Embed Size (px)
Citation preview

Clinical Endocrinology (1991) 35, 379-397
Review
Radiation oncogenesis in relation to the treatment of pituitary tumours
Arthur Jones Department of Radiotherapy, St. Bartholomew’s Hospital, London EClA 7BE, UK
(Received 2 January 1991; returned for revision 12 April 1991; finally revised 21 May 1991; accepted 3 June 1991)
Radiotherapy has been used in the treatment of pituitary disorders for the past 80 years and, with modern megavol- tage techniques, and understanding of tissue tolerances, adverse effects of treatment have been clinically uncommon. The important possible late effects-hypopituitarism; effects on hypothalamus, optic chiasm and brain; and oncogene- sis-differ in their pathogenesis, and each has to be quanti- tated differently. Hypopituitarism, dose-dependent (Littley et al., 1989) and fortunately amenable to hormonal replace- ment, is numerically the most significant. But the most important dose-limiting factor is the possible effect on optic pathways and brain, and several studies (especially the work of Sheline (1961, 1979) have indicated the optimal dosage range (for maximal effectiveness of pituitary tumour control with minimal probability of side-effects) to lie between 4000 and 5000 cGy with individual fractions of below 200 cGy per day. With such dosage regimes late visual or neurological deficit has been proved to be extremely uncommon. It follows that since the ceiling of dosage is so determined, practical interest in the stochastic process of radiation oncogenesis will relate to evocative doses at or below this level.
Late oncogenesis has proved much harder to quantify but is regarded by experienced radiation oncologists as being exceptionally rare. In the early 1960s a few cases of parasellar fibrosarcoma, which were reported after repeated courses of orthovoltage irradiation, gave rise to concern; but by a decade later (Lawrence et al., 1971) the perceived risk was considered remote, and to be related to the multiple low- energy irradiations and to a reputedly appreciable incidence of spontaneous sarcoma. In the subsequent two decades attention has been focussed on radiation-induced brain tumours in general, mainly by two developments: the increased incidence of both meningioma and glioma follow- ing X-ray epilation of the scalp for ringworm in childhood, and the occurrence of glioma as a ‘second neoplastic disorder’ (SND) after multi-modal therapy (including X- irradiation) for childhood cancer. The post-epilation studies, with their low dosage and prolonged latent periods, have entered the canon of radiobiological data for risk projection;
cranial irradiation for tumour has enabled the long-term survival of many children but the pace of reporting radia- tion-associated tumours has increased; and there have been reports of a few sequential tumours after adult irradiation. In the pituitary context, following reports by Bogdanowicz and Sachs (1974) of meningioma, and by Piatt et al. (1983) of glioma, after pituitary irradiation, there has been a small number of such cases, almost always as individual case reports and with no indication of the ‘denominator’ of incidence. Their occurrence has been viewed in the literature against the changing background of CNS oncogenesis (by some with considerable speculation) but the question of the extent which data mainly from the paediatric age-group can be extrapolated requires careful consideration.
Pituitary adenomata ate now among the few non-malig- nant tumours which are regularly subjected to therapeutic irradiation, and with subsequent survival measured in decades it is all the more necessary to examine available experience of the risk of late oncogenesis. In evaluating such risks in high-dose studies the relationship between site- specific excess risk and base-line risk is commonly considered as a function of time since exposure. To provide such a basis in the pituitary situation would, for a number of reasons, be very difficult. Clinical experience leads us to believe that such SNDs are rare; those reported have been of a number of tumour species, each correspondingly rarer and with its own specific propensity for development. The stochastic nature of carcinogenesis implies that the risk is volume-dependent, and the pituitary target-volume is one of the smallest in radio- therapy. Decades are required for both recruitment and observation, but even so no radiotherapeutic centre can expect to satisfy the necessary statistical criteria and, when the natural incidence is low, relative risk (RR) factors are prone to be fallacious. Difficulties with a retrospective multi- centre study include differences in treatment policies and the inevitable variations of technique over past decades.
In developing clinical studies of radiation oncogenesis many have followed with modifications the criteria laid down by Cahan et al. (1948) for radiation-induced bone sarcoma: evidence that the initial and second neoplastic disorders were of different cell lineage, that the SND arose in the area included within the radiation beam, and that a long latent period (of at least 3 years) had elapsed before the appearance of the new tumour. This method has two disadvantages in that spontaneous tumours arising within the irradiated volume may be misinterpreted, and that there
379

380 A. Jones Clinical Endocrinology (1991) 35
0" SUPERIOR
4MeV Q 50% I
.____- -----
is no recognition of tumours arising outside the geometric beams. But if the incidence of SNDs in relation to the pituitary target volume is low, those more remote would be even rarer and unrecognizable even by sophisticated statisti- cal techniques. For the present study the Cahan method has therefore been adopted as the initial frame of reference.
The investigation is based on a series of 332 consecutive cases of pituitary adenoma treated at this centre by a uniform method of megavoltage irradiation between 1961 and 1982, and reviewed in 1988; on an individual experience of40 years of irradiation of these and cognate tumours at megavoltage energies; and on a literature search which has been as comprehensive as possible.
Cllnicai studies
For the clinical series pituitary irradiation was carried out using 4MV or 15MV linear accelerators to deliver a lesion dose of 4500 cGy in 25 fractions in 35 days. Treatment was
4.0 crn
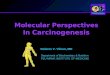
Fig. 1 Typical 4MV isodose plan used for pituitary irradiation in the 1961-82 series: lesion dose 4500 cGy/25 fractions/35 days. (In some cases isodoses of 4 and 15MV were combined.)
planned individually, using the smallest target volume compatible with uniform irradiation of the lesion as detected by radiological imaging techniques. With immobilization in an individually-constructed plastic shell, X-ray simulation and full isodosimetry, a 3-field technique was employed to localize radiation to the pituitary and minimize dose to the optic pathways, brain-stem and temporal lobes (Fig. I ) .
In the period 1961-1982 inclusive, 332 patients were so treated and the long-term results have been reported in prolactinoma (Grossman et al., 1984), in acromegaly (Cic- carelli et al., 1989). and in Cushing's disease (Howlett et al., 1989). There has been no instance of optic chiasmal damage or brain necrosis. The series was reviewed after periods of observation of 7-27 years (median 1 1 years) post-irradiation. Using the modified Cahan criteria for ascertainment, four cases were recognized for consideration: one of glioma, one of malignant naso-ethmoidal tumour, and two of myeloge- nous leukaemia. In relation to the investigation of these four index cases, also considered below are two other cases of

Clinical Endocrinology (1991) 35 Radiation oncogenesis pituitary tumours 381
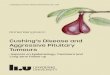
Flg. 2 Malignant astrocytoma, grade 4, 12 years after pituitary irradiation for acromegaly (case 2). a, Computerized tomographic section showing mass effect in right temporal lobe; b, isodose plan in horizontal plane, indicating dose range of 33754370 cGy at glioma site.
pituitary adenoma and glioma: one from a previous IMV era, and one contemporary with this series but in an unirradiated patient. No instance of fibrosarcoma or meningioma was encountered.
Case 1: Glioma (outside series)
A man of 34 presented in 1947 with symptoms of suprasellar extension of pituitary tumour and showed bitemporal hemianopia and optic disc pallor. The greater part of the tumour was removed but its close adhesion to the right optic nerve and to the anterior cerebral artery precluded further excision. Histology: chromophobe adenoma. In subsequent weeks there was excellent improvement in both visual acuity and fields. Post-operative X-ray therapy was given at IMV: lesion dose 4000 R/22 fractions126 days by a 4-field tech- nique.
Thereafter the patient remained well and required no hormone replacement. However, 28 years later (in 1975) he re-presented with a 6-weeks history of dysphasia, olfactory hallucinations and right hemiparesis, without headache or fits. A left temporal lobe tumour was demonstrated, and shown by needle biopsy to be a grade 3 astrocytoma.
Palliative X-irradiation was given without improvement, and the patient died 2 months after the diagnosis of the glioma.
At autopsy, poorly defined tumour was seen in the left amygdaloid nucleus and adjacent putamen. There was also another tumour, apparently unconnected, in the right post- frontal region, again poorly defined but about 2 x 2 cm in size. In the sella there was a small area of normal pituitary together with persisting chromophobe adenoma.
The positions of the gliomata of 1975 were located on the original isodose plan of 1947; that in the left temporal region arose in an area which had received 3600 cGy, and that in the right hemisphere at 3850 cGy.
Case 2: Gliorna
A woman of 47 presented in 1973 with a 5-years history of acromegaly and hypertension, and an intrasellar tumour. The diagnosis was confirmed by growth hormone estimation of 212 mU/l, unsuppressed after oral glucose. Megavoltage X-ray therapy to the pituitary tumour was administered in 1974: a lesion dose of 4500 cGy/24 fractions136 days by a 3-field technique (Fig. 1). From 1975 bromocriptine was

382 A. Jones Clinical Endocrinology (1991) 35
administered with great improvement, and 10 years later the mean growth hormone was 16 mU/1 whether on or off bromocriptine.
The patient remained well until 1986 when she had a grand ma1 attack without other neurological features. A CT scan revealed an area of low attenuation involving the right temporal lobe and extending into the parietal region; there was no mass effect, and the appearances were compatible with an infarct. But 3 months later the patient developed headache, followed by ataxia and depressed level of con- sciousness, and a further CT scan (Fig. 2a) now showed an obvious mass in the right temporal lobe, with contrast enhancement. At craniotomy tumour was encountered at a depth of 2 cm, and a standard temporal lobectomy was performed, but not clear of tumour. Histology revealed an astrocytoma grade 4. Post-operative X-ray therapy was given to the right hemisphere but, following a remission of 8 months, there was clinical and CT evidence of tumour recurrence. The patient died one year after histological diagnosis of the glioma.
Comparison of the CT scans with the original isodose of pituitary irradiation shows that the glioma arose in an area which had received between 3375 and 4370 cGy (Fig. 2b).
Case 3: Glioma (no irradiation)
A woman of 44 was investigated in 1962 for mild Cushing’s disease, the diagnosis being confirmed on the basis of loss of circadian rhythm of plasma cortisol and lack of suppres- sion on dexamethasone (2, 4 and 6 mg daily, each for 48 hours). No space-occupying lesion of pituitary or adrenal had been demonstrated radiologically, and in view of the mild symptoms she was managed satisfactorily by diet alone. Four years later, in 1966, while the diagnosis was again confirmed, a clinical impression of improvement was borne out by lower plasma cortisol readings and reversion of glucose tolerance to normal. Total adrenalectomy was not indicated, and although pituitary irradiation was considered (1966) it was not proceeded with because of the sponta- neously improving situation. Six years later, at the age of 56, symptoms of hypertension developed, and review in 1974 revealed no stigmata of Cushing’s disease, only the presence of hypertension. However, 2 years later she developed persistent headache and, over a week, slight hemiparesis. Technetium-99m brain scan showed an area of increased uptake deep in the left hemisphere, which increased over a period of 4 weeks to become no longer compatible with an infarct. Biopsy of this area revealed an astrocytoma grade 4. Intracranial pressure increased despite dexamethasone, the condition rapidly deteriorated, and the patient died in 1976, 9 weeks from the onset of her neurological symptoms.
Autopsy revealed a large deep necrotic grade 4 astrocy- toma extending through the corpus callosum from the left parieto-occipital region and thalamus. The adrenals were enlarged and nodular, with non-specific cortical hyperplasia. In the pituitary two lesions were present: massive necrosis of the pars nervosa; and a chromophobe microadenoma, immunostaining of which was positive with anti-prolactin and negative with anti-ACTH. There were no identified examples of Crooke’s hyalinization, and no histological evidence of active Cushing’s syndrome at the time of death.
Comment The gliomas in both irradiated cases occurred in the normal age distribution of glioblastoma and ran a characteristically rapid course. Applying Cahan’s criteria, both would be acceptable as instances of radiation-induced glioma (although the latency of 28 years in case 1 would now appear inordinately long for this histology (Table 3)); both arose in zones of sub-maximal dosage. But we also have case 3 in which a similar malignant astrocytoma supervened in the absence of irradiation, which had been considered but not proceeded with; and the interval of 10 years was similar to the latencies set out for the irradiated cases in Table 3. The incidence in the irradiated series was 1/332; but the un- irradiated patient was contemporaneous, and occurred in a series of 58 cases of Cushing’s disease not given radio- therapy. Although not amenable to direct statistical com- parison, it suggests that at this centre and in this period the risk of glioma induction associated with pituitary irradiation was not more than unity.
Case 4: Malignant neuroepithelial tumour of nasal passages: olfactory neuroblastoma
A man of 39 was investigated in 1974 for acromegaly, the symptoms of which had been present for 14 years. The unsuppressible level of growth hormone on dynamic testing was over 120 mU/I, and an intrasellar tumour was delineated radiographically. Megavoltage X-ray therapy was given to the pituitary by the technique of Fig. 1 (lesion dose 4500 cGy/ 25 fractions/35 days; lateral field sizes 4 x 4.3 cm). One year later bromocriptine was started and the GH fell to 8 mU/I; after 2 years the levels were undetectable, and the tests of anterior pituitary function were normal.
In 1980, 6 years after radiotherapy for the pituitary tumour, he presented with 3-months history of watering of the right eye and nasal discharge, and a week of right facial and orbital pain with diplopia. Clinically there was gross periorbital and maxillary swelling; all movements of the eye were painful and restricted; and the right airway was completely blocked by a firm mass extending down to the nostril. A palpably enlarged right submandibular node measured 4 x 2 cm; there was no evidence of remote

