Embed Size (px)
Citation preview

ASSAY and Drug Development TechnologiesVolume 2, Number 5, 2004© Mary Ann Liebert, Inc.
QT-Screen: High-Throughput Cardiac Safety Pharmacology byExtracellular Electrophysiology on Primary Cardiac Myocytes
Thomas Meyer,1 Christine Leisgen,1 Barbara Gonser,2 and Elke Günther2
Abstract: Cardiac safety pharmacology focuses mostly on the drug-induced prolongation of the QTinterval in the electrocardiogram. A prolonged QT interval is an important indicator for an increasedrisk of severe ventricular arrhythmia. Guidelines demand safety tests addressing QT prolongation invitro and in vivo before a drug enters clinical trials. If safety risks will be detected not until anadvanced stage of preclinical drug development, a considerable sum of money has already beeninvested into the drug development process. To prevent this, high-throughput systems have beendeveloped to obtain information on the potential toxicity of a substance earlier. We will discuss inthis publication that the QT-Screen system, which is based on primary cardiac myocytes, is able toprovide a sufficient throughput for secondary screening. With this system, extracellular fieldpotentials can be recorded from spontaneously beating cultures of mammalian or avian ventricularcardiac myocytes simultaneously on 96 channels. The system includes software-controlled andautomated eight-channel liquid handling, data acquisition, and analysis. These features allow a user-friendly and unsupervised operation. The throughput is over 100 compounds in six replicates andwith full dose–response relationships per day. This equals a maximum of approximately 6,000 datapoints per day at an average cost for consumables of $0.20 (U.S.) per data point. The system isintended for a non–good laboratory practice-compliant screening; however, it can be adapted to beused in a good laboratory practice environment.
507
Introduction
YOU CAN BREAK DOWN the complex process of drugdevelopment into two main stages: high-throughput
screening for identifying compounds that show a desiredeffect and the following characterization of positivelytested compounds (drug profiling). Testing for unwantedor even dangerous side effects takes place quite late inthe profiling stage. Before a drug candidate enters theclinical research phase, where it is tested on volunteersor very ill patients, safety-pharmacology studies are nec-essary to ensure that it is safe for human health.
National and international boards, for example, theEMEA in the European Union and the Food and DrugAdministration in the United States, constitute guidance
for these studies. International organizations like the In-ternational Conference on Harmonization of TechnicalRequirements for Registration of Pharmaceuticals forHuman Use harmonize those standards.1
One of the major difficulties in the drug discovery pro-cess is shown by the fact that only a few hundreds of po-tential drugs are identified among several hundreds ofthousands of compounds during the primary screening.In the following secondary functional screening, thesepositively tested compounds undergo more specific teststo find only the most effective potential drugs.
Only about 10–20 most promising compounds are leftin the preclinical phase. Again, the preclinical researchfocuses on the effectiveness and availability of the po-tential drug rather than on safety issues. It is only after
1Multi Channel Systems MCS GmbH, Reutlingen, Germany.2NMI Natural and Medical Sciences Institute, Tübingen University, Reutlingen, Germany.
ABBREVIATIONS: DMSO, dimethyl sulfoxide; ECG, electrocardiogram; EMEA, European Agency for the Evaluation of Medicinal Prod-ucts; hERG, human ether-a-go-go-related gene; MEA, microelectrode array.
5315_e04_p507-514 11/5/04 12:28 PM Page 507

the identification of only a few lead compounds—up to4 years after the start of the primary screening—that thesafety-pharmacological research is about to begin.
This research results in costs of up to $80 million(U.S.) per drug that enters the clinical test phase. Theseinvestments are completely lost if severe safety problemsshow up during this late stage of development. The pre-clinical research causes costs of about $367 million (U.S.)for each approved drug. In total, it takes about 12 yearsand costs about $802 million (U.S.) to get the approvalfor one out of about 10,000 compounds that have beenpositively tested in the primary screening.
