Embed Size (px)
Citation preview

Psoriatic Arthritis: the Role of Psoriatic Arthritis: the Role of Radiologic Assessment in Radiologic Assessment in
Diagnosis and ManagementDiagnosis and Management
Stephanie W. Hu, HMS IVStephanie W. Hu, HMS IVBIDMC Department of RadiologyBIDMC Department of Radiology
August 25, 2008August 25, 2008

OverviewOverview
Patient ACPatient ACPsoriatic arthritis (Psoriatic arthritis (PsAPsA))
EpidemiologyEpidemiologyPathogenesisPathogenesisClinical and radiographic featuresClinical and radiographic featuresDxDx and and DDxDDx
Role of imaging in Role of imaging in PsAPsAPatient ACPatient ACClassic radiographic manifestationsClassic radiographic manifestationsOther modalitiesOther modalities
Summary Summary

Patient ACPatient AC
24 year24 year--old gentleman referred to BWH Center for Skin old gentleman referred to BWH Center for Skin and Related Musculoskeletal Diseasesand Related Musculoskeletal Diseases>10>10--year year h/oh/o severe severe cutaneouscutaneous psoriasis and 8psoriasis and 8--year year h/oh/oarthritisarthritisFailed topical Rx, Failed topical Rx, plaquenilplaquenil, and MTX; lost insurance at , and MTX; lost insurance at age 18 age 18 persisted on Tylenol and Ibuprofen for painpersisted on Tylenol and Ibuprofen for painNow complains of flaring psoriasis, inability to bear Now complains of flaring psoriasis, inability to bear weight on his L foot x 3 weight on his L foot x 3 mosmos, and inability to work due , and inability to work due to involvement of L handto involvement of L handH/o anxiety and depression H/o anxiety and depression

Patient AC: Patient AC: CutaneousCutaneous
ManifestationsManifestations
Courtesy of A. Qureshi, BWH Dermatology

Patient AC: Patient AC: CutaneousCutaneous
ManifestationsManifestations
Courtesy of A. Qureshi, BWH Dermatology

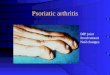
Patient AC: HandsPatient AC: Hands
Courtesy of A. Qureshi, BWH Dermatology

Patient AC: FeetPatient AC: Feet
Courtesy of A. Qureshi, BWH Dermatology

PsAPsA: Epidemiology: Epidemiology
Psoriasis is estimated to affect at least 7 million people Psoriasis is estimated to affect at least 7 million people in the United Statesin the United StatesBetween 5% and 42% of this group will develop Between 5% and 42% of this group will develop PsAPsAPsAPsA significantly impacts significantly impacts healthhealth--related quality of liferelated quality of life
There is greater role limitations associated with There is greater role limitations associated with PsAPsA than RA than RA due to emotional problems and more bodily paindue to emotional problems and more bodily pain
PsAPsA is a lifelong condition and carries is a lifelong condition and carries ~60% higher risk ~60% higher risk of mortalityof mortality relative to the general population, relative to the general population, correlated w/ radiologic damage at presentationcorrelated w/ radiologic damage at presentationThe course of The course of PsAPsA is unpredictable, with periods of is unpredictable, with periods of relapse and remissionrelapse and remission

PsAPsA: Pathogenesis: Pathogenesis
Genetic factors: Genetic factors: susceptibility genes, HLAsusceptibility genes, HLA--B27 and others (B27 and others (--B17, B17, --Cw6, Cw6, --DR4, DR4, --DR7)DR7)Environmental factors: Environmental factors: viral (HIV) and viral (HIV) and bacterial infections implicated as triggersbacterial infections implicated as triggersImmunologic factors:Immunologic factors:
Deposition of immune complexesDeposition of immune complexesAgents that inhibit TAgents that inhibit T--cell function or cell function or proliferation improve proliferation improve PsAPsAClonalClonal and and oligoclonaloligoclonal expansions of expansions of both CD8+ and CD4+ T cells in skin both CD8+ and CD4+ T cells in skin and and synoviumsynoviumElevated levels of Elevated levels of TNFTNF in serum and in serum and synovial fluid synovial fluid cytokines induce cytokines induce aactivation and proliferation of ctivation and proliferation of keratinocyteskeratinocytes and synovial fibroblastsand synovial fibroblasts (Mease
and Goffe, 2005)

