Embed Size (px)
Citation preview

Prognosis of Patients with Acute PulmonaryEdema and Normal Ejection FractionAfter Acute Myocardial Infarction
MARY ANN WARNOWICZ, D.O., HOWARD PARKER, M.D., AND MELVIN D. CHEITLIN, M.D.
SUMMARY To assess the prognostic importance of resting left ventricular function in survivors of acutemyocardial infarction with pulmonary edema, we retrospectively identified 39 consecutive patients whopresented with acute pulmonary edema and myocardial infarction. Sixteen patients had radionuclideejection fractions 10 2 days postinfarction of > 0.45 (group A, mean 0.55 0.06), and 23 patients hadejection fractions S 0.45 (group B, 0.32 + 0.06). There were no significant differences between the twogroups for age or sex, but group A patients had a significantly greater incidence of first myocardialinfarction predominantly inferior in location. The calculated stroke work index during the acute event wassignificantly greater in group A than in group B (33.4 + 2.4 vs 23.4 + 2.0) (p < 0.05). During a follow-up of9 3 months, mortality was not significantly different between the two groups: Four (25%) died in group Aand seven (30%) died in group B. In addition, eight patients (50%) in group A were hospitalized forrecurrent angina, new myocardial infarction or recurrent pulmonary edema, compared with 11 (48%) ingroup B (NS). Three deaths in group A were preceded by infarction of the anterior wall of the left ventricle,confirmed at autopsy, and two nonfatal infarctions were anterior by electrocardiography. Four patients ingroup A had coronary arteriography performed during the follow-up period because of unstable angina,and all had significant (Dr 70% stenosis) three-vessel disease and two had left main coronary artery disease.Therefore, the predischarge ejection fraction did not predict prognosis for this group of patients.
Patients with acute pulmonary edema in the course of myocardial infarction form a high-risk group
despite good resting left ventricular function at discharge. They have a significant incidence of recurrentmyocardial infarction and death and, because they have good residual left ventricular function, are
excellent candidates for surgical intervention.
THE EARLY and late prognoses for acute myocardialinfarction are adversely affected by the occurrence ofleft ventricular failure. 1-3 The manifestation of acutepulmonary edema is particularly lethal.' 4, 10 Presum-ably, pulmonary edema reflects the severity and extentof acute and chronic abnormalities in left ventricularcontraction. Thus, pulmonary edema is more commonin patients with a history of infarction and in patientswith large initial infarctions, which are usually anteriorwall infarctions. It is not surprising that in a study bySchelbert et al. ,14 measuring radionuclide ejectionfractions after myocardial infarction, patients with pul-monary edema had severely depressed ejection frac-tions and no patient had a normal ejection fraction (>0.52).
Since January 1980, we have routinely obtained apredischarge radionuclide angiocardiogram for all sur-vivors of acute myocardial infarction. It became appar-ent that certain patients who had manifested pulmo-nary edema had an unexpectedly normal or only mildlydepressed ejection fraction at the time of discharge.This was distinctly in contrast to other reports.14' 11Possible explanations were either that acute transientabnormalities had occurred in left ventricular functionor that acute preload or afterload burdens had existedearly after the infarction. Because a good left ventricu-lar ejection fraction at discharge after a myocardial
From the Medical Service, San Francisco General Hospital MedicalCenter, and the Department of Medicine and the Cardiovascular Re-search Institute, University of California, San Francisco, San Francis-co, California.
Address for correspondence: Mary Ann Warnowicz, D. 0., 5G 1 Car-diology, San Francisco General Hospital, San Francisco.
Received April 9, 1982; revision accepted July 29, 1982.Circulation 67, No. 2, 1983.
816infarction generally predicts a good prognosis,' 1 wepostulated that patients with pulmonary edema whosepredischarge ejection fraction was within normal lim-its or only mildly depressed should have a goodprognosis.
Accordingly, we retrospectively evaluated the clini-cal course and determined the morbidity and mortalityof 39 consecutive patients with acute myocardial in-farction and pulmonary edema who survived for atleast 8 days in the hospital and underwent radionuclideangiocardiography.