Clinical Endocrinology (1991) 35 Radiation oncogenesis pituitary turnours 3%3
metastasis. Radiography showed a large mass occupying the right ethmoid, maxillary antrum and nasal cavity, and further delineation, including CT, showed it to extend into the nasopharynx; there was destruction of both walls of the ethmoid and medial wall of the orbit, and abnormal tissue was present around the posterior part of the right optic nerve. Biopsy excision of the polypoid mass in the right nasal cavity was reported as showing small-cell anaplastic carci- noma. The therapeutic problem was formidable, for the rapidly growing and extensive neoplasm encroached poster- iorly on the volume previously irradiated for the pituitary tumour so as to preclude effective radiotherapy as the primary measure. Chemotherapy was instituted as initial treatment, using a regime of cyclophosphamide, vincristine, CCNU and methotrexate (with folinic acid rescue), and tumour response was rapid. But at 8 weeks (after two further courses) the patient became less well, and a new CT scan showed that the tumour had extended into both orbital cavities and upwards into the floor of the frontal fossa. The patient’s condition thereafter deteriorated rapidly, and he
died 3 months after presentation with the nasoethmoidal tumour.
At autopsy the large mass, which had eroded through the floor of the anterior fossa, had involved the antrum, sphenoid and frontal sinuses and extended across the midline. It also extended for 3.5 cm into both frontal lobes and backwards along penvascular spaces; and haemorrhages noted in midbrain and pons also contained microscopic tumour. There was no evidence of distant metastasis. In the pituitary a small amount of eosinophil adenoma remained.
The SND in this case had been regarded as an unusual rapidly growing small-cell carcinoma of the upper air passages, but when for this review the histological sections were re-examined in 1988, with immunochemical staining, the results accorded with those described in olfactory neuroblustomu. In these uncommon malignant turnours, which arise from the sensory mucosa of the roof of the nasal cavity, maxillary or ethmoidal sinus, the diagnosis is often difficult, for besides being usually poorly differentiated they exhibit a spectrum of appearances (Ng et al., 1988), espe-
Ag. 3 Olfactory neuroblastoma in acromegaly (case 4). Photomicrographs showing a, tumour composed of well defined trabeculae of darkly staining cells, between which are numerous blood-vessels. Haematoxylin & eosin. x 90. b, Higher power of turnour, showing small irregularly staining cells with atypical, irregular nuclei exhibiting many mitoses. The edges of the trabeculae are well defined. The intervening connective tissue contains numerous closely packed capillary blood vessels. Haematoxylin & eosin. x 225.

384 A. Jones Clinical Endocrinology (1991) 35
cially mimicking carcinoma. We therefore sought the advice of Professor L. Michaels (of the Institute of Laryngology and Otology, University of London), who commented on the well defined round tumour lobules of dark-staining cells, some with syncytial agglomeration of nuclei. While the component cells were more atypical than normally seen, and mitoses were numerous, the stromal blood vessel arrange- ment was similar to that seen in olfactory neuroblastoma (Fig. 3). Immunocytochemical investigations by the immu- noperoxidase method showed neurone specific enolase and protein gene product (PGP 9.5) to be strongly positive, indicating ‘neuroendocrine’ differentiation. Cytokeratin staining reactions (CAM 5.2 and LP 34) were negative.
Comment The SND in this case of acromegaly was thus a poorly differentiated neuroendocrine tumour, more active than the usual form of olfactory neuroblastoma but with the features of packaging of tumour cells and type of vascularity supporting this designation (Michaels, 1987). Its close juxtaposition to the previous target volume of irradiation required careful consideration, for a small part of the nasopharynx and sphenoidal sinus is inevitably included in the high-dose zone. Epithelial tumours of paranasal sinuses have not been recorded after modern X-ray therapy of pituitary tumour and, in the absence of genomic aberration (retinoblastoma), neuroblastoma is not known to be radia- tion-associated.
As olfactory neuroblastoma arises from the basal cells of olfactory epithelium a knowledge of its exact distribution is required for any application of Cahan’s criteria for radiation induction. The area of this specialized mucous membrane in the postero-superior part of the nasal cavity decreases greatly in early life (Naessen, 1970) so that in the adult it covers from the cribriform plate to the superior turbinates and upper 1 cm of the sides of the nasal septum (an area at most of 10 cm*). Examination of the radiotherapy plan and the simu- lator and port check films in this case showed the potential area to have been outside the radiation beams; and isodosi- metry showed the maximum radiation dose to the posterior limit of the cribriform plate to have been only 450-225 cGy. One other possibility, relating to the potential distribution of ‘cell nests’ of olfactory epithelium, required consideration. The primitive neuroepithelial cells develop from the olfac- tory placode (at the anterior end of the neural tube) and have been regarded as the origin of the unusual cases of olfactory neuroblastoma presenting as frontal or parasellar tumours (Ng et al., 1988). Such an origin would lie within the high- dose zone of pituitary irradiation. But in the present case, which presented with naso-ethmoidal symptoms, the tumour had spread sequentially into the cranial cavity, quite unlike the described intracranial cases.
At first sight this case could have been regarded as a radiation-induced carcinoma of upper air passages, but for reasons of histology and spatial dosimetry it seems unlikely that this unusual SND was radiation-associated.
Case 5: Chronic myelogenous Ieukaemia
In 1972 a man of 50 presented with gross acromegaly, present for at least 17 years, and with an unsuppressible growth hormone level of 164 mU/1. Pituitary X-irradiation was carried out by the technique of Fig. 1 (lesion dose 4500 cGy/ 25 fractions/34 days: lateral field size 4 x 4 cm). Two years later the growth hormone level was still raised at 27 mU/1, and bromocriptine was prescribed from September 1974. At follow-up 2 months later the patient complained of lassitude, but except for slight pallor clinical examination was unre- markable. However, the blood count, which had been normal in 1973, now showed: haemoglobin 15 g/dl, RBC 4 . 6 4 ~ 10t2/1, WBC 31 x 109/1, with differential count of promyelocytes 4%, myelocytes 6%, metamyelocytes 8%, neutrophils 57%, eosinophils 1 %, lymphocytes 14% and monocytes 10%; platelets 256 x 109/l. Sternal marrow exami- nation revealed the picture of chronic myelogenous leukae- mia, with a leucocyte alkaline phosphatase of 88, and positive Philadelphia chromosome. In the absence of specific symptoms the leukaemia was managed expectantly. The patient remained in reasonably good health for over a year, but in 1976 the total white cell count rose to36 x 109/1, and busulphan was administered. The pace of the disease increased; despite hydroxyurea and prednisolone his condi- tion continued to deteriorate, and he died in September 1977. The period of survival from diagnosis of chronic myeloge- nous leukaemia was 2.9 years.
Case 6: Acute myelogenous leukaemia
A woman of 67, investigated in 1977, had a 7 years’ history of acromegaly. She had had a transitional cell carcinoma of the bladder removed in 1968, and breast cysts excised on three occasions. In the family history, three brothers had had bowel carcinoma, and her mother died of ‘cancer of the spleen’. Clinically there was obvious acromegaly, and the patient was shown to have diabetes mellitus. The growth hormone level was 120 mU/I; the blood count was unremark- able. Treatment with bromocriptine reduced the GH level to 14 mU/I, and pituitary X-irradiation was carried out in October 1977 (lesion dose 4500 cGy/26 fractions/37 day& field sizes (Fig. 1) being 4 x 4 cm). Treatment was completed uneventfully, and the blood count remained unchanged.
Despite an aortic valve replacement for stenosis, and an