To avoid any unnecessary costs, the pharmaceutical in-dustry tends to screen not only for the effectiveness of acompound, but also for safety-pharmacological risks inan earlier stage—in parallel to the secondary functionalscreening—in the recent past. These efforts have beenhampered, though, by the lack of test systems that com-bine reliable results with a medium or high throughput(at reasonable costs). This is where the QT-Screen comesinto play. It automates a novel test model based on a pri-mary cell culture of heart muscle cells (cardiomyocytes).The 96-well format is important for a medium or evenhigh throughput at low costs.
Instead of testing compounds for unwanted side effectsafter 4 years of expensive research, the QT-Screen is con-sidered to be capable of testing several hundreds of po-tential drugs for effects on the cardiovascular system al-ready at a quite early stage, after about 2 years of drugdiscovery. Safety risks will be identified much earlier be-fore high investments have been made in unusable com-pounds, thus avoiding further unnecessary costs duringlater stages of drug development.
QT Prolongation
As stated above, national and international boards con-stitute guidance for safety-pharmacology studies. In theyear 2002, casualties caused by drug-induced arrhythmiaof the heart led to the guideline S7B announced by theFood and Drug Administration.1,2 This guidance has beenacknowledged by the EMEA and other organizations.The guideline “Safety Pharmacology Studies for Assess-ing the Potential for Delayed Ventricular Repolarization(QT Interval Prolongation) by Human Pharmaceuticals”states that all new pharmaceuticals, even those that donot target the heart directly, have to be tested for an ab-normal prolongation of the QT interval in an ECG.
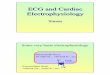
Figure 1 shows how such a QT prolongation is per-ceived by different methods of measurement.
A prolongation of the QT interval itself does not im-pair human health, but the long-QT syndrome is knownto be associated with ventricular tachycardia, torsade depointes, and lethal arrhythmia.3–6
As these factors present an unbearable risk, a reliablein vitro test system is demanded. A pharmaceutical com-pany will only ignore this risk and develop a drug can-didate with a known potency for QT prolongation if thisdrug promises to be a highly effective and extraordinar-ily innovative pharmaceutical.
QT-Screen—recording principle
This assay is based on extracellular recording of spon-taneously beating cardiomyocytes. It is a non-invasivemethod and thus allows observation of drug effects with-out damaging the cell membrane. The recorded signalsare proportional to the first derivative of the action po-tential.7 In contrast to classical electrophysiological tech-niques like patch clamp or transmembrane recordings, alabor-intensive and exact positioning of the measuringelectrode is not necessary.8–10 Here, the cells are cultureddirectly on the electrode that is integrated in the substrate.The cardiomyocytes form a monolayer of cells that areelectrically coupled by gap junctions. Only cells fromneonatal or embryonic tissue are sufficiently able to cou-
Meyer et al.508
FIG. 1. Alignment of QT intervals resulting from differentassays. The top illustration shows field potential data recordedwith the QT-Screen technology. The initial rapid component re-flects sodium channel-driven depolarization, whereas the posi-tive terminal waveform represents the repolarization. A dose-dependent prolongation of the field potential is observed witha potassium channel blocker (IKATP blocker HMR1098, 0–100�M). In the middle illustration, you can see a cardiac actionpotential as it is perceived by transmembrane recording. Thedotted line indicates how a prolonged QT interval is reflectedin the action potential. The bottom image illustrates a QT pro-longation shown by an ECG. The action potential and the ECGdrawing are illustrations.
5315_e04_p507-514 11/5/04 12:28 PM Page 508

ple in vitro. Due to the simplicity of the cell culture andthe recording principle, this technology has a high po-tential for developing an automated system.
Basically the same principle is used for the MEAsystem of Multi Channel Systems MCS GmbH (Reut-lingen, Germany). This proven technology has beenemployed for cardiac recordings since several years.7,11
The shape of the cardiac field potential was analyzedpharmacologically and by theoretical approaches.7
Even though the rapid depolarization is the most promi-nent part of the field potentials, the repolarization canbe detected as well. As cultivated cells might dediffer-entiate in culture, and as the composition of ion chan-nels varies between species, the expression level of thechicken hERG channel analogue was monitored overtime in a previous study.12 With this knowledge, it waspossible to align results obtained by classical electro-physiological assays with the data retrieved with theMEA system. We think that the interpretation of fieldpotential data for the analysis of action potential dura-tion, which correlates with the QT interval in the ECG,is an attractive alternative method for safety pharma-cologists. The high requirements of safety pharmacol-ogy are fulfilled by a simultaneous recording from 60electrodes, which provides information on conduction
velocity and excitation patterns. Recordings fromwhole hearts13 or cardiac tissue preparation reveal in-formation on spatial changes in field potential shapeand frequency.
