Embed Size (px)
Citation preview

Pp
REa
b
c
Fd
e
f
g
a
AA
KAEEH
1
fmarmuas
eT
1d
Respiratory Physiology & Neurobiology 179 (2011) 294– 299
Contents lists available at SciVerse ScienceDirect
Respiratory Physiology & Neurobiology
jou rn al h om epa ge: www.elsev ier .com/ locate / resphys io l
ulmonary arterial systolic pressure and susceptibility to high altitudeulmonary edema
émi Mouniera,b,c, Aimé Amonchotd, Nicolas Caillot c,e, Cécile Gladinef, Bernard Citrond, Mario Beduc,1,rica Chiricog, Jean Coudertc,2, Vincent Pialouxc,g,∗,2
Institut Cochin, Université Paris Descartes, CNRS (UMR 8104), Paris, FranceINSERM, U1016, Paris, FranceUniversité d’Auvergne, Centre Hospitalier Universitaire de Clermont-Ferrand, Service de Médecine du Sport et des Explorations Fonctionnelles, Hôpital G. Montpied, Clermont-Ferrand,ranceCentre Hospitalier Universitaire, Hôpital Gabriel Montpied, Service de Cardiologie et Maladies Vasculaires, 28 Place Henri Dunant – BP 38, 63000 Clermont-Ferrand, FranceSociété NRC Médical, 63450 Saint-Saturnin, FranceINRA, Research Unit on Herbivores, Nutrients and Metabolisms group, 63122 Saint Genès Champanelle, FranceUniversité Claude Bernard Lyon 1, EA 647, Centre de Recherche et d’Innovation sur le Sport, Université de Lyon, 69622 Villeurbanne Cedex, France
r t i c l e i n f o
rticle history:ccepted 20 September 2011
eywords:ltitude pulmonary diseasechocardiographyxerciseypoxia
a b s t r a c t
There is evidence that pulmonary arterial hypertension plays a major role in the occurrence of highaltitude pulmonary edema (HAPE). We tested the hypothesis that the pulmonary arterial systolic pressureresponse to a challenge associated with hypoxia and mild exercise may be considered a predictive factorof HAPE. Pulmonary arterial systolic pressure was measured by Doppler echocardiography in 8 HAPEsusceptible (HAPE-S) subjects and 8 HAPE resistant mountaineers (HAPE-R) during a hypoxic exercisechallenge established by the French Association for Sport Medicine (Richalet’s test).
Pulmonary arterial systolic pressure during hypoxic exercise allowed a significant discriminationbetween the groups, although an overlap of values was observed. When expressed as individual vari-
ations from baseline to hypoxic exercise level however, we found a highly significant difference. Nooverlap was observed between HAPE-R (range: 6.7–18.5 mmHg) and HAPE-S (range: 19.2–30.4 mmHg)groups, with a cut-off value at 19 mmHg. Plasma Vascular Endothelial growth factor (VEGF) and malon-dialdehyde (MDA) increased in response to hypoxic exercise only in HAPE-S group. Individual increasesin pulmonary arterial systolic pressure during hypoxic exercise from basal resting normoxic values seemE susc
relevant to estimate HAP. Introduction
High altitude pulmonary edema (HAPE) is a life-threateningorm of non-cardiogenic pulmonary edema occurring in healthy
ountaineers. Although the exact pathophysiological mechanismsre still unclear, there is a general agreement about the crucialoles of pulmonary vascular hypertensive response and hyperper-eability parameters in response to hypoxia exposure. Symptoms
sually evolve within 1–3 days after rapid ascent to altitudesbove 2500 m (Houston, 1960). Lack of pre-acclimatization, exces-ive rate of ascent, early strenuous exercise, elevation in altitude,
∗ Corresponding author at: Université Claude Bernard Lyon 1, Centre de Recherchet d’Innovation sur le Sport, EA 647, 69622 Villeurbanne Cedex, France.el.: +33 4 72 43 28 42; fax: +33 4 72 43 80 10.
E-mail address: [email protected] (V. Pialoux).1 Deceased.2 Co-senior authors.
569-9048/$ – see front matter © 2011 Elsevier B.V. All rights reserved.oi:10.1016/j.resp.2011.09.011
eptibility when measured during the Richalet’s test.© 2011 Elsevier B.V. All rights reserved.
cold exposure, and individual susceptibility are the major deter-minants in its occurrence (Hackett et al., 1976). The incidence ofHAPE is estimated to be less than 1% in the general mountaineeringpopulation but may increase up to 10% following rapid ascent at4559 m and up to 60% in vulnerable subjects (Bartsch et al., 1991).Several studies attempting to identify HAPE-Susceptible (HAPE-S)subjects at sea level have been published over recent decades. InHAPE-S, pulmonary arterial hypertension plays a major role in thispathogenesis (Bartsch et al., 1991; Hackett et al., 1992; Scherreret al., 1996). However, Doppler echocardiography failed to conclu-sively distinguish HAPE-S and HAPE-Resistant (HAPE-R) subjectsby estimating pulmonary artery systolic pressure (PASP) duringshort exposure to acute hypoxia (Grunig et al., 2000; Hohenhauset al., 1995; Vachiery et al., 1995). Although pulmonary arterialhypertension induced by acute hypoxia was significantly higher
in HAPE-S, it was concluded that such a method was not reliable,due to overlap between the groups (Hohenhaus et al., 1995). Nev-ertheless, none of these studies used hypoxia exposure coupledwith exercise, which could exacerbate the arterial desaturation as
logy & Neurobiology 179 (2011) 294– 299 295
osoHHchhCchtdatcccPvamttetwtitwruhniHn
2
2
d“c
2
ygapwabHt4mtsm
Table 1Characteristics of the subjects.
