Embed Size (px)
Citation preview
PDPM Bulletin PT & OT Classification
019
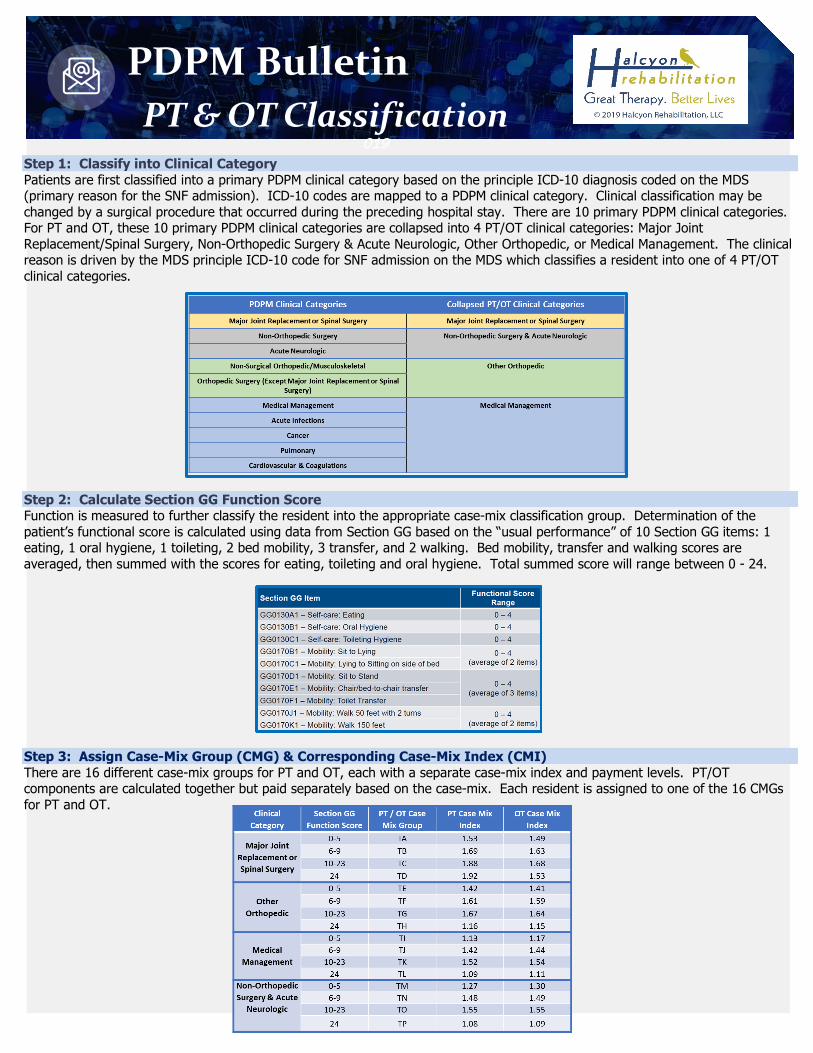
Step 1: Classify into Clinical Category Patients are first classified into a primary PDPM clinical category based on the principle ICD-10 diagnosis coded on the MDS (primary reason for the SNF admission). ICD-10 codes are mapped to a PDPM clinical category. Clinical classification may be changed by a surgical procedure that occurred during the preceding hospital stay. There are 10 primary PDPM clinical categories. For PT and OT, these 10 primary PDPM clinical categories are collapsed into 4 PT/OT clinical categories: Major Joint Replacement/Spinal Surgery, Non-Orthopedic Surgery & Acute Neurologic, Other Orthopedic, or Medical Management. The clinical reason is driven by the MDS principle ICD-10 code for SNF admission on the MDS which classifies a resident into one of 4 PT/OT clinical categories. Step 2: Calculate Section GG Function Score Function is measured to further classify the resident into the appropriate case-mix classification group. Determination of the patient’s functional score is calculated using data from Section GG based on the “usual performance” of 10 Section GG items: 1 eating, 1 oral hygiene, 1 toileting, 2 bed mobility, 3 transfer, and 2 walking. Bed mobility, transfer and walking scores are averaged, then summed with the scores for eating, toileting and oral hygiene. Total summed score will range between 0 - 24. Step 3: Assign Case-Mix Group (CMG) & Corresponding Case-Mix Index (CMI) There are 16 different case-mix groups for PT and OT, each with a separate case-mix index and payment levels. PT/OT components are calculated together but paid separately based on the case-mix. Each resident is assigned to one of the 16 CMGs for PT and OT.