Methods
PatientsBetween January 1980 and March 1981, 39 survi-
vors of acute myocardial infarction had overt pulmo-nary edema (Killip class IHI)'7 during the early postin-farction period and had predischarge ejection fractionsdetermined by radionuclide angiocardiography. Theywere 45-83 years old (mean 64.9 years). Twenty-eightpatients (72%) were men. The ejection fractions weredetermined 10 ± 2 days after infarction.
Acute myocardial infarction was diagnosed when atleast two of the following were present: a history oftypical prolonged chest pain, evolution of electrocar-diographic changes of acute transmural infarction orST-T changes and characteristic serial elevations ofserum enzymes (creatine kinase and MB fraction orlactic dehydrogenase isoenzymes).
Equilibrium-gated radionuclide angiocardiographywas performed after injection of 24 mCi of 99mTctagged to human serum albumin. Technetium albuminwas the sole agent used for the equilibrium radionu-clide angiocardiogram in the course of this study. La-
330
by guest on May 29, 2018
http://circ.ahajournals.org/D
ownloaded from
PROGNOSIS AFTER AMI/Warnowicz et al.
beling of red blood cells in vivo has now largely re-placed this technique. Despite somewhat greater liverand spleen activity, the usual background levels sub-tracted in our laboratory are not significantly greaterthan those for in vivo labeled red blood cells. Althoughmeasurement of the distribution of technetium indi-cates a highly variable proportion in hydrolized form,the ratio of free to bound is more constant and, in mostbatches, averaged 0.05 (range 0.003-0.20). Correla-tion with contrast angiography in our laboratory hasbeen performed with-the human serum albumin tech-nique and the results of the latter are consistently high-er, but the correlation coefficient is good (0.82). Im-ages were obtained in multiple projections, includingat least the 450 left anterior oblique, anterior and 300right anterior oblique, using a General Electric porta-ble scintillation camera with a "MED III" computer.After equilibration of the radionuclide in the bloodpool, 14 frames of 128 X 128 matrix image data,gated by the R wave of the ECG, were acquired fromthe first three-fourths of the cardiac cycle, acquiring200,000 counts/frame, which required 5-7 minutesper projection.
Left ventricular ejection fraction was measured withthe Muge program, which uses a semiautomatic edge-finding algorithm to place a region of interest on theborders of the left ventricle in each of the 14 frames ofthe left anterior oblique projection. The program alsoplaces a background region of interest over the nearbyleft lung, subtracts background from each frame anduses the curve of corrected count rate over the leftventricle to compute global left ventricular ejectionfraction. Operator intervention was rarely necessaryexcept, at times, in the case of a very large ventricle.Inter- and intraoperator tests of reproducibility of theejection fraction by this method in our laboratory hasbeen excellent. The method is essentially that of Mad-dahi et al.'8
The clinical records were reviewed for site of infarc-tion, history of myocardial infarction and hemody-namic measurements performed at the time of the acuteinfarction. The presence or absence of a regurgitantmurmur was noted. Patients who had clinically signifi-cant mitral or aortic regurgitation were not included inthe study.
Twenty-four of the 39 patients had hemodynamicmeasurements made within 12 hours of admission.Pulmonary arterial wedge pressure was measuredthrough a flow-directed, balloon-tipped catheter19 andcardiac output by thermodilution.20The patients were divided into two groups, based on
ejection fraction. Group A patients had an ejectionfraction > 0.45, and group B patients an ejection frac-tion , 0.45. During the late follow-up period (mean 9months, range 1-15 months), a new event was definedas death, reinfarction, recurrent angina (New YorkHeart Association functional class III or IV) or hospitaladmission for recurrent acute pulmonary edema.
Late follow-up data were obtained from clinic andhospital records in 36 of 39 patients; three patientswere followed by telephone interview only. All pa-
tients in groups A and B were managed medically, andcardiac catheterization or coronary arteriography wasnot performed unless unstable angina developed dur-ing follow-up.
Statistical analysis was performed using the t test forunpaired data or the chi-square method. The Z test wasused for differences in proportions. Survival was ana-lyzed by life-table method.2' Results are expressed asmean ± SD.