PsAPsA: Clinical Features: Clinical FeaturesPsAPsA belongs to the belongs to the seronegativeseronegative spondyloarthropathiesspondyloarthropathies,, which share which share characteristics:characteristics:
Asymmetric peripheral arthritisAsymmetric peripheral arthritisAxial involvement (esp. Axial involvement (esp. sacroiliitissacroiliitis))The usual absence of RFThe usual absence of RFUnique radiologic featuresUnique radiologic featuresA greater degree of involvement of malesA greater degree of involvement of malesDistinctive HLA patternsDistinctive HLA patterns
In addition, In addition, PsAPsA also demonstrates:also demonstrates:EnthesitisEnthesitisDactylitisDactylitis (up to 30% of pts) (up to 30% of pts) ““ssausage ausage digitsdigits””Joint deformities, Joint deformities, subluxationssubluxationsPsoriatic skin lesionsPsoriatic skin lesions
Moll and WrightMoll and Wright’’s s Classification of Classification of PsAPsA1. 1. DIP joint predominant2. Arthritis mutilans3. Polyarticular symmetrical (RA-like)4. Oligoarticular asymmetrical5. Spondylitis and sacroiliitis

PsAPsA: Radiographic Features: Radiographic Features
OsteolysisOsteolysis (bony erosion)(bony erosion)Esp. Esp. paramarginalparamarginal erosionserosions““PencilPencil--inin--cupcup”” deformitydeformity
Loss of joint spaceLoss of joint spaceEnthesitisEnthesitisAsymmetric Asymmetric sacroiliitissacroiliitisAnkylosisAnkylosisJoint Joint subluxationsubluxationPeriostitisPeriostitisSpur formation, Spur formation, ““whiskeringwhiskering””
(Jacobson et al., 2008)
** Radiographs are the study of choice for Dx
of PsAdue to cost-effective detection of bony changes (erosions and proliferation)**
PACS, BIDMC
Plain film of R foot, lateral view
Plain film of pelvis, AP view: asymmetric sacroiliitis
spur

LetLet’’s Review Synovial Joint Anatomy!s Review Synovial Joint Anatomy!
f = joint fluid, c = articular
cartilage
Marginal erosions
(arrows) are seen where subchondral
bone plate is exposed to intraarticular
synovitis.
(Jacobson et al, 2008)
Diagram of normal and inflamed synovial joint: Plain film of IP joint in finger, AP view:

Patient AC: Plain Film of HandsPatient AC: Plain Film of HandsCentricity, BWH
Frontal views: joint space narrowing;
subluxation,
pencil-in-cup deformities,
erosions

Patient AC: Plain Film of FeetPatient AC: Plain Film of FeetCentricity, BWH
Frontal views: pencil-in-cup deformities

PsAPsA: Diagnosis and Differential Diagnosis: Diagnosis and Differential Diagnosis
Signs and Signs and SxSx PsAPsA RARA OAOA ASAS
Peripheral Peripheral dzdz AsymmetricAsymmetric SymmetricSymmetric VariesVaries ––
DIP DIP involvementinvolvement
+ + –– +, +, HeberdenHeberden
nodesnodes––
SacroiliitisSacroiliitis AsymmetricAsymmetric –– –– SymmetricSymmetric
StiffnessStiffness Peripheral Peripheral joints, some joints, some spine, morningspine, morning
MorningMorning With activityWith activity Significant spineSignificant spine
EnthesitisEnthesitis + + –– –– ++
(Adapted from Mease
and Goffe, 2005)

PsAPsA RARA OAOA ASAS
Radiographic Radiographic changeschanges
Erosions, Erosions, paramarginalparamarginal, , absence of absence of osteopeniaosteopenia, , pencilpencil--inin--cup, cup, asymmetric asymmetric syndesmosyndesmo--
phytesphytes
Erosions, Erosions, synovitissynovitis, , periarticularperiarticular
osteopeniaosteopenia
OsteophytesOsteophytes, , subchondralsubchondral
sclerosis and sclerosis and cystscysts
Squaring of Squaring of vertebral bodies, vertebral bodies, symmetric symmetric syndesmosyndesmo--
phytesphytes, spinal , spinal osteopeniaosteopenia
Gender biasGender bias 1:1, male to 1:1, male to femalefemale
3:1, female to 3:1, female to malemale
Hand and toe Hand and toe OA more OA more frequent in frequent in femalesfemales
3:1, male to 3:1, male to femalefemale
RFRF –– + + –– ––
HLA HLA assoasso.. B27, Cw6B27, Cw6 DR4DR4 –– B27B27
ExtraarticularExtraarticular
manifestationsmanifestationsOnychodystroOnychodystro--
phyphy, , iritisiritis, PSO, PSONodules, Nodules, vascuvascu--
litislitis, renal , renal dzdz–– ––