Group HAPE-R HAPE-S
Gender 2 female, 6 male 2 female, 6 maleAge (years) 38.5 ± 14.7 49.4 ± 6.1Height (cm) 174 ± 9 173 ± 8Weight (kg) 68.6 ± 8.7 72.5 ± 10.9BMI (kg m−2) 22.7 ± 2.5 24.1 ± 2.4
maximal power and corresponding heart rate according to Astrandand Ryhming abacus (Astrand and Ryhming, 1954). Adjusting thebackrest and the additional head and shoulder supports ensuredthe subjects’ optimum comfort. The height of the saddle was also
R. Mounier et al. / Respiratory Physio
bserved during mountains ascents. To our knowledge, only onetudy investigated the combined effect of exercise and hypoxian PASP though it was not able to improve the identification ofAPE-S subjects in laboratory conditions (Dehnert et al., 2005).owever, the 2 h resting hypoxic exposure preceding the exer-ise under hypoxia and/or the exercise intensity (exhaustion) couldave affected the subsequent PASP responses and invalidated itsypothetical cut-off value between HAPE-S and HAPE-R subjects.onsidering these observations, a standardized test consisting ofardiovascular and pulmonary response measurements to hypoxiaas been established by the French Association for Sport Medicineo detect subjects who are more liable to suffer from high-altitudeiseases (Brugniaux et al., 2006; Richalet et al., 1988). Heart ratend cardiac output elevations are hallmarks of human adaptationo acute hypoxia, since the systemic mechanisms by which theardiovascular system matches O2 supply with O2 demand arehallenged by a hypoxic environment. It is of great interest to asso-iate the analysis of these parameters in such investigation sinceASP elevations do not exclusively account for hypoxic pulmonaryasoconstriction but also for cardiac output adaptations to exercisend/or acute hypoxia. Pulmonary endothelial hyperpermeabilityay be caused by impaired endothelium-dependent vasodilata-
ion, which is a result of reduced production and/or activity ofhe vasodilatator nitric oxide (Kleinbongard et al., 2006; Scherrert al., 1996). Reactive oxygen species seem to play a key role inhis endothelial dysfunction. Superoxide (O2•−) is known to reactith nitric oxide synthesized by endothelial nitric oxide synthase
o form the oxidant peroxynitrite, thereby inducing nitric oxidenactivation and uncoupling of the endothelial nitric oxide syn-hase (Thomas et al., 2008). The aim of this study was to clarifyhether HAPE-S subjects can be reliably identified by their PASP
esponses to a well-standardized hypoxic exercise using Dopplerltrasound. We tested the hypothesis that the combined effects ofypoxia and exercise could be a valuable method to predict vul-erability to HAPE. We measured the parameters suggested to be
nvolved in the mechanisms leading to pulmonary hypertension inAPE: cardiovascular and ventilatory responses, oxidative stress,itric oxide, and VEGF (Crosswhite and Sun, 2010).
. Materials and methods
.1. Ethics statement
The protocol (PHRC no. 8141) was conducted according to theeclaration of Helsinki and approved by the local ethics committeeComité de Protection des Personnes Sud Set VI”. Written informedonsent was obtained for all subjects.
.2. Subjects
Sixteen healthy volunteer subjects (age ranging from 24 to 60ears) were recruited for this protocol. Inclusion criteria were: bothenders, age between 20 and 60 years, normal medical history,bsence of confounding medication, and clearly detectable tricus-id regurgitation on echocardiography. Eight HAPE-S subjects (2omen, 6 men) participated in our study. They were identified and
dmitted on the basis of one or more episodes of HAPE, attestedy radiographical evidences and clinical reports. The altitude of theAPE occurred at a mean of 4925 m (range: 3300–6500 m). The alti-
ude reached by subjects from HAPE-S groups was ranged between300 m and 7000 m (mean = 5960 m). Eight subjects (2 women, 6
en), identified as good responders to hypoxia in absence of alti-ude illness history during previous expeditions at high altitude,erved as HAPE-R group. The HAPE-R subjects were all confirmedountaineers and performed numerous expeditions in Andean and
Values represent means (±SD). HAPE-R, high altitude pulmonary edema resistantsubjects; HAPE-S, high altitude pulmonary edema susceptible subjects.