ResultsEjection Fractions
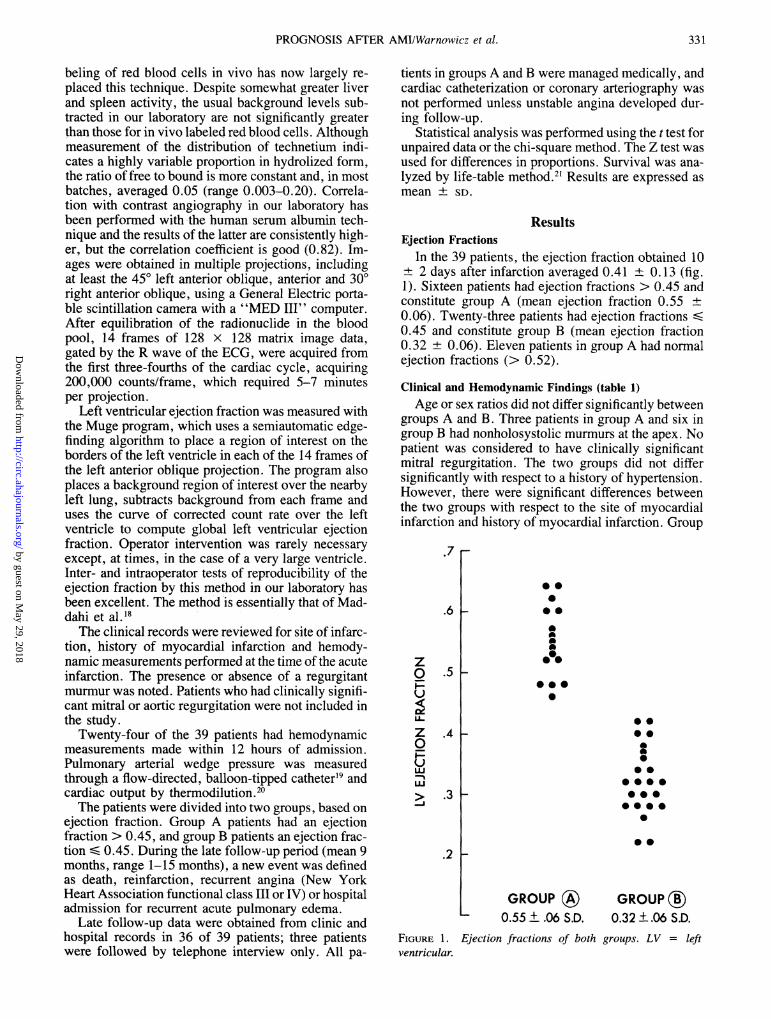
In the 39 patients, the ejection fraction obtained 10± 2 days after infarction averaged 0.41 ± 0.13 (fig.1). Sixteen patients had ejection fractions > 0.45 andconstitute group A (mean ejection fraction 0.55 ±0.06). Twenty-three patients had ejection fractions S0.45 and constitute group B (mean ejection fraction0.32 ± 0.06). Eleven patients in group A had normalejection fractions (> 0.52).
Clinical and Hemodynamic Findings (table 1)Age or sex ratios did not differ significantly between
groups A and B. Three patients in group A and six ingroup B had nonholosystolic murmurs at the' apex. Nopatient was considered to have clinically significantmitral regurgitation. The two groups did not differsignificantly with respect to a history of hypertension.However, there were significant differences betweenthe two groups with respect to the site of myocardialinfarction and history of myocardial infarction. Group
.7 r
.6 V
z01-U
z0-ULUJ1-J
0*0
0*
A0,0@0
.5 -
.410O0@0
00 0
*0 000000000
S
.3 F
0*.2 1
FIGURE 1.ventricular.
GROUP (®)0.55 + .06 S.D.
GROUP ®0.32 ±.06 S.D.
Ejection fractions of both groups. LV = left
331
by guest on May 29, 2018
http://circ.ahajournals.org/D
ownloaded from
VOL 67, No 2, FEBRUARY 1983
TABLE 1. ClinicalandHemodynamicCharacteristicsofPatientswith Myocardial Infarction and Acute Pulmonary Edema
Signifi-cance
Group A Group B ofVariable (EF > 0.45) (EF S 0.45) differenceClinical n = 16 n 23Age (years) 62.8±9.4 66.4±10.6 NS
Sex (male:female) 11:5 17:6 NSLocation of
infarctionAnterior 0 8
Anteroseptal 1 2p 0.005
Inferior 11 2Subendocardial 4 11
History ofinfarction 3 (19%) 19 (83%) p < 0.005
Hemodynamic n = 9 n - 15(obtained 6 ± 1.4
hours afteradmission)
Mean pulmonarycapillary wedgepressure (mm Hg) 16.8 ±2.0 17.4 ± 2.2 NS
Mean arterialpressure (mm Hg) 104± 12 96± 10 NS
Stroke work index(g-mIm2) 33.4± 2.4 23.4 ± 2.0 p < 0.005
Abbreviation: EF = ejection fraction.