However, for screening purposes that require a higherthroughput, the information obtained from a single elec-trode is sufficient. The data provide information on thelength of the field potential (for QT prolongation stud-ies) and allow the detection of drug-induced changes inthe intrinsic beat rate of the cells, which is a valuable in-dicator for drug-induced arrhythmia. With the QT-Screensystem, parallel recordings from 96 independent cham-bers generate data with a throughput that is suitable forsecondary screening.
QT-Screen—system description
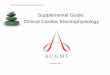
The QT-Screen system (Fig. 2A) integrates two corecomponents: the amplifier and recording unit, and the liq-uid handling system. Compound application, data acqui-sition, and analysis are software-controlled by one inte-grated and one external computer. The amplifier unithouses the QT-Well plate with 96 temperature-, humid-ity-, and CO2-controlled culture and recording chambers.The lid is opened only for a short moment during com-
QT-Screen for Cardiac Safety Pharmacology 509
FIG. 2. QT-Screen system. (A) Developed on the basis of the proven MEA technology from Multi Channel Systems and apipetting workstation from Tecan. The eight-channel dispenser is filling the recording chambers on the right side with test solu-tions. (B) Detailed view. On the left are three 96-well plate holders for stock solutions; on the right, the recording and data ac-quisition unit are visible. (C) and (D) A 96-well plate. The higher magnification reveals a substrate-integrated, round gold mi-croelectrode with a 100-�m diameter and a large octagonal reference electrode in each well.
5315_e04_p507-514 11/5/04 12:28 PM Page 509

pound application for ensuring stable environmental con-ditions.
The automated liquid handling is based on a systemdeveloped by the Tecan Group AG (Maennedorf,Switzerland) that has been adapted for the QT-Screentechnology. Stock solutions of the test compounds arestored in up to three standard 96-well plates (Fig. 2B).The QT-Screen prepares dilutions for dose–response con-centration series according to the user’s specifications.Compounds are applied to the cell cultures by an eight-channel dilutor. Preceding viability tests help to savevaluable compounds.
The QT-Well plates (Fig. 2C and D) are designed forsingle use and are supplied sterile and ready for use withcell cultures. A gold recording electrode with a diameterof 100 �m is positioned in the center of each well, sur-rounded by a large octagonal reference electrode. The ref-erence electrodes in all 96 wells are interconnected forguaranteeing a stable baseline.
Experimental Procedures
Cell culture and preparation
Cardiac myocytes can be isolated either from neona-tal rodents (rat or mouse) or from chicken embryo. Alldata shown in this publication were recorded fromchicken ventricular cell preparations. In our lab, we usedembryonic chicken (day E13). The ventricles were iso-lated and collected in 20% fetal calf serum medium: Dul-becco’s modified Eagle’s medium/nutrient mixture F-12HAM (D8062, Sigma Aldrich, Deisenhofen, Germany).The ventricular tissue was minced and transferred intophosphate-buffered saline without calcium/magnesium.Four subsequent digestion cycles of 8 min each in 0.05%trypsin (T 7409, Sigma)/phosphate-buffered saline with-out calcium/magnesium at 37°C led to isolated cells,which were collected by centrifugation and plated in adensity of approximately one E5 cells/well. The prepa-ration was routinely performed using eight eggs andyielded sufficient cell material for one 96-well plate. Thetotal time for the preparation was about 70 min. The cellswere cultured directly on the QT-Well plates—specifi-cally designed 96-well plates with integrated gold elec-trodes (recording and reference)—for 5–7 days in a stan-dard incubator at 37°C. Medium was exchanged everysecond day with a Tecan Columbus Microplate Washer.The well plate is shown in Fig. 2C, with a close-up viewin Fig. 2D.
