Introduction
The family of tropomyosin kinase receptors, TRKA, B and C are
encoded by three distinct genes, NTRK1, 2, and 31
After embryogenesis, TRK proteins are primarily restricted to
the nervous system, and function during normal neuronal development
and maintenance2-4
Fusion events with the kinase domain of NTRK1, 2, and 3 genes
with various partners result in NTRK gene fusions, which are
oncogenic drivers (Figure 1)1,2
Recurrent chromosomal rearrangements that involve each NTRK gene
have been identified and shown to be oncogenic drivers across a
wide variety of adult and pediatric cancers1,5,6
NTRK gene fusions have been identified in >20 tumor types;2
they have been implicated in up to 1% of all solid tumors,
including non-small-cell lung cancer (NSCLC) and are nearly
pathognomonic among certain rare cancers, including mammary
analogue secretory carcinoma (MASC) and secretory breast
carcinoma1,3,7,8,9
– In NSCLC, NTRK gene fusions have been reported to occur at an
approximate frequency of 0.23%1
– Patients with NSCLC harboring NTRK gene fusions had no
concurrent oncogenic alterations in KRAS, EGFR, ALK, ROS1, or other
known drivers1
– NTRK gene fusions occur in patients with NSCLC regardless of
gender, age, and smoking history1
– Fusions identified in patients with NSCLC predominantly
involve either NTRK1 or NTRK31
Larotrectinib is the first highly selective oral TRK inhibitor
in clinical development (Figure 2)3,10
– Larotrectinib demonstrated tumor-agnostic efficacy in 55
patients with TRK fusion cancers in 17 unique tumor types enrolled
across 3 clinical trials3
– Larotrectinib was well tolerated in children and adults in the
clinical trials3
– Larotrectinib demonstrated durable antitumor activity in the
overall study population with an independent review (IR)-assessed
objective response rate (ORR) of 75%, and an ORR of 80% according
to investigator assessment, with 71% patients still responding to
treatment at one year (Figure 3)3
Figure 1: TRK fusions are rare but recurrent oncogenic
drivers
Rapid, robust and durable responses to larotrectinib in patients
with TRK fusion non-small cell lung cancerFarago AF,1 Kummar S,2
Ibabekci S,3 Corsi-Travali S,3 Cruickshank S,3 Cox MC,3 Ku NC,3
Drilon A4
1Cancer Center, Massachusetts General Hospital, Boston, MA, USA;
2Stanford Cancer Institute, Stanford, CA, USA; 3Loxo Oncology,
Inc., South San Francisco, CA, USA; 4Memorial Sloan Kettering
Cancer Center, New York, NY, USA
Figure 2: Larotrectinib is a highly selective pan-TRK
inhibitor
Objectives
The primary endpoint of the combined analysis across three
clinical studies (NCT02122913, NCT02637687, and NCT02576431) is to
determine the ORR of larotrectinib, by an independent review
committee (IRC)
Secondary objectives included the determination of the safety of
larotrectinib and ORR according to investigator assessment
Here, we report the details and follow-up of 4 patients with TRK
fusion NSCLC as of February 19, 2018
ERK
AKT
Promoter 5ʹ partner
5ʹ partner
Tyr Tyr
LBD Kinase domain
TRK kinase domain
5ʹ partner
Tyr Tyr
TRK kinase domain 5ʹ partner
Tyr Tyr
TRK kinase domain
NTRK1/2/3
TKL
STE
CK1
AGC
CAMK
CMGC
TK
TRKA/B/C
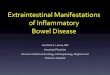
Figure 3: Efficacy of larotrectinib in patients with
non-small-cell lung cancer
50
40
30
20
10
0
–10
–20
–30
–40
–50
–60
–70
–80
–90
–100
Max
imum
cha
nge
in tu
mor
siz
e (%
)
Lung
Other solid tumors
Data presented in this waterfall plot are
investigator-assessedNote: One patient not shown here. Patient
experienced clinical progression and no post-baseline tumor
measurements were recordedModified from: Drilon et al. N Engl J
Med. 2018; 378:731-39
Adverse events regardless of attribution Treatment-related
adverse events
Grade 1 Grade 2 Grade 3 Grade 4 Any grade Grade 3 Grade 4Any
gradePercent of patients with event
Increased ALT or AST 31 4 7 0 42 5 0 38Fatigue 20 15 2 0 36 0 0
16Vomiting 24 9 0 0 33 0 0 11Dizziness 25 4 2 0 31 2 0 25Nausea 22
7 2 0 31 2 0 16Anemia 9 9 11 0 29 2 0 9Diarrhea 15 13 2 0 29 0 0
5Constipation 24 4 0 0 27 0 0 16Cough 22 4 0 0 25 0 0 2Increased
body weight 11 5 7 0 24 0 0 11Dyspnea 9 9 0 0 18 0 0 2Headache 13 4
0 0 16 0 0 2Pyrexia 11 2 2 2 16 0 0 0Arthralgia 15 0 0 0 15 0 0
2Back pain 5 9 0 0 15 0 0 0Decreased neutrophil count 0 7 7 0 15 2
0 9
AST, aspartate aminotransferase; ALT, alanine aminotransferase;
Modified from: Drilon et al. N Engl J Med. 2018; 378:731-39. The
adverse events listed here are those that occurred in at least 15%
patients, regardless of attribution. The relatedness of the
treatment to adverse events was determined by the
investigators.