B had a significantly greater incidence of anterior andsubendocardial infarctions, whereas group A predomi-nantly had inferior infarctions. Group B also had asignificantly higher percentage of previous myocardialinfarctions compared with group A. Hemodynamicmeasurements were obtained in nine of 16 patients ingroup A and 15 of 23 patients in group B. Acutepulmonary capillary wedge pressure and mean arterialpressures recorded on admission did not differ signifi-cantly. However, the calculated stroke work index wassignificantly greater in group A than in group B.Drug therapy in both groups was initiated with digi-
talis, diuretics or antihypertensive agents alone or incombination. Two patients in group A and three pa-tients in group B required early support of blood pres-sure with pressor agents. Initial hemodynamic valuestended to improve in both groups after therapy butwere not uniformly recorded. In general, patients ingroup A responded rapidly to therapy; 20 patients ingroup B were taking digitalis at the time of discharge,whereas only three in group A were receiving digitalistherapy.
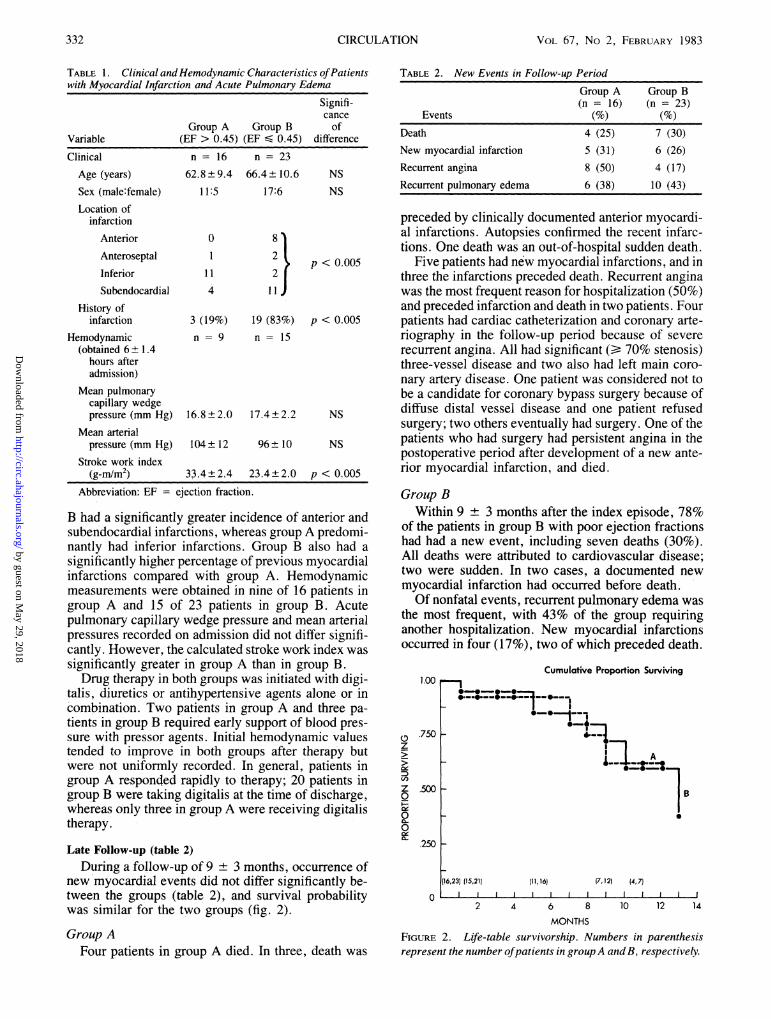
Late Follow-up (table 2)During a follow-up of 9 ± 3 months, occurrence of
new myocardial events did not differ significantly be-tween the groups (table 2), and survival probabilitywas similar for the two groups (fig. 2).