Himalayan summits before the protocol. Maximal altitude reachedby HAPE-R subjects was ranged between 4807 m and 6432 m(mean = 5842 m). The subject characteristics are summarized inTable 1. Before inclusion, subjects were submitted to medical exam-ination. Written informed consent was obtained for all subjects. Allwere healthy, Caucasian mountaineers and natives of low altitude.None of them had been exposed to altitudes above 1000 m withinthe 3 months before the test.
2.3. Experimental design
The protocol was conducted in Clermont-Ferrand (320 m, baro-metric pressure = 730 mmHg, France). The subjects were free towithdraw from the test at any time. All parameters were mea-sured in a quiet room (temperature = 20 ◦C) at the same time ofday (early afternoon) for all subjects. We decided to separatethe effects of hypoxia and exercise on cardiovascular and pul-monary vascular responses. Therefore, our test was composed offour different phases with duration of 8 min each, in successionand without interruption. The first two phases consisted of 8 minof baseline immediately followed by 8 min of hypoxic rest. Withoutdelay, the subjects began 8 min of exercise in hypoxia immedi-ately followed by 8 min of exercise in normoxia. Fig. 1 representsthe overall organization of our protocol. Hypoxic and normoxicphases were monitored with a mechanism allowing an instanta-neous switch between room air and hypoxic mixture (FiO2 = 0.118with a local mean barometric pressure of 730 mmHg, thereby sim-ulating an elevation of 4800 m). Throughout the test session, thesubjects were unaware of whether they were breathing room airor hypoxic gas. This protocol, calls also Richalet’s test, emergingfrom a national consensus that aims to identify poor and goodresponders to hypoxia, was chosen in accordance with previouslypublished investigations that aimed to identify subjects suscepti-ble to acute mountain sickness (Richalet et al., 1988; Brugniaux etal., 2006).
The exercise phase consisted of cycling (30% VO2max innormoxia) on a supine ergometer suitable for stress Dopplerechocardiography (er900EL, ERGOLINETM, Germany). The exerciseintensity was estimated using gender, age, training status, sub-
Fig. 1. Experimental design.

2 logy & Neurobiology 179 (2011) 294– 299
atpi43wasgBfeb
2
olav5Pe4Pttopm
2
bHtewmoo
re
2
m(mdpmew(u
2
t
0
10
20
30
40
50
60
RN RH EH EN RN RH EH EN
HAPE-R HAPE-S
PASP
(mm
Hg)
**
** ††
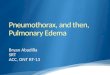
Fig. 2. Variations in pulmonary arterial systolic pressure (PASP) across test con-ditions in HAPE-R (empty circles) and HAPE-S subjects (filled circles). Horizontalbars represent the mean values in each group. RN: rest normoxia; RH: rest hypoxia;
96 R. Mounier et al. / Respiratory Physio
djusted so that the position of the upper body and legs in rela-ion to the crank was always optimal. Inclination was adjustedrior the test so that tricuspid regurgitation jet ultrasound trac-
ngs were clearly detectable. This represented an angle of about5◦ to the ground in the anterior–posterior axis and laterally 10◦ to0◦ to the left. Venous blood sample were collected concomitantlyith Doppler echocardiographic measurements during baseline
nd hypoxic exercise (i.e. during the last 30 s of each respectivetep). 5 ml blood sample (2× 2.5 ml) was also collected into Pax-ene Blood RNA tubes (Qiagen, France) for RNA extraction. Paxgenelood RNA tubes contain reagents that protect RNA molecules
rom degradation by RNases and prevent modification of genexpression. Samples were stored at −20 ◦C until the assay coulde performed.
.4. Doppler echocardiographic measurements
All echocardiographic recordings were started in the 4th minutef each experimental phase. The examiner, a cardiologist with aong-standing experience in Doppler echocardiography, performedll measurements for all subjects. Peak tricuspid regurgitation jetelocity was assessed by continuous-wave Doppler (ATL HDI®
000cv, PhilipsTM) guided by two-dimensional echocardiography.ASP was then estimated by the mean of the simplified Bernoulliquation with an assumed right atrial pressure of 5 mmHg (e.g.V2 + 5 mmHg, where V is the peak velocity in m s−1) (Yock andopp, 1984). Recordings were analysed off-line in random order bywo blind reviewers, unaware of either the subject’s medical his-ory or the experimental conditions. We reported averaged valuesbtained with a minimum of three different cycles. Cardiac out-ut was classically estimated from aortic outflow and heart rate. Ainimum of 5 different cardiac cycles were required.
.5. Ventilatory and cardiovascular parameters
Pulmonary gas exchange was measured with a breath-by-reath ergospirometry system (Oxycon Pro®, Jaeger, VIASYSealthcareTM) and averaged values over 30 s were reported. Ven-
ilatory measurements were started in the 4th minute of eachxperimental phase (i.e. when steady state was obtained) andere recorded concomitantly with Doppler echocardiographiceasurements to ensure optimal significance. In addition, arterial
xygen saturation (SaO2) was continuously monitored by a pulsedxymeter using a finger probe.
Heart rate was derived from continuous electrocardiogramecording. The measurements were performed concomitantly withchocardiographic recordings.