Drug preparation
All drugs were obtained from Sigma Aldrich. For alllipophilic drugs, a stock solution of 100 mM was pre-pared with DMSO. The maximum DMSO concentration
was 0.1%. DMSO controls did not show any effect com-pared with control conditions without DMSO (data notshown).
Recording
Cells were recorded for 2 min under control condi-tions. The recording was started after a wash-in time of2 min following each compound application. Recordingtime was 2 min per concentration. Sampling frequencywas 5,000 Hz, gain was 1,200, and amplifier bandwidthwas 4 Hz to 3 kHz.
Dose–response relationships were recorded cumula-tively starting from the lowest concentration to the high-est. Thus, a full dose–response relationship was obtainedfrom each well.
Results
In order to validate the QT-Screen system, a typicalselection of reference compounds with known effects wastested. The data shown were recorded from chicken ven-tricular cardiac myocytes (E13) on day 5–7 in culture, inat least six independent experiments. Error bars indicatethe standard deviation.
As most drugs that are known to prolong the QT in-terval target the hERG potassium channel,14–16 the firstexperiment was to study the effect of a potent hERG-selective blocker. For this purpose, we selected thecompound E-4031 (Sigma). E-4031 caused a twofoldprolongation of the field potential in nanomolar concen-trations (Fig. 3). This underlines the sensitivity of the
Meyer et al.510
FIG. 3. Dose–response curves showing the influences of E-4031, sotalol, and verapamil on the field potential of cardiacmyocytes recorded with the QT-Screen technology. Normal-ized field potential duration as a percentage of control condi-tions is plotted against drug concentration in nM (decadic log-arithmic scale). Error bars reflect standard deviation; all datapoints represent the mean of at least n � 6.
5315_e04_p507-514 11/5/04 12:28 PM Page 510

system. Sotalol17–19 was tested as a classical antiar-rhythmic drug. Sotalol caused a sustained prolongationof the cardiac field potential in a micromolar concentra-tion range (Fig. 3). This is in line with other electro-physiological assays. All recordings are based on thespontaneous activity of coupled cardiomyocytes. As thisspontaneous activity is lost at high concentrations of ac-tive compounds, it is in most cases not possible to recorda plateau at high concentrations. The data were analyzedby aligning the concentrations causing a 20% prolonga-tion of the field potential.
Even though verapamil is a potent blocker of the hERGchannel, it does not cause a QT prolongation in vivo. Thisis due to the dual affinity of this drug to L-type calciumchannels and the hERG channel. Both channels areblocked with an IC50 of approximately 150 nM.20–23 Ablockade of the L-type Ca2� channel shortens the actionpotential, whereas a blockade of the hERG channel pro-longs the action potential. Both effects that can be shownin vitro cancel each other out in an in vivo situation.Therefore, verapamil is a typical false-positive in in vitroassays that are based on the hERG channel affinity alone.Remarkably, verapamil showed no effect on cardiomyo-cytes in our studies with the QT-Screen.
Another special case is quinidine (Sigma). Quini-dine12,24,25 is a class IA antiarrhythmic drug that blocksthe depolarizing sodium currents. In Fig. 4A and B, acomparison of signals under control conditions and in thepresence of 10 �M quinidine is shown. It could be shownthat the rapid component of the signal, which representssodium currents, could be substantially blocked. Figure4C shows an overlay of the waveforms on a smaller timescale. The repolarization is reflected in the positive wave-form at the end of the signal. This component can becompared with the T wave in an ECG. The QT-prolong-ing effect of quinidine is reflected in a right shift of theT wave. In addition, as the field potential prolongation iscaused by a block of the repolarizing potassium chan-nels, the amplitude of the T wave is reduced. A dose–re-sponse curve is shown in Fig. 4D.
The throughput of the QT-Screen was approximately100 compounds per day with dose–response measurementsof seven or eight concentrations. This equals approxi-mately 6,000 data points per day. Compared with othersystems (Table 1), the obtained data are of a higher qual-ity, because they are based on native cardiac myocytes.
