Embed Size (px)
DESCRIPTION
Prof. MAM Ibnouf, FRCSEd. Omdurman Islamic university MBDI Bile duct injury was estimated 1-3/1000 in Open Cholecystectomy 4-6/1000 Laparoscopic Cholecystectomy 1- Nuzzo G. Giuliante F. Giovannini,I et al. Bile Duct Injury During Laparoscopic Cholecystectomy. Results of an Italian National Survey on 56 591 Cholecystectomies. Arch Surg. 2005;140:986-992. 2- Windsor JA, Pong J. Laparoscopic biliary injury: more than a learning curve problem. Aust NZ J Surg. 1998; 68: 186-189. 3- Calvete J, Sabater L, Camps B et al. Bile duct injury during laparoscopic cholecystectomy: myth or reality of the learning curve? Surg Endosc. 2000; 14: 608-611.) 4- Kern KA. Medicolegal analysis of bile duct injury during open cholecystectomy and abdominal surgery. Am J Surg. Am J Surg. 1994; 168: 217-222. 5- Howes N, Chagla L, Thorpe M, et al. Surgical practice is evidence based. British Journal of Surgery 1997;84:1220–3. Prof. MAM Ibnouf, FRCSEd. Omdurman Islamic university
Citation preview

The Iatrogenic Major Bile Duct Injuries:
Experience at Ibn Siena Hospital
MAM Ibnouf AM Masaad
Prof. MAM Ibnouf, FRCSEd. Omdurman Islamic university

MBDI
Bile duct injury was estimated1-3/1000 in Open Cholecystectomy 4-6/1000 Laparoscopic Cholecystectomy
1- Nuzzo G. Giuliante F. Giovannini,I et al. Bile Duct Injury During Laparoscopic Cholecystectomy. Results of an Italian National Survey on 56 591 Cholecystectomies. Arch Surg. 2005;140:986-992.
2- Windsor JA, Pong J. Laparoscopic biliary injury: more than a learning curve problem. Aust NZ J Surg. 1998; 68: 186-189.
3- Calvete J, Sabater L, Camps B et al. Bile duct injury during laparoscopic cholecystectomy: myth or reality of the learning curve? Surg Endosc. 2000; 14: 608-611.)
4- Kern KA. Medicolegal analysis of bile duct injury during open cholecystectomy and abdominal surgery. Am J Surg. Am J Surg. 1994; 168: 217-222.
5- Howes N, Chagla L, Thorpe M, et al. Surgical practice is evidence based. British Journal of Surgery 1997;84:1220–3. Prof. MAM Ibnouf, FRCSEd. Omdurman
Islamic university

• This rate may reach 14/10001,2
• mortality as high as 11/10003.
1- Gronroos J M. Unsuccessful Endoscopic Stenting in Iatrogenic Bile Duct Injury: Remember Rendezvous Procedure. Surgical Laparoscopy, 2007; 17(3):186-189,
2- Gentileschi P, Di Paola M , Catarci M, et al. Bile duct injuries during laparoscopic cholecystectomy. Surgical Endoscopy. 2004; 18 ( 2): 232-236.
3- Buanes T, Mjaland O, Waage A, et al. A population-based survey of biliary surgery in Norway: relationship between patient volume and quality of surgical treatment. Surg Endosc. 1998;12:852-855.Prof. MAM Ibnouf, FRCSEd. Omdurman
Islamic university

Learning curve
• “The incidence of BDI significantly decreased with increasing number of LCs performed, ranging from 0.9% for surgeons who had performed fewer than 150 LCs to 0.3% for those who had performed more than 450 LCs”*.
*Howes N, Chagla L, Thorpe M, et al. Surgical practice is evidence based. British Journal of Surgery 1997;84:1220–3.Prof. MAM Ibnouf, FRCSEd. Omdurman Islamic university