.6. Plasma analysis
Concentrations of plasma malondialdehyde (MDA) were deter-ined as thiobarbituric reactive substances as previously described
Pialoux et al., 2006). Plasma total nitrite and nitrate levels wereeasured by using the Griess reaction procedure as previously
escribed (Rock et al., 1995). Nitrite and nitrate as degradationroducts of nitric oxide (NOx) are preferentially measured to esti-ate the production of nitric oxide in biological samples. Vascular
ndothelial growth factor (VEGF) concentrations in plasma samplesere determined using a sandwich enzyme-linked immunoassay
Quantikine R&D Systems, Minneapolis, MN) according to the man-facturer’s instructions.
.7. RNA preparation and expression analysis
Paxgene Blood RNA tubes were used for total RNA extrac-ion using the Paxgene Blood RNA kit (Qiagen, France). The RNA
EH: exercise hypoxia; EN: exercise normoxia. **P < 0.01 vs. corresponding RH step.††P < 0.01 vs. HAPE-R at HE.
preparation and expression analysis of HIF-1� were determined aspreviously described (Mounier et al., 2006, 2009a,b).
2.8. Statistical analysis
Results are presented as the overall mean and standard devi-ation (mean ± SD). After testing the variables for normality usingKolmogorov–Smirnov test, differences between HAPE-S and HAPE-R groups, and physiological and biological responses to each phaseof the test were evaluated by two-way repeated measures ANOVAfollowed by a post-hoc test. Differences in sensitivity and specificitywere compared by McNemar’s test. Coefficient of variation (intra-variability) and t-value (difference of the means divided by SD)calculated from the off line analyses done by the two experiencedexaminers were respectively 4.94% and 0.74.
The relationships between variables were investigated usingPearson correlation coefficients. Statistical analyses were per-formed with SPSS (Version 15.0, Chicago, IL, USA). Differences wereconsidered significant at a P < 0.05.
3. Results
3.1. Pulmonary vascular responses
Echocardiographic data were successfully obtained in all condi-tions for the 16 subjects. In comparison to baseline, PASP increasedsignificantly in both groups for the 3 other steps (i.e. hypoxia atrest, hypoxic exercise and normoxic exercise) (Fig. 2). Additionally,PASP was significantly higher during hypoxic exercise than dur-ing RH (10.8 ± 3.8 mmHg, P < 0.01 for HAPE-R and 15.7 ± 2.8 mmHg,P < 0.001 for HAPE-S).
Mean PASP (mmHg) was significantly higher in the HAPE-Sgroup than in the HAPE-R group only during hypoxic exer-cise (39.3 ± 9.8 vs. 27.4 ± 6.4 mmHg, P < 0.01). As expressed asindividual increases between baseline and hypoxic exercise, weobserved a highly significant difference (P < 0.001) between HAPE-R(range: 6.7–18.5 mmHg) and HAPE-S subjects (Fig. 3). No over-lap was observed in the individual increase of PASP (�PASP) inhypoxic exercise compared to baseline between HAPE-R (range:
6.7–18.5 mmHg) and HAPE-S (range: 19.2–30.4 mmHg) groups,with a cut-off value at 19 mmHg (Fig. 3). The sensitivity and speci-ficity of this cut off are 100%.
R. Mounier et al. / Respiratory Physiology & Neurobiology 179 (2011) 294– 299 297
Table 2Cardiac output (CO), heart rate (HR), arterial oxygen saturation (SaO2), ventilation (VE) and power output (PO) during the four steps of the hypoxic test.
Group Rest normoxia Rest hypoxia Exercise hypoxia Exercise normoxia
HAPE-R HAPE-S HAPE-R HAPE-S HAPE-R HAPE-S HAPE-R HAPE-S
HR (bpm) 67 ± 5 71 ± 12 75 ± 8 84 ± 12 132 ± 10 131 ± 14 112 ± 8 115 ± 10
CO (L min−1) 4.9 ± 0.7 5.2 ± 1.0 5.2 ± 0.9 6.4 ± 1.2 11.6 ± 1.1 11.5 ± 1.8 9.3 ± 0.9 10.2 ± 1.4
SaO2 (%) 96.8 ± 2.3 95.8 ± 1.5 81.8 ± 4.7 77.6 ± 5.5 68.4 ± 4.2 64.8 ± 7.8 94.6 ± 1.6 93.4 ± 0.8
VE (L min−1) 9.9 ± 2.0 11.4 ± 3.5 12.6 ± 3.8 15.0 ± 5.7 49.3 ± 11.3 53.4 ± 13.5 37.5 ± 5.8 38.9 ± 6.6
PO (W) 0 ± 0 0 ± 0 0 ± 0 0 ± 0
Values represent means (±SD). HAPE-R, high altitude pulmonary edema resistant subject
5
10
15
20
25
30
35
ΔPA
SP (E
H-R
N) (
mm
Hg)
HAPE-R HAPE-S
††
Fig. 3. Individual increase in pulmonary arterial systolic pressure (�PASP) betweenrae
3
oto
3
ecwa
TPfh
Vs
wide scatter of PASP values across the four conditions of our test
esting normoxic values (RN) and hypoxic exercise (EH) in HAPE-R (empty circles)nd HAPE-S (filled circles) subjects. Horizontal bars represent the mean values inach group. ††P < 0.01 vs. HAPE-R.