Clinical Endocrinology (1991) 35 Radiation oncogenesis pituitary tumours 385
excision of further recurrence of bladder carcinoma she continued in fair condition until 1987 when, at the age of 78, she presented with several weeks of dizziness, dyspnoea and chest pain. She was grossly anaemic and in mild cardiac failure. The blood count showed the haemoglobin to be 6.8 g/dl, WBC 4.0 x 10g/l, with 23% blast cells, I % promyelo- cytes, 4% myelocytes, 1 % metamyelocytes, 11 % neutrophils, 2% eosinophils, 54% lymphocytes and 4% monocytes; platelets 220 x lo9/]. The sternal marrow showed 70% blasts with a myeloid phenotype, the picture being that of acute myeloid leukaemia FAB M2; no Philadelphia chromosome was demonstrated. Chemotherapy was considered to be inappropriate, and the leukaemia was managed by blood transfusions and symptomatic measures. The patient died in 1988, 7 months after the diagnosis of acute leukaemia.
Comment With such a small target volume it is not surprising that leukaemia after pituitary X-irradiation does not figure in the clinical or epidemiological literature. The only men- tions have been by Lawrence et al. (1970) of one acromegalic patient treated by heavy ion therapy, and retreated elsewhere 3 years later, who died after a year with acute myeloblastic leukaemia; and by Wright et al. (1970) of two acromegalic patients who had been treated by large doses of radio-iodine for thyroid carcinoma. In the National Cancer Institute (SEER) analysis of the leukaemic risk associated with cancer treatment, Curtis et al. (1984) found no risk (RR=O) for brain and CNS tumours treated by irradiation alone. Boivin et al. (1986), in their study which extended over 1933-1972, found an RR of 0.9 for ‘non-trunk’ sites (which included all tumours of and above the larynx), and correlated this with the distribution of active marrow in adults. Risk factors generated in other studies relate to mean marrow dose, and the methodological problem of heterogeneous marrow irra- diation was highlighted in that of Boice er al. (1987), of a cohort of 150 OOO women with cervical carcinoma, which showed a twofold increase in leukaemia associated with an average marrow dose of 400 cGy. The pituitary situation and that in cervical carcinoma are very different. For in the former a very small target volume, remote from the bulk of haemopoietic tissue, is irradiated to a dose which would undoubtedly sterilize active marrow in siru, and with minimal extraneous irradiation; while in the latter the target volume is large, over major sites of haemopoiesis, with intracavitary gamma radiation contributing to total body dose. But in developing their concept, that the total leukaemogenic risk (as a linear-exponential function) equals the sum of in- cremental risks to individually-exposed masses of marrow, Boice et al. (1987) emphasized the need for accurate information on actual distribution in adults, at present ‘not well defined‘.
The proportion of active marrow within the skull assumed in modem studies for radiation protection has ranged from 7.6 to 13.1 %, the most recent (Lewis et al., 1988, accepted in UNSCEAR, 1988) being 11.9%. For the normal adult skull these values may be much too high, as radio-iron (ferritin) studies (Schneider t Montz, 1966; Alfrey ef al., 1969) had shown only minimal uptake over the skull (4.6% for head and neck together; 6.3% for head and arms). Magnetic resonance imaging (MRI) can now elucidate the gross distribution of active marrow (Richards et al., 1988; personal comunication 1988), and comparing MR images of healthy adults with the topography in the pituitary cases revealed that what had been regarded as red marrow in the basi- cranium gave fat signals only, as did the vault diploe. No haemopoietic tissue was identified in the paths of the beams. The question of isolated contribution of low-dose peripheral scatter can be approached only statistically. For high MV radiations, and small fields so positioned, such exposure is extremely small. Moreover, within 95% confidence limits, the observed leukaemia (two cases) is not significantly different from the spontaneous leukaemia mortality, and given the small size of the population (332 cases) any increase from scattered radiation would be indistinguishable from such normal variation.
Since they are not amenable to statistical analysis the significance of these two cases is uncertain, but the considera- tions of spatial dosimetry given provide no evidence for their having been radiogenic.
Review
As the characteristically long natural history of pituitary adenomata may provide unusual opportunities for the expression of other tumours we have first to consider possible modes of interaction with other, particularly intra- cranial, neoplastic processes.
Multiple primary intracranial tumours are in general uncommon; the infrequent concomitant or consecutive development of even the two most commonest, glioma and meningioma, is most probably based on chance (Moots & Rubinstein, 1984). But the incidence of meningioma depends on the mode of ascertainment; about a third as common as glioma in neurosurgical series, the increasing use of CT and MR imaging has revealed many silent tumours, sometimes small and multiple, while incidental meningiomas have been found in 2.3% of routine autopsies (Nakasu et al., 1987). Similar considerations apply with even greater force to pituitary tumours, for epidemiological data refer to an era before the widespread biochemical recognition of hyperpro- lactinaemia and, moreover, routine autopsy studies have

386 A. Jones Clinical Endocrinology (1991) 35
revealed an incidence of silent pituitary tumours in some 10- 20% of cases (Doniach, 1982). It is thus not possible to calculate in a meaningful way the possible chance association of pituitary adenoma with either meningioma or glioma at the present time.
The major neurophakomatoses are characteristically asso- ciated with an increased incidence of multiple tumours, and while there are several reports of acromegaly with neurofi- bromatosis, a chance association is likely. But a putative connection between biochemically active pituitary adeno- mata and the incidence of other tumours has to be examined, for it is possible that certain hormones might act as promoters or amplifiers of events set in motion through the interaction of an oncogene and radiation. Relatively minor manipulations of endocrine status have been shown to influence profoundly the incidence of certain tumours in mice. Patients with acromegaly are known to have a reduced life expectancy which has been thought to be due partly to an increased incidence of malignant disease (Alexander et al., 1980; Bengtsson et al., 1988). As long ago as 1957 Mustacchi and Shimkin had compared the incidence of cancer in 223 patients with acromegaly and gigantism with that in patients with hypopituitarism, and in the normal population, and there was no significant difference between the observed and ‘expected’ numbers. The mortality in acromegaly was stu- died in greater detail by Wright et al. (1970): the number of deaths was almost twice that expected in the general population, due mainly to cardiac and respiratory disease, but while malignant neoplasms occurred in 18% (with a variety of primary sites, and including three in irradiated patients) the total of deaths from malignant neoplasm was no more than expected. Despite the occasional case report, there is no support for a suggested increased pace of neoplasia associated with persistently high levels of growth hormone, and Clayton et al. (1987) have also shown that substitution GH therapy does not induce an increased relapse rate of medulloblastoma, astrocytoma or leukaemia.
There is thus no evidence that in cases of pituitary adenoma the spontaneous occurrence of other intracranial tumours, whether synchronous or sequential, is other than random, and while ‘uncommon’ it cannot be quantitated with any precision at the present time. Nevertheless, a proportion of patients (in acromegaly about 20%) will die of various types of malignant disease, and this is the back- ground against which evidence for radiation induction has to be considered.
Specific associations with irradiation: Over the last 30 years there have been some 40 papers from diverse parts of the world linking radiotherapy of pituitary tumours with sub- sequent induction of fibrosarcoma, meningioma and glioma. The vast majority have been individual case reports, without
any indication of underlying denominator, which with the small number of cases has prevented useful radiobiological analysis. While the collection of case reports is epidemiologi- cally a sterile pursuit (for as well as the absence of denominators there is a tendency to report both the unusual, and positive but not negative associations), when dealing with very rare conditions such an approach can give clinical insights not otherwise available; the patterns of reported cases may then be viewed in the light of more general knowledge of the radiation oncogenesis of the particular tumour species.
Sellar and parasellar fibrosarcoma
Post-irradiation sarcoma, although still clinically uncom- mon in general oncology, is appearing more frequently as the number of long-term survivors increases (Robinson et al., 1988), and the connective tissues in and around the sella are not immune from this stochastic process. Terry et al. (1959) described three cases of ‘combined non-metastasizing fibro- sarcoma and chromophobe adenoma of the pituitary’ fol- lowing repeated courses of X-irradiation for pituitary ade- noma, after intervals from 3 to 12 years. In the following three decades a total of 29 such cases has been reported in the world literature (Table I) , and a characteristic clinical and pathological picture has emerged. The tumours are usually rapidly growing, infiltrating the parasellar regions, usually into the cavernous sinuses, hypothalamus and brain-stem. Histologically they have been interpreted as pleomorphic spindle cell sarcomas with occasional variants. In one (Gonzales-Wale et al., 1976) it was a malignant fibrous histiocytoma; in another, the poorly differentiated spindle cell tumour contained osteoid (Amine & Sugar, 1976); while one presenting in the temporal lobe and Sylvian fissure contained cartilage and osteoid trabeculae (Pagb et al., 1986). In the whole series the latent period between the initial radiotherapy and clinical expression of SND ranged from 2 to 27 years; in two-thirds it lay between 7 and 15 years, with a median of 10 years. Characteristically the clinical course has been as short as 6-24 months, and the problems of treatment have proved intractable. Remarkably, in no instance has remote metastasis been documented, though this may be due to the short time course of the primary tumour.
The reported parameters of radiotherapy are set out in Table 1. Over the period of 40 years there were obvious differences in treatment policy, radiation energy and tech- nique which limit detailed correlations. In the initial cases (Terry et al., 1959) multiple courses of orthovoltage radia- tion had been given, the doses being documented as sum- mated field doses (air). With present knowledge of the latency and pace of this SND we can discern that in five cases

Clinical Endocrinology (1991) 35 Radiation oncogenesis pituitary tumours 387
Table 1 Post-irradiation sellar and parasellar fibrosarcoma (29 cases reported in 23 papers, 1959-86)
Author Case no.
Terry et al. (1959)
Goldberg el a/. (1963)
Wheelock (1963) Greenhouse (1964) Waltz and Brownell (1966)
Russell ( 1966) Chang and Pool ( I 967) Wright et al. (1970) Rubinstein (1972) Amine and Sugar ( I 976) Gonzales-Vitale et al. (1976) Powell et al. (1977) Ahmad and Fayos (1978) Gerlach and Janisch (1979) Coppeto and Roberts (1979) Kojima (1979) Shin et al. (1980) Vikhert and Kasunova (1980)
Martin et al. (1980) Pieterse et al. (1982) Nagatani et al. (I 984) Shi et al. (1984) Pages et al. (1 986)
I 2 3 3 4
1 2
I 2 3
No. of Pituitary Initial pituitary courses dose Latency
Age* adenoma of XRT Beam energy (summated) (years)?
47 44 26 29 31 38 24 38 42 ? ? ?
33 16 26 52 56 26 46 46 33 43 58 50 18 48 55 54 23
Chromophobe Chrornophobe Chromophobe Eosinophil Eosinophil Eosinophil Eosinophil Chromophobe Chromophobe Eosinophil Chromophobe Eosinophil
? Chromophobe Chromophobe Chromophobe Chromophobe Chromophobe (acromegaly) Eosinophil
? Chromophobe Eosinophil Chromophobe Eosinophil Chromophobe Chromophobe holactinoma Chromophobe Aden o rn a
4$ 2$ 4 2 3 ?
1 1 ?
M ? ? 1 1$ I I 2$ 1 I I 2 3 2 1 I 1 1 1
200 kV 250 kV 200 & 400 kV 200 & 1000 kV
1000 kV ?
HV 250 kV 250 kV
? 200 kV
? ?
Betatron ?
WCO W c o
Proton ?
? ? ? ? ?
8 MV ?
Lin. acc. WCO
?
4576 R 7375 R 6500 R 3940 R 6000 R
? 4000 R 3500 R 4000 R
? ? ? ?
5100 cGy 3600 cGy 5000 cGy 4292 cGy 6OOO cGy
10000 cGy 4092 cGy 5000 C G y
10 100 cGy 12000cGy
? 4500 CGy 4500 CGy 5000 CGy 5000 cGy 5400 C G y
7 3
12 10 20 12 7 8 5
15 27 15 17 10 I I 13 10 20 7 10 1 1 12 13 8 5
18 2 8
27
*Age at first radiotherapy. t Latency from first radiotherapy to clinical expression of SND. $Excluding ultimate course and dosage given for SND.
the ultimate course of irradiation had, in fact, been given for symptoms of the SND, and the relevant fractions have been subtracted. In only six of the 29 cases was the radiation stated as being of megavoltage energy; one was cyclotron protons; and in the other 22 cases ‘orthovoltage’ or ‘unknown’. In the orthovoltage cases the dose to sellar bone and periosteum would be augmented by a factor of 1.7, resulting in summated maximal tissue doses of 5950-12 500 cGy. With the advent of megavoltage radiation, and the avoidance of multiple courses, it was anticipated that the incidence of such SNDs would fall. Particular interest therefore attaches to the eight presumed megavoltage cases: three treated by radio- cobalt, two by linear accelerator, one by betatron, and two ‘unstated’, with doses ranging from 4000 to 5100 cGy in 21- 35 days. The clinical picture was similar to that described for
the whole series and the latent periods ranged from 2 to 13 years, again with a median of 10 years. These eight instances were reported as single cases over a period of 8 years, but with no indication of the size of the groups treated. For lower energies, Goldberg et al. (1 963) reported two cases occurring in 75 acromegalic patients irradiated between 1931 and 1961 ; and Waltz and Brownell (1966), two out of 65 irradiated between 1949 and 1958. But except for the one figure for proton irradiation, of one case in 734 (Kjellberg & Kliman, 1979), the later literature (other than to mention the extreme rarity) is silent. No instance has been encountered in our own series, and the problem of elucidating the true incidence of this random event at the modern dosage level of 4500 cGy is compounded both by the small numbers ever reported and by the complete absence of underlying denominators.