Classic Radiographic Features of Classic Radiographic Features of PsAPsA: Spine: Spine
PACS, BIDMC
BrighamRAD
Compare with a non-pathological C-spine:
Companion patient #1: Companion patient #2:
Plain film of thoracolumbar spine, AP view Plain film of cervical spine, lateral view
Ankylosis
Asymmetric,syndesmophytes

Classic Radiographic Features of Classic Radiographic Features of PsAPsA: Pelvis: Pelvis
PACS, BIDMC
“Whiskering”
Companion patient #3: Companion patient #4:
Plain film of pelvis, AP viewPlain film of pelvis, AP view
Asymmetric
Sacroiliitis
Syndesmophyte

Patient AC: TreatmentPatient AC: TreatmentAC was started on AC was started on etanerceptetanercept ((EnbrelEnbrel)) 50 mg SC twice per week50 mg SC twice per weekSxSx improved in just improved in just 2 months2 months: began to regain motion of some of : began to regain motion of some of his L fingers and toes, able to make a fist with L hand, and almhis L fingers and toes, able to make a fist with L hand, and almost ost completely able to bear weight on his L footcompletely able to bear weight on his L footHis skin is completely clear except for 2 dimeHis skin is completely clear except for 2 dime--sized spots on the sized spots on the back of the R legback of the R legF/u plain films reveal no radiographic progression of joint F/u plain films reveal no radiographic progression of joint dzdzHis CRP (60) and ESR (52.2) are now WNLHis CRP (60) and ESR (52.2) are now WNL
Started etanercept
Working full-
time, could walk around mall
Shoveled snow!
Could run up steps to house, got 2nd
job as crossing guard
0 3 4 6 8 Months

PsAPsA: Role of Plain Films in Clinical Trials: Role of Plain Films in Clinical Trials
Modified Sharp Scoring Method:Modified Sharp Scoring Method: assessment of assessment of baseline and post-treatment disease severity
(Mease
and Goffe, 2005)
Etanercept: showed inhibition of radiographic disease progression com-pared to placebo at 1 year FDA approval for PsA
in 2002

PsAPsA: Role of Ultrasound and Magnetic : Role of Ultrasound and Magnetic Resonance ImagingResonance Imaging
U/S is not as validated for U/S is not as validated for PsAPsA as it is for RAas it is for RAUseful for Useful for enthesitisenthesitis, joint effusions, synovial proliferation, and erosions, joint effusions, synovial proliferation, and erosionsDoppler U/S can help detect hyperemia as an indirect sign of Doppler U/S can help detect hyperemia as an indirect sign of inflammation and differentiate acute synovial proliferation frominflammation and differentiate acute synovial proliferation from effusioneffusion
U/S and MRI are more sensitive to inflammatory and U/S and MRI are more sensitive to inflammatory and destructive changes than radiographs and clinical examdestructive changes than radiographs and clinical examMRI can detect inflammation and bone destruction in joints MRI can detect inflammation and bone destruction in joints earlier than projection radiography in earlier than projection radiography in PsAPsAMRI has also revealed evidence of subclinical arthritis in a larMRI has also revealed evidence of subclinical arthritis in a large ge proportion of pts with psoriasis alone proportion of pts with psoriasis alone PsAPsA could be much could be much more common than previously suspectedmore common than previously suspected

(Kleinert, Feuchtenberger, Kneitz, Tony, 2007)
PsA: Role of Ultrasound
Inflammation
Synovial proliferation
Companion patient #5: Ultrasound with color Doppler of MCP joint, dorsal longitudinal view

(McQueen, Lassere, Ostergaard, 2006)
A) Short tau inversion recovery (STIR) B) T1-weighted pre-contrast C) T1-weighted post-contrastsagittal
view
sagittal
view sagittal
view
PsA: Role of Magnetic Resonance Imaging
Companion patient #6: enthesitis, synovitis, bony erosions in ankle region

SummarySummary
PsAPsA has been defined as a unique, progressive, has been defined as a unique, progressive, and often destructive form of and often destructive form of seronegativeseronegativeinflammatory arthritis associated with psoriasis inflammatory arthritis associated with psoriasis Radiologic imaging plays a key role in the Radiologic imaging plays a key role in the diagnosis and management of diagnosis and management of PsAPsA ptsptsU/S and MRI may be increasingly utilized as U/S and MRI may be increasingly utilized as sensitive tools for assessment of disease sensitive tools for assessment of disease progression and in clinical trialsprogression and in clinical trials

