Embed Size (px)
Citation preview
Page | 1
Page | 2
Putting people at the centre of GP commissioning:
experience led commissioning
“It is not often you hear about truly innovative approaches. This is one.
Its potential to support delivery of patient centred commissioning is exciting.”
Dr James Kingsland, National Clinical Commissioning Lead, Department of Health
“This approach offers a really effective way of incorporating users’ views
into the commissioning process. We look forward to its wider use and
adaptation across the country.”
Dr Brian Fisher, NHS Alliance Lead for Patient and Public Involvement
"How we bring patient experience to bear on commissioning decisions is
a fundamental question about which we have very little clarity.
Experience led commissioning is a fascinating and rich model that seeks to
provide that clarity, and now needs to be tried in the field".
Jeremy Taylor, Chief Executive, National Voices
Page | 3
Policy context
The publication of the recent White Paper Equity and excellence: liberating the NHS1 signals
that in less than two years, GP commissioning consortia will have full responsibility for
commissioning the vast majority of NHS care.
In this transitional period, the challenge is working out how GP commissioning will differ
from what has gone before and what good GP commissioning looks like. Doing this,
alongside managing transition, is a huge challenge. It requires the collective wisdom of all
those who have insights to share.
We believe this is a time of great opportunity and provides the chance to do things
radically differently. The White Paper emphasises the priority it attaches to ‘putting
patients and the public first’, and notes that:
“The NHS....scores relatively poorly on being responsive to the patients it serves. It
lacks a genuinely patient-centred approach in which services are designed around
individual needs, lifestyles and aspirations. Too often, patients are expected to fit
around services, rather than services around patients. [section 1.9]
Healthcare systems are in their infancy in putting the experience of the user first,
and have barely started to realise the potential of patients as joint providers of
their own care and recovery. Progress has been limited in making the NHS truly
patient led. [section 2.2]”
It signals that the NHS must live by the motto ‘no decision about me without me’. This
means, by implication, that GP commissioning must do the same since the decisions that GP
commissioners make will directly impact on the care of patients.
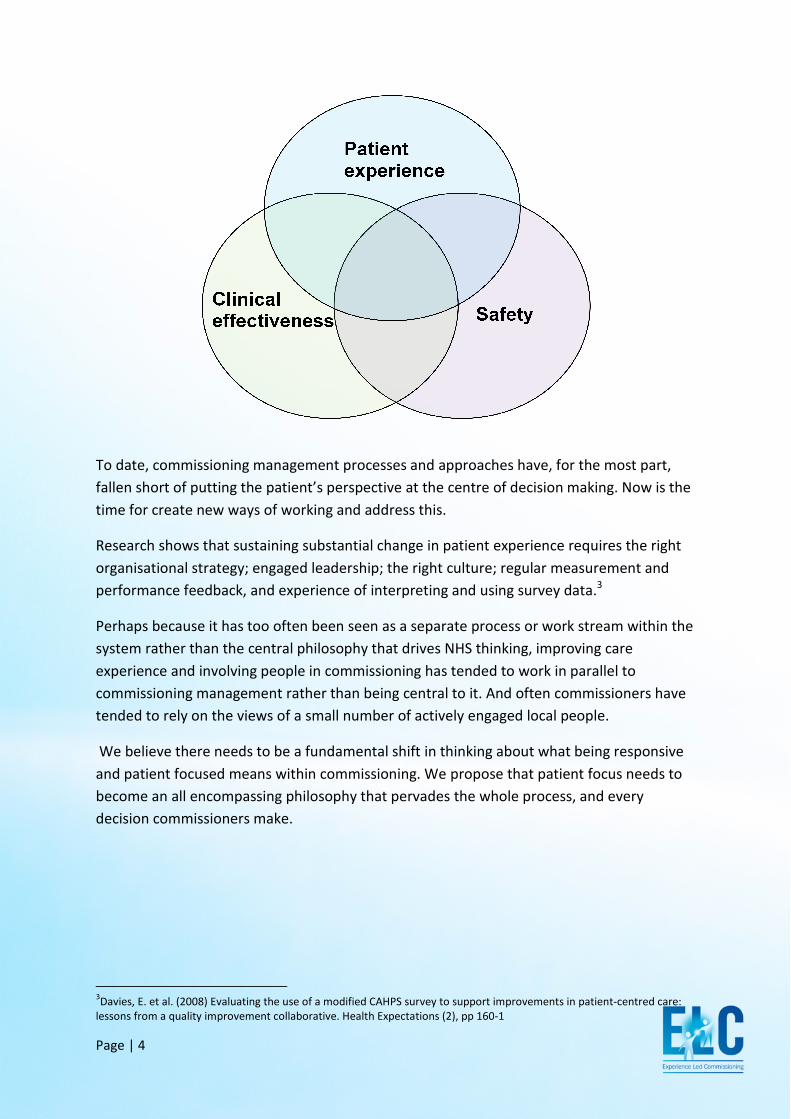
Transparency in Outcomes - a framework for the NHS 2 sets experience alongside
effectiveness and safety as the three domains of quality against which the NHS will be
monitored and around which improvement will focus.