PDPM Bulletin SLP Classification
019
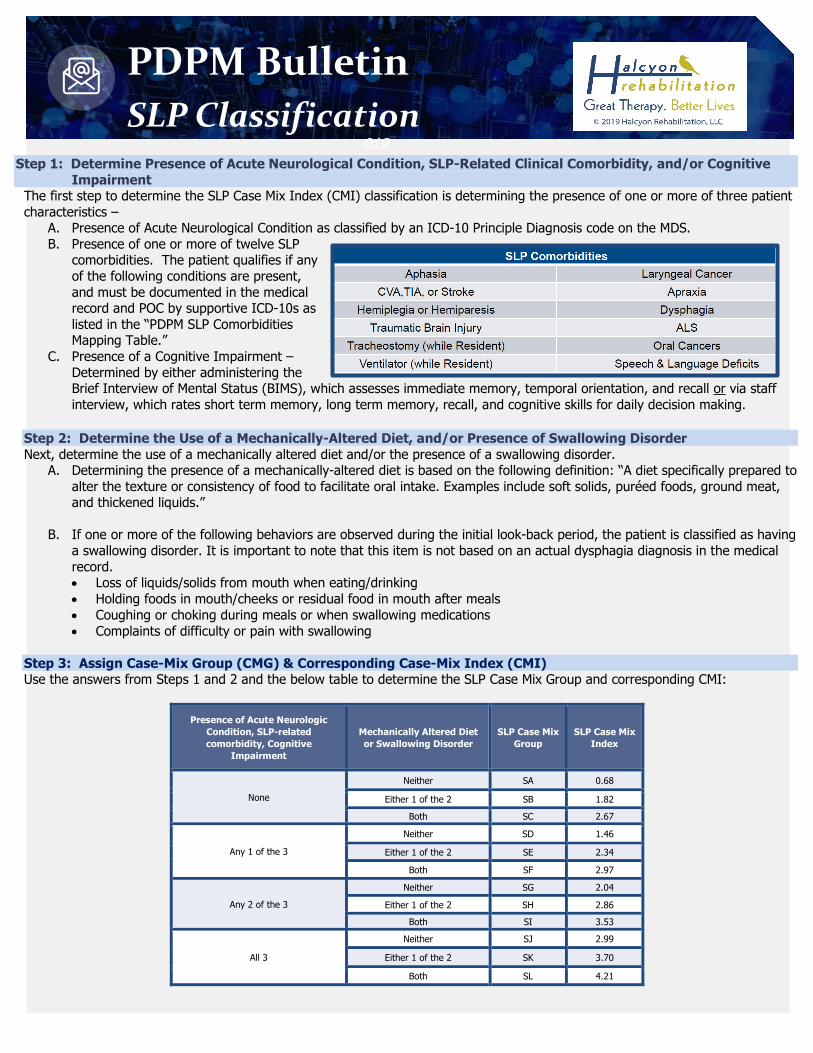
Step 1: Determine Presence of Acute Neurological Condition, SLP-Related Clinical Comorbidity, and/or Cognitive Impairment
The first step to determine the SLP Case Mix Index (CMI) classification is determining the presence of one or more of three patient characteristics –
A. Presence of Acute Neurological Condition as classified by an ICD-10 Principle Diagnosis code on the MDS. B. Presence of one or more of twelve SLP
comorbidities. The patient qualifies if any of the following conditions are present, and must be documented in the medical record and POC by supportive ICD-10s as listed in the “PDPM SLP Comorbidities Mapping Table.”
C. Presence of a Cognitive Impairment – Determined by either administering the Brief Interview of Mental Status (BIMS), which assesses immediate memory, temporal orientation, and recall or via staff interview, which rates short term memory, long term memory, recall, and cognitive skills for daily decision making.
Step 2: Determine the Use of a Mechanically-Altered Diet, and/or Presence of Swallowing Disorder Next, determine the use of a mechanically altered diet and/or the presence of a swallowing disorder.
A. Determining the presence of a mechanically-altered diet is based on the following definition: “A diet specifically prepared to alter the texture or consistency of food to facilitate oral intake. Examples include soft solids, puréed foods, ground meat, and thickened liquids.”
B. If one or more of the following behaviors are observed during the initial look-back period, the patient is classified as having
a swallowing disorder. It is important to note that this item is not based on an actual dysphagia diagnosis in the medical record. • Loss of liquids/solids from mouth when eating/drinking • Holding foods in mouth/cheeks or residual food in mouth after meals • Coughing or choking during meals or when swallowing medications • Complaints of difficulty or pain with swallowing
Step 3: Assign Case-Mix Group (CMG) & Corresponding Case-Mix Index (CMI) Use the answers from Steps 1 and 2 and the below table to determine the SLP Case Mix Group and corresponding CMI:
Presence of Acute Neurologic Condition, SLP-related comorbidity, Cognitive
Impairment
Mechanically Altered Diet or Swallowing Disorder
SLP Case Mix Group
SLP Case Mix Index
None
Neither SA 0.68
Either 1 of the 2 SB 1.82
Both SC 2.67
Any 1 of the 3
Neither SD 1.46
Either 1 of the 2 SE 2.34
Both SF 2.97
Any 2 of the 3
Neither SG 2.04
Either 1 of the 2 SH 2.86
Both SI 3.53
All 3
Neither SJ 2.99
Either 1 of the 2 SK 3.70
Both SL 4.21
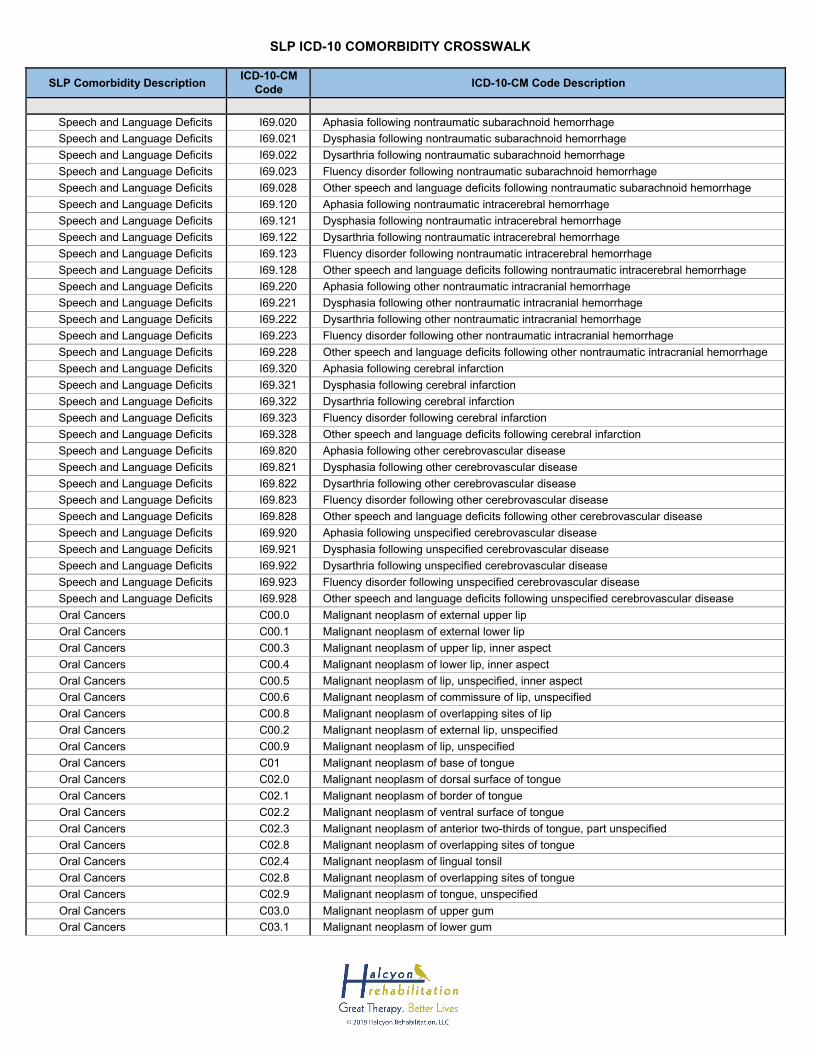
SLP ICD-10 COMORBIDITY CROSSWALK
SLP Comorbidity Description ICD-10-CM
Code ICD-10-CM Code Description
Speech and Language Deficits I69.020 Aphasia following nontraumatic subarachnoid hemorrhage Speech and Language Deficits I69.021 Dysphasia following nontraumatic subarachnoid hemorrhage Speech and Language Deficits I69.022 Dysarthria following nontraumatic subarachnoid hemorrhage Speech and Language Deficits I69.023 Fluency disorder following nontraumatic subarachnoid hemorrhage Speech and Language Deficits I69.028 Other speech and language deficits following nontraumatic subarachnoid hemorrhage Speech and Language Deficits I69.120 Aphasia following nontraumatic intracerebral hemorrhage Speech and Language Deficits I69.121 Dysphasia following nontraumatic intracerebral hemorrhage Speech and Language Deficits I69.122 Dysarthria following nontraumatic intracerebral hemorrhage Speech and Language