manual and codedpractice responses before the actualstudy. The surveys were coded by inde-pendent raters who received 10 h of train-ing and held regular discussions of codingdisparities. Ratings were summed acrossitems in that scale to produce an averageoverall rating of problem-solving skill fordiet and physical activity, respectively. In-terrater reliability for a randomly selectedsubset of surveys (25%) coded by two dif-ferent coders was r � 0.96 (P � 0.001).Demographic and diabetes treatmentvariables. These included age, sex, eth-nicity (Hispanic, non-Hispanic white, Af-rican American, or Asian American),education in years, and type of diabetesmedication (diet/exercise, oral medica-tion, or insulin determined by self-report).Biological variables. These includedstandardized A1C and non-HDL cho-lesterol assays conducted in a centrallaboratory.Behavioral variables. The behavioralmanagement measures included averagecalories from saturated fat as a percentageof total calories consumed per day, de-rived from the Block 2000 Brief Food Fre-
quency Questionnaire (Block DietaryData Systems, Berkeley, CA). The otherbehavioral measure was physical activity,assessed by the International Physical Ac-tivity Questionnaire (16). This score re-flects minutes of activity per week acrossthree categories (walking, moderate, andvigorous) weighted by multiples of theresting metabolic rate for each activity fora 60-kg person.Psychosocial variables. The Center forEpidemiologic Studies Depression Scaleis a 20-item questionnaire that assessesdepressive symptoms over the previous 7days (17). The Diabetes Distress Scale wasused to assess discomfort and negativeemotions specifically related to diabetes(18). It has strong psychometric proper-ties and produces an overall score as wellas subscales measuring distress related toemotional burden, physician-related dis-tress, regimen-related distress, and inter-personal distress (18).
AnalysesAnalyses included descriptive statistics tocharacterize the sample, psychometriccharacteristics of the DPSI (interrater re-liabilities), adjusted and unadjusted biva-riate correlations and multiple regressionanalyses to evaluate the association be-tween problem solving, and 1) patientcharacteristics, 2) self-management be-haviors, 3) biological variables, and 4)psychosocial variables, including depres-sive affect and diabetes distress.
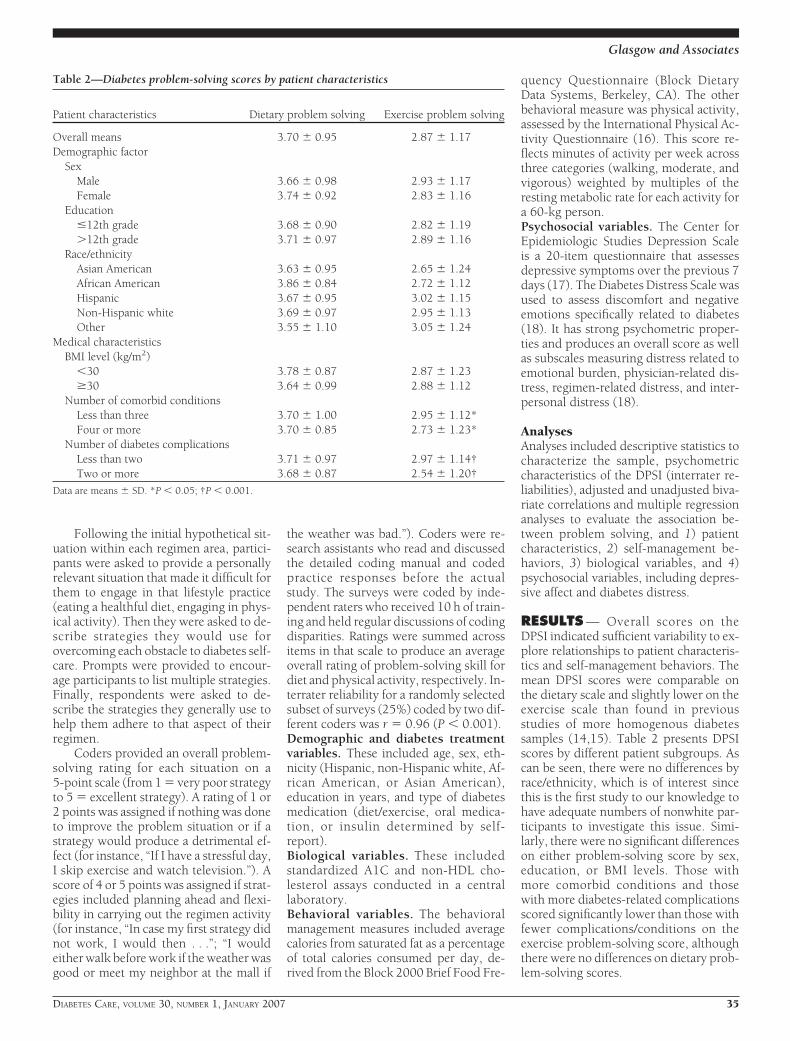