1 Department of Health. (2010) Equity and excellence: liberating the NHS. London: Department of Health
2 Department of Health. (2010) Transparency in outcomes – a framework for the NHS. London: Department of Health
Page | 4
To date, commissioning management processes and approaches have, for the most part,
fallen short of putting the patient’s perspective at the centre of decision making. Now is the
time for create new ways of working
Research shows that sustaining substantial change in patient experience requires the right
organisational strategy; engaged leadership; the right culture; regular measurement and
performance feedback, and experience of interpreting and using survey data
Perhaps because it has too often been seen as a separate process or work stream within the
system rather than the central philosophy that drives NHS thinking, improving care
experience and involving people in commissioning has
commissioning management
tended to rely on the views of a small number of actively engaged local people.
We believe there needs to be
and patient focused means within commissioning. We propose that patient focus needs to
become an all encompassing philosophy that pervades the whole process, and every
decision commissioners make.
3Davies, E. et al. (2008) Evaluating the use of a modified CAHPS survey to support improvements in patient
lessons from a quality improvement collaborative. Health Expectations (2), pp 160
To date, commissioning management processes and approaches have, for the most part,
fallen short of putting the patient’s perspective at the centre of decision making. Now is the
time for create new ways of working and address this.
t sustaining substantial change in patient experience requires the right
organisational strategy; engaged leadership; the right culture; regular measurement and
performance feedback, and experience of interpreting and using survey data
often been seen as a separate process or work stream within the
system rather than the central philosophy that drives NHS thinking, improving care
experience and involving people in commissioning has tended to work in parallel to
rather than being central to it. And often commissioners have
tended to rely on the views of a small number of actively engaged local people.
there needs to be a fundamental shift in thinking about what being responsive
and patient focused means within commissioning. We propose that patient focus needs to
become an all encompassing philosophy that pervades the whole process, and every
decision commissioners make.
. (2008) Evaluating the use of a modified CAHPS survey to support improvements in patient
quality improvement collaborative. Health Expectations (2), pp 160-1
To date, commissioning management processes and approaches have, for the most part,
fallen short of putting the patient’s perspective at the centre of decision making. Now is the
t sustaining substantial change in patient experience requires the right
organisational strategy; engaged leadership; the right culture; regular measurement and
performance feedback, and experience of interpreting and using survey data.3
often been seen as a separate process or work stream within the
system rather than the central philosophy that drives NHS thinking, improving care
in parallel to
. And often commissioners have
tended to rely on the views of a small number of actively engaged local people.
shift in thinking about what being responsive
and patient focused means within commissioning. We propose that patient focus needs to
become an all encompassing philosophy that pervades the whole process, and every
. (2008) Evaluating the use of a modified CAHPS survey to support improvements in patient-centred care:
Page | 5
We have developed an innovative approach to help commissioners and care managers to:
• Create the right organisational strategies;
• Engage leadership across the health economy;
• Drive cultural change;
• Effectively use performance feedback and survey data to improve experience
so that being experience-led becomes ‘the way we do things around here’.