In Table 1, the QT-Screen system is compared withother assays that address cardiac safety studies. The es-
QT-Screen for Cardiac Safety Pharmacology 511
FIG. 4. Case study of quinidine showing a typical field potential under control conditions. (A–C) Field potential in �V is plot-ted against time in s. A prominent rapid depolarization component, a small plateau, and a repolarization wave characterize theshape of the field potential. B: In the presence of 10 �M quinidine, the rapid depolarization is blocked. The peak-to-peak am-plitude is reduced from 2 mV to 700 �V. C: Overlay of waveforms recorded under control conditions and in the presence of 10 �M quinidine. The T wave is shifted by more than 200 ms to the right. D: Dose–response curve showing the field potential-prolonging effect of quinidine.
A B
C D
5315_e04_p507-514 11/5/04 12:29 PM Page 511

Meyer et al.512
TA
BL
E1.
CO
MP
AR
ISO
NO
FV
AR
IOU
SA
SS
AY
SU
SE
DIN
CA
RD
IAC
SA
FE
TY
SC
RE
EN
ING
Ass
ay
ME
A s
yste
mP
lana
r pa
tch
Xen
opus
R
adio
liga
ndF
luor
esce
nce
QT
-Scr
een
(wit
h 4
ampl
ifie
rs)
Pur
kinj
e fi
ber
Pat
ch c
lam
pcl
amp
oocy
tes
disp
lace
men
tdy
esR
ubid
ium
eff
lux
Dat
aF
ield
pot
enti
al�
Fie
ld p
oten
tial
,A
ctio
n po
tent
ial
Spe
cifi
c S
peci
fic
Spe
cifi
c hE
RG
aff
init
y,
Mem
bran
eC
hann
el s
tate
arrh
ythm
iaar
rhyt
hmia
,ch
anne
l ch
anne
lch
anne
l e.
g.,
dofe
tili
de
pote
ntia
l, co
nduc
tion
data
data
data
bind
ing
FL
IPR
velo
city
, an
dex
cita
tion
pa
tter
nsT
hrou
ghpu
t da
ta
6,00
025
050
5020
0–1,
000
800
�10
,000
�10
,000
�1,
000
poin
ts/d
ayA
utom
ated
Yes
No
No
No
Yes
Yes
Yes
Yes
Yes
syst
em e
xist
sC
an d
etec
tY
esY
esY
es (
lim
ited
)N
oN
oN
oN
oN
oN
oar
rhyt
hmia
Mea
sure
sN
oY
esY
esN
oN
oN
oN
oN
oN
oco
nduc
tion
velo
city
Cel
ls/t
issu
eE
mbr
yoni
c/E
mbr
yoni
c/P
urki
nje
fibe
rN
ativ
e ce
lls
Cel
l li
nes
Ooc
ytes
Cel
l li
nes
Cel
l li
nes
Cel
l li
nes
neon
atal
car
diac
neon
atal
an
d ce
ll l
ines
myo
cyte
sca
rdia
c m
yocy
tes
Man
ufac
ture
rM
ulti
Cha
nnel
Mul
ti C
hann
elH
EK
A,
Axo
nC
ytoc
entr
ics,
Mul
ti C
hann
elM
olec
ular
A
uror
a(s
elec
ted)
Sys
tem
sS
yste
ms
Nan
ion,
S
yste
ms,
D
evic
esS
ophi
on,
Axo
nE
vote
c A
xon
OA
IC
osts
per
dat
a$0
.20
$5–2
0$5
0$5
0$1
5$2
0$0
.15
$0.1
5$1
–10
poin
t (U
.S.)