Mortality The mean mortality rate in 15 case series composed of a
total of 602 IMBDIs with a follow up period 1-7 years was 17(2.8%)1.
Poor results are associated with:1- delayed referrals,2- biliary peritonitis3- associated vascular injury4-other co-morbid factors resulting in as high as 9.4%
mortality rate2
1- Johnson SR, Koehler A, Pennington LK, Hanto DW. Long-term results of surgical repair of bile duct injuries following laparoscopic cholecystectomy. Surgery. 2000 Oct;128(4):668-77.
2- Flum DR, Koespsell T, Heagerty P et al. Common Bile Duct Injury During Laparoscopic Cholecystectomy and the Use of Intraoperative Cholangiogram: adverse outcome or preventable error. Arch Surg. 2001; 136:1287-1292.
Prof. MAM Ibnouf, FRCSEd. Omdurman Islamic university

• The mortality rate in 39 cases of Bisthmus type III and IV was reported to be 25%*.
*Chaudhary A, Chandra A, Negi SS, Sachdev A. Reoperative surgery for postcholecystectomy bile duct injuries. Dig Surg. 2002;19(1):22-7.Prof. MAM Ibnouf, FRCSEd. Omdurman
Islamic university

The experience at Ibn sina Hospital
• Period: Jan 1998 to date• Exclusion criteria: 1- Residual CBD stone retrieved by
ERCP 2- Post cholecystectomy bile duct injuries managed successfully with endoscopic stenting
Prof. MAM Ibnouf, FRCSEd. Omdurman Islamic university

Number: 85 patients
Male: female : 3:82
Mean (±SD) age: 38.6 ± 10.66, range 22- 66 years
Type of surgery: Open Chole 73(85.8%) LC 12(14.2%)
Mode of presentation: Jaundice:54(63.5%) Bile leak:31(36.5%)
Prof. MAM Ibnouf, FRCSEd. Omdurman Islamic university

bile leak jaundice TotalOpen chole 27 46 73Lap chole 4 8 12 Total 31 54 85
Massage: High tendency towards over sewing or over clipping bleeders
Prof. MAM Ibnouf, FRCSEd. Omdurman Islamic university

Method of diagnosis
• ERCP 47 patients• MRCP 28 “• Both 15 “
Prof. MAM Ibnouf, FRCSEd. Omdurman Islamic university

Types of injuries
• Bisthmus III and IV 68 cases• Bisthmus type II 15
cases• Unkown 02
cases Massage: Most of the cases are high injuries
Prof. MAM Ibnouf, FRCSEd. Omdurman Islamic university

Period of delay: Range 00 days* – 1 year
* 3 occurred at Ibn Siena Hospital: One in laparoscopic workshop and the second by a surgeon under training and one by registrar to right bile duct
Prof. MAM Ibnouf, FRCSEd. Omdurman Islamic university

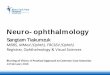
Poor referrals reports
MassageERCP does show the surgeon the site and size of the upper stump he should use for reconstruction
• ERCP
Prof. MAM Ibnouf, FRCSEd. Omdurman Islamic university

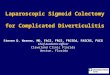
MRCP
Prof. MAM Ibnouf, FRCSEd. Omdurman Islamic university

MRCP
Prof. MAM Ibnouf, FRCSEd. Omdurman Islamic university

MRCP
Prof. MAM Ibnouf, FRCSEd. Omdurman Islamic university

MRCP
Prof. MAM Ibnouf, FRCSEd. Omdurman Islamic university

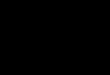
Bisthmus IV: high narrow ducts
Prof. MAM Ibnouf, FRCSEd. Omdurman Islamic university

Biliary peritonitis
Prof. MAM Ibnouf, FRCSEd. Omdurman Islamic university

Management
Initial drainage 23 patients
Rodney Smith (Mucosal graft) 55(64.7%) Hepatico-jejunostomy 23(27%)Repaired over T-tube 2(2.3%)
Died before reconstruction 2(2.3%)
Left abroad 3(3.5%)Prof. MAM Ibnouf, FRCSEd. Omdurman
Islamic university

Prof. MAM Ibnouf, FRCSEd. Omdurman Islamic university

Post-operative stenting
3 months 58pts 6 months 18pts1.5-2 months 3pts
Prof. MAM Ibnouf, FRCSEd. Omdurman Islamic university