We recognise that focusing on this may seem particularly challenging at a time of great
financial pressure. Yet in fact, our analysis of health experience research tells us that many
of things that matter most to people, including co-ordination and integration; information
and education are the very things that create a more efficient and joined up care system.
It is also important to remember that many of the things patients say they want most - such
as emotional support, kindness, human empathy and dignity - often cost little or nothing at
all.
And whilst improving patient experience does not always save money in easy to measure
ways, there is a well documented link between poor patient experience and poor outcomes
of care – and we know improved outcomes will reap both financial and social returns.
Page | 6
Introducing experience led commissioning (ELC)
There is increasing interest in improving experience and a willingness to engage with this
agenda amongst providers and commissioners alike.
We believe we have found a way in which we can help people take an evidence based
approach and address what is ultimately a major cultural shift for some.
The package of management tool and processes we have developed, using the secondary
analysis of existing health experience research combine both commissioning and care
management ‘process’ tools with narrative based change and internal communication
management techniques that drive cultural change.
By holding health experience research up as a mirror to commissioners and providers, we
have observed that it helps commissioners remain focused and people-centred, and gives
them confidence that their decisions reflect what really matters to those using services.
In this way, the ELC process underpins and supports a change in organisational and
individual attitudes and beliefs, which we know to be the precursor to changed behaviour.
By setting out to win the hearts and minds of managers, professionals and staff as part of
successful commissioning of a good care, we believe we are creating a powerful programme
that fundamentally redefines what commissioning is about and will help the new system be
systematically patient centred from the start.

Page | 7
The theoretical background to ELC
Experimental research on narrative persuasion theory4 5 finds that if a person becomes
absorbed in a story, the story is likely to have a significant impact on the person’s beliefs
and attitudes. Oral and written narrative accounts have the ability to capture the listener’s
imagination and create a bridge of empathic connection that illuminates the life-world of
another person. For this reason, narratives are a powerful way to engage commissioners
and care providers at a deep emotional level in thinking about health services from the
patient’s perspective, allowing the discovery of new paths to service improvement6 7 .
Detailed patient accounts of their experiences can reveal what patients value in existing
services, what patients do not value, and what matters to them most. Analysis of patient
experiences can identify barriers to accessing services, problems not previously recognised,
and solutions to problems that may not occur to people who are immersed in the process of
commissioning or service delivery8 9 .
Many NHS organisations are now successfully experimenting with ways of gathering
qualitative user views and using them to improve services. When we combine this with the
use of rigorous research with a broad sample of users and a full range of different
perspectives, it creates a powerful rationale for change.
4 Green MC & Brock TC. (2000). The role of transportation in the persuasiveness of public narratives. J Personality and Soc
Psychol. 79(5):701-21
5 Green MC, Strange JJ and Brock TC (eds.) (2002) Narrative impact: social and cognitive foundations. Mahwah NJ:
Lawrence Erlbaum Associates
6 Greenhalgh T, Russell J & Swinglehurst D. (2005) Narrative methods in quality improvement research. QSHC 14:443-449
7 Bate SP and Robert G. (2007) Bringing User Experience to Healthcare Improvement: the Concepts, Methods and Practices
of Experience-Based Design. Oxford: Radcliffe Publishing
8 Locock L. (2001) Maps and Journeys: Redesign in the NHS. Birmingham: University of Birmingham
9 Iles V & Sutherland K. (2001) Organisational change: a review for health care managers, professionals and researchers.
London: SDO
Page | 8
What does ELC entail?
The hypothesis that underpins ELC is that unless you really understand the experiences of a
broad range of service users, you will tend to base commissioning decisions on assumptions,
personal beliefs and anecdotal experiences.