An
over
view
on
reco
rdin
g pr
inci
ple
and
cell
s/ti
ssue
s us
ed i
s gi
ven,
and
rec
orde
d pa
ram
eter
s an
d th
roug
hput
cha
ract
eris
tics
for
var
ious
ass
ay s
yste
ms
are
list
ed. M
anuf
actu
rers
of
the
auto
mat
ed s
yste
ms
are
list
ed f
or r
efer
ence
. D
ata
wer
e ob
tain
ed f
rom
use
rs,
pers
onal
com
mun
icat
ion
wit
h th
e m
anuf
actu
rer,
and
sci
enti
fic
pres
enta
tion
s.26
–31
5315_e04_p507-514 11/5/04 12:29 PM Page 512

timated throughput and costs vary according to the sys-tem and manufacturer. The figures are obtained fromusers, manufacturers, and literature.32–34 This list is in-tended to give a rough overview rather than exact num-bers.
The spectrum of in vitro assays ranges from com-plex repolarization studies on Purkinje fiber or papil-lary muscle to simple fluorescent dye and dofetilidebinding assays. All standard electrophysiological tech-niques fail the assumption that the average cost of adata point in a high-throughput screening should be lessthan $0.50 (U.S.).
Discussion
It was shown that cardiac field potential data allow anestimation of the duration of the ventricular action po-tential. Thus, drug-induced disturbances of ventricular re-polarization are a reliable in vitro indicator for QT pro-longation in vivo. As shown above, standard referencecompounds evoke field potential prolongations in thesame concentration range as observed with standard elec-trophysiological recording techniques. This adds to thevalidation of the MEA system, which is based on a verysimilar recording principle and uses the same cell prepa-ration and species, but other electrode and recordingchamber geometries.35
The QT-Screen system was developed for satisfyingthe demands both for high-quality data from cardiac myocytes and for a high throughput.
The use of cardiac myocytes ensures that all cardiacion channels contribute to the recorded signals in theirnative environment. As there are high structural ho-mologies between the pore domains of various ionicchannels, the risk that a drug affects more than one chan-nel type is reasonably high. As shown by the example ofverapamil, dual effects might act antagonistically or syn-ergistically. The use of native cardiomyocytes greatly re-duces the risk of false positives and false negatives.
The second goal of the QT-Screen system is to ana-lyze indicators for arrhythmia in vitro. It has to be stressedthat QT prolongation is just one of the risk factors for se-vere tachyarrhythmia. No casualties have been reportedthat were directly caused by a prolonged QT interval,whereas torsades de pointe or other form of ventriculararrhythmia can be lethal.36 Therefore, the information ofwhether a drug causes proarrhythmogenic indicators likeearly or delayed after depolarizations or even arrhythmiain vitro is very important.
One might ask how important it is to obtain thesedata in an early stage of drug development such as thesecondary screening. Based on this information, a well-founded decision can be reached on whether a target-effective compound can move on to the preclinical
stage or whether its further development is cancelledto minimize safety risks and costs. To make sure thatonly the most effective and safest drugs enter clinicaltrials, safety-pharmacological studies should be per-formed as soon as possible. This screening should notonly focus on hERG channel blockers, but also takeinto account the complete physiological situation of anative cardiac myocyte, and monitor indicators forproarrhythmogenic effects as well.
However, the system presented here utilizes a noveltest system and shall be discussed in this point. The useof chicken cardiac myocytes is not a standard assay sofar. The drugs tested in this study show a response com-parable to published data obtained with established as-says and species. In this work, only a relatively smallnumber of drugs from various substance classes wastested. Further experiments are required to validate thistest model and technique. One limitation currently liesin the interpretation of the data. As shown in the fig-ures, dose–response curves can be measured, but athigh concentrations of effective hERG channel block-ers, it is not possible to observe a plateau, because highconcentrations cause a loss of spontaneous activity. Forthis reason, no classical 50% inhibitory concentra-tion/50% effective concentration value was determinedhere. Data were analyzed by measuring the concentra-tion that caused a 20% prolongation of the control fieldpotential.
In summary, our work shows that this system repre-sents an innovative way of measuring drug effects on car-diac myocytes. The increased throughput and the widerange of parameters (including arrhythmia-related data)represent the main benefits, which in our opinion out-weigh the limitations described above.
References
1. Bode G, Olejniczak K, ICH Expert Working Group: ICHtopic: the draft ICH S7B step 2: note for guidance on safetypharmacology studies for human pharmaceuticals. FundamClin Pharmacol 2002;16:105–118.