388 A. Jones Clinical Endocrinology (1991) 35
When we seek instances of spontaneous sellar fibrosar- coma for base-line comparison we find an interesting situation. Following the report of the original radiation- induced tumours it was often averred that intra-sellar sarcoma ‘had long been recognized’ in the absence of prior irradiation. But what had previously been regarded as ‘sarcomatous changes’ later came to be understood merely as variants of pituitary adenoma. Even in 1932, Atkinson, who had found 43 pituitary ‘sarcomas’ in a review of 248 autopsied cases of acromegaly, indicated that many would consider all such cases to be adenomata, a view again affirmed by Kraus in 1945. So greatly have the nomenclature and diagnostic criteria for pituitary tumour changed that inferences based on the distant past can no longer be regarded as valid. A study of the literature over the last half- century reveals no documented instance of non-irradiated sellar fibrosarcoma (the much-quoted case of Willis (1938), with metastases, could have been of naso-pharyngeal origin). On the tenet of radiation oncogenesis that, in general, radiation exposure only increases the incidence of an already prevalent tumour, UNSCEAR (1988, p. 409) concedes a measure of specificity for extremely rare tumours which are commoner after irradiation, and parasellar fibrosarcoma should be regarded as one of these few.
Radiation-induced sarcoma is a most serious complica- tion, and its perceived rarity requires a search for collateral evidence which might help quantitate the risk. Immediately, we strike the difficulty that the vast majority of radiation- associated intracranial (non-pituitary) sarcomas have been in children (Tiberin et al., 1984; Kingston et al., 1987), especially in association with brain tumour and leukaemia; and as discussed later, in these there may be a predisposition to SND. This and the paucity of adult cases (which number fewer than the parasellar fibrosarcomas) prevent any useful deduction. Of irradiation sarcoma in general, cases number- ing several hundreds have been collected over decades (e.g. Fietkau et af., 1988; Robinson et al., 1988) and it might be thought possible to extrapolate information from these groups, with appropriate scaling down of the probability of incidence for the small volume at risk: the concept of ‘oncogenic risk proportional to mass exposed‘ (Archer & Simpson, 1963; Mayneord & Clarke, 1975; Boice et al., 1987). But when examined in relation to prior irradiation for breast carcinoma (a common tumour with appropriate survival pattern), the very small numbers of evoked sarco- mas in a relevant dose range and with known denominators precluded quantitative extrapolation. Thus we are left with the interpretation of the actual reports detailed in Table 1.
Post-irradiation sellar fibrosarcoma is seen to be a rare condition, reported in the world literature only eight times after modern megavoltage X-ray therapy and with a median
latency of 10 years. It evidently occurs as a random process, with a risk too low to be exactly quantified at the present time. But the remote possibility of this major late complica- tion will continue to exist, whatever the technology of external irradiation, when this small mass of connective tissue in a neurologically eloquent area is exposed to effective dosage of this order. In general, the higher the dose the greater the probability of induction, and irradiation sarcoma at other sites has been described in adults with dosage of from 1800 cGy to over 10 000 cGy; but because of the small numbers, no exact dose-response has been established in man. The importance of adequate dosage in controlling the growth of pituitary adenoma is, however, well established (Sheline et at., 1961; Chang & Pool, 1967), and no evidence has been adduced which would justify dose reduction on the grounds of oncogenesis alone.
Meningioma
With meningioma we have a totally different situation, for this relatively common tumour occurs spontaneously with well defined characteristics, more cases are being uncovered by imaging, and general autopsy studies reveal meningioma as a significant incidental finding. Because of their frequency and long natural histories it is not surprising that pituitary adenoma and meningioma should occur together and, starting with Love and Blackburn (1955), I8 instances of such sporadic coincidence have been recorded (Table 2a). In 13, the association was concomitant; in two, meningioma appeared 4 and 9 years after the pituitary disorder; and in one, the Cushing’s disease became evident 6 months after excision of a suprasellar meningioma. (In a further two cases (Pak & Uzmanova, 1965; Hainer et al., 1978) the pituitary was ultimately irradiated and a meningioma was found in each at autopsy, but only one year later. In the light of recent information on latency these cannot be accepted as ‘radia- tion-induced’ and must be considered with the 16 other cases of ‘spontaneous’ meningioma.) Two-thirds of the meningio- mas in this unirradiated group were in the general vicinity of the sella.
Nevertheless, radiation-associated meningioma has been well documented (Table 2b) in 12 cases over a period of 20 years. Lawrence et al. (1970), reporting on heavy ion therapy in acromegaly, mentioned one case of meningioma occurring after 1 1 years, but felt that as that area of brain was estimated to have received only 300 cGy a causal relationship was unlikely. Of the other 11 cases, meningioma appeared in nine after latencies of 8-22 years, and in two after 30 and 32 years (median 19 years). The average age at presentation with the SND was 43 years, compared with 53 for the spontaneous cases. The total radiation dose was often high, and only three

Clinical Endocrinology (1991) 35 Radiation oncogenesis pituitary tumours 389
A. Meningioma and pituitary adenoma in patients without relevant hdintioo
Author Initial pituitary Site of
Sex Age adenoma meningioma Time sequence
Love and Blackburn (1955) F 65 Ziilch ( 1956) F 55
OConnell(l961) F 47 Kitamura et al. (1965) F 66 Pak and Uzmanova (1965) F 69
Probst (1971) F 48
von Wild and Ruf (1973) F 42 Brennan et al. (1977) M 36 Bunick er al. (1978) M 57 Hainer et al. (1978) M 72
Andrioli et al. (1981) F 61 Hyodo et al. (1982) F 52 Irsy et al. (1985) F 59
Ohata (1985) F 50 Yamada et al. (1986) F 52 Zentner and Gilbach (1989) (1) M 46
(2) F 63 (3) F 61
Chromophobe Chromophobe
Chromophobe Chromophobe Eosinophil
Chromophobe with Cushing’s disease
Adenoma Chromophobe Eosinophil Eosinophil
Prolactinoma Eosinophil Mixed cell
Chromophobe (acromegaly) Chromophobe Prolactinoma Hormone inactive Hormone inactive
Sylvian fissure Frontal
Suprasellar (tuberculum) Sphenoidal ridge Frontal convexity
Suprasellar (tuberculum)
Suprasellar Sphenoidal ridge Subfrontal Suprasellar
NS Parietal Centroparietal
Falcotentorial Parasellar Planum sphenoidale Sphenoid wing Sellar
Synchronous (S) PM finding of meningioma
4 years after diagnosis of pituitary adenoma
S S
6 months after pituitary XRT
after meningioma
PM finding of meningioma
Cushing’s Disease 6 months
S S S
PM finding of meningioma 1 year after wCo for pituitary adenoma of 20 years duration
S S
Acromegaly for 9 years before simultaneous diagnosis of adenoma and meningioma
S S S S S
8. Meningioma and pituitary adenoma in irrndiated patients (12 cases) Age Initial pituitary Site of Radiation dose Latency
Author Sex at XRT adenoma meningioma (summated total) (years)
Lawrence et al. (1970) M ? Acromegaly NS
Bogdanowicz and Sachs (1974) Stock el al. (1 975)
Meyrignac et al. (1981) Spallone (1982) (1)
Yang (1982) Kolodny and Dluhy (1985)
(2)
Kasantikul er al. (1988) Sridhar and Ramamurthi (1989) Partington and Davis (1990) Parent (1990)
F 15 M 15
F 34 F 29 F 23 F 27 M 23
M 26 F ? M 26 F 35
Acromegalic gigantism Acromegalic gigantism
(eosinophil) Acromegaly (chromophobe) Chromophobe Acromegaly (eosinophil) Adenoma Prolactinoma
Prolactinoma Aden o m a Adenoma (Cushing) Acromegaly
Cerebellopontine angle Parasellar
Basicranial Suprasellar Olfactory groove Sphenoidal ridge Parasellar
Intrasellar Sellar Suprasellar Clivus (lower)
Heavy particle (900 MV He) 300 cGy to area of meningioma
7000 CGy
5300 cGy 6600 R 6200 R
12 374 cGy 4OOO cGy
(+penultimate 2700 cGy) 4700 cGy
4480 cGy
6114 R
?
?
16 21
20 22 13 22
18 8
32 9
30
had received doses in the current range; all the listed cases satisfied Cahan’s topographical criteria. On incidence, most reports give no indication of the ‘denominator’, excepting those of Lawrence er ul. (1970) (1/145 after helium ion therapy) and Spallone (1982) (l/l98). No instance has been
encountered in our own series of 332 patients irradiated between 1961 and 1982; but one case, with a tuberculum sellae meningioma, has been reported from this centre (OConnell, 1961) in an unirrudiuted patient.
The evidence for radiation-induced meningioma in general