In a worst case scenario, one individual, shouting very loudly, could effectively succeed in
driving commissioners to make whole scale system change that may not be necessary or the
best use of public money – and may not even be viewed as important by the vast majority of
local service users and clinical staff. What is more, when a wealth of existing research
exists, there really is no need to use individual views as the basis of commissioning and
service design decisions.
You could say, we are creating an ‘evidence based’ approach to patient centred
commissioning and service design.
The Health Experiences Research Group (HERG) at the University of Oxford collects rigorous
qualitative interview studies on experiences of health and illness. The group has an archive
form of over 2,000 interviews covering more than 55 health conditions, all collected in the
last 10 years.
The research group collaborate with the DIPEx charity to publish analysis and carefully
selected extracts from the interviews on two websites: www.healthtalkonline.org and
www.youthhealthtalk.org, thus making the research directly available to the public, patients
families and carers. The archive is also an unrivalled source for secondary analysis of patient
experiences.
We believe that targeted secondary analysis of the HERG interview collections could provide
commissioners and service providers with narratives and robust insight data that improve
their ability to see their world through the eyes of service users.
Page | 9
Beyond anecdote: understanding most people’s health experience
The interviews collected and analysed by HERG provide a rigorous, evidence-based
summary of patients’ experiences of a particular condition. Sampling ensures coverage of a
broad range of different types of people and different types of experience. We believe the
themes identified in these national studies cover very similar ground to what local people
would tell us matters most to them. To test this, we have conducted a scoping study,
comparing a ‘best in class’ PCT experience led commissioning process where the PCT
invested heavily in extensive local experience research in end of life care with a secondary
analysis of an existing HERG end of life care health experience data set10
, collected in line
with the high level qualitative research methodology used by the Health Experiences
Research Group11
.
The comparative thematic analysis across the two pieces of research showed that the vast
majority of experience themes identified in the local study had already been identified in
the national data set. The more extensive national study also identified several additional
themes in patient experiences that were not identified in the local study and that would also
be likely to be important for local patients, including preferences for palliative care and
where to die and the importance of advance refusals and getting affairs in order. Themes
identified in the local study that were not identified in the national study concerned aspects
such as local access and opening hours of particular local services.
This is encouraging. It suggests that combining:
• Secondary analysis of qualitative interview studies collected throughout the UK
• A targeted local programme of user and carer engagement underpinned by material
based on the national data; and
• Feedback and analysis of performance management data from local providers,
collected with the specific purpose of helping commissioners to understand the
quality of local services and what it is like to experience the local service, focusing
especially closely on the key touch points that we know impact on people’s service
experience
would enable commissioners to create a rigorous, integrated and vitally important, cost
effective approach to experience led commissioning that enjoys economies of scale where
it can; ensures a robust experience data set underpins commissioning, whilst enabling local
variations to be recognised, measured and addressed.
10
Calabrese J. (2010) A Comparison of Data on Patient Experiences of End of Life Care. Oxford: Green Templeton
College
11
http://www.healthtalkonline.org/Overview/Research

Page | 10
Progress to date
National dataset: we have developed a standard process to undertake secondary analysis
of existing health experience research data sets to create generic condition specific ELC data
sets for commissioner and care providers to use.
These will help fast track clinicians’ and health managers’ understanding and ability to
become truly patient focused by increasing their ability to walk in the shoes of service users.
The next step to take this national work forward is attracting funding to undertake
secondary analyses and translate them into ELC data sets, and to do the original research to
plug a number of important gaps e.g. people’s experience of COPD and dementia.
We also need to create a sustainable way of providing and refreshing this data over time
and making it available for NHS commissioners and providers to use. Georgina Craig
Associates, HERG and University of Oxford and Green Templeton College are working
together to explore how best to do this.
We believe that these ELC data sets will form a key part of the commissioning support
information that GP commissioners will want and need to access to deliver patient centred
commissioning.
Local implementation process: We hypothesise that responding to and addressing the
critical touch points identified in the ELC data sets in a highly focused way will deliver the
vast majority of the quality improvement benefits from a patient’s perspective.
We also anticipate that many of these changes will be small, incremental and often low cost
or cost neutral for providers; yet could generate savings across the system.