.2. Cardiovascular responses
Cardiac and arterial oxygen saturation responses and powerutput across test conditions are expressed in Table 2. Regardlesshe test conditions, we did not find differences for heart rate, cardiacutput, SaO2 between HAPE-R and HAPE-S subjects.
.3. Biochemical values
The plasma concentration of VEGF was unaltered by hypoxic
xercise in the HAPE-R group, although we observed an increasedoncentration in the HAPE-S group (Table 3). MDA and NOx levelsere measured in the plasma of the different patients before andfter exercise to determine the effect of health status and exercise
able 3lasmatic concentration of malondialdehyde (MDA), vascular endothelial growthactor (VEGF), nitric oxide end-products (NOx) and leukocyte mRNA expression ofypoxia inducible factor 1-alpha (HIF-1�).
Group HAPE-R HAPE-S
Baseline Post test Baseline Post test
MDA (mmol L−1) 5.7 ± 1.0 4.9 ± 1.4 5.3 ± 2.1 9.0 ± 6.3*,**
VEGF (mmol L−1) 15.8 ± 12.5 16.2 ± 12.4 29.1 ± 47.3 41.8 ± 38.5***
NOx (mmol L−1) 36.3 ± 10.5 33.3 ± 12.2 31.9 ± 16.5 28.6 ± 14.3HIF-1� (fold change) 1 0.68 1.14 0.92
alues represent means (±SD). HAPE-R, high altitude pulmonary edema resistantubjects; HAPE-S, high altitude pulmonary edema susceptible subjects.
* P < 0.05 vs. baseline.** P < 0.05 vs. HAPE-R.
*** P = 0.058 vs. baseline.
80 ± 17 78 ± 18 80 ± 17 78 ± 18
s; HAPE-S, high altitude pulmonary edema susceptible subjects.
on the oxidative and vasodilatation processes (Table 3). As forVEGF, MDA increased in response to hypoxic exercise only inHAPE-S group. Regardless of the group (HAPE-R vs. HAPE-S) or thecondition (baseline vs. hypoxic exercise) NOx and HIF-1� mRNAdid not change (Table 3).
3.4. Correlations
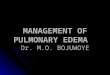
In the HAPE-S group, HIF-1� mRNA after the test was signifi-cantly correlated with PASP (r2 = 0.60, P < 0.05; Fig. 4).
4. Discussion
This study demonstrates that an increase in PASP using a pro-tocol associating hypoxia and exercise specifically established todetect altitude disease seems relevant to estimate the susceptibilityto HAPE (Brugniaux et al., 2006; Richalet et al., 1988). Importantly,we did not observe overlap in individual increases of PASP (hypoxicexercise vs. baseline) between HAPE-S and HAPE-R groups, with acut-off value at 19 mmHg. These results bring convincing evidencethat interpretation of individual PASP increases with hypoxia andexercise should carefully take into account the basal resting nor-moxic values. Individual PASP increases during Richalet’s test aretherefore likely to be a reliable tool to reveal HAPE-susceptibility.
Although exact mechanisms leading to HAPE are not completelyunderstood, there is a general agreement about the crucial role ofpulmonary arterial hypertension in the pathogenesis of the dis-ease (Bartsch et al., 1991; Houston, 1960; Hultgren et al., 1971).Indeed, the association between pulmonary arterial hypertensionand HAPE has been confirmed on several occasions by invasive(Hultgren et al., 1971) and non-invasive techniques (Hackett et al.,1976; Swenson et al., 2002; Vachiery et al., 1995). In our results, the
is in agreement with previous studies that used comparable meth-ods of assessing hypoxic pulmonary vascular reactivity (Allemannet al., 2000; Hackett et al., 1976; Swenson et al., 2002; Vachiery
R² = 0.5 982P=0.04
15
19
23
27
31
0 50 0 100 0 150 0 200 0 250 0
Δ HIF -1α mRN A (u.a.)
ΔPA
SP (m
mH
g)
Fig. 4. Relationship between changes in leukocytes HIF-1� mRNA (�HIF-1� mRNA)and pulmonary arterial systolic pressure (�PASP) between normoxic values (RN)and hypoxic exercise (EH) in HAPE-S subjects.

2 logy &
eher
tvSSnpTbdmefihilt(HoIif
HAc(blwm(oecti
fttHItaeoboDPiiiead
ot
98 R. Mounier et al. / Respiratory Physio
t al., 1995). The mean PASP among HAPE-S subjects is significantlyigher compared to the mean PASP in the HAPE-R group. How-ver, we found a small overlap between the groups as previouslyeported.