RESULTS — Overall scores on theDPSI indicated sufficient variability to ex-plore relationships to patient characteris-tics and self-management behaviors. Themean DPSI scores were comparable onthe dietary scale and slightly lower on theexercise scale than found in previousstudies of more homogenous diabetessamples (14,15). Table 2 presents DPSIscores by different patient subgroups. Ascan be seen, there were no differences byrace/ethnicity, which is of interest sincethis is the first study to our knowledge tohave adequate numbers of nonwhite par-ticipants to investigate this issue. Simi-larly, there were no significant differenceson either problem-solving score by sex,education, or BMI levels. Those withmore comorbid conditions and thosewith more diabetes-related complicationsscored significantly lower than those withfewer complications/conditions on theexercise problem-solving score, althoughthere were no differences on dietary prob-lem-solving scores.
Table 2—Diabetes problem-solving scores by patient characteristics
Patient characteristics Dietary problem solving Exercise problem solving
Overall means 3.70 � 0.95 2.87 � 1.17Demographic factor
SexMale 3.66 � 0.98 2.93 � 1.17Female 3.74 � 0.92 2.83 � 1.16
Education�12th grade 3.68 � 0.90 2.82 � 1.19�12th grade 3.71 � 0.97 2.89 � 1.16
Race/ethnicityAsian American 3.63 � 0.95 2.65 � 1.24African American 3.86 � 0.84 2.72 � 1.12Hispanic 3.67 � 0.95 3.02 � 1.15Non-Hispanic white 3.69 � 0.97 2.95 � 1.13Other 3.55 � 1.10 3.05 � 1.24
Medical characteristicsBMI level (kg/m2)
�30 3.78 � 0.87 2.87 � 1.23�30 3.64 � 0.99 2.88 � 1.12
Number of comorbid conditionsLess than three 3.70 � 1.00 2.95 � 1.12*Four or more 3.70 � 0.85 2.73 � 1.23*
Number of diabetes complicationsLess than two 3.71 � 0.97 2.97 � 1.14†Two or more 3.68 � 0.87 2.54 � 1.20†
Data are means � SD. *P � 0.05; †P � 0.001.
Glasgow and Associates
DIABETES CARE, VOLUME 30, NUMBER 1, JANUARY 2007 35
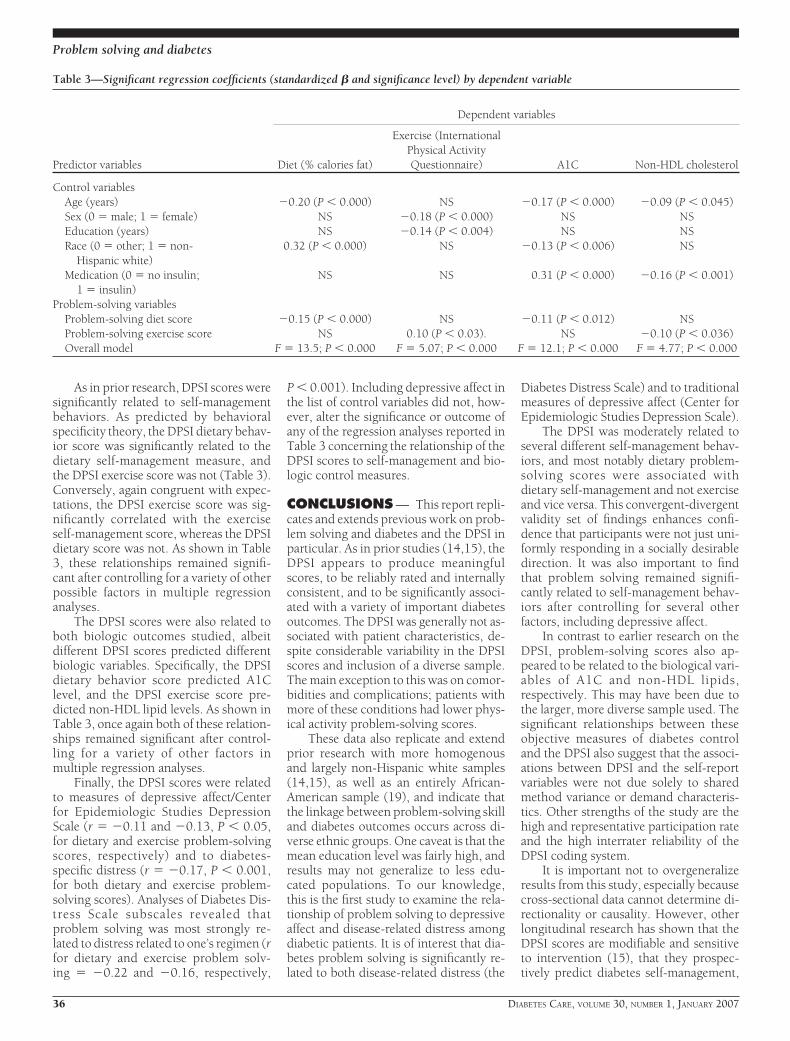
As in prior research, DPSI scores weresignificantly related to self-managementbehaviors. As predicted by behavioralspecificity theory, the DPSI dietary behav-ior score was significantly related to thedietary self-management measure, andthe DPSI exercise score was not (Table 3).Conversely, again congruent with expec-tations, the DPSI exercise score was sig-nificantly correlated with the exerciseself-management score, whereas the DPSIdietary score was not. As shown in Table3, these relationships remained signifi-cant after controlling for a variety of otherpossible factors in multiple regressionanalyses.