390 A. Jones Clinical Endocrinology (1991) 35
comes mainly from studies following two quite different types of exposure in childhood. In the low-dose range were the cases following X-ray epilation of the scalp for tinea capitis (when the brain surface received a dose of about 140 cGy). In an extensive study of the Israeli group of over 10 000 irradiated patients with matched controls, Ron et al. (1988) found 19 meningiomas, a relative risk of 9-5 and an excess risk of 5.9 per 10000 person-years. As a group, such tumours, appearing after latent periods of 15-58 years, differed biologically from the usual in age and sex incidence, location, multiplicity and more aggressive behaviour (Soffer et al., 1983; Rubinstein et al., 1984). At the much higher doses employed in tumour treatment (the ‘tumour-rad- meningioma sequence’) meningioma has been reported 40 times in the last 20 years, with latencies of 5 to 40 years. Within the large cohort of 1OOOO cases of 3-year survivors of childhood cancer treated between 1940 and 1979, Hawkins et al. (1987, M. M. Hawkins, personal communication, 1989) found four meningiomas among 1107 survivors of a child- hood CNS tumour treated by irradiation-even in this age- group an uncommon sequel. Evidence has been adduced (Spallone et al., 1979; Iacono et al., 1981; Soffer et al., 1989) that a shorter latent period separates meningiomas following such high-dose treatment (median 19 years) from those after small (epilation) dosage (median c.38 years); and both age and dosage can influence latency, and in the same inverse direction (Mayneord, 1978; BEIR 111 1980).
A general ‘host susceptibility factor’ for radiation carcino- genesis in man is the age a t exposure, higher risk being associated with younger ages (BEIR 111, 1980; UNSCEAR, 1988; Rotblat, 1988); and this is borne out in animal studies, particularly for CNS tumours (Knowles, 1982; Morin et al., 1989). Moreover, in the paediatric tumour group the nature of the first neoplastic disease often necessitated wide or whole-brain irradiation, in contrast to the small tissue volume (and meningeal area) irradiated for pituitary tumours by megavoltage techniques. Thus the possible incidence of late meningioma following pituitary irradiation cannot be estimated from the paediatric experience, mainly because of early age susceptibility (and in some cases genetic proclivity) but also because of very different factors of spatial dosimetry.
The question of meningioma has been considered in some detail for two reasons. In general statements on radiation carcinogenesis much of the evidence for induction of neuro- genic tumours comes from the epidemiological studies in childhood, and risk factors so generated cannot be extra- polated to the pituitary situation in adults. Further, in the neurosurgical literature there has been considerable specula- tion, and the remote risk of meningioma has been cited (Spallone, 1982; Parent, 1990) as a reason for limiting
pituitary irradiation to cases having incomplete surgical removal or persistent and unresponsive hormonal hyper- secretion. But in fact, compared with the 18 reported cases of spontaneous association of meningioma with pituitary adenoma, only three cases have been reported after modem radiation techniques and, for the reasons discussed, it is unlikely to become other than a rare event in subsequent decades.
Glioma
Evidence for radiation induction of glial tumours has again come mainly from paediatric oncology, and very few cases have been described in adults. Whereas the initial report (Jones, 1960)-of anaplastic astrocytoma 10 years after megavoltage irradiation of a meningioma-referred to an adult, in the subsequent three decades only three similar examples of ‘meningioma-rad-astrocytoma’ have been recorded (Robinson, 1978; Zuccarello, 1986; Gelabert Gon- zalez et al., 1988), with evocative doses of 2750-5600 cGy and latencies of 10-21 years. Individual cases have been observed after adult irradiation for glomus jugulare tumour (Preissig et al., 1979), for brain metastasis of placental choriocarcinoma (Barnes et al., 1982), and as the third malignant tumour in cranial fibrosarcoma (Dierrsen et al., 1988).
At the same time a number of cases have followed childhood irradiation for glioma, for medulloblastoma, and particularly for acute leukaemia. As to their incidence, the Late Effects Study Group had internationally over 300 children with second malignant neoplasms (Packer et al., 1987), and of 35 with their initial tumour in the CNS in only five was the second also in the brain. Again, Hawkins et al. (1987). reporting in the UK on 2341 3-year survivors of childhood CNS tumours, found that while 17 SNDs had occurred in various organs, none of these was a glioma. However, for acute lymphoblastic leukaemia (ALL) in childhood (where cure rates have dramatically improved since the introduction of effective prophylactic treatment of the CNS with cranial irradiation and methotrexate), the last decade has also seen increasing numbers of glioma arising 3- 10 years after treatment (Rimm et al., 1987; Fontana et al., 1987). The Children’s Cancer Study Group in the USA accrued 880 cases of ALL in 1975-77, of whom 468 became long-term survivors; and among these, 10 developed astrocy- toma after 16-54 months, an RR factor of 227 (Miller et ai., 1986). Yet the role of irradiation in the aetiology is uncertain, for unirradiated patients have also developed glioma. A genetic predisposition to multiple neoplasms, and a synergic action of irradiation with methotrexate, have been suggested as risk factors. Although the recent concern and perceived

Clinical Endocrinology (1991) 35 Radiation oncogenesis pituitary tumours 391
possible risk stems from paediatric experience, again the evidence cannot be extrapolated: not only for the reasons discussed for meningioma, but also because, in the ‘ALL
cranial-irradiation’ situation in which most cases have occurred, factors additional to irradiation are believed to play an important part.
TaMo 3 Association of sellar and parasellar tumours with glioma
A. Following X-irradiatim
Author no. Sex a tXRT Initial tumour dose (cGy) (years) Glioma site and type Case Age Radiation Latency
____ ~
Pituitary Piatt ef af. (1983) I M
2 M 2 F 2 F
39 25 39 52
Acromegaly Chromophobe adenoma Chromophobe adenoma Acromegaly
4900 4500 So00 4500
13 10 5 8
Temporal: glioblastoma Thalamic: glioblastoma Temporal: glioblastoma Frontal:
astrocytoma gr. 3 Temporal & parasellar:
oligodendroglioma Post-fronto-basal: astrocytoma gr. 3 4 Optic chiasm:
astrocytoma (anaplastic) Basal ganglia:
glio biastoma Fronto-temporal:
glio blastoma Temporal:
anaplastic astrocytoma Temporal:
malign. astrocytoma Temporo-parietal:
glioblastoma multif. Temporal:
astrocytoma gr. 3 Temporal:
astrocytoma gr. 4
Okamato et al. (1985) Marus ef al. (1986)
Huang ef al. (1987)
Dierssen er a/. (1 988)
M
3 M
26
28
Acromegaly
Eosinophil adenoma
6600
6Ooo
12
6
Hufnagel ef al. (1988)
Flickinger el al. (1989)
M
M
29
55
Prolactinoma 5500
4750
12
Non-function adenoma 7.5
Shapiro ef al. (1989)
Zampieri el al. (1989)
Suda ef al. (1989)
I M 27 Chromophobe adenoma
Acromegaly (eosinophil and chromophobe) Eosinophil adenoma
Chromophobe adenoma
4500 + SO00
SO00
22
9 2 F 45
1 F 38 5
1 M 5500 Salvati era/. (1990) 52 6
Jones (1991) I M 34 Chromophobe adenoma 4Ooo 28
2 F 48 Acromegaly 4500 12
Parasellar Komaki er al. (1 977) Sogg et al. (1988)
2 M F
22 9
Craniopharyngioma Craniopharyngioma
5400 6OoO
6 5
Temporal: glioblastoma Temporal:
astrocytoma (malignant) Temporo-parietal:
glioblastoma Cerebellar vermis:
astrocytoma gr. 3 Fron to-parietal:
glioblastoma Basal ganglia and
brain-stem: glioblastoma Frontal:
astrocytoma gr.3 Temporo-parietal:
astrocytoma (anaplastic) Frontal:
astrocytoma gr. 4 Cerebellar:
astrocytoma gr. 3
Gutjahr and Dietrich (1979) F
M
4.5 Craniopharyngioma 6Ooo 7-5
Maat-Schieman ef al. (1985) 5 Craniopharyngioma
Craniophary ngioma
6Ooo 14
5900 Liwnicz ef al. (1985) 1 M 11 25
Ushio ef al. (1987) F 2 Craniopharyngioma
Craniopharyngioma
5460 5
Kitanaka et al. (1989) 2 F 8 16
1 M 13 Pineal germinoma 5400 7
Robinson (1978)
Tamura ef al. (1 989)
M 10 Pineal teratoma 4Ooo 26
M 31 Suprasellar germinoma
4250 8

392 A. Jones Clinical Endocrinology (1991) 35
Table 3 (continued)
B. Without irradiation
Author no. Sex Age* Initial tumour Time sequence Glioma site and type Case
Carson and Hellwig (1933) Kirschbaum (1945)
List et al. (1952)
Wise et al. (1953)
Gartner (19%) McPhedran and Tom (1962)
Gori and Nucci (1965)
Shuangshoti (1986)
Ezura er al. (1 988)
Jones (1991)
M F
M
It M 2 M
F F
F
M
M
3 F
5.5 37
52
56 52
57 78
43
15
33
55
Craniopharyngioma Obesity syndrome:
intrasellar meningioma
Chromophobe adenoma
Chromophobe adenoma Chromophobe adenoma
Pituitary adenoma Chromophobe adenoma
Eosinophil adenoma
Germinoma (3rd ventricle)
Chromophobe adenoma
Cushing’s d. and chromophobe microadenoma
Synchronous (S) 18 years of endocrinopathy;
gliomas and pituitary meningioma at PM
S
S S
S S
S
S
S
Glioma 14 years after diagnosis of Cushing’s d.
Temporal: astrocytoma Multiple cerebral
glio blastomas
h u l a and basal ganglia:
Frontal: oligodendroglioma Frontal and post-central:
oligodendroglioma Temporal: glioblastoma Basal ganglia:
astrocytoma (well diff.) Frontal:
undiff. ependymoma Hypothalamic:
astrocytoma and oligodend. Temporal:
astrocytoma (anaplastic) Parieto-thalamic:
glioblastoma
glioblastoma
‘Age at diagnosis of glioma. t X-ray therapy given only 4 months before operation (for large suprasellar pituitary tumour, and at which frontal oligodendroglioma found).
Glioma following irradiation of pituitary tumour has nevertheless been described in 14 instances since 1983 (Table 3a), and after latencies of 5-28 years (median 10 years); and only five of these 14 had received dosage in excess of 5000 cGy. All the gliomata were anaplastic, and half arose in the temporal lobes. The male/female ratio, and the age at presentation (34-62, median 49 years), were unremarkable. However, now assembled (Table 3b) are nine cases of glioma associated with pituitary tumour in the absence of irradiation. Of the new cases here described, in the present series of 332 irradiated patients there was one (Case no. 2) who developed temporal lobe glioblastoma 12 years after irradiation for acromegaly; but there was also a concurrent case (no. 3) of glioblastoma who had been under observation for Cushing’s disease for 14 years with no radiotherapy.
Because of their topography, cases in the literature reported after parasellar tumour irradiation have been similarly considered, and there have been seven instances of glioma following irradiation for craniopharyngioma and three for pineal tumour (Table 3a). Apart from two aged 22 and 31, all the others were children (mean age 7 years); and the radiation doses for craniopharyngioma varied from 5400
to 6000 cGy. Thus gliomata have been recorded in numbers of the same order after the irradiation of the rare cranio- pharyngioma and pineal teratoma as after that of the common pituitary tumour. Apart from the pituitary doses and field sizes being smaller, the two groups differed in that almost all the other cases were in children. Craniopharyngioma usually produces gliosis in adjacent brain, and while this may be a risk factor for radiation-induced tumour (Sogg et al., 1978; Ushio et ul., 1987) a number of the gliomata were not in continuity with the cyst. More importantly, craniopharyn- gioma and pineal teratoma are developmental lesions with a propensity for associated tumours. This, combined with the greater proclivity for radiation oncogenesis in childhood, and the small numbers, precludes meaningful application of data from an ostensibly similar anatomical situation.
From the variety of evidence adduced, radiation-induced glioma is seen as an established entity which may rarely follow radiotherapy, mainly in childhood, and which is extremely rare in adults. In the pituitary situation, while the potential for oncogenesis on a random basis exists, the additional risk must be very small, and none has been demonstrated in the case review from this centre.