Deficits I69.123 Fluency disorder following nontraumatic intracerebral hemorrhage Speech and Language Deficits I69.128 Other speech and language deficits following nontraumatic intracerebral hemorrhage Speech and Language Deficits I69.220 Aphasia following other nontraumatic intracranial hemorrhage Speech and Language Deficits I69.221 Dysphasia following other nontraumatic intracranial hemorrhage Speech and Language Deficits I69.222 Dysarthria following other nontraumatic intracranial hemorrhage Speech and Language Deficits I69.223 Fluency disorder following other nontraumatic intracranial hemorrhage Speech and Language Deficits I69.228 Other speech and language deficits following other nontraumatic intracranial hemorrhage Speech and Language Deficits I69.320 Aphasia following cerebral infarction Speech and Language Deficits I69.321 Dysphasia following cerebral infarction Speech and Language Deficits I69.322 Dysarthria following cerebral infarction Speech and Language Deficits I69.323 Fluency disorder following cerebral infarction Speech and Language Deficits I69.328 Other speech and language deficits following cerebral infarction Speech and Language Deficits I69.820 Aphasia following other cerebrovascular disease Speech and Language Deficits I69.821 Dysphasia following other cerebrovascular disease Speech and Language Deficits I69.822 Dysarthria following other cerebrovascular disease Speech and Language Deficits I69.823 Fluency disorder following other cerebrovascular disease Speech and Language Deficits I69.828 Other speech and language deficits following other cerebrovascular disease Speech and Language Deficits I69.920 Aphasia following unspecified cerebrovascular disease Speech and Language Deficits I69.921 Dysphasia following unspecified cerebrovascular disease Speech and Language Deficits I69.922 Dysarthria following unspecified cerebrovascular disease Speech and Language Deficits I69.923 Fluency disorder following unspecified cerebrovascular disease Speech and Language Deficits I69.928 Other speech and language deficits following unspecified cerebrovascular disease Oral Cancers C00.0 Malignant neoplasm of external upper lip Oral Cancers C00.1 Malignant neoplasm of external lower lip Oral Cancers C00.3 Malignant neoplasm of upper lip, inner aspect Oral Cancers C00.4 Malignant neoplasm of lower lip, inner aspect Oral Cancers C00.5 Malignant neoplasm of lip, unspecified, inner aspect Oral Cancers C00.6 Malignant neoplasm of commissure of lip, unspecified Oral Cancers C00.8 Malignant neoplasm of overlapping sites of lip Oral Cancers C00.2 Malignant neoplasm of external lip, unspecified Oral Cancers C00.9 Malignant neoplasm of lip, unspecified Oral Cancers C01 Malignant neoplasm of base of tongue Oral Cancers C02.0 Malignant neoplasm of dorsal surface of tongue Oral Cancers C02.1 Malignant neoplasm of border of tongue Oral Cancers C02.2 Malignant neoplasm of ventral surface of tongue Oral Cancers C02.3 Malignant neoplasm of anterior two-thirds of tongue, part unspecified Oral Cancers C02.8 Malignant neoplasm of overlapping sites of tongue Oral Cancers C02.4 Malignant neoplasm of lingual tonsil Oral Cancers C02.8 Malignant neoplasm of overlapping sites of tongue Oral Cancers C02.9 Malignant neoplasm of tongue, unspecified Oral Cancers C03.0 Malignant neoplasm of upper gum Oral Cancers C03.1 Malignant neoplasm of lower gum
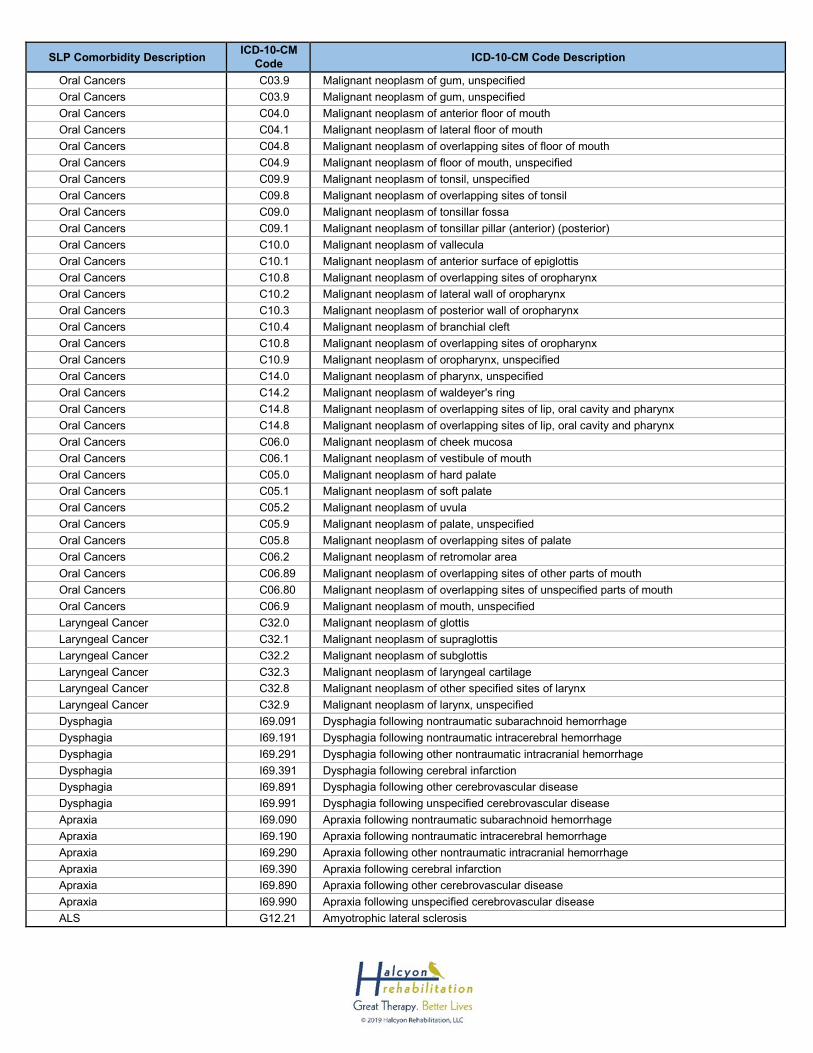
SLP Comorbidity Description ICD-10-CM Code ICD-10-CM Code Description