This is borne out by examples of good practice we know of. For instance, Principia, a
Nottinghamshire based GP commissioning group found that when they used patient
interviews to inform their commissioning of COPD service, the fear they heard in people’s
voices when they talked about facing a weekend without access to a GP led them to
reassess the importance of commissioning additional community nursing. Following the
introduction of more community nursing support, unplanned admissions to hospital fell
significantly, and thus so did the overall cost of care. People’s fears were addressed and
their experience of care improved – and costs fell.

Page | 11
We are working with existing and emerging GP commissioning groups to explore and scope
the local engagement elements of our programme. Issues we are scoping with GP
commissioners include:
• How does ELC change the quality of the questions commissioners ask?
• What kind of local user and carer engagement needs to happen to ensure we
validate and test the relevance of the national data fully with local health and service
experience and understand the similarities, differences and unique local issues?
• When should commissioners engage providers and how can providers help co design
their contracts so they focus on improving the quality of care experience?
• How can ‘must do’ performance management processes that are being developed
centrally be streamlined so that we minimise local commissioners’ management
work load, whilst ensuring they have the management data they need to truly judge
how well they are succeeding in commissioning providers to deliver a high quality
service experience?
• How do we effectively drive the cultural change necessary within local
commissioning and provider organisations to embed a patient centred approach and
make it ‘the way we do things around here’?
• How do we disseminate this work and scale it up across the country?
• How do we build on the evident interest and enthusiasm for learning from patients
and experiences of health care?
We are currently seeking funding to undertake the necessary scoping work to answer these
questions and test our prototype commissioning management and organisation
transformation tools, and ensure they can be adapted to any health condition by populating
them with the relevant ELC data set.
Page | 12
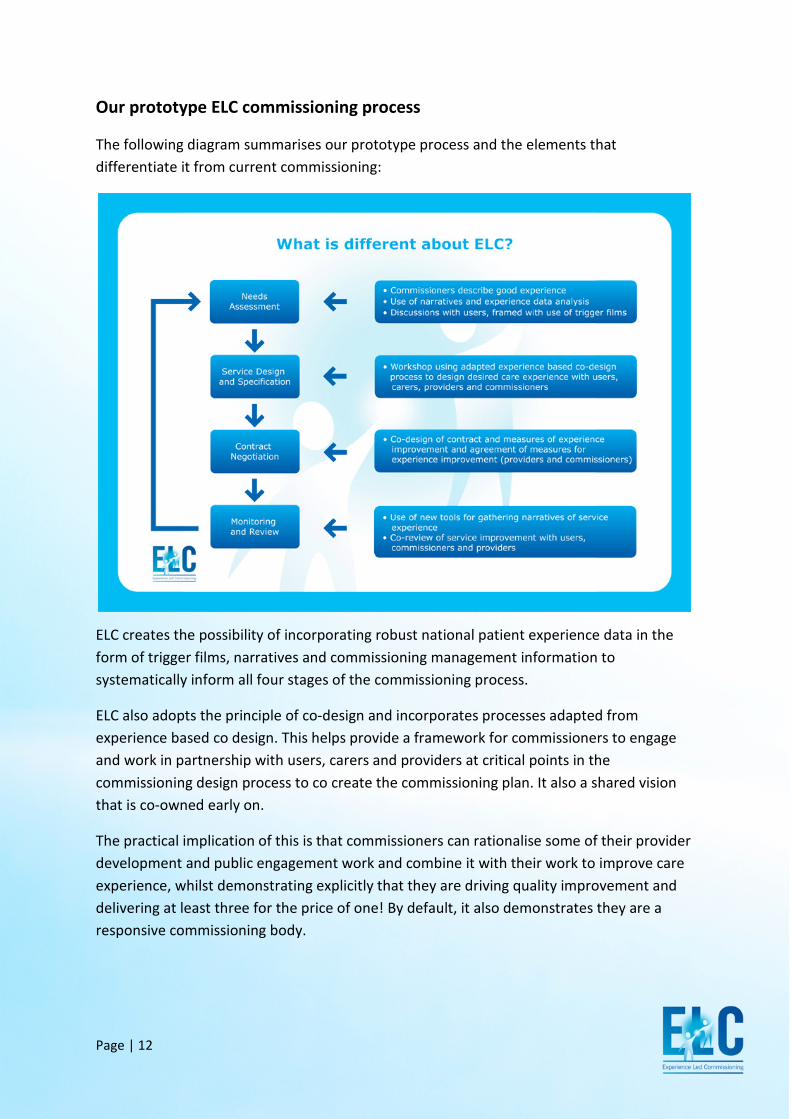
Our prototype ELC commissioning process
The following diagram summarises our prototype process and the elements that
differentiate it from current commissioning:
ELC creates the possibility of incorporating robust national patient experience data in the
form of trigger films, narratives and commissioning management information to
systematically inform all four stages of the commissioning process.