The DPSI scores were also related toboth biologic outcomes studied, albeitdifferent DPSI scores predicted differentbiologic variables. Specifically, the DPSIdietary behavior score predicted A1Clevel, and the DPSI exercise score pre-dicted non-HDL lipid levels. As shown inTable 3, once again both of these relation-ships remained significant after control-ling for a variety of other factors inmultiple regression analyses.
Finally, the DPSI scores were relatedto measures of depressive affect/Centerfor Epidemiologic Studies DepressionScale (r � �0.11 and �0.13, P � 0.05,for dietary and exercise problem-solvingscores, respectively) and to diabetes-specific distress (r � �0.17, P � 0.001,for both dietary and exercise problem-solving scores). Analyses of Diabetes Dis-tress Scale subscales revealed thatproblem solving was most strongly re-lated to distress related to one’s regimen (rfor dietary and exercise problem solv-ing � �0.22 and �0.16, respectively,
P � 0.001). Including depressive affect inthe list of control variables did not, how-ever, alter the significance or outcome ofany of the regression analyses reported inTable 3 concerning the relationship of theDPSI scores to self-management and bio-logic control measures.
CONCLUSIONS — This report repli-cates and extends previous work on prob-lem solving and diabetes and the DPSI inparticular. As in prior studies (14,15), theDPSI appears to produce meaningfulscores, to be reliably rated and internallyconsistent, and to be significantly associ-ated with a variety of important diabetesoutcomes. The DPSI was generally not as-sociated with patient characteristics, de-spite considerable variability in the DPSIscores and inclusion of a diverse sample.The main exception to this was on comor-bidities and complications; patients withmore of these conditions had lower phys-ical activity problem-solving scores.
These data also replicate and extendprior research with more homogenousand largely non-Hispanic white samples(14,15), as well as an entirely African-American sample (19), and indicate thatthe linkage between problem-solving skilland diabetes outcomes occurs across di-verse ethnic groups. One caveat is that themean education level was fairly high, andresults may not generalize to less edu-cated populations. To our knowledge,this is the first study to examine the rela-tionship of problem solving to depressiveaffect and disease-related distress amongdiabetic patients. It is of interest that dia-betes problem solving is significantly re-lated to both disease-related distress (the
Diabetes Distress Scale) and to traditionalmeasures of depressive affect (Center forEpidemiologic Studies Depression Scale).