Oral Cancers C03.9 Malignant neoplasm of gum, unspecified Oral Cancers C03.9 Malignant neoplasm of gum, unspecified Oral Cancers C04.0 Malignant neoplasm of anterior floor of mouth Oral Cancers C04.1 Malignant neoplasm of lateral floor of mouth Oral Cancers C04.8 Malignant neoplasm of overlapping sites of floor of mouth Oral Cancers C04.9 Malignant neoplasm of floor of mouth, unspecified Oral Cancers C09.9 Malignant neoplasm of tonsil, unspecified Oral Cancers C09.8 Malignant neoplasm of overlapping sites of tonsil Oral Cancers C09.0 Malignant neoplasm of tonsillar fossa Oral Cancers C09.1 Malignant neoplasm of tonsillar pillar (anterior) (posterior) Oral Cancers C10.0 Malignant neoplasm of vallecula Oral Cancers C10.1 Malignant neoplasm of anterior surface of epiglottis Oral Cancers C10.8 Malignant neoplasm of overlapping sites of oropharynx Oral Cancers C10.2 Malignant neoplasm of lateral wall of oropharynx Oral Cancers C10.3 Malignant neoplasm of posterior wall of oropharynx Oral Cancers C10.4 Malignant neoplasm of branchial cleft Oral Cancers C10.8 Malignant neoplasm of overlapping sites of oropharynx Oral Cancers C10.9 Malignant neoplasm of oropharynx, unspecified Oral Cancers C14.0 Malignant neoplasm of pharynx, unspecified Oral Cancers C14.2 Malignant neoplasm of waldeyer's ring Oral Cancers C14.8 Malignant neoplasm of overlapping sites of lip, oral cavity and pharynx Oral Cancers C14.8 Malignant neoplasm of overlapping sites of lip, oral cavity and pharynx Oral Cancers C06.0 Malignant neoplasm of cheek mucosa Oral Cancers C06.1 Malignant neoplasm of vestibule of mouth Oral Cancers C05.0 Malignant neoplasm of hard palate Oral Cancers C05.1 Malignant neoplasm of soft palate Oral Cancers C05.2 Malignant neoplasm of uvula Oral Cancers C05.9 Malignant neoplasm of palate, unspecified Oral Cancers C05.8 Malignant neoplasm of overlapping sites of palate Oral Cancers C06.2 Malignant neoplasm of retromolar area Oral Cancers C06.89 Malignant neoplasm of overlapping sites of other parts of mouth Oral Cancers C06.80 Malignant neoplasm of overlapping sites of unspecified parts of mouth Oral Cancers C06.9 Malignant neoplasm of mouth, unspecified Laryngeal Cancer C32.0 Malignant neoplasm of glottis Laryngeal Cancer C32.1 Malignant neoplasm of supraglottis Laryngeal Cancer C32.2 Malignant neoplasm of subglottis Laryngeal Cancer C32.3 Malignant neoplasm of laryngeal cartilage Laryngeal Cancer C32.8 Malignant neoplasm of other specified sites of larynx Laryngeal Cancer C32.9 Malignant neoplasm of larynx, unspecified Dysphagia I69.091 Dysphagia following nontraumatic subarachnoid hemorrhage Dysphagia I69.191 Dysphagia following nontraumatic intracerebral hemorrhage Dysphagia I69.291 Dysphagia following other nontraumatic intracranial hemorrhage Dysphagia I69.391 Dysphagia following cerebral infarction Dysphagia I69.891 Dysphagia following other cerebrovascular disease Dysphagia I69.991 Dysphagia following unspecified cerebrovascular disease Apraxia I69.090 Apraxia following nontraumatic subarachnoid hemorrhage Apraxia I69.190 Apraxia following nontraumatic intracerebral hemorrhage Apraxia I69.290 Apraxia following other nontraumatic intracranial hemorrhage Apraxia I69.390 Apraxia following cerebral infarction Apraxia I69.890 Apraxia following other cerebrovascular disease Apraxia I69.990 Apraxia following unspecified cerebrovascular disease ALS G12.21 Amyotrophic lateral sclerosis

Section C Basics: An SLP’s Guide to the Cognitive Patterns
Section on the MDS
© 2019 Halcyon Rehabilitation, LLC
Section C: The Basics