ELC also adopts the principle of co-design and incorporates processes adapted from
experience based co design. This helps provide a framework for commissioners to engage
and work in partnership with users, carers and providers at critical points in the
commissioning design process to co create the commissioning plan. It also a shared vision
that is co-owned early on.
The practical implication of this is that commissioners can rationalise some of their provider
development and public engagement work and combine it with their work to improve care
experience, whilst demonstrating explicitly that they are driving quality improvement and
delivering at least three for the price of one! By default, it also demonstrates they are a
responsive commissioning body.
Page | 13
Taking the building blocks of commissioning, here is a brief description of ELC:
• Needs assessment: The ELC approach sees commissioners combining public
health, socio economic, demographic, epidemiological and service usage data,
alongside any pre-existing local information about how people experience services
with the relevant national ELC data set, created using the condition specific
secondary analysis of qualitative interviews collected by HERG. These data sources
combined create a rich picture of local need. Once a national ELC data set is
available, it can be used by all GP commissioning groups that want to adopt an ELC
approach. ELC data is presented in a number of format, including: management
reports, narratives and triggers films. We then encourage commissioners to test
their assumptions about how a good experience should be, against the evidence
from experience research before they share their thinking with service users. The
second part of the ELC needs assessment process see commissioners discussing
the rich picture of local need and their emerging thinking on good experience with
service users. In a facilitated, collaborative workshop (pre-framed by a trigger film
and narratives drawn from the qualitative interviews), commissioners and users
and carers review what is known; ensure that there are no significant gaps in the
needs assessment AND have the opportunity to start to co-design what a good
care experience would feel like.
• Service design and specification: at this stage, commissioners, users and providers
engage in co design of a good care experience and discuss how high quality care
can be delivered in an integrated way. The output of this meeting is a shared vision
of ‘what good looks like’ and the critical factors for delivery. This output is co-
owned by commissioners, providers and users.
• Contracting: the next stage is for commissioners and providers to co-design the
contract that will deliver the desired outcomes. Focusing on a small number of
critical touch points that have been identified with users and carers as the biggest
priority for driving experience improvement during the previous stage, ELC sees
commissioners and providers jointly agreeing a performance management
framework that will systematically measure experience improvement. This
contracting process can be applied in the context of any willing provider, primary
contractor model or to design contractual mechanisms like CQUIN or other local
quality improvement frameworks.
Page | 14
• Monitoring and review: ELC monitoring must deliver useful management data that
will support commissioning decision making during the review phase; and ideally it
will capture narratives of care because we know these are especially compelling
and drive change. A key objective of monitoring and review is to engage staff and
motivate them to further improve care experience. We also want our monitoring
tools to encourage reflective practice at both commissioner and provider level. We
envisage review as an annual process where commissioners, providers and users
come together; understand what has changed and what the data (which may
include national surveys, narratives, complaints and compliments) tells us about
how well we have succeeded in delivering the good experience all parties signed
up to 12 months ago. Because we anticipate the system will address on a relatively
small number of nevertheless critical touch points, our pilots will establish
a very focused process. It will also help all three parties identify and prioritise the
next areas for improvement before completing the circle and revisiting the needs
assessment phase.