Group AFour patients in group A died. In three, death was
TABLE 2. New Events in Follow-up Period
Group A Group B(n = 16) (n = 23)
Events (%) (%)
Death 4 (25) 7 (30)New myocardial infarction 5 (31) 6 (26)Recurrent angina 8 (50) 4 (17)Recurrent pulmonary edema 6 (38) 10 (43)
preceded by clinically documented anterior myocardi-al infarctions. Autopsies confirmed the recent infarc-tions. One death was an out-of-hospital sudden death.
Five patients had new myocardial infarctions, and inthree the infarctions preceded death. Recurrent anginawas the most frequent reason for hospitalization (50%)and preceded infarction and death in two patients. Fourpatients had cardiac catheterization and coronary arte-riography in the follow-up period because of severerecurrent angina. All had significant (Da 70% stenosis)three-vessel disease and two also had left main coro-nary artery disease. One patient was considered not tobe a candidate for coronary bypass surgery because ofdiffuse distal vessel disease and one patient refusedsurgery; two others eventually had surgery. One of thepatients who had surgery had persistent angina in thepostoperative period after development of a new ante-rior myocardial infarction, and died.
Group BWithin 9 ± 3 months after the index episode, 78%
of the patients in group B with poor ejection fractionshad had a new event, including seven deaths (30%).All deaths were attributed to cardiovascular disease;two were sudden. In two cases, a documented newmyocardial infarction had occurred before death.Of nonfatal events, recurrent pulmonary edema was
the most frequent, with 43% of the group requiringanother hospitalization. New myocardial infarctionsoccurred in four (17%), two of which preceded death.
1.00
z
Ci)
z0
00a-
.7501
Cumulative Proportion Surviving
1
a~~~~~~
.-.-1---A* -6
_~~~~~-_ An
.5001
.250 _
0
(16,23) (15,21)
l
11,16) (7,12) (4, 7J1l
2 4 6 8 10 12 14
MONTHSFIGURE 2. Life-table survivorship. Numbers in parenthesisrepresent the number ofpatients in groupA andB, respectively.
332 CIRCULATION
by guest on May 29, 2018
http://circ.ahajournals.org/D
ownloaded from

PROGNOSIS AFTER AMI/Warnowicz et al.
Angina pectoris alone as a reason for readmission tothe hospital was least common (17%). Five patientsunderwent catheterization in the follow-up period be-cause of severe recurrent angina or left ventricularfailure and two eventually had surgery.
DiscussionThe patients in group A were remarkable in that they
had unexpectedly normal or only mildly depressed,ejection fractions (0.55 ± 0.06). This was in contrastto the study by Schelbert et al.,14 which showed thatpatients who had manifested overt pulmonary edemain the course of acute myocardial infarction had ejec-tion fractions that were severely depressed (0.33 +0.07). In their study, however, the ejection fractionswere measured less than 5 days after infarction, com-pared with more than 10 days in our study. Also,Schelbert et al. showed serial improvement in ejectionfractions for 27 patients (54%) during the early postin-farction period. Therefore, the higher mean ejectionfraction in our group could reflect the serial improve-ment described by Schelbert et al., although their datadid not reveal whether the subgroup of patients withovert pulmonary edema had a rate of improvementsimilar to that of the whole group.A significant number of survivors of acute myocar-
dial infarction with pulmonary edema have good resid-ual left ventricular function. Those who have goodresidual function (group A) are more likely to have hadtheir first myocardial infarction, predominantly inferi-or in location.Our patients could have had severe transient left
ventricular dysfunction earlier in the clinical course ofinfarction, as suggested by the serial studies of Schel-bert et al.14 The patients in our group were not studiedserially, but serial radionuclide ejection fractions wereperformed in two similar patients with acute inferiormyocardial infarction and pulmonary edema. Thesetwo patients showed marked improvement between theacute measurement of left ventricular ejection fraction(0.32 and 0.38 12 hours after admission) and the latevalue (0.52 and 0.54 10 days after admission).