→ Effective 10/1/19, Medicare will be incorporating the MDS’ Section C, Cognitive Patterns, as a part of the patient characteristics profile that is used to define the patient’s Case Mix Index for the SLP component of PDPM. While understanding a patient’s cognitive status has always been important for care planning and therapeutic interventions, Section C now steps into the reimbursement spotlight.
→ Per the Centers for Medicaid and Medicare Services (CMS), “The items in this section are intended to determine the resident’s attention, orientation and ability to register and recall new information. These items are crucial factors in many care-planning decisions.”
→ The MDS Coordinator should review the SLP evaluation, if present, as a comparison to the MDS information and to capture any additional clinical information.
→ Keep in mind that the instructions provided by CMS on the MDS are for the nurse completing the MDS section. → The clinical “lookback” for Section C is 7 days. → Documentation describing potential signs and symptoms related to each item should be present in the therapy
medical record to support correct coding and assist the MDS in capturing the most accurate Case Mix Index.
MDS Section C General Considerations and Instructions
→ The MDS Coordinator must determine if a Brief Interview for Mental Status (BIMS) should be conducted. Per CMS,
most residents are able to attempt the Brief Interview for Mental Status (BIMS). → The BIMS is a brief screener that aids in detecting cognitive impairment. The BIMS total score is highly correlated
with Mini-Mental State Exam scores. It does not assess all possible aspects of cognitive impairment. Furthermore, it is not a comprehensive, functional cognitive assessment, which can only be administered by a therapist.
→ The BIMS briefly assesses the following areas: o Repetition of Three Words (Immediate Recall) o Temporal Orientation (Orientation to year, date, and day) o Recall (Delayed)
→ The assessor must determine if the resident is able to answer the BIMS
questions verbally, in writing, or via another method. → The assessor must make every effort to administer the BIMS. → If the BIMS cannot be administered, nursing must complete a Staff Assessment for Mental Status, which briefly
assesses the following areas: o Short Term Memory o Long Term Memory o Memory/Recall Ability o Cognitive Skills for Daily Decision Making
BIMS SCORE Cognitively Intact 13 – 15 Mildly Impaired 8 – 12 Moderately Impaired 0 – 7 Severely Impaired -
Section C Basics: An SLP’s Guide to the Cognitive Patterns
Section on the MDS
© 2019 Halcyon Rehabilitation, LLC
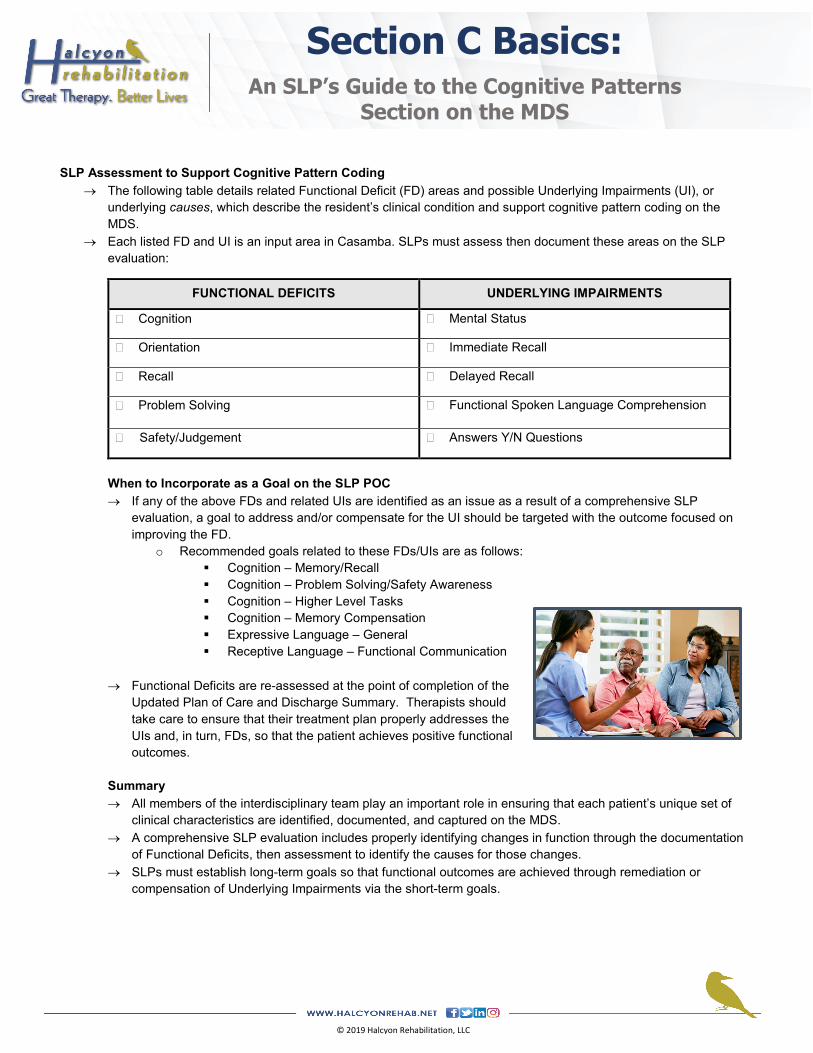
SLP Assessment to Support Cognitive Pattern Coding
→ The following table details related Functional Deficit (FD) areas and possible Underlying Impairments (UI), or underlying causes, which describe the resident’s clinical condition and support cognitive pattern coding on the MDS.
→ Each listed FD and UI is an input area in Casamba. SLPs must assess then document these areas on the SLP evaluation:
FUNCTIONAL DEFICITS UNDERLYING IMPAIRMENTS
� Cognition � Mental Status
� Orientation � Immediate Recall
� Recall � Delayed Recall
� Problem Solving � Functional Spoken Language Comprehension
� Safety/Judgement � Answers Y/N Questions
When to Incorporate as a Goal on the SLP POC → If any of the above FDs and related UIs are identified as an issue as a result of a comprehensive SLP
evaluation, a goal to address and/or compensate for the UI should be targeted with the outcome focused on improving the FD.