2. Barbier A, Caille D: [Regulatory status of safety pharma-cology. Implications]. Therapie 2002;57:104–108.
3. Passino C, Magagna A, Conforti F, Buralli S, KozakovaM, Palombo C, Emdin M: Ventricular repolarization is pro-longed in nondipper hypertensive patients: role of left ven-tricular hypertrophy and autonomic dysfunction. J Hyper-tens 2003;21:445–451.
4. Elming H, Sonne J, Lublin HK: The importance of the QTinterval: a review of the literature. Acta Psychiatr Scand2003;107:96–101.
5. El-Sherif N, Turitto G: Torsade de pointes. Curr Opin Car-diol 2003;18:6–13.
6. Mikheeva IS, Kheifets LM, Zakharova OV, AstrakhantsevaSS: [QT prolongation as risk factor of arrhythmias in pa-tients treated with chronic hemodialysis]. Kardiologiia2002;42:48–49.
QT-Screen for Cardiac Safety Pharmacology 513
5315_e04_p507-514 11/5/04 12:29 PM Page 513

7. Halbach M, Egert U, Hescheler J, Banach K: Estimationof action potential changes from field potential recordingsin multicellular mouse cardiac myocyte cultures. Cell Phys-iol Biochem 2003;13:271–284.
8. Egert U, Knott T, Schwarz C, Nawrot M, Brandt A, Rot-ter S, Diesmann M: MEA-Tools: an open source toolboxfor the analysis of multi-electrode data with MATLAB. JNeurosci Methods 2002;117:33–42.
9. Thomas CA Jr, Springer PA, Loeb GE, Berwald-Netter Y,Okun LM: A miniature microelectrode array to monitor thebioelectric activity of cultured cells. Exp Cell Res 1972;74:61–66.
10. Hämmerle H, Egert U, Mohr A, Nisch W: Extracellularrecording in neuronal networks with substrate integrated mi-croelectrode arrays. Biosens Bioelectron 1994;9:691–696.
11. Banach K, Halbach MD, Hu P, Hescheler J, Egert U: De-velopment of electrical activity in cardiac myocyte aggre-gates derived from mouse embryonic stem cells. Am JPhysiol Heart Circ Physiol 2003;284:H2114–H2123.
12. Anyukhovsky EP, Sosunov EA, Feinmark SJ, Rosen MR:Effects of quinidine on repolarization in canine epicardium,midmyocardium, and endocardium: II. In vivo study. Cir-culation 1997;96:4019–4026.
13. Lu ZJ, Pereverzev A, Liu HL, Weiergraber M, Henry M,Krieger A, Smyth N, Hescheler J, Schneider T: Arrhyth-mia in isolated prenatal hearts after ablation of the Cav2.3(alpha1E) subunit of voltage-gated Ca2� channels. CellPhysiol Biochem 2004;14:11–22.
14. Ackerman MJ: The long QT syndrome: ion channel dis-eases of the heart. Mayo Clin Proc 1998;73:250–269.
15. Ficker E, Obejero-Paz CA, Zhao S, Brown AM: Thebinding site for channel blockers that rescue mis-processed human long QT syndrome type 2 ether-a-gogo-related gene (hERG) mutations. J Biol Chem 2002;277:4989–4998.
16. Wang S, Morales MJ, Liu S, Strauss HC, Rasmusson RL:Modulation of HERG affinity for E-4031 by [K�]o and C-type inactivation. FEBS Lett 1997;417:43–47.
17. Advani SV, Singh BN: Pharmacodynamic, pharmacoki-netic and antiarrhythmic properties of d-sotalol, the dex-tro-isomer of sotalol. Drugs 1995;49:664–679.
18. Rizza C, Valderrabano M, Singh BN: Recurrent torsadesde pointes after sotalol therapy for symptomatic paroxys-mal atrial fibrillation in a patient with end-stage renal dis-ease. J Cardiovasc Pharmacol Ther 1999;4:129–134.
