Embed Size (px)
Citation preview

Pulmonary Complications in HIV
By
Andrew Walker
Medical Rotation

1. To understand the basic physiology of HIV and AIDS.
2. To outline the respiratory complications associated with HIV; particularly PCP.
3. To investigate the diagnosis of PCP and TB4. Physiotherapy for these patients.
Objectives

Physiology of HIV and AIDs
• HIV is a retrovirus and is divided into two types: HIV-1 and HIV-2.
• HIV-2 is mainly endemic in western Africa.
• The chief targets for the HIV virion are the CD4 T-lymphocytes.
• Infection occurs when the gp-120 envelope attaches to the host cells CD4 receptor.

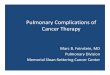
HIV virion

Viral Action
• On attachment, viral contents are then released into the host cells cytoplasm.
• Viral reverse transcriptase produces viral DNA within the host and it is then integrated into the host cells genome.
• Viral reverse transcriptase is very error prone, leading to high mutation rate – leading to the inability of host defence.

• The CD4 T-cells have essential helper/inducing function in both cellular and humoral arms of specific immunity.
• The depletion of peripheral CD4 T-cells and progression to AIDS is driven by the HIV viral burden.
• Hence, key biochemistry markers for HIV infection are the viral load and CD4 count.
CD 4 Effects

CD4 and AIDs defining illness
• Once an individual is infected with HIV, damage to the immune system leads to the development of AIDs defining illnesses.
• When diagnosing these illnesses, the CD4 count is an important diagnostic factor.
• AIDs defining illnesses tend to occur with specific CD4 levels

Pulmonary Complications
• CD4<500 - Recurrent bacterial pneumonias, Pulmonary mycobacterial pneumonia (Non- TB)
• CD4<200 - Pneumocystis carinii pneumonia (PCP), Cryptococcus neoformans pneumonia, Bacterial pneumonia (associated with sepsis)
• CD4<100 - Pulmonary Kaposi's Sarcoma, Toxoplasma pneumonitis.
• CD4<50 - Disseminated Histoplasma capsulatum, Disseminated Mycobacterium avium complex, Aspergillus pneumonia, Candida pneumonia.

PCP
• Pneumonia caused by the fungi - Pneumocystis carinii.
• A widespread organism in the environment, but not present in healthy individuals.
• In immune compromised states, such as HIV, PCP can occur.
• PCP is often the first infection that may be noticed in a patient that leads to HIV diagnosis

PCP - symptoms
• Fever
• Dry Cough
• SOB, particularly on exertion
• ↑ Respiratory rate

PCP - diagnosis
• Chest X-ray – bilateral interstitial infiltrates
• Sputum Induction
• Bronchoscopy – with lavage
• Lung Biopsy – last choice in diagnosis



Physiotherapy
• What can physiotherapy do for these patients?• We can be involved in diagnosis using normal
respiratory physiotherapy skills and also using induced sputum technique, for those patients who have an unproductive cough.
• Induced sputum as a diagnosis for PCP, mycobacterium tuberculosis (MTB) and unspecified mycobacterium is being presented at congress by Melissa Irwin an HIV clinical specialist physiotherapist.

Induced Sputum Procedure
• Rationale: The use of hypertonic saline inhaled through an ultrasonic nebuliser to produce irritant particles small enough to reach the small airways and alveoli through ACBT.
Main Requirements/equipment: Ultrasonic nebuliser Hypertonic saline – Requires prescription Negative Pressure Room Pulse oximeter Infection control policy

Important notes on induced sputum
• It is important to note that this procedure takes 30-60mins to complete to get the required samples.
• Patients in bronchospasm, pleural effusion, heart failure, haemoptysis should be excluded.
• Due to the multi-pathological nature of HIV, particularly with those patients with CD4<250, 5 samples should be taken. One sent for PCP testing and 3 for MTB and 1 for MC+S.

Other forms of physiotherapy
• Once patients are medically stable (In PCP, by prescription of septrin), rehabilitation will be required.
• This will need to take the form of strength and cardiovascular training, as the patient will likely be deconditioned
• Our treatment will be more efficacious if the appropriate MDT members are referred; dietician, pharmacists, microbiologists etc.

Conclusion
• We can be involved in assisting the diagnosis of PCP and other respiratory complications if equipment is available.
• We can be involved in helping control features associated with the respiratory complications – I.e. sputum clearance, breathing control.
• We can be involved in the later rehabilitation of the patient as an active part of the MDT.

References
• Miller, R.F et al.Sputum induction for the diagnosis of pulmonary disease in HIV positive patients. J Infect 1991 Jul: 23(1): 5-15
• Gershman, N.H. Comparison of two methods of collecting induced sputum. Eur Respir J. 1996: 9:2448-2453
• Leigh, T.R et al. Sputum induction for the diagnosis of Pneumocystis carini pneumonia. Lancet 1989 (22 July): 205-206.
• Turner D, Schwarz Y, Yust I. Induced sputum for diagnosing Pneumocystis carinii pneumonia in HIV patients: new data, new issues. Eur Respir J. 2003 Feb;21(2):204-8.
• Pneumocystis Carinii Pneumonia http://www.emedicine.com/MED/topic1850.htm
• Respiratory symptoms in HIV-infected patients http://www.medical-library.org/journals2a/respiratory_HIV.htm