o Recommended goals related to these FDs/UIs are as follows: Cognition – Memory/Recall Cognition – Problem Solving/Safety Awareness Cognition – Higher Level Tasks Cognition – Memory Compensation Expressive Language – General Receptive Language – Functional Communication
→ Functional Deficits are re-assessed at the point of completion of the
Updated Plan of Care and Discharge Summary. Therapists should take care to ensure that their treatment plan properly addresses the UIs and, in turn, FDs, so that the patient achieves positive functional outcomes.
Summary → All members of the interdisciplinary team play an important role in ensuring that each patient’s unique set of
clinical characteristics are identified, documented, and captured on the MDS. → A comprehensive SLP evaluation includes properly identifying changes in function through the documentation
of Functional Deficits, then assessment to identify the causes for those changes. → SLPs must establish long-term goals so that functional outcomes are achieved through remediation or
compensation of Underlying Impairments via the short-term goals.
Section K Basics: An SLP’s Guide to the Swallowing/Nutritional
Status Section on the MDS
© 2019 Halcyon Rehabilitation, LLC
Section K: The Basics
→ Effective 10/1/19, Medicare will be incorporating the MDS’ Section K, Swallowing/Nutritional Status, as a part of the patient characteristics profile that is used to define the patient’s Case Mix Index. While swallowing and nutritional status have always been important for care planning and interventions, Section K will soon step into the reimbursement spotlight for the speech-language pathology (SLP) component of PDPM.
→ Per CMS, “the items in this section are intended to assess the many conditions that could affect the resident’s ability to maintain adequate nutrition and hydration.”
→ CMS recognizes that the ability to swallow directly relates to patient safety and quality of life. → The MDS Coordinator should review the SLP evaluation, if present, as a comparison to the MDS information and to
capture any additional clinical information. → While not every item in Section K applies to SLP’s scope of practice, this resource details the items that do. → The clinical “lookback” for Section K is 7 days. → Documentation describing potential signs and symptoms related to each item should be present in the therapy medical
record to support correct coding and assist the MDS in capturing the most accurate Case Mix Index score.
1. Item K0100. Item K0100: “Swallowing Disorders” is a “check all that apply” item. → Item K0100 does not require that the resident actually have a diagnosed swallowing disorder. A sub-item is
applicable if the resident had the presence of signs and symptoms of a possible swallowing disorder in the seven-day look-back period.
→ Specifically, the coding instructions for Item K0100 state,” Observe the resident during meals or at other times when he or she is eating, drinking, or swallowing to determine whether any of the listed symptoms of possible swallowing disorder are exhibited.” Keep in mind that these instructions are for the nurse completing the MDS section.
K0100 Sub-Item Coding Instructions. Below are CMS’ instructions for completion of K0100. → K0100A, loss of liquids/solids from mouth when eating or drinking. When the resident has food or liquid in his or
her mouth, the food or liquid dribbles down chin or falls out of the mouth. → K0100B, holding food in mouth/cheeks or residual food in mouth after meals. Holding food in mouth or cheeks
for prolonged periods of time (sometimes labeled pocketing) or food left in mouth because resident failed to empty mouth completely.