The DPSI was moderately related toseveral different self-management behav-iors, and most notably dietary problem-solving scores were associated withdietary self-management and not exerciseand vice versa. This convergent-divergentvalidity set of findings enhances confi-dence that participants were not just uni-formly responding in a socially desirabledirection. It was also important to findthat problem solving remained signifi-cantly related to self-management behav-iors after controlling for several otherfactors, including depressive affect.
In contrast to earlier research on theDPSI, problem-solving scores also ap-peared to be related to the biological vari-ables of A1C and non-HDL lipids,respectively. This may have been due tothe larger, more diverse sample used. Thesignificant relationships between theseobjective measures of diabetes controland the DPSI also suggest that the associ-ations between DPSI and the self-reportvariables were not due solely to sharedmethod variance or demand characteris-tics. Other strengths of the study are thehigh and representative participation rateand the high interrater reliability of theDPSI coding system.
It is important not to overgeneralizeresults from this study, especially becausecross-sectional data cannot determine di-rectionality or causality. However, otherlongitudinal research has shown that theDPSI scores are modifiable and sensitiveto intervention (15), that they prospec-tively predict diabetes self-management,
Table 3—Significant regression coefficients (standardized � and significance level) by dependent variable
Predictor variables
Dependent variables
Diet (% calories fat)
Exercise (InternationalPhysical ActivityQuestionnaire) A1C Non-HDL cholesterol
Control variablesAge (years) �0.20 (P � 0.000) NS �0.17 (P � 0.000) �0.09 (P � 0.045)Sex (0 � male; 1 � female) NS �0.18 (P � 0.000) NS NSEducation (years) NS �0.14 (P � 0.004) NS NSRace (0 � other; 1 � non-
Hispanic white)0.32 (P � 0.000) NS �0.13 (P � 0.006) NS
Medication (0 � no insulin;1 � insulin)
NS NS 0.31 (P � 0.000) �0.16 (P � 0.001)
Problem-solving variablesProblem-solving diet score �0.15 (P � 0.000) NS �0.11 (P � 0.012) NSProblem-solving exercise score NS 0.10 (P � 0.03). NS �0.10 (P � 0.036)Overall model F � 13.5; P � 0.000 F � 5.07; P � 0.000 F � 12.1; P � 0.000 F � 4.77; P � 0.000
Problem solving and diabetes
36 DIABETES CARE, VOLUME 30, NUMBER 1, JANUARY 2007

even after controlling for potential con-founding variables (14), and that DPSImediated treatment outcomes (15). Con-sidered along with related conceptualwork on understanding how problemsolving impacts health behaviors and dis-ease management (10,13), the presentstudy helps to explicate paths betweenskills such as problem solving, self-management, and diabetes control(13,20). Our findings also suggest thatproblem-solving therapy may be benefi-cial for those with low levels of regimenself-management (9,10), including thosewith depression and diabetes distress.
A practical limitation to the broaderuse of the current DPSI interview proce-dure is that it does not provide immediatefeedback and is moderately expensive, re-quiring trained raters (15). We estimatethat the assessment procedure used in thisstudy took 10 min of participant time,and the coding responses cost �$10 perpatient. From an ease of use and immedi-acy of feedback perspective, it would bedesirable if the DPSI could be immedi-ately scored by clinic staff or even self-administered. This may someday bepossible, but to date we have not foundversions of the assessment such as paper-and-pencil or multiple-choice formats tobe sufficiently sensitive, perhaps pointingout the difference between the ability torecognize versus generate high-qualitysolutions to potential problems (9).
Future research is needed to deter-mine whether shorter or self-report mea-sures of problem solving can perform aswell, to determine whether problem solv-ing is a general or specific skill (or both),and to investigate culturally sensitive,cost-efficient interventions to see if theycan significantly increase problem-solving skills and produce long-term im-provements in diabetes self-management,control, and quality of life.
Acknowledgments— This research was sup-ported by grants DK062732 and DK061937
from the National Institute of Diabetes and Di-gestive and Kidney Diseases.
The following medical groups and diabeteseducation centers collaborated in this re-search: Alta Bates Diabetes Education Center,Brown and Toland Medical Group, CaliforniaPacific Diabetes Education Center, Hill Physi-cians Medical Group, Marin IPA, St. Luke’sDiabetes Education Center, St. Mary’s MedicalCenter, University of California, and San Fran-cisco Hospital and Clinics. We also thankShannon McCarthy and Sally Skolnick fortheir expert coding.