Clinical Endocrinology (1991) 35 Radiation oncogenesis pituitary tumours 393
Dlscuralon
The investigation of radiation-induced tumours in the clinical dose range requires ideally a combination of statisti- cal assessment and evaluation by Cahan’s topographical criteria. An extensive review has shown that in 30 years, world-wide and irrespective of the spontaneous incidence, 58 cases of SND have been reported in association with pituitary irradiation of any energy; but in very few has there been any indication of the denominator group. The reported cases comprised 29 sellar fibrosarcoma, 12 meningioma and 14 glioma; together with three osteosarcoma (of the vault, from orthovoltage irradiation). Of this total, only 20 had been irradiated by modern techniques of energy and dosage. Risk projection from radiation requires a knowledge of many factors (UNSCEAR, 1988). But the paucity of cases and the dearth of information on groups at risk precludes an analysis of dose-response which could provide any extrapo- lative risk estimate, and constrains us to depend on other types of information. Ascertainment is, of course, of primary importance and requires appropriate pathological and physical data, including full isodosimetry.
At this centre, in the series of 332 cases of pituitary adenoma irradiated by a uniform megavoltage technique over 21 years and reviewed after periods of up to 27 years, we have observed no case of parasellar fibrosarcoma. There has been one of glioma (but also one in a parallel unirradiated patient). No instance of meningioma has been seen after pituitary irradiation (although one meningioma synchro- nous with pituitary adenoma has occurred in an unirradiated patient). The median period of observation of 11 years matched the median latencies of both fibrosarcoma and glioma, but did not extend to that of meningioma (19 years). Three other irradiated cases were identified for considera- tion: one of nasoethmoidal neuroblastoma, and two of myelogenous leukaemia, and these were reviewed in detail; but for the reasons given under Comment (Cases no. 4 and nos 5, 6) these were considered unlikely to have been radiation-induced.
Any review based on collected case-reports without de- nominators may be no more than an extended exercise in verisimilitude for, inevitably, published reports are weighted towards describing the unusual, and an association may be one of ascertainment rather than causation. Even an equally energetic search among the ranks of the unirradiated can provide no more than clinical insights. Nevertheless, 18 instances of meningioma were so identified in unirradiated patients, 12 of which would have satisfied ‘Cahan geometry’ compared with 12 for the radiation-associated condition; and while 14 cases of glioma were identified after pituitary irradiation, there were nine without. A graphic illustration of
spontaneous association is also provided by Mindel and Fete11 (1985) in a man who had a trans-sphenoidal resection of a prolactinoma. Serum prolactin levels remained elevated but the patient refused radiotherapy. Two years later a CT scan, performed because of neuro-ophthalmological signs, revealed a pineal mass which proved to be a spindle-cell sarcoma: had the patient been irradiated post-operatively few would have doubted the association. This is analogous to our case of Cushing’s syndrome, formally considered for radiotherapy but not irradiated and who developed a glioma after 10 years, at about the median latency of radiation- induced gliomata.
There is no evidence that irradiation transforms a pre- existing pituitary adenoma. Primary carcinoma (diagnosed on the basis of remote metastasis rather than polymorphism and invasion) is rare, and less than half the 38 published cases had received irradiation (Mountcastle et al., 1989). The risk of radiation-induction lies in the surrounding tissues, and has been established for fibrosarcoma, and to a lesser extent for meningioma and glioma. Despite the lapse of sufficient time for latency, with modern techniques of megavoltage irradiation only eight cases of fibrosarcoma have been reported world-wide in 8 years. Oncogenesis is however a random process and, despite the small irradiated volume, such cases will probably continue to occur, albeit as rare events. Of the 12 radiation-associated meningiomas docu- mented over 20 years, only three followed modern megavol- tage dosage, against the 12 spontaneous analogous cases. While radiation-induced glioma is also an established entity and 14 cases are documented, in the clinical report from this centre no increased risk has been demonstrated. Radiation- induced tumours following modern treatment of pituitary adenoma are thus seen to be rare random events, and ‘rare’ cannot be further semantically qualified.
It is however the perceived risk which dominates the making of clinical decisions, and this incorporates not only the probability of the adverse effect but also the conse- quences of its occurrence, for perceived risk changes when multiplying a very small risk with a very large consequence, and the radiogenic tumours discussed are certainly in this category. A third factor is the latency in relation to the natural history. An event is heuristically conceived as probable to the extent that instances are easily recalled or imagined. Second CNS tumours are such as to make a lasting impression, and the perspective of their ascertainment is therefore particularly relevant. Neurological surgery and histopathology are the only two disciplines with immediate experience of the whole spectrum of radiogenic intracranial tumours and their role in ascertainment is fundamental: to them is due our first appreciation of the considerably increased prevalence of such tumours over the last two

394 A.Jones Clinical Endocrinology (1991) 35
decades. This spectrum is however not a continuum and, for the reasons set out here, the experience of such tumours from childhood irradiation (whether for epilation or tumour) cannot be applied to risk estimation in the adult pituitary situation, particularly as the 'perception of risk' may ema- nate from diagnosis at tertiary referral centres irrespective of the original population at risk.
Pituitary irradiation remains a valuable part of the armamentarium against both functioning and non-function- ing tumours. Treatment decisions depend on the natural history, particularly whether related to overt tumour or early biochemical diagnosis, and on the efficacy and possible adverse effects of each available therapeutic modality as it develops. What is perceived as a very low risk of radiation- induced tumour has to be balanced against the well docu- mented benefits in the particular circumstances of the individual patient.
Acknowledgements
It is a pleasure to express my thanks to colleagues for their interest and cooperation, and particularly to Professors I. Doniach, G. M. Besser and J. A. H. Wass. I am most grateful also to Professor L. Michaels, who reviewed the sections and provided the photomicrographs of case 4; to Dr M. A. Richards for his advice on MR imaging of bone marrow; to Dr J. E. Kingston and Mr M. M. Hawkins for paediatric data; to Dr W. M. Gregory and Dr B. Lambert for statistical help; and to Mr D. Doughty for the radiation dosimetry.
References
Ahmad, K. & Fayos, J.V. (1978) Pituitary fibrosarcoma secondary to radiation therapy. Cancer, 42, 107-1 10.
Alexander, L., Appleton, D., Hall, R., Ross, W.M. & Wilkinson, R. (1980) Epidemiology of acromegaly in the Newcastle region. Clinical Endocrinology, 12.71 -79.
Alfrey, C.P., Lynch, E.C. & Hettig, R.A. (1969) Studies of iron kinetics using a linear scanner. Journalof Laboratory and Clinical Medicine, 73,4054 17.
Amine, A.R.C. & Sugar, 0. (1976) Suprasellar osteogenic sarcoma following radiation for pituitary adenoma. Journal of Neurosur- gery, 44, 88-91.
Andriolo, G.C., Zuccarello, M., Scanarini, M. & DAvella, D. (1 98 1) Concurrent primary intracranial tumours of different histogenesis. Acta Neuropathologica (Berlin) (Suppl. 7), 1 11-1 15.
Archer, V.E. & Simpson, C.L. (1963) Semi-quantitative relationship of radiation and neoplasia in man. Health Physics, 9,4556.
Atkinson, F.R.B. (1932) Acromegaly, p. 21. Bale, London. ~Barnes, A.F., Liwnicz, B.H., Schellhas, H.F., Altshuler, G., Aron,
B.S. & Lippert, W.A. (1982) Successful treatment of placental choriocarcinoma metastatic to brain followed by primary brain glioblastoma. Gynaecologic Oncology, 13, 108- 1 14.
BEIR 111 (1980) Committee on Biological Effects of Ionising
Radiation. The efects on populations of exposure to low levels of ionising radiation. US National Academy of Sciences, National Research Council. National Academic Press, Washington.
Bengtsson, B.-A., Eden, S., Ernest. I.,Oden, A. &Sjogren, B. (1988) Epidemiology and long-term survival in acromegaly. Acta Medica Scandinavica, 223,327-335.
Bogdanowicz, W.M. & Sachs, E. (1974) The possible role of radiation in oncogenesis of meningioma. Surgical Neurology, 2,
Boice, J.D., Blettner, M. & Kleinerman, R.A. (1987) Radiation dose & leukaemia risk in patients treated for cancer of the cervix. Journal of the Nationaf Cancer Institute, 79, 1295-13 1 1.
Boivin, J.-F., Hutchison, G.B. & Evans, F.B. (1986) Leukaemia after radiotherapy for first primary cancers of various anatomical sites. American Journal of Epidemiology, 123,993-1003.
Brennan, T.G., Krishna Rao, C.V.G., Robinson, W. & Itani, A. (1977) Tandem lesions: chromophobe adenoma and meningioma in the same patient. Journal of Computer Assisted Tomography, 1, 517.
Bunick, E.M., Mill, L.C. & Rose, L.I. (1978) Association of acromegaly and meningiomas. Journal of the American Medical Association, 240, 1267-1268.
Cahan, W.G., Woodward, H.Q.,Higinbotham, N.L., Stewart, F.W. & Coley, L. (1948) Sarcoma arising in irradiated bone. Cancer, 28,
Carson, P.C. & Hellwig, C.A. (1933) Multiple intracranial tumours in children: suprasellar adamantinoma associated with cerebral glioma. American Journal of Diseases of Childhood, 46, 1 19-131.
Chang, C.H. & Pool, J.L. (1967) The radiotherapy of pituitary chromophobe adenoma. Radiology, 89, 1005-1016.
Ciccarelli, E., Corsello, S.M., Plowman, P.N., Jones, A.E., Towel, R., Rees, L.H., Besser, G.M. & Wass, J.A.H. (1989) Long-term effects of radiotherapy for acromegaly on circulating prolactin. Acta Endocrinologica (Copenh.), 121, 827-832.
Clayton,P.E.,Price, D.A.,Shalet,S.M. &Gattemaneni, H.R. (1987) Does growth hormone cause relapse of brain tumours? Lancet, i,
Coppeto, J.R. & Roberts, M. (1979) Fibrosarcoma after proton- beam pituitary ablation. Archives of Neurology, 36, 380-381.
Curtis, R.E., Hankey. B.F., Myers, M.H. &Young, J.L. (1984) Risk of leukaemia associated with first course of cancer treatment. Journal of the National Cancer Institute, 72, 53 1-544.
Dierrsen, G., Alvarez, G. & Figols, J. (1988) Anaplastic astrocyto- mas associated with previous radiotherapy. Neurosurgery, 22,
Doniach, I. (1982) The pathology of adenomas of the pituitary gland. In Current Concepts in Endocrinology (ed. By E. D. Williams) p. 22, Praeger.
Ezura, M., Kayama, T., Sakurai, Y., Ogawa, A. & Wada, T. (1988) A case of anaplastic astrocytoma associated with pituitary adenoma. No Shinkei Geka (Neurological Surgery. Tokyo), 16, 73-77.
Fietkau, R., Diepgen, T.L., Stehr, L. & Sauer, R. (1988) Zur Malignominduktion durch Strahlentherapie: eine retrospektive Untersuchung von 454 Tumoren. Strahlentherapie und Onkologie,
Flickinger, J.C., Nelson, P.B., Martinez, A.J., Deutsch, M. & Taylor, F. (1989) Radiotherapy of non-functional adenomas of the pituitary gland. Cancer, 63,2409-2414.
Fontana, M., Stanton, C.. Pompili, A., Amadori, S., Mandelli, F.,
379-383.
1087-1099.
71 1-713.
1095-1097.
1649247-259.