Page | 15
ELC and decommissioning
The current financial climate means that there is an increasing focus on decommissioning.
We believe that decommissioning is a natural process that falls out of a responsive health
care system. As technology advances, it is self evident that some services will become
obsolete.
ELC is equally powerful as decommissioning process. By providing insights into the benefits
people experience from accessing the service, it helps ensure that when a service is
decommissioned, the benefits the service delivers in terms of a good experience can be built
into the replacement service or delivered in a different, more cost effective way. An
example of how this might work is illustrated below in relation to follow up care for cancer
survivors. By redefining the commissioning challenge in terms of delivery reassurance, it
enables commissioners to think broadly about how reassurance can be delivered and costly
outpatient care decommissioned.
Page | 16
The ELC Bonus: creating a common purpose and language
We believe (and have some emerging evidence) that ELC delivers additional benefits:
1. For many years, managers and clinicians have struggled to find a common language
to underpin joint working. We believe that an ELC helps articulate a shared vision
and thus addresses this. Our early experience shows that once managers and
clinicians have a common understanding of what it really feels like to be a service
user or carer (based on a strong evidence base of experience data) they have more
constructive discussions and ask different questions that focus on the shared goal of
improving the quality of care. We believe that ELC will engender greater co-
operation between managers and clinicians.
2. We have observed that when the NHS makes clinical care pathways the basis for
commissioning, people often become territorial about segments of the pathway,
believing they belong to them. When we chunk up and shift focus beyond clinical
care and towards designing a good experience of appropriate care, mind sets also
shift. Discussions focus on changing people’s experience of care and thus on
delivering real change at the front line. We are finding when discussions about
people’s experience are evidence based, clinicians, grounded in an evidence-based
culture are convinced to change their personal beliefs and behaviour.
3. Moving, compelling user and carer stories help break down barriers. Narratives
challenge assumptions. In our early experience, this leads to a more flexible attitude
and recognition that commissioners and providers may not fully comprehend how it
feels to be on the receiving end of care. Stories help people connect with care
experience and reflect on how it can be improved. Stories change attitudes towards
the role of local service users within the commissioning design process.
A common purpose and vision across the care system (within both commissioning and
provider organisations) creates a powerful force to overcome barriers to change; build
consensus across competing interests and organisations, and drive a transformational
focus on improving patient experience. This will ultimately improve the quality of care
and support delivery of the QIPP agenda.
Page | 17
In fact, in terms of the seven factors identified as essential to patient centred care at
organisational level12
, ELC supports commissioners to deliver on all but two directly:
• Leadership at the level of the Chief Executive and Board
• A strategic vision clearly and constantly communicated
to every staff member
• Involvement of patients and families at multiple levels
• Supportive work environment for staff, which engages them in process design and
treats them with dignity and respect
• Systematic measurement and feedback
• Quality of the built environment
• Supportive technology facilitating information access for patients and
communication with their care givers
12 Shaller, D. (2007) Patient-centred care: what does it take? Oxford: Picker Institute and The Commonwealth Fund
Page | 18
Next steps
We now plan to pilot the ELC programme in end of life care with a GP commissioning group.
Once we have identified the key interventions that help to change organisational thinking
and behaviour and have tested in practice the models that underpin our commissioning
management processes, we will be looking to expand beyond end of life care to other areas.
We are looking actively at: COPD, dementia and depression.
How you can help
We are looking to recruit more strategic partner organisations who share our vision of a
patient centred GP commissioning system. We are interested in talking to organisations that
can take forward our scoping work and move into a national roll out
To talk to us about our work, contact:
Georgina Craig, Managing Director
Georgina Craig Associates Limited
Best contact number: 07879 480005
Email: [email protected]
Louise Locock
Deputy Research Director
Health Experiences Research Group, University of Oxford
Research Fellow, Green Templeton College
Email: [email protected]





