AcknowledgementsAcknowledgements
Dr. Dr. AbrarAbrar A. A. QureshiQureshiBrigham and WomenBrigham and Women’’s Hospital, Dermatologys Hospital, Dermatology
Dr. Jim S. WuDr. Jim S. WuBeth Israel Deaconess Medical Center, RadiologyBeth Israel Deaconess Medical Center, Radiology
Dr. Ferris HallDr. Ferris HallBeth Israel Deaconess Medical Center, RadiologyBeth Israel Deaconess Medical Center, Radiology
Dr. Gillian LiebermanDr. Gillian LiebermanBeth Israel Deaconess Medical Center, RadiologyBeth Israel Deaconess Medical Center, Radiology
Maria Maria LevantakisLevantakisBeth Israel Deaconess Medical Center, RadiologyBeth Israel Deaconess Medical Center, Radiology

ReferencesReferences1.1.
MeaseMease
P, P, GoffeGoffe
BS. Diagnosis and treatment of psoriatic arthritis. BS. Diagnosis and treatment of psoriatic arthritis. J Am J Am AcadAcad
DermatolDermatol
2005; 52: 12005; 52: 1--19.19.2.2.
GladmanGladman
DD< DD< AntoniAntoni
C, C, MeaseMease
P, Clegg DO, Nash P. Psoriatic arthritis: P, Clegg DO, Nash P. Psoriatic arthritis: epidemiology, clinical features, course, and outcome. epidemiology, clinical features, course, and outcome. Ann Rheum Ann Rheum DisDis
2005; 64 2005; 64 ((SupplSuppl
II): ii14II): ii14--ii17.ii17.3.3.
HelliwellHelliwell
PS, Taylor WJ. Classification and diagnostic criteria for psorPS, Taylor WJ. Classification and diagnostic criteria for psoriatic arthritis. iatic arthritis. Ann Rheum Ann Rheum DisDis
2005; 64 (2005; 64 (SupplSuppl
II): ii3II): ii3--ii8.ii8.4.4.
Jacobson JA, Jacobson JA, GirishGirish
G, G, JianJian
Y, Y, ResnickResnick
D. Radiographic evaluation of arthritis: D. Radiographic evaluation of arthritis: inflammatory conditions. inflammatory conditions. Radiology Radiology 2008; 248: 3782008; 248: 378--389.389.
5.5.
KleinertKleinert
S, S, FeuchtenbergerFeuchtenberger
M, M, KneitzKneitz
C, Tony HP. Psoriatic arthritis: clinical C, Tony HP. Psoriatic arthritis: clinical spectrum and diagnostic procedures. spectrum and diagnostic procedures. ClinClin
DermatolDermatol
2007; 25: 5192007; 25: 519--523.523.6.6.
WiellWiell
C, C, SzkudlarekSzkudlarek
M, M, HasselquistHasselquist
M, M, MollerMoller
JM, JM, VestergaardVestergaard
A, A, NorregaardNorregaard
J, J, TerslevTerslev
L, L, OstergaardOstergaard
M. M. UltrasonographyUltrasonography, magnetic resonance imaging, , magnetic resonance imaging, radiography, and clinical assessment of inflammatory and destrucradiography, and clinical assessment of inflammatory and destructive changes in tive changes in fingers and toes of patients with psoriatic arthritis. fingers and toes of patients with psoriatic arthritis. ArthArth
Res Res TherTher
2007; 9: 1192007; 9: 119--132.132.7.7.
McQueen F, McQueen F, LassereLassere
M, M, OstergaardOstergaard
M. Magnetic resonance imaging in psoriatic M. Magnetic resonance imaging in psoriatic arthritis: a review of the literature. arthritis: a review of the literature. ArthArth
Res and Res and TherTher
2006; 8: 2072006; 8: 207--215.215.8.8.
Weiner SM, Weiner SM, JurenzJurenz
S, S, UhlUhl
M, LangeM, Lange--NoldeNolde
A, A, WarnatzWarnatz
K, Peter HH, Walker UA. K, Peter HH, Walker UA. UltrasonographyUltrasonography
in the assessment of peripheral joint involvement in psoriatic in the assessment of peripheral joint involvement in psoriatic arthritis. arthritis. ClinClin
RheumatolRheumatol
2008; 27: 9832008; 27: 983--989.989.

Thank you!Thank you!