Clinical Endocrinology (1991) 35 Radiation oncogenesis pituitary fumours 395
Meloni, G., Riccio, A. & Rubinstein, L.J. (1987) Late multifocal gliomas in adolescents previously treated for acute lymphoblastic leukaemia. Cancer, 60, 1510-1518.
Gartner, J. (1955) Statistiche Untersuchungen an 654 intrakranial- len raumfordernden Prozessen. Zentralblatt fur Neurochirurgie,
Gelabert Gonzales, M., Bollar Zabala, A., Martinez Rumbo, R., Garcia A h , A. & Reyes Oliveros, F. (1988) Cerebral astrocy- toma secondary to radiation of a meningioma. Neurologia (Barcelona), 3, 68-70.
Gerlach, H. & Janisch. W. (1979) lntrakranielles Sarkom nach Bestrahlung eines Hypophysenadenoms. Zentralblatt fur Neuro- chirurgie, 40, 13 I - 136.
Goldberg, M.B., Sheline, G.E. & Malamud, N. (1963) Malignant intracranial neoplasms following radiotherapy for acromegaly. Radiology, 80,465470.
Gonzalez-Vitale, J.C., Slavin, R.E. & McQueen, J.D. (1976) Radia- tion-induced intracranial malignant fibrous histiocytoma. Cancer,
Gori, G. & Nucci, U. (1965) Frontal ependymoma associated with pituitary adenoma. Minerva Neurochirurgica (Turin), 9,211-213.
Greenhouse, A.H. (1964) Pituitary sarcoma; a possible consequence of radiation. Journal of the American Medical Association, 190,
Grossman, A., Cohen, B.L., Charlesworth, M., Plowman, P.N., Rees, L.H., Wass, J.A.H., Jones, A.E. & Besser, G.M. (1984) Treatment of prolactinomas with megavoltage radiotherapy. British Medical Journal, 288, 1 105-1 109.
Gutjahr, P. & Dietrich, E. (1979) Risko zweiter maligner Neoplasien nach erfolgreicher Tumorbehandlung im Kindesalter. Deutsche medizinische Wochenschrifr, 104,969-972.
Hainer, V., Krejcik, L., Pelikan, J., Tvaroh, F. & Urbanek, J. (1978) Meningioma in contact with eosinophilic adenoma in a patient with acromegaly. C?asopis Iikaiu Feskych (Prague), 117, E . 27,
Hawkins, M.M., Draper, G.J. & Kingston, J.E. (1987) Incidence of second primary tumours among childhood cancer survivors. British Journal of Cancer, 56,339-347.
Howlett, T.A., Plowman, P.N., Wass, J.A.H., Rees, L.H., Jones, A.E. & Besser, G.M. (1989) Megavoltage pituitary irradiation in the management of Cushing’s disease and Nelson’s syndrome: long-term follow-up. Clinical Endocrinology, 31,309-323.
Huang, C.-I., Chiou, W.-H. & Ho, D.M. (1987) Oligodendroglioma occurring after radiation therapy for pituitary adenoma. Journal of Neurology, Neurosurgery and Psychiatry, 50, 1619-1624.
Hufnagel, T.J., Kim, J.H., Lesser, R., Miller, J.M., Abrahams, J.J., Piepmeier, J. & Manuelidis, E.E. (1988) Malignant glioma of the optic chiasm eight years after radiotherapy for prolactinoma. Archives of Ophthalmology, 106, 1701-1705.
Hyodo, A,, Nose, T., Maki, Y. & Enomoto, T. (1982) Pituitary adenoma and meningioma in the same patient. Neurochirurgia,
Iacono. R.P., Apuzzo, M.L.J., Davis, R.L. & Tsai, F.Y. (1981) Multiple meningiomas following radiation therapy for medullo- blastoma. Journal of Neurosurgery, 55,282-286.
Irsy, G., Goth, M., Slovik, F., Bah t , K., Szaboles, I., Pasztor, E. & Szilagyi, G. (1985) Growth hormone producing pituitary ade- noma and meningioma. Zentralblatt fur Neurochirurgie, 46,337- 343.
Jones, A. (1960) Supervoltage X-ray therapy of intracranial
15,333-351.
37,2960-2963.
269-273.
829-83 I .
25966-67.
tumours. Annals of the Royal College of Surgeons of England 27, 310-354.
Kasantikul, V., Shuangshoti, S. & Phonprasert, C. (1988) Intrasellar meningioma after radiotherapy For prolactinoma. Journal of the Medical Association of Thailand, 71, 524-527.
Kingston, J.E., Hawkins, M.M., Draper, G.J., Marsden, H.B. & Kinnier Wilson, L.M. (1987) Patterns ofmutiple primary tumours in patients treated for cancer during childhood. British Journal of Cancer, 56,331-338.
Kirschbaum, W. (1945) Intrasellar menigioma and multiple cerebral glioblastomas. Journal of Neuropathology and Experimental Neurology, 4,370-378.
Kitamura, K., Nakamura, N. & Terao, H. (1965) Primary multiple brain tumours. Brain andNerve (Tokyo), 17, 109-117.
Kitanaka, C., Shitara, N., Nakagomi, T., Nakamura, H., Genka, S., Nakagawa, K., Akanuma, A., Aoyama, H. & Takakura, K. ( I 989) Post-radiation astrocytoma. Journal of Neurosurgery, 70, 469474.
Kjellberg, R.N. & Kliman, B. (1979) Lifetime effectiveness-a system of therapy for pituitary adenomas, emphasising Bragg- peak proton hypophysectomy. In Recent Advances in the Diagno- sis and Treatment of Pituitary Tumours (ed. J. A. Linfoot), p. 277. Raven Press, New York.
Knowles, J.F. (1982) Radiation-induced nervous system tumours in the rat. International Journal of Radiation Biology, 41, 79-84.
Kojima, G. (1979) Pituitary tumour developing subsequent to radiation therapy of pituitary. Igaku No Ayumi, 108, 601-602.
Kolodny, J. & Dluhy, R.G. (1985) Recurrent prolactinoma and meningioma following irradiation & bromocriptine treatment. American Journal of Medicine, 78, 153-155.
Komaki, S., Komaki, R., Choi, H. & Correa-Paz, F. (1977) Radiation and drug-induced intracranial neoplasm with angio- graphic demonstration. Neurologia Medico-Chirurgica (Tokyo), 17, 5562.
Kraus, J.E. (1945) Neoplastic disease of the human hypophysis. Archives of Pathology (Chicago), 39,343-349.
Lawrence, A.M., Pinsky, S.M. & Goldfine, I.D. (1971) Conven- tional radiation therapy in acromegaly. Archives of Internal Medicine, 128, 369-377.
Lawrence, J.H., Tobias, C.A., Linfoot, J.A., Born, J.L., Lyman, J.T., Chong, C.Y., Manougian, E. & Wei, W.C. (1970) Successful treatment of acromegaly; metabolic & clinical studies in 145 patients. Journal of Clinical Endocrinology and Metabolism, 31,
Lewis, C.A., Smith, P.G., Stratton, I.M., Darby, S.C. & Doll, R. (1988) Estimated radiation doses to different organs among patients treated for ankylosing spondylitis with a single course of X-rays. British Journal of Radiology, 61,2 12-220.
List, C.F., Williams, J.R. & Balyeat, G.W. (1952) Vascular lesions in pituitary adenomas. Journal of Neurosurgery, 9, 177-1 87.
Littley, M.D., Shalet, S.M., Beardwell, C.G., Robinson, E.L. & Sutton, E.M. (1989) Radiation-induced hypopituitarism is dose- dependent. Clinical Endocrinology, 31,363-373.
Liwnicz, B.H., Berger, T.S., Liwnicz, R.G. & Aron, B.S. (1985) Radiation-associated gliomas: a report of four cases & analysis of post-radiation tumours of the CNS. Neurosurgery, 17,43645.
Love, J.G. & Blackburn, C.M. (1955) Association of intracranial meningioma with pituitary adenoma. Minnesota Medicine, 37,
Maat-Schieman, M.L.C., Bots, G.T.A.M., Thomeer, R.T.W.M. &
180-198.
335-336.