The possibility that acute mitral insufficiency couldaccount entirely for this disparity in acute clinical pre-sentation and the predischarge ejection fraction is un-likely. The incidence of regurgitation murmurs was nogreater in group B than in group A, and no patient withclinically significant regurgitation was included. An-other explanation for transient myocardial dysfunctionmight be acute impedance or afterload burden, eitherbecause of increased sympathetic tone or acute hyper-tension. Acute afterload burdens are possible becausegroup A had a greater mean blood pressure, but indi-vidual variation was great. In addition, group B had asignificantly lower stroke work index that probablyindicated more depressed left ventricular function.The late prognosis after acute myocardial infarction
for any individual patient is influenced by many clini-cal and laboratory features. However, the left ventricu-lar ejection fraction is a powerful predictor of short-and long-term survival.8' 14, 16 Nelson et al.8 found that
ejection fraction was a more discriminant prognostica-tor than the severity of angiocardiographic coronarydisease or the clinical functional class. Schulze et al.22found that survivors of acute myocardial infarctionwith a predischarge radionuclide ejection fraction >0.40 had an overall good prognosis. The history of firstmyocardial infarction, inferior location and good re-sidual left ventricular function in group A patientsshould therefore characterize a low-risk subgroup ofsurvivors of acute myocardial infarction, even if theyhave a history of pulmonary edema. However, ourfollow-up of patients showed that morbidity and mor-tality were similarly high for those with normal andlow ejection fractions. More recently, some investiga-tors have shown that the resting left ventricular ejec-tion fraction alone does not completely predict out-come. Corbett et al.23 used exercise radionuclideangiograms to reflect permanently damaged myocardi-um as well as "myocardium at risk" during exercise.The exercise measurements proved to be better prog-nostic indicators. In addition, Silverman et al.24 stud-ied 42 patients within 15 hours of myocardial infarc-tion with thallium-201 scintigraphy and found that thisearly measurement of the perfusion defect was a sig-nificant prognostic indicator. This early study wasconsidered to reflect the permanently injured myocar-dium as well as that "at risk. " In our study, the pulmo-nary edema may also be reflecting "myocardium atrisk." Three of the patients in group A who died hadischemia and eventual infarction of the anterior wall ofthe left ventricle; two nonfatal infarctions were alsoanterior. In no case was arrhythmia a primary cause ofdeath. Thus, one explanation for the pulmonary edemaoccurring with the original inferior infarction is thatischemia of the anterior wall with consequent poorfunction had also occurred but resolved.
These data suggest that patients with myocardialinfarction and pulmonary edema form a high-riskgroup despite good resting left ventricular function.They have severe coronary artery disease and in amedically treated group have a significant incidence ofrecurrent transmural myocardial infarction and death.The identification of this high-risk subgroup of medi-cally managed patients with good residual left ventric-ular function is particularly important because they areexcellent candidates for surgical intervention.25
References1. Peel AAF, Semple T, Wang I, Lancaster WM, Dall JLG: A coro-
nary prognostic index for grading the severity of infarction. BrHeart J 24: 745, 1962
2. Moss AJ, DeCamilla J, Davis H, Bayer L: The early posthospitalphase of myocardial infarction. Prognostic stratification. Circula-tion 54: 58, 1976
3. Verdouw PD, Hagemeijer F, van Dorp WG, van der Vorm A,Hugenholtz PG: Short-term survival after acute myocardial infarc-tion predicted by hemodynamic parameters. Circulation 52: 413,1975
4. Norris RM, Brandt PWT, Caughey DE, Lee AJ, Scott PJ: A newcoronary prognostic index. Lancet 1: 274, 1969
5. Bigger JT Jr, Heller CA, Wenger TL, Weld FM: Risk stratificationafter acute myocardial infarction. Am J Cardiol 42: 202, 1978
6. White AE, Moore FJ, Marmorston J: Prognostic features of acute
333
by guest on May 29, 2018
http://circ.ahajournals.org/D