Despite a significantly higher increase in PASP with exercise inhe HAPE-S group compared to the HAPE-R group (27 ± 8 mmHgs. 8 ± 2 mmHg), this parameter is not sufficient to identify HAPE-
subjects contrary to previous findings (Hohenhaus et al., 1995).tress Doppler echocardiography during supine bicycle exercise inormoxia performed after a 90-min hypoxic exposure has beenroven to predict HAPE susceptible subjects (Grunig et al., 2000).hese authors found a cut-off of PASP at 40 mmHg without overlapetween HAPE-R and HAPE-S. However, because of the extensiveuration of this protocol it is not feasible to perform a standardedical examination. Additionally, the measurements by stress
chocardiography during incremental exercise protocol may beurther limited by difficulty to estimate PASP by Doppler ultrasoundn all subjects, especially at high levels of exercise with elevatedeart rates. Indeed, the absence of adequate tracing in some
ndividuals during exercise has been pointed to as an importantimitation of the ultrasound technique because tricuspid regurgi-ation jet may not always be recovered during hypoxia or exerciseHohenhaus et al., 1995). On the contrary, the identification ofAPE-S subjects using our standardized 30-min protocol elicitingnly a 30% VO2max intensity can fit with medical exam standards.n this context the classification of the subject using the increasen PASP in responses to hypoxic exercise situation did not result inurther overlap between HAPE-S and HAPE-R.
The study of Dehnert et al. (2005) found an overlap betweenAPE-R and HAPE-S subjects for PASP during hypoxic exercise.
few differences regarding the protocol can explain the dis-repancies between their study and ours. In the Dehnert’ studyDehnert et al., 2005), the intensity of the hypoxic exercise hadeen progressively increased starting a low intensity (initial work-
oad of 25 watts with an increment of 25 watts every 2 min),hereas our subject were immediately exposed to exercise at aean of 80 watts. As recommended by the Richalet’s test guideline
Brugniaux et al., 2006; Rathat et al., 1992; Richalet et al., 1988),ur exercise protocol was performed in a slightly higher hypoxicnvironment than in Dehnert’s study (4500 vs. 4800 m). Our proto-ol, which was developed specially to detect subjects’ susceptibleo high-altitude diseases, can be used as a tool to detect the increasen PASP as predictor of HAPE.
Dehnert’s article indicated that the hypoxic exercise was per-ormed after 2 h of hypoxia exposure (FIO2 of 12%). In this study,he preliminary hypoxia exposure and the progressive nature ofhe exercise may explain the small overlap between HAPE-R andAPE-S subjects for the PASP during the hypoxic exercise stimulus.
n assessing the highest measurable PASP during their incremen-al test, the sustained relative workload may be not the same forll subjects, thus inducing potential stimulus differences that mayxplain their small overlap. Moreover, pulmonary edema can alsoccur in subjects with a mild rise in PASP during acute normo-aric hypoxia exposure (Hohenhaus et al., 1995), as confirmed byur significantly lower PASP maximum HAPE-S values compared toehnert’s (39 vs. 69 mmHg). This could suggest that despite lowerASP responses a mild-intensity (with the same relative intensity,.e. 30% of sea-level VO2max) hypoxic exercise with short prelim-nary hypoxia exposure may better help to predict HAPE than anncremental all-out hypoxic exercise preceded by longer hypoxiaxposure. Nevertheless, although Denhert’s subjects experiencedt least twice HAPE episodes than ours, HAPE severity did not seem
ifferent between the 2 HAPE-S cohorts.Other mechanisms seem to be involved in the physiopathologyf HAPE since all individuals with a pulmonary arterial hyper-ension do not necessarily develop HAPE (Sartori et al., 2000).
Neurobiology 179 (2011) 294– 299
Some authors exposed individuals with a history of perinatal pul-monary hypertension to an altitude of 4559 m (Sartori et al., 1999).Those with perinatal pulmonary hypertension are known to havebrisk hypoxic pulmonary vasoconstriction believed in part to bedue to pulmonary vascular endothelial dysfunction. Under alti-tude exposure, these subjects had marked pulmonary hypertension(PASP = 62 mmHg) but none of them developed HAPE. Therefore,this information should be taken in account for the discriminationof HAPE-S subjects.
The correlations between HIF-1� mRNA and PASP during EHconfirm previous results suggesting that HIF-1� may be involvedin the susceptibility to HAPE (Mortimer et al., 2004).
The cardiovascular parameters did not allow any discriminationbetween the groups. The increase in cardiac output at rest underhigh altitude exposure was mostly due to an elevation in HR, whilechanges in stroke volume only played a minor role in the acute car-diovascular response (Vogel and Harris, 1967). In our study, plasmaVEGF release was profoundly stimulated by exercise and hypoxia inthe HAPE-S group. Some authors concluded that VEGF was unlikelyto induce any critical pulmonary vascular permeability variationin HAPE-prone people (Pavlicek et al., 2000). Interestingly, otherauthors reported that VEGF release was significantly increased inblood samples of mountaineers, 24 h after their arrival at 4559 m(Walter et al., 2001). Our results clearly showed an increased secre-tion of the VEGF protein in the HAPE-S group, leading to thespeculation that this factor might play a significant role in thephysiopathology of the disease. Finally, the higher oxidative stressreported in HAPE-S group corroborates the hypothesis that ROS isinvolved in the pulmonary endothelial hyperpermeability and pul-monary arterial hypertension occurring in HAPE (Crosswhite andSun, 2010). Hypoxic conditions were shown to increase the rate ofROS generation mainly by mitochondrial dysfunction causing anexcessive leakage of electrons from the respiratory chain (Kehrerand Lund, 1994). However, the values of plasma VEGF and oxida-tive stress should be interpreted with caution since they might notreflect exactly what happens in the lungs.