→ K0100C, coughing or choking during meals or when swallowing medications. The resident may cough or gag, turn red, have more labored breathing, or have difficulty speaking when eating, drinking, or taking medications. The resident may frequently complain of food or medications “going down the wrong way.”
→ K0100D, complaints of difficulty or pain with swallowing. Resident may refuse food because it is painful or difficult to swallow.
→ K0100Z, none of the above. If none of the K0100A through K0100D signs or symptoms were present during the look-back.
Section K Basics: An SLP’s Guide to the Swallowing/Nutritional
Status Section on the MDS
© 2019 Halcyon Rehabilitation, LLC
SLP Assessment to Support K0100. → The following table details related Functional Deficit (FD) areas and Underlying Impairments (UI), or underlying
causes, which describe the resident’s clinical condition and support item K0100 on the MDS. → Each listed FD and UI is an input area in Casamba. SLPs should assess then document these areas when
swallowing is an identified problem at the time of referral:
FUNCTIONAL DEFICITS UNDERLYING IMPAIRMENTS
� Swallow Status � Dentition � Signs/Symptoms of Aspiration – Liquids
� Affected Phase � Formation of Bolus � Signs/Symptoms of Aspiration – Solids
� Intake Method � Swallow Initiation � Labial Function
� Diet Level � Pocketing � Lingual Function
� Liquid Level � Choking � Mandibular Function
� Labial Closure � Coughing � Labial O/M Assessment
Mastication � Sensation of Lips/Oral Cavity � Buccal O/M Assessment
→ Additionally, and complaints of pain when swallowing should be documented in the free-type box under the
Underlying Impairments tab to support Sub-Item K0100D, if applicable.
When to Incorporate as a Goal on the SLP POC. → If any of the above FDs and related UIs are identified as an issue as a result
of a comprehensive SLP evaluation, a goal to address and/or compensate for the UI should be targeted with the outcome focused on improving the FD.
→ Functional Deficits are re-assessed at the point of completion of the Updated Plan of Care and Discharge Summary. Therapists should take care to ensure that their treatment plan properly addresses the UIs and, in turn, FDs, so that the patient achieves positive functional outcomes.
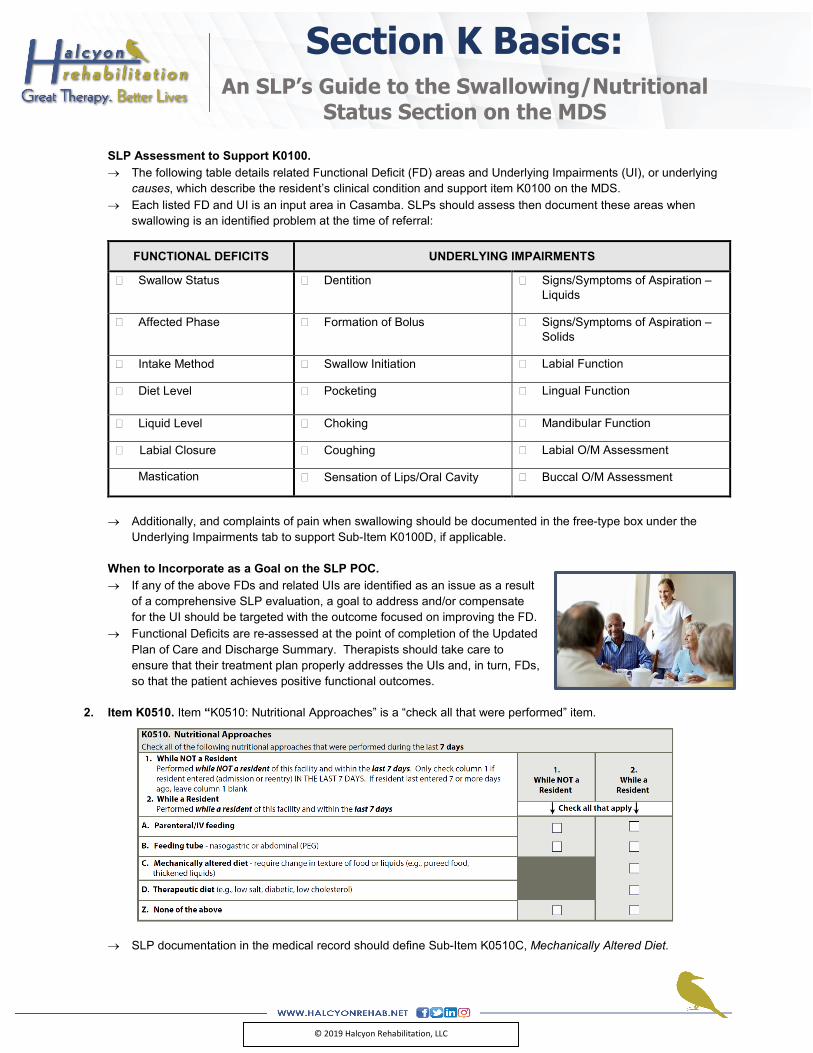
2. Item K0510. Item “K0510: Nutritional Approaches” is a “check all that were performed” item.
→ SLP documentation in the medical record should define Sub-Item K0510C, Mechanically Altered Diet.