Table 2: Safety profile of larotrectinib in overall study
population (n=55) Patient 2: TPR-NTRK1 fusion non-small-cell lung
cancer 28-year-old male diagnosed with Stage IV NSCLC,
adenocarcinoma with neuroendocrine features, with brain and bone
metastases
NTRK fusion gene detected by FoundationOne Prior treatment with
cisplatin and etoposide, which was discontinued due to progressive
disease (PD), followed by radiotherapy resulting in stable
disease
Following initiation of larotrectinib at a starting dose of 100
mg twice-daily, the patient experienced a marked improvement in
symptoms of cough and back pain by Study Day 29
Best overall response was partial response, with a duration of
response of 8.21 months (Table 1) PD was identified as metastasis
to the right femur. Treatment continued with an escalated dose (150
mg BID) for 5.22 months and discontinued after development of more
widespread PD (Figure 4)
At disease progression, sequencing of plasma DNA using the
Guardant360 platform revealed the presence of a G595R solvent front
mutation and a G667S xDFG mutation in NTRK1, likely explaining the
disease progression
All adverse events were grade 1 with no serious adverse events
reported
Gene fusion MeasurablediseaseBest
responseDOR
(months)Ongoing
treatmentPatient 1 ETV6-NTRK3 No SD* >14.78* Yes
Patient 2 TPR-NTRK1 Yes PR 8.21 No**
Patient 3 IRF2BP2-NTRK1 No CR >20.27 Yes
Patient 4 SQSTM1-NTRK1 Yes PR >12.88 NoData presented are as
per IRC of February 19, 2018*PR per investigator
assessment**Identified solvent front acquired resistance mutation
in the fusion gene at the time of progressionCR, complete response;
DOR, duration of response; PR, partial response; SD, stable
disease
Table 1: Efficacy of larotrectinib in patients with
non-small-cell lung cancer
1. Farago AF et al. JCO Precis Oncol 2018:2;1-12.2. Vaishnavi A
et al. Cancer Discov. 2015; 5:25-34.3. Drilon A et al. N Engl J
Med. 2018; 22(378):731-39.4. Huang EJ et al. Annu Rev Biochem.
2003; 72:609-42.5. Landman et al. Clin Breast Cancer, 2018;
18(3):e267-e270.
6. Laetsch TW et al. Lancet Oncol. 2018;19(5):705-714.7. Amatu A
et al. ESMO Open. 2016; 1:e000023.8. Skalova A et al. Am J Surg
Pathol. 2010; 34:599-608.9. Tognon C et al. Cancer Cell. 2002;
2:367-76.
10. Hyman DM et al. J Clin Oncol. 2017; 35(suppl):abstr
LBA2501.
AcknowledgmentsWe thank the patients and their families, many of
whom traveled long distances to participate in these studies. Under
the authors’ conceptual direction, medical writing assistance was
provided by Alison Scott, PhD and Tina Tremaine, PhD, of Scion
(London, UK), funded by Bayer Healthcare. These studies are funded
by Loxo Oncology, Inc.
Baseline Cycle 3, Day 1 Cycle 7, Day 1
Figure 4: Durable response in TPR-NTRK1 fusion non-small-cell
lung cancer
Patient 3: IRF2BP2-NTRK1 fusion non-small cell lung cancer
31-year-old female diagnosed with Stage IV NSCLC adenocarcinoma,
with metastases to the left side of the neck, axillae, and the
right internal mammary node
NTRK fusion gene detected by FoundationOne History of Hodgkin
lymphoma treated with ABVD chemotherapy and subsequent radiation to
the abdomen and supraclavicular fossa
At baseline, the patient presented with peripheral neuropathy,
neck pain, and mucositis with no response to all prior systemic
treatments including cisplatin, pemetrexed, and docetaxel
In response to larotrectinib 100 mg BID, a complete response was
confirmed at Study Day 56, with complete resolution of all baseline
symptoms (Figure 5)
The duration of response by RECIST was >20.27 months, and the
patient remains on treatment (Table 1) Adverse events were
primarily grade 1, with no serious adverse events reported
Patient 1: ETV6-NTRK3 fusion in adenocarcinoma of the lung
76-year-old male diagnosed with Stage IV lung adenocarcinoma, with
metastases to the liver and bone NTRK fusion gene detected by
FoundationOne Prior treatment included a pneumonectomy in
combination with radiotherapy and unspecified chemotherapy. After
localized and systemic relapse, he received systemic treatment with
carboplatin, pemetrexed, gemcitabine, and nivolumab, with best
response of SD
Baseline symptoms were cough, dyspnea, and fatigue The starting
dose of larotrectinib was 100 mg twice daily, by cycle 2 there was
notable improvement in anorexia and the ECOG PS improved from ECOG
2 to ECOG 1
A partial response was assessed by the investigator with a
duration of response (DOR) >14.78 months and the patient remains
on treatment (Table 1)
Treatment-emergent adverse events (TEAEs) were all grade 1.
There were no grade 2, 3, or 4 TEAEs reported
Conclusions Targeted TRK inhibition with larotrectinib produced
rapid symptom resolution, a high RECIST response rate, and durable
disease control in patients with NSCLC harboring NTRK gene
fusions
Larotrectinib was well tolerated in patients with NSCLC with no
progressive central nervous system events observed; this safety
profile suggests that long-term treatment is feasible
The results from these cases provide specific support for the
tumor-agnostic efficacy observed in the pooled analysis3
Data from these patients, and the overall clinical trial
program, provide strong evidence for the inclusion of routine
testing for NTRK gene fusions in patients with lung cancer
References
Methods
For the primary analysis, 55 patients (aged 4 months to 76
years) with TRK fusion cancer detected by molecular profiling, were
enrolled across 3 clinical trials (NCT02122913, NCT02637687, and
NCT02576431)
Eligibility criteria for enrollment of patients into clinical
studies required locally advanced or metastatic solid tumor, ECOG
score of 0–3, adequate major organ function and no prior
TRK-inhibitor therapy
Patients received larotrectinib at 100 mg twice-daily (BID)
orally