396 A. Jones Clinical Endocrinology (1991) 35
Vielvoye, J. (1 985) Malignant astrocytoma following radio- therapy for craniopharyngioma. British Journal of Radiology, 58, 480482.
Martin, W.H., Cail, W.S., Morris, J.L. &Constable, W.D. (1980) Fibrosarcoma after high energy radiation therapy for pituitary adenoma. American Journal of Roentgenology, 135, 1087-1090.
Marus, G., Levin, C.V. & Rutherford, G.S. (1986) Malignant glioma following radiotherapy for unrelated primary tumours. Cancer, 58,886-94?.
Mayneord, W.V. (1978) The time factor in carcinogenesis. Health
Mayneord, W.V. & Clarke, R.H. (1975) Carcinogenesis and radia- tion risk: a biomathematical reconnaissance. British Journal of Radiology (Suppl. 12), 8-9.
McPhedran, R.S. &Tom, M.I. (1962) Multiple primary intracranial tumours. Neurology (Minneapolis), 12,524528.
Meyrignac. C., N’Guyen, J.P., Blatrix. C. & Degos, J.D.D. (1981) Meningiome postradique: complication tardive de I’irradiation de la selle turcique. La Nouvelle Presse Medicale, 10, 3246-3247,
Michaels, L. (1987) Ear, Nose and Throat Histoputhology. pp. 194- 20 I . Springer-Verlag. London.
Miller, D.R., Albo, V., Leikin, S., Littman, P., Boesl, C., Sather, H. & Hammond, D. (1986) Brain tumours in survivors of childhood acute lymphoblastic leukaemia. Proceedingsof the 18th Meeting of the International Society of Paediarric Oncology, pp. 77-79.
Mindel, J.S. & Fetell. M.R. (1985) A pituitary adenoma with dilated ventricles. Survey of Ophthalmology, 30,59-61.
Moots, P.L. & Rubinstein, L.J. (1984) Multiple neoplasms of the nervous system. In Risk Factorsand Multiple Cancer, pp. 331-351. (ed. B. A. Stoll), J. Wiley, Chichester.
Morin, M., Boncorps, J. & Masse, R. (1989) Etude exphimentale des effets biologiques d’une irradiation gamma pendant les pkriodes intra-uterine et post-natale chez le rat. Radioprotection,
Mountcastle, R.B., Roof, B.S., Mayfield, R.K., Mordes, D.B., Sagel, J., Biggs, P.J. & Rawe, S.E. (1989) Pituitary adenocarci- noma in an acromegalic patient (case report & review of literature). American Journal of the Medical Sciences, 298(2), 109- 118.
Mustacchi, P. & Shimkin, M.B. (1957) Occurrence of cancer in acromegaly and in hypopituitarism. Cancer, 10, 100-104.
Naessen, R. (1 970) The identification and topographical localisation of the olfactory epithelium in man & other mammals. Acta Otolaryngologica, 70, 51-57.
Nagatani, M., Ikeda, T., Otsuki, H., Mizuta,T., Mori, S., Ushio, Y., Hayakawa, T., Mogami, H., Matsumoto, K. & Mori, H. (1984) Sellar fibrosarcoma following radiotherapy for prolactinoma. No Shinkei Geka (Neurological Surgery). 12 (Suppl. 3), 339-346.
Nakasu, S., Hirano, A., Shimura, T. & Llena, J.F. (1987) Incidental meningiomas in autopsy study. Surgical Neurology, 27,319-22.
Ng, H.K., Poon, W.S., Poon, C.Y.F. & South, J.R. (1988) lntracranial olfactory neuroblastoma mimicking carcinoma, His- topathology, 12,393-403.
O’Connell, J.E.A. (1961) Intracranial meningiomata associated with other tumours involving the central nervous system. British Journal of Surgery, 48, 313-383.
Ohata, K. (1985) Simultaneous occurrence of pituitary adenoma & falcotentorial junction meningioma. Neurologia Medico-Chirur- gica (Tokyo) , 25,680-686.
Okamoto, S., Handa, H., Yamashita J., Tokuriki, Y. & Abe, M.
Physics, 34, 297-309.
24, 109-121.
(1 985) Post-irradiation brain tumours. Neurologia Medico- Chirurigica (Tokyo), 25,528-533.
Packer, R.J., Meadows, A.T., Rorke, L.B., Goldwein, J.L. & DAngio, G. (1987) Long-term sequelae of cancer treatment on the central nervous system in childhood. Medical and Pediatric Oncology, 15,241-253.
Pages, A., Pagks, M., Ramos, J. & Benezech, J. (1986) Radiation- induced intracranial fibrochrondrosarcoma. Journal of Neuro-
Pak, S.G. & Uzmanova, R.R. (1965) On primary multiple brain tumours. Zdravookhr Kazakhstana, 8,4243.
Parent, A.D. (1990) Late complications of radiation-induced neo- plasms (letter). Neurosurgery, 26, 1090-1091.
Partington, M.D. & Davis, D.H. (1990) Radiation-induced men- ingioma after treatment for pituitary adenoma. Neurosurgery, 26,
Piatt, J.H., Blue, J.M., Schold, S.C. & Burger, P.C. (1983) Glio- blastoma after radiotherapy for acromegaly. Neurosurgery, 13,
Pieterse, S., Dinning, T.A.R. & Blumberg, P.C. (1982) Post- irradiation sarcomatous transformation ofa pituitary adenoma: a combined pituitary tumour. Joural of Neurosurgery, 56,283-286.
Powell, H.C., Marshall, L.F. & Ignelzi, R.J. (1977) Post-irradiation pituitary sarcoma. Acta Neuropathologica (Berlin), 39, 165-1 67.
Preissig, S.A., Bohmfalk,G.L., Reichel,G.W.&Smith, M.T. (1979) Anaplastic astrocytoma following radiation for a glomus jugulare tumour. Cancer, 43,2243-2247.
Probst, A. (1971) Kombination eines Cushing-Syndroms, Hypophy- sadenoms und suprasellaren Meningioms-Fallbericht. Zenrralb- latr f i r Neurochirurgie, 32,75-82.
Richards, M.A., Webb, J.A.W., Jewel], S.E., Gregory. W.M. & Reznek, R.H. (1988) In-vivo measurement of spin lattice relaxa- tion time (TI) of bone marrow in healthy volunteers: the effects of age and sex. British Journal of Radiology, 61,3&33.
Rimm, LA., Li, F.C., Tarbell, N.J., Winston, K.R. & Sallan, S.E. (1987) Brain tumours after cranial irradiation for childhood acute lymphoblastic leukaemia. Cancer, 59, 1506-1 508.
Robinson, E., Neugut, A.I. & Wylie, P. (1988) Clinical aspects of postirradiation sarcomas. Journalof rhe National Cancer Institute,
Robinson, R.G. (1978) A second brain tumour and irradiation. Journal of Neurology. Neurosurgery and Psychiatry, 41, 1005- 1012.
Ron, E., Modan, B., Boice, J.D., Alfandary, E., Stovall, M., Chetrit, A. & Katz, L. (1988) Tumors of the brain and nervous system after radiotherapy in childhood. New England Journalof Medicine, 319,
Rotblat, J. (1988) The cancer risk from low doses of radiation. What can be learned from the A-bomb survivors? Journal of Radiation Protection, 8,3946.
Rubinstein, A.B., Salit, M.N., Cohen, M.L., Zandbank, U. & Reichenthal, E. (1984) Radiation-induced cerebral meningioma: a recognisable entity. Journal of Neurosurgery, 61, 966-971.
Rubinstein, L.J. (1972) Tumours of the central nervous system. In ArIas of Tumor Pathology. 2nd. Series, Fascicle 6, p. 191. Armed Froces Institute of Pathology, Washington.
Russell, J.A. (1966) Quoted (ref. 21) as’personal communication’ by Waltz and Brownell (1966).
Salvati, M., Ramundo Orlando, E., Causo, R., Innocenzi, G., Capone. R., Cosentino, F. Jr. & Cosentino, F. (1990) Tumors of
logy. 233, 309-3 10.
329-331.
85-89.
80,233-240.
1033- 1039.

Clinical Endocrinology (1991) 35 Radiation oncogenesis pituitary tumours 397
the central nervous system induced by ionising radiation. Giornale Italiano Oncologico, 10, 15-18.
Schneider, C. & Montz, R. (1966) Die quantitative Verteilung des erythropoietischen Knochenmarks beim Menschen gemessen mit Radioeisen. Klinische Wochenschrift, 16,969-973.
Schapiro, S . , Mealey, J. & Sartorius, C. (1989) Radiation-induced intracranial malignant gliomas. Journal of Neurosurgery, 71, 77- 82.
Sheline, G.E. (1979) Role of conventional radiation therapy in treatment of functional pituitary tumours. In Recent Advances in the Diagnosis and Treatment of Pituitary Tumours (ed. J. A. Linfoot), pp. 289-313. Raven Press, New York.
Sheline, G.E., Goldberg, M.B. & Feldman, R. (1961) Pituitary irradiation in acromegaly. Radiology, 76, 70-75.
Shi, T., Farrell, M.A. & Kaufmann, J.C.E. (1984) Fibrosarcoma complicating irradiated pituitary adenoma. Surgical Neurology, 22,277-283.
Shin, H., Ishige, N., Nakamura, T. Yamamura, A. & Makino, H. ( I 980) Pituitary fibrosarcoma secondary to radiation therapy for the treatment of chromophobe adenoma. No Shinkei Geka
Shuangshoti, S. (1986) Combined Occurrence of third ventricular germinoma & hypothalamic mixed glioma. Journal of Surgical Oncology, 31, 148-152.
Soffer, D., Pittaluga, S., Feiner, M. & Beller, A.J. (1983) Intracranial meningiomas following low-dose irradiation to the head. Journal of Neurosurgery, 59, 1048-1053.
Soffer, D., Gornori, J.M., Siegl. T. & Shalit, M.N. (1989) Intra- cranial meningiomas after high-dose irradiation. Cancer, 63,
Sogg, R.L.. Donaldson, S.S. & Yorke, C.H. (1978) Malignant astrocytoma following radiotherapy of a craniopharyngioma. Journal of Neurosurgery, 48,622-627.
Spallone, A. (1982) Meningioma as a sequel of radiotherapy for pituitary adenoma. Neurochirurgia, 25, 68-72.
Spallone, A., Gagliardi, F.M. & Vagnozzi, R. (1979) Intracranial meningiomas related to external cranial irradiation. Surgical Neurology, 12, 153-159.
Sridhar, K. & Ramamurthi, B. (1989) Intracranial meningioma subsequent to radiation for a pituitary tumour. Neurosurgery, 25,
Stock, J.M., Ghatak, N.R. & Oppenheimer. J.H. (1975) Unsus- pected meningioma in a patient with pituitary gigantism. Meta- bolism, 24, 767-775.
Suda, Y., Mineura, K. & Kowada, M. (1989) Malignant astrocy- toma following radiotherapy for pituitary adenoma. No Shinkei Geka (Tokyo), 17,783-787.
Tamura, T., Nakamura, S., Shirata, K., Sato, K., Tsubokawa, T. & Sawada, T. (1989) Cerebellar malignant glioma after radiation therapy for suprasellar germinoma. Neurological Medicine and Surgery (Tokyo), 29,223-229.
Terry, R.D., Hyams, V.J. & Davidoff, L.M. (1959) Combined non-
(Tokyo) 8,605-614.
15 14-1 5 19.
643-645.
metastasizing fibrosarcoma and chromophobe tumour of the pituitary. Cancer, 12, 791-798.
Tiberin, M., Maor, E., Zaizov, R., Cohen, I.J., Hirsch, M., Yosefovich, T., Ronen, J. & Goldstein, J. (1984) Brain sarcoma of meningeal origin after cranial irradiation in childhood acute lymphocytic leukaemia. Journal of Neurosurgery, 61, 772-776.
UNSCEAR (United Nations Scientific Committee on the Effects of Atomic Radiation) (1988) Sources, effects & risks of ionising radiation (Annex F). United Nations, New York.
Ushio, Y., Arita, N., Yohimine, T., Nagatani. M. & Mogami, H. ( I 987) Glioblastoma after radiotherapy for craniopharyngioma. Neurosurgery, 21,33-38.
Vikhert, T.M. & Kasunova, S.V. (1980) Postirradiation fibrosar- coma of pituitary. Zhurnal Voprosy Nierokhirurgii, 457-58.
Von Wild, K. & Ruf. H. (1973) Diagnostic problems and errors in suprasellar meningiomas. In Modern Aspects of Neurosurgery (ed. H. Kuhlendahl), pp. 4347. Excerpta Medica: International Congress Series No. 306.
Waltz, T.A. & Brownell, B. (1966) Sarcoma: a possible result of effective radiation therapy for pituitary adenoma. Journal of Neurosurgery. 24,901-907.
Wheelock, M.C. (1963) Eosinophilic adenoma of pituitary with sarcomatous changes. Cancer Seminar, 3, 77-80.
Willis, R.A. (1938) A pathological study of tumours of the pituitary region. Medical Journal of Australia, 1,287-291.
Wise, B.L., Malamud, N. & Baldrey, E.B. (1953) Multiple intra- cranial tumours: glioma associated with hypophyseal chromo- phobe adenorna: a report of two cases. Journalof Neuropathology and Experimental Neurology, 12,224-23 I .
Wright, A.D.. Hill, D.M., Lowy, C. & Russell Fraser, T. (1970) Mortality in acromegaly. Quarterly Journal qf Medicine 39 (NS),
Yamada, K.. Hatayama, T., Ohta, M., Sakoda, K. & Uozumi, T. (1986) Coincidental pituitary adenoma & parasellar meningioma. Neurosurgery, 19,267-270.
Yang, D.T. (1 982) Intracranial malignant meningioma occurring after radiotherapy. Chung Hua Shen Ching Ching Shen KO Tsa Chih (Chinese Journal of Neurology and Psychiatry), 15(4). 245- 248.
Zampieri, P., Zorat, P.L., Mingrino. S . & Soattin, G.B. (1989) radiation-associated cerebral gliomas. Journal of Neurosurgical Science, 33, 27 1-279.
Zentner, J. & Gilsbach, J. (1989) Pituitary adenoma & meningioma in the same patient: report of 3 cases. European Archives of Psychiatry and Neurological Science, 228, 144148.
Zuccarello, M., Sawaya, R. & De Courten-Myers, G. (1986)1 Glioblastoma occurring after radiation therapy for meningioma. Neurosurgery, 19, 114-1 19.
Ziilch, K.J. (1956) Biologie und Pathologie der Hirngeschwulste. In Handbuch der Neurochirurgie. Volume 3 (ed. H. Olivecrona & W. TBnnis), pp. 62,492. Springer: Berlin.
1-16.