Hospitalization period: Before surgery: 3-10 days After surgery: 10 days -3 weeks
Operative time: 2.5 - 4 hours
Massage: reconstruction of IMBDI is technically difficult and has very high costs
Prof. MAM Ibnouf, FRCSEd. Omdurman Islamic university

Follow up
Stricture: 22 patients
Specific complications:
Recurrent Cholangitis 15(17.6%)Biliary cirrhosis: 7(8.2%)
Intra-hepatic duct stones (Redo-surgery) 2 patientsCirrhosis (Redo-surgery abroad) 1 patients
Prof. MAM Ibnouf, FRCSEd. Omdurman Islamic university

Stricture with stones
Prof. MAM Ibnouf, FRCSEd. Omdurman Islamic university

Type of surgery and outcome was dictated by the level of injury
complications Rodney-Smith Hepatico-jej T-tube Total (n=55) (n=23) (n=2) 80Cholangitis 13 2 … 15(17.6%)Cirrhosis 6 1 … 7(8.2%)PE 1 0 … 1(1.2%)*Septicaemia 0 0 … ….No complications 35 20 2 57(67%)
* DiedProf. MAM Ibnouf, FRCSEd. Omdurman
Islamic university

Outcome after 3 years follow up
No complications 57(67%)Recurrent Cholangitis 15(17.6)Cirrhosis 7(8.2%Pulmonary embolisim 2(2.3%) DiedSepticaemia 2(2.3%) DiedAdvanced cirrhosis hepatic failure 1(1.1%
Massage: Morbidity rate 22(25.9%) Mortality rate 5(5.9%)
Prof. MAM Ibnouf, FRCSEd. Omdurman Islamic university

Out come of ligation & transection P 0.001
Bile leak Jaundice Total (n=54pts) (31pts) 85Cholangitis 12 3 15Cirrhosis 6 1 7PE 1 1Septicaemia 2 2No complications 33 29 60
Massage: IMBDI with bile leak tend to have poorer results
Prof. MAM Ibnouf, FRCSEd. Omdurman Islamic university

Adverse outcome
Died before reconstruction 2 Patients
Left abroad 3(1.5%)
Massage: In hospital death after reconstruction 1 Patient
Massage: 2 out of 3 Died after reconstruction abroad
Massage: Mortality rate 5(5.9%)
Prof. MAM Ibnouf, FRCSEd. Omdurman Islamic university

Where do we stand?Series Number of repairs M&M re-stricture/cholangitisMacFadyen BV Jr 1998 561 27(4.9%)Walsh RM 2004 133 46(35%)Slater K et al 131 2(1.5%) one of them diedIbn Siena Hospital 85 22(25.9%) five of them diedChaudhary A et al 41 3(7%) one of them diedWalsh RM et al 1998 34 18(25%)Johnson SR et al 2000 21 7(33.3%)Al-Sebaye MI 17 7(41%)Topal B et al 1999 16 4(25%) one of them diedKarvonen J 2007 14 3(26%) one of them died
Massage: Ibn Sina Series is the 4th biggest series and the 4th in the rate of complications
MAM Ibnouf1, A.Majid M. Massaad2 Iatrogenic Major Bile duct Injuries Injury. Sudan JMS Vol. 2, No. 3, Sep. 2007Mohammad A M Ibnouf, A. M. Massaad, Sulaiman S Fediel "Iatrogenic major bile duct injury in Sudan" Sudan Med. J. (19) 3; 2001: 36-39.
Prof. MAM Ibnouf, FRCSEd. Omdurman Islamic university

Conclusion1- IMBDI leads to life long morbidity and high
chances for mortality 2- High injuries are common in OC and LC and are
difficult to repair.
3- Injuries leading to bile leak prevent ductal dilatation and hence are associated with high rate of re-stricture.
Prof. MAM Ibnouf, FRCSEd. Omdurman Islamic university

Conclusion4- Stents should be left till maturation of the
fibrous tissue of the anastomotic line matures.
5- Results of reconstructive surgery at Ibn Siena is comparable to reported literature.
6- National Cholecystectomy Registry:to evaluate the real magnitude of the IMBDI.
Prof. MAM Ibnouf, FRCSEd. Omdurman Islamic university

Prof. MAM Ibnouf, FRCSEd. Omdurman Islamic university