-
8/2/2019 Procedures Workshop 2012
1/49
Procedures Workshop
Joel Pasternack, MD, PhD
University of Rochester
-
8/2/2019 Procedures Workshop 2012
2/49
Core Procedures
1. Central Venous line - femoral vein, subclavian vein,
internal jugular vein
2. Lumbar puncture
3. Foley catheter
4. Nasogastric tube
5. Intravenous line*
6. Arterial Blood Gas* - radial artery, femoral artery
* These procedures are difficult to simulate on a cadaver.
-
8/2/2019 Procedures Workshop 2012
3/49
Additional Procedures
Endotracheal intubation - curved blade, straight blade
Digital blocks - fingers, thumb, toes
Joint aspiration - knee, elbow, ankle
Thoracentesis
Arterial lines* - radial artery, femoral artery
* This procedure is difficult to simulate on a cadaver.
-
8/2/2019 Procedures Workshop 2012
4/49
General Principles
Know the following:
1. Indications
2. Equipment sizes
3. Level of sterility
4. Anatomy and positioning which makesprocedure easiest for
operator and patient.
5. Complications and modes of failure.
6. Anesthesia/analgesia
-
8/2/2019 Procedures Workshop 2012
5/49
Important Caveat for any procedure with a needle
**DO NOT SWING THE NEEDLE **
If you need to redirect needle, withdraw to just under the
skin, and redirect.
Otherwise, redirecting by swinging allows the needle tip to
act like a knife cutting tissue.
-
8/2/2019 Procedures Workshop 2012
6/49
Central Venous line
Indications:
- inability to obtain peripheral IV- need for multiple ports and
repeated blood draws
- need for very large bore access
- central pressure monitoring or passage of Swan Ganz
catheter or cardiac pacer.
-
8/2/2019 Procedures Workshop 2012
7/49
Central Venous line
Adults:- standard 3-way central line is 7 French
(one 16 gauge port and two 18 gauge ports)
- Large bore introducer 9 French
Pediatrics:- double lumen catheter
4 French for < 10 kg
5 French for > 10 kg
-
8/2/2019 Procedures Workshop 2012
8/49
Central Venous line
- Needs to be sterile
- Use large drape to keep the wire
sterile.
-
8/2/2019 Procedures Workshop 2012
9/49
Central Venous line Positioning
Femoral vein:
- Leg extended at hip (difficult with hip flexed)
- Slight abduction and external rotation.
- Folded towel under buttocks helps in problem cases
Subclavian vein:
- Slight Trendelenburg (head & shoulders lower than
heart)
Internal jugular:
- Slight Trendelenburg, right IJ preferred(no thoracic duct,
straight shot at SVC, dome of right lung is lower)
- Sternocleidomastoid muscle defines the 3 approaches
(anterior, posterior, central)
-
8/2/2019 Procedures Workshop 2012
10/49
Central Venous line
Complications:- hemorrhage
- vascular injury
- cardiac arhythmia
- wire embolus
- catheter embolus- air embolus, infection
- thrombosis
- pneumothorax (subclavian or internal jugular)
- airway compromise (internal jugular).
Modes of failure:
- cant find vein
- cant pass wire
- catheterize artery
- misplacement of subclavian line up into neck
-
8/2/2019 Procedures Workshop 2012
11/49
Central Venous line
Anesthesia:
Local lidocaine
-
8/2/2019 Procedures Workshop 2012
12/49
-
8/2/2019 Procedures Workshop 2012
13/49
-
8/2/2019 Procedures Workshop 2012
14/49
-
8/2/2019 Procedures Workshop 2012
15/49
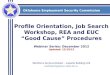
Jugular Vein Size Variation
I l J l V i
-
8/2/2019 Procedures Workshop 2012
16/49
Internal Jugular Vein
-
8/2/2019 Procedures Workshop 2012
17/49
-
8/2/2019 Procedures Workshop 2012
18/49
-
8/2/2019 Procedures Workshop 2012
19/49
-
8/2/2019 Procedures Workshop 2012
20/49
-
8/2/2019 Procedures Workshop 2012
21/49
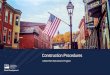
Femoral Vein and Artery
-
8/2/2019 Procedures Workshop 2012
22/49
Lumbar Puncture
Indications:
Evaluate for:
- meningitis- subarachnoid hemorrhage
- psuedo-tumor cerebri
-
8/2/2019 Procedures Workshop 2012
23/49
Lumbar Puncture
Sterile procedure
22 gauge needleLength: - adults 3 inch
- young children 1.5 inch
- Indicate top of iliac crests with line on skin- Position
patient with back in forward flexion
(lying on side or sitting up)
- Enter skin at or cephalad to line demarcating iliac crest
(stay in mid sagital plane)
-
8/2/2019 Procedures Workshop 2012
24/49
Lumbar Puncture
Complications:
- paresthesias
- nerve root injury (rare)
Modes of Failure:
- inability to obtain CSF because puncture site over sacrum
- inability to obtain CSF because path of needle not
inmid-sagital plane
- bloody tap
-
8/2/2019 Procedures Workshop 2012
25/49
Lumbar Puncture
Anesthesia:
- Local lidocaine
- Conscious sedation for children age 2-10
-
8/2/2019 Procedures Workshop 2012
26/49
-
8/2/2019 Procedures Workshop 2012
27/49
-
8/2/2019 Procedures Workshop 2012
28/49
-
8/2/2019 Procedures Workshop 2012
29/49
Foley Catheter
Indications:
- monitor urinary output
- relieve urinary obstruction
-
8/2/2019 Procedures Workshop 2012
30/49
Foley Catheter
- Sterile technique
- Use 16 or 18 French in adults (larger if hematuria with
clots)
- Coude catheter for difficult catheterization in males
Females - urethral meatus in midline.