In conclusion, individual increases of PASP during hypoxic exer-cise from basal resting normoxic values may be used to detectsusceptibility to HAPE. The absence of an overlap in these con-ditions justifies the use of Doppler echocardiography to measurePASP increases using the Richalet’s test (Brugniaux et al., 2006;Richalet et al., 1988). However, our protocol and the associated cut-off value of change in PASP need to be tested in an independentpopulation exposed to hypoxia in order to verify its real validityand utility in HAPE prevention. The prevalences of HAPE eventsin mountaineers at 4500 m (0.2–6.0%) and of an abnormal PASPresponse to hypoxia in healthy subjects (9–10%) (Dehnert et al.,2005) should orient the screening of inexperienced person whowants to undertake a high altitude mountain expedition.
Acknowledgements
The authors cheerfully thank all the mountaineers for their par-ticipation. Finally, we thank all the personnel from the serviceof Sport and Respiratory Medicine at the Hospital of Clermont-Ferrand.
References
Allemann, Y., Sartori, C., Lepori, M., Pierre, S., Melot, C., Naeije, R., Scherrer, U., Mag-giorini, M., 2000. Echocardiographic and invasive measurements of pulmonaryartery pressure correlate closely at high altitude. Am. J. Physiol. Heart Circ. Phys-iol. 279, H2013–H2016.
Astrand, P.O., Ryhming, I., 1954. A nomogram for calculation of aerobic capacity(physical fitness) from pulse rate during sub-maximal work. J. Appl. Physiol. 7,218–221.
Bartsch, P., Maggiorini, M., Ritter, M., Noti, C., Vock, P., Oelz, O., 1991. Prevention ofhigh-altitude pulmonary edema by nifedipine. N. Engl. J. Med. 325, 1284–1289.

logy &
B
C
D
G
H
H
H
HH
K
K
M
M
M
M
P
high-altitude exposure on vascular endothelial growth factor levels in man. Eur.J. Appl. Physiol. 85, 113–117.
R. Mounier et al. / Respiratory Physio
rugniaux, J.V., Schmitt, L., Robach, P., Jeanvoine, H., Zimmermann, H., Nicolet, G.,Duvallet, A., Fouillot, J.P., Richalet, J.P., 2006. Living high-training low: toleranceand acclimatization in elite endurance athletes. Eur. J. Appl. Physiol. 96, 66–77.
rosswhite, P., Sun, Z., 2010. Nitric oxide, oxidative stress and inflammation in pul-monary arterial hypertension. J. Hypertens. 28, 201–212.
ehnert, C., Grunig, E., Mereles, D., von Lennep, N., Bartsch, P., 2005. Identificationof individuals susceptible to high-altitude pulmonary oedema at low altitude.Eur. Respir. J. 25, 545–551.
runig, E., Mereles, D., Hildebrandt, W., Swenson, E.R., Kubler, W., Kuecherer, H.,Bartsch, P., 2000. Stress Doppler echocardiography for identification of suscep-tibility to high altitude pulmonary edema. J. Am. Coll. Cardiol. 35, 980–987.
ackett, P.H., Rennie, D., Levine, H.D., 1976. The incidence, importance, and prophy-laxis of acute mountain sickness. Lancet 2, 1149–1155.
ackett, P.H., Roach, R.C., Hartig, G.S., Greene, E.R., Levine, B.D., 1992. The effect ofvasodilators on pulmonary hemodynamics in high altitude pulmonary edema:a comparison. Int. J. Sports Med. 13 (Suppl. 1), S68–S71.
ohenhaus, E., Paul, A., McCullough, R.E., Kucherer, H., Bartsch, P., 1995. Ventilatoryand pulmonary vascular response to hypoxia and susceptibility to high altitudepulmonary oedema. Eur. Respir. J. 8, 1825–1833.
ouston, C., 1960. Acute pulmonary edema of high altitude. N. Engl. J. Med., 263.ultgren, H.N., Grover, R.F., Hartley, L.H., 1971. Abnormal circulatory responses to
high altitude in subjects with a previous history of high-altitude pulmonaryedema. Circulation 44, 759–770.
ehrer, J.P., Lund, L.G., 1994. Cellular reducing equivalents and oxidative stress. FreeRadic. Biol. Med. 17, 65–75.
leinbongard, P., Dejam, A., Lauer, T., Jax, T., Kerber, S., Gharini, P., Balzer, J., Zotz,R.B., Scharf, R.E., Willers, R., Schechter, A.N., Feelisch, M., Kelm, M., 2006. Plasmanitrite concentrations reflect the degree of endothelial dysfunction in humans.Free Radic. Biol. Med. 40, 295–302.