19. Ruffy R: Sotalol. J Cardiovasc Electrophysiol 1993;4:81–98.20. De Ponti F, Poluzzi E, Cavalli A, Recanatini M, Monta-
naro N: Safety of non-antiarrhythmic drugs that prolongthe QT interval or induce torsade de pointes: an overview.Drug Saf 2002;25:263–286.
21. Fossa AA, DePasquale MJ, Raunig DL, Avery MJ, Leish-man DJ: The relationship of clinical QT prolongation tooutcome in the conscious dog using a beat-to-beat QT-RRinterval assessment. J Pharmacol Exp Ther 2002;302:828–833.
22. Somberg JC: Calcium channel blockers that prolong theQT interval. Am Heart J 1985;109:416–421.
23. Nose I, Kataoka T, Honda Y, Yamada T, Ikeno A, FukuyaF, Minato H, Takeyama K, Hosoki K, Karasawa T: In vitroand in vivo electrocardiographic evaluation of the novel
calcium antagonist monatepil on cardiac conduction sys-tem. Arzneimittelforschung 1993;43:722–728.
24. Lazzara R: Antiarrhythmic drugs and torsade de pointes.Eur Heart J 1993;14(Suppl H):88–92.
25. Vaughan Williams EM: Delayed ventricular repolarizationas an anti-arrhythmic principle. Eur Heart J 1985;6(SupplD):145–149.
26. Cronk D, et al.: Cell-based high-throughput screening ofion channels using FLIPR and VIPR membrane potentialassay technology. Presented at the Society for Biomolecu-lar Screening 7th Annual Conference, 2001, Baltimore,MD.
27. Gonzalez JE, Tsien RY: Improved indicators of cell mem-brane potential that use fluorescence resonance energytransfer. Chem Biol 1997;4:269–277.
28. Gonzalez JE: Fluorescence technologies for ion transporttargets. Presented at Cambridge Healthtech Institute’sEighth Annual High Throughput Technologies, 2001, Phil-adelphia, PA.
29. Johnston P, et al.: Ionotropic glutamate receptor (iGluR’s)HTS assays: comparison of FLIPR and VIPR formats. Pre-sented at Society for Biomolecular Screening 7th AnnualConference, 2001, Baltimore, MD.
30. Loew LM: How to choose a potentiometric membraneprobe. In: Spectroscopic Membrane Probes, pp. 139–152.CRC Press, Boca Raton, FL. 1988.
31. Waggoner A: Optical probes of membrane potential. JMembr Biol 1976;27:317–334.
32. Finlayson K, Turnbull L, January CT, Sharkey J, Kelly JS:[3H]Dofetilide binding to HERG transfected membranes: apotential high throughput preclinical screen. Eur J Phar-macol 2001;430:147–148.
33. Larsen LA, Johnson M, Brown C, Christiansen M, Frank-Hansen R, Vuust J, Andersen PS: Automated mutationscreening using dideoxy fingerprinting and capillary arrayelectrophoresis. Hum Mutat 2001;18:451–457.
34. Netzer R, Ebneth A, Bischoff U, Pongs O: Screening leadcompounds for QT interval prolongation. Drug Discov To-day 2001;6:78–84.
35. Meyer TG, Boven K-H, Guenther E, Fejtl EM: Micro-elec-trode arrays (MEA): a novel tool in cardiac safety phar-macology to study QT prolongation. Drug Saf 2004;27:763–772.
36. De Ponti F, Poluzzi E, Vaccheri A, Bergman U, BjerrumL, Ferguson J, Frenz KJ, McManus P, Schubert I, Selke G,Terzis-Vaslamatzis G, Montanaro N: Non-antiarrhythmicdrugs prolonging the QT interval: considerable use in sevencountries. Br J Clin Pharmacol 2002;54:171–177.
Address reprint requests to:Dr. Thomas Meyer
Cardiovascular ResearchMulti Channel System MCS GmbH
Aspenhaustrasse 2172770 Reutlingen
Germany
E-mail: [email protected]
Meyer et al.514
5315_e04_p507-514 11/5/04 12:29 PM Page 514