Males - anatomic position of penis is erect
(catheter passes easier as U than S)Hypospadias - urethra is
ventral in midline.
-
8/2/2019 Procedures Workshop 2012
31/49
Foley Catheter
Modes of failure:
- failure to visualize meatus in females
- failure to pass through prostate with or without catheter
looping around in posterior urethra
-
8/2/2019 Procedures Workshop 2012
32/49
Foley Catheter
Anesthesia:
Lidocaine Urojet for males
-
8/2/2019 Procedures Workshop 2012
33/49
-
8/2/2019 Procedures Workshop 2012
34/49
-
8/2/2019 Procedures Workshop 2012
35/49
-
8/2/2019 Procedures Workshop 2012
36/49
Nasogastric tube
Indications:
- decompress stomach in bowel obstruction
- assess for UGI bleeding
-
8/2/2019 Procedures Workshop 2012
37/49
Nasogastric tube
Adults - Use 18 French
Babies - 8 or 10 French
- tube goes straight back in nasal cavity
- tilt head in extension to get around bend at nasopharynx
- flex head forward to keep tube out of trachea.
-
8/2/2019 Procedures Workshop 2012
38/49
Nasogastric tube
Modes of failure:
- Tube curling around in mouth
- Tube in trachea
-
8/2/2019 Procedures Workshop 2012
39/49
Nasogastric tube
Anesthesia: Problematic.
- LET or Lido w Epi or Cocaine in nose
- Cetacaine spray of throat.
(Alternative Lidocaine neb)
-
8/2/2019 Procedures Workshop 2012
40/49
-
8/2/2019 Procedures Workshop 2012
41/49
Arterial Blood Gas
Indications:
- Assess acid/base status and ventilation
-
8/2/2019 Procedures Workshop 2012
42/49
Arterial Blood Gas
- 22 gauge sterile needle
- 21 or 23 butterfly w stop cock for additional blood tests
- clean gloves
Femoral arteryjust distal to inguinal ligament way
between pubic tubercle & ant. sup. iliac spine
but usually palpable pulse
Radial arteryradial to flex carpi radialis tendon
easiest to puncture with full supination forearm
and moderate extention wrist
-
8/2/2019 Procedures Workshop 2012
43/49
Arterial Blood Gas
Complications:
- arterial injury (hematoma, pseudoaneurysm, or thrombosis)
Modes of failure:
- inability to hit artery despite feeling pulse.
Suggested technique
- feel pulse with index and long finger slightly separated
-dont push down too hard with proximal finger
- keep needle in line of artery
- puncture between fingers
-
8/2/2019 Procedures Workshop 2012
44/49
Arterial Blood Gas
Anesthesia:
Lidocaine without epinephrine
-
8/2/2019 Procedures Workshop 2012
45/49
Arterial Lines
- Similar to ABG.
- 20 gauge IV catheter or
Seldinger technique (kits available)
- Radial line kit with enclosed wire
obviates need to sterile drape.
-
8/2/2019 Procedures Workshop 2012
46/49
-
8/2/2019 Procedures Workshop 2012
47/49
-
8/2/2019 Procedures Workshop 2012
48/49
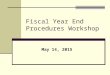
Thoracentesis or
Chest tube insertion
Enter thoracic cavity just above a rib rather
than just below a rib. Remember the neuro-
vascular bundle is just below the rib.
Place chest tubes posterior to pectoralis major
in the anterior or mid axillary line.
-
8/2/2019 Procedures Workshop 2012
49/49