Section K Basics: An SLP’s Guide to the Swallowing/Nutritional
Status Section on the MDS
© 2019 Halcyon Rehabilitation, LLC
K0510 Sub-Item Coding Instructions. Below are CMS’ instructions for completion of K0510C. → Mechanically Altered Diet Definition. A diet specifically prepared to alter the texture or consistency of food to
facilitate oral intake. Examples include soft solids, puréed foods, ground meat, and thickened liquids. A mechanically altered diet should not automatically be considered a therapeutic diet.
SLP Assessment to Support K0510. → The following table details related Functional Deficit (FD) areas and possible Underlying Impairments (UI), or
underlying causes, which describe the resident’s clinical condition and support item K0510 on the MDS. → Each listed FD and UI is an input area in Casamba. SLPs should assess then document these areas when
swallowing is an identified problem at the time of referral:
FUNCTIONAL DEFICITS UNDERLYING IMPAIRMENTS
� Swallow Status � Overall Swallowing Function
� Intake Method � Dentition
� Diet Level � Formation of Bolus
� Liquid Level � Signs/Symptoms of Aspiration – Liquids
� Signs/Symptoms of Aspiration – Solids
When to Incorporate as a Goal on the SLP POC. → If any of the above FDs and related UIs are identified as an issue as a result of a comprehensive SLP evaluation, a
goal to address and/or compensate for the UI should be targeted with the outcome focused on improving the FD. → Functional Deficits are re-assessed at the point of completion of the Updated Plan of Care and Discharge Summary.
Therapists should take care to ensure that their treatment plan properly addresses the UIs and, in turn, FDs, so that the patient achieves positive functional outcomes.
Summary. → A comprehensive SLP evaluation includes properly identifying
changes in function through the documentation of Functional Deficits, then assessment to identify the causes for those changes.
→ SLPs must establish long-term goals so that functional outcomes are achieved through remediation or compensation of Underlying Impairments via the short-term goals.
→ All members of the interdisciplinary team play an important role in ensuring that each patient’s unique set of clinical characteristics are identified, documented, and captured on the MDS.
PDPM Bulletin RU -IV to PDPM Transition
019
The transition between RUG-IV and PDPM will be a “hard” transition, meaning the 2 systems will not run concurrently at any point. All days of service for the month of September 2019 will require a PPS MDS assessment with an ARD on or before September 30 to generate a RUG-IV HIPPS code for billing, while all days of service beginning October 1, 2019 will be billed under PDPM using an assessment with an ARD in October.
Mid-September or Earlier Admissions For Medicare stays that begin mid-September or earlier, SNFs should follow the current PPS assessment schedule through the end of September. Be sure to track the need for OMRAs through the end of September, including the need to do COTs. If a COT observation period would end on October 1st or later, a COT will not be required. Late September Admissions If an admission arrives late enough in September, there may not be an option to capture 5 days of therapy by September 30th and that admission should be viewed with a PDPM strategy from the day of admission (10/1 is a Tuesday). For example, if a facility does not typically provide therapy on weekends, a new admission would have to start therapy by September 24 in order to receive 5 days of therapy by September 30. Weekend therapy the last weekend of September will be critical. If a facility provides therapy 7 days a week, a resident would have to start therapy by September 26 in order to receive 5 days of therapy by September 30. Therapy started on September 27 or later should be provided but will not qualify a resident for a rehab RUG, as the resident would not qualify for a short-stay assessment. For these admissions at the end of September, SNFs will need a 5-day assessment with an ARD no later than September 30 in order to bill for the September dates of service, even if the 5-day assessment will not capture a therapy RUG score. However, a skilled level of care will still be required during this period. Once SNFs have reached the September 27 cutoff date for not being able to capture five days of therapy delivered by September 30, SNFs will want to begin thinking with a PDPM mindset, where therapy days and minutes do not affect the payment rate. Transitional Interim Payment Assessment (IPA) A transitional IPA will be done on every Medicare A patient in your building with an ARD between 10/1 – 10/7. Section GG assessments are required for all with functional assessment occurring 1-3 days preceding the ARD (ARD + 2 prior days). It is critical that ARD selection will capture the clinical information that will generate the most appropriate payment rate. DORs will need to obtain ARD dates selected for each Med A patient transitioning from the MDS/PPS Coordinator. October 1, 2019, will be considered Day 1 of the VPD schedule under PDPM, even if the patient began their stay prior to October 1, 2019. Clinicians must complete a PDPM Transition Worksheet and all discipline-specific assessment areas per the worksheet. No therapy UPOC is required. PDPM Initial Medicare Assessment – Transitioning Residents Under PDPM, the Initial Medicare Assessment will most likely determine the base payment rate for the resident’s entire stay. It is critical that ARD selection will capture the clinical information that will generate the most appropriate payment rate. Under RUG-IV, MDS Coordinators have grown accustomed to use later ARDs for the 5-day assessment in order to capture five days of therapy delivered by the ARD. This meant often using day 7 or day 8 of the stay as the ARD. Under PDPM, the ARD that would capture the highest rate could be a much earlier ARD. Section I – Active Diagnoses is used to calculate certain nursing components under PDPM and captures many of the conditions that assign points for the NTA component. The look back period for Section I is seven days, and it allows looking prior to admission to the facility if the ARD is set early enough. Thus, using a very early ARD might allow a provider to capture a diagnosis that was active in the hospital stay but might be resolved once the resident is admitted to the SNF. For example, if the ARD was chosen as day 1 of the stay, the MDS coordinator could capture a diagnosis that had been active within the last six days of the hospital stay even if it is not going to be active in the SNF. DORs must meet with MDS/PPS Coordinators to obtain selected PDPM ARD dates for transitioning Med A patients.
For questions about PDPM or this information, please email [email protected].