ortimer, H., Patel, S., Peacock, A.J., 2004. The genetic basis of high-altitude pul-monary oedema. Pharmacol. Ther. 101, 183–192.
ounier, R., Pialoux, V., Robach, P., Schmitt, L., Richalet, J.P., Coudert, J., Fellmann, N.,Clottes, E., 2009a. Effects of acute hypoxia tests on blood markers in high levelendurance athletes. Eur. J. Appl. Physiol. 106, 713–720.
ounier, R., Pialoux, V., Cayre, A., Schmitt, L., Richalet, J.P., Robach, P., Lasne, F.,Roels, B., Millet, G., Coudert, J., Clottes, E., Fellmann, N., 2006. Leukocyte’s Hif-1 expression and training-induced erythropoietic response in swimmers. Med.Sci. Sports Exerc. 38, 1410–1417.
ounier, R., Pialoux, V., Roels, B., Thomas, C., Millet, G., Mercier, J., Coudert, J., Fell-
mann, N., Clottes, E., 2009b. Effect of intermittent hypoxic training on HIF geneexpression in human skeletal muscle and leukocytes. Eur. J. Appl. Physiol. 105,515–524.avlicek, V., Marti, H.H., Grad, S., Gibbs, J.S., Kol, C., Wenger, R.H., Gassmann, M., Kohl,J., Maly, F.E., Oelz, O., Koller, E.A., Schirlo, C., 2000. Effects of hypobaric hypoxia
Neurobiology 179 (2011) 294– 299 299
on vascular endothelial growth factor and the acute phase response in subjectswho are susceptible to high-altitude pulmonary oedema. Eur. J. Appl. Physiol.81, 497–503.
Pialoux, V., Mounier, R., Ponsot, E., Rock, E., Mazur, A., Dufour, S., Richard, R., Richalet,J.P., Coudert, J., Fellmann, N., 2006. Effects of exercise and training in hypoxia onantioxidant/pro-oxidant balance. Eur. J. Clin. Nutr. 60, 1345–1354.
Rathat, C., Richalet, J.P., Herry, J.P., Larmignat, P., 1992. Detection of high-risk subjectsfor high altitude diseases. Int. J. Sports Med. 13 (Suppl. 1), S76–S78.
Richalet, J.P., Kéromés, A., Dersch, B., Corizzi, F., Mehdioui, H., Pophillat, B., Chardon-net, H., Tassery, F., Herry, J.P., Rathat, C., Chaduteau, C., Darnaud, B., 1988.Caractéristiques physiologiques des alpinistes de haute altitude. Sci. Sports 3,89–108.
Rock, E., Astier, C., Lab, C., Malpuech, C., Nowacki, W., Gueux, E., Mazur, A., Rayssigu-ier, Y., 1995. Magnesium deficiency in rats induces a rise in plasma nitric oxide.Magnes. Res. 8, 237–242.
Sartori, C., Allemann, Y., Trueb, L., Delabays, A., Nicod, P., Scherrer, U., 1999. Aug-mented vasoreactivity in adult life associated with perinatal vascular insult.Lancet 353, 2205–2207.
Sartori, C., Allemann, Y., Trueb, L., Lepori, M., Maggiorini, M., Nicod, P., Scher-rer, U., 2000. Exaggerated pulmonary hypertension is not sufficient to triggerhigh-altitude pulmonary oedema in humans. Schweiz. Med. Wochenschr. 130,385–389.
Scherrer, U., Vollenweider, L., Delabays, A., Savcic, M., Eichenberger, U., Kleger, G.R.,Fikrle, A., Ballmer, P.E., Nicod, P., Bartsch, P., 1996. Inhaled nitric oxide for high-altitude pulmonary edema. N. Engl. J. Med. 334, 624–629.
Swenson, E.R., Maggiorini, M., Mongovin, S., Gibbs, J.S., Greve, I., Mairbaurl, H.,Bartsch, P., 2002. Pathogenesis of high-altitude pulmonary edema: inflamma-tion is not an etiologic factor. JAMA 287, 2228–2235.
Thomas, S.R., Witting, P.K., Drummond, G.R., 2008. Redox control of endothelial func-tion and dysfunction: molecular mechanisms and therapeutic opportunities.Antioxid. Redox Signal 10, 1713–1765.
Vachiery, J.L., McDonagh, T., Moraine, J.J., Berre, J., Naeije, R., Dargie, H., Peacock, A.J.,1995. Doppler assessment of hypoxic pulmonary vasoconstriction and suscep-tibility to high altitude pulmonary oedema. Thorax 50, 22–27.
Vogel, J.A., Harris, C.W., 1967. Cardiopulmonary responses of resting man duringearly exposure to high altitude. J. Appl. Physiol. 22, 1124–1128.
Walter, R., Maggiorini, M., Scherrer, U., Contesse, J., Reinhart, W.H., 2001. Effects of
Yock, P.G., Popp, R.L., 1984. Noninvasive estimation of right ventricular systolic pres-sure by Doppler ultrasound in patients with tricuspid regurgitation. Circulation70, 657–662.