References1. Norris SL, Nichols PJ, Caspersen CJ, Glas-
gow RE, Engelgau MM, Jack L, Snyder SR,Carande-Kulis VG, Isham G, Garfield S,Briss P, McCulloch D: Increasing diabetesself-management education in commu-nity settings: a systematic review. Am JPrev Med 22:39–66, 2002
2. Bodenheimer TS, Lorig K, Holman H,Grumbach K: Patient self-management ofchronic disease in primary care. JAMA288:2469–2475, 2002
3. Glasgow RE, Bayliss E, Estabrooks EA:Translation research in diabetes: askingbroader questions. In Evidence-Based En-docrinology. Montori VM, Ed. Totowa, NJ,Humana Press, 2005, p. 241–256
4. Lorig KR, Sobel DS, Ritter PL, Laurent D,Hobbs M: Effect of a self-managementprogram on patients with chronic illness.Eff Clin Pract 4:256–262, 2001
5. Glasgow RE, Funnell MM, Bonomi AE,Davis C, Beckham V, Wagner EH: Self-management aspects of the improvingchronic illness care breakthrough series:implementation with diabetes and heartfailure teams. Ann Behav Med 24:80–87,2002
6. Glasgow RE, Davis CL, Funnell MM, BeckA: Implementing practical interventionsto support chronic illness self-manage-ment. 29:563–574, 2003
7. Whitlock EP, Orleans CT, Pender N, Al-lan J: Evaluating primary care behavioralcounseling interventions: an evidence-based approach. Am J Prev Med 22:267–284, 2002
8. Perri MG, McAllister DA, Gange JJ, JordanRC, McAdoo WG, Nezu AM: Effects of
four maintenance programs on the long-term management of obesity. J ConsultClin Psychol 56:529–534, 1988
9. D’Zurilla TJ: Problem-Solving Therapy: ASocial Competence Approach to Clinical In-tervention. New York, Springer, 1996
10. Chang E, D’Zurilla TJ, Sanna LJ: SocialProblem-Solving: Theory, Research, andTraining. Washington, DC, American Psy-chological Association, 2004
11. Elliott TR, Shewcuk RM, Miller DM, Rich-ards JS: Profiles in problem-solving: psy-chological well-being and distress amongpersons with diabetes mellitus. J Clin En-docrinol Metab 8:283–291, 2001
12. Johnson MO, Elliott TR, Neilands TB,Morin SF, Chesney MA: A social problem-solving model of adherence to HIV med-ications. Health Psychol 25:355–363,2006
13. Hill-Briggs F: Problem solving in diabetesself-management: a model of chronic ill-ness self-management behavior. Ann Be-hav Med 25:182–193, 2003
14. Toobert DJ, Glasgow RE: Problem-solvingand diabetes self-care. J Behav Med 14:71–86, 1991
15. Glasgow RE, Toobert DJ, Barrera M Jr,Strycker LA: Assessment of problem-solv-ing: a key to successful diabetes self-man-agement. J Behav Med 27:477–490, 2004
16. Ainsworth BE, Haskell WL, Whitt MC:Compendium of physical activities: anupdate of activity codes and MET intensi-ties. Med Sci Sports Exer 32:S498–S504,2000
17. Radloff LS: The CES-D scale: a self-reportdepression scale for research in the gen-eral population. Appl Psychol Meas 3:385–401, 1997
18. Polonsky WH, Fisher L, Darles J, Dudl RJ,Lees J, Mullan J, Jackson RA: Assessingpsychosocial distress in diabetes: devel-opment of the diabetes distress scale. Di-abetes Care 28:626–631, 2005
19. Hill-Briggs F, Gary TL, Yeh HC, Batts-Turner M, Powe NR, Saudek CD, BrancatiFL: Association of social problem solvingwith glycemic control in a sample of ur-ban African Americans with type 2 diabe-tes. J Behav Med 29:69–78, 2006
20. Glasgow RE: A practical model of diabetesmanagement and education. DiabetesCare 18:117–126, 1995
Glasgow and Associates
DIABETES CARE, VOLUME 30, NUMBER 1, JANUARY 2007 37





