ownloaded from

VOL 67, No 2, FEBRUARY 1983
myocardial infarction in men. A one-year study at the Los AngelesCounty Hospital. Arch Intern Med 105: 859, 1960
7. Moss AJ, DeCamilla J, Engstrom F, Hoffman W, Odoroff C,Davis H: The posthospital phase of myocardial infarction. Identifi-cation of patients with increased mortality risk. Circulation 49:460, 1974
8. Nelson GR, Cohn PF, Gorlin R: Prognosis in medically-treatedcoronary artery disease. Influence of ejection fraction compared toother parameters. Circulation 52: 408, 1975
9. Shanoff HM, Little JA, Csima A, Yano R: Heart size and ten-yearsurvival after uncomplicated myocardial infarction. Am Heart J78: 608, 1969
10. Beard OW, Hipp HR, Robins M, Taylor JS, Ebert RV, Beran LG:Initial myocardial infarction among 503 veterans: five-year surviv-al. Am J Med 28: 871, 1960
11. Weinblatt E, Shapiro S, Frank CW, Sager RV: Prognosis of menafter first myocardial infarction: mortality and first recurrence inrelation to selected parameters. Am J Public Health 58: 1329, 1968
12. Geltman EM, Ehsani AA, Campbell MK, Schechtman K, RobertsR, Sobel BE: The influence of location and extent of myocardialinfarction on long-term ventricular dysrhythmia and mortality. Cir-culation 60: 805, 1979
13. Luria MH, Knoke JD, Margolis RM, Hendricks FH, Kuplic JB:Acute myocardial infarction: prognosis after recovery. Ann InternMed 85: 561, 1976
14. Schelbert HR, Henning H, Ashburn WL, Verbra JW, Karliner JS,O'Rourke RA: Serial measurements of left ventricular ejectionfraction by radionuclide angiography early and later after myocar-dial infarction. Am J Cardiol 38: 407, 1976
15. Rigo P, Murray M, Strauss HW, Taylor D, Kelly D, Weisfeldt M,Pitt B: Left ventricular function in myocardial infarction evaluatedby gated scintiphotography. Circulation 50: 678, 1974
16. Murray JA, Chinn N, Peterson DR: Influence of left ventricular
function on early prognosis in atherosclerotic heart disease. Am JCardiol 33: 159, 1974
17. Killip T III, Kimball JT: Treatment of myocardial infarction in acoronary care unit. A two year experience with 250 patients. Am JCardiol 20: 457, 1967
18. Maddahi J, Berman DS, Diamond GA, Shah PK, Gray RJ, Forres-ter JS: Evaluation of left ventricular ejection fraction and segmentalwall motion by multiple-gated equilibrium cardiac blood pool scin-tigraphy. In Computer Techniques in Cardiology, edited by CadyLD. New York, Marcel Dekker, 1979
19. Swan HJC, Ganz W, Forrester J, Marcus H, Diamond G, ChonetteD: Catheterization of the heart in man with use of a flow-directedballoon-tipped catheter. N Engl J Med 283: 447, 1970
20. Ganz W, Swan HJC: Measurement of blood flow by thermodilu-tion. Am J Cardiol 29: 241, 1972
21. Lee ET: Statistical Methods for Survival Data Analysis. Belmont,CA, Wadsworth, 1980, p 88
22. Schulze RA Jr, Strauss HW, Pitt B: Sudden death in the yearfollowing myocardial infarction. Relation to ventricular prematurecontractions in the late hospital phase and left ventricular ejectionfraction. Am J Med 62: 192, 1977
23. Corbett JR, Dehmer GJ, Lewis SE, Woodward W, Henderson E,Parkey RW, Blomqvist CG, Willerson JT: The prognostic value ofsubmaximal exercise testing with radionuclide ventriculographybefore hospital discharge in patients with recent myocardial infarc-tion. Circulation 64: 535, 1981
24. Silverman KJ, Becker LC, Bulkley BH, Burow RD, Mellits ED,Kallman CH, Weisfeldt ML: Value of early thallium-201 scinti-graphy for predicting mortality in patients with acute myocardialinfarction. Circulation 61: 996, 1980
25. Cohn PF, Gorlin R, Cohn LH, Collins JJ Jr: Left ventricular ejec-tion fraction as a prognostic guide in surgical treatment of coronaryand valvular heart disease. Am J Cardiol 34: 136, 1974
334 CIRCULATION
by guest on May 29, 2018
http://circ.ahajournals.org/D
ownloaded from

M A Warnowicz, H Parker and M D Cheitlinacute myocardial infarction.
Prognosis of patients with acute pulmonary edema and normal ejection fraction after
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1983 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.67.2.330
1983;67:330-334Circulation.
http://circ.ahajournals.org/content/67/2/330the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on May 29, 2018
http://circ.ahajournals.org/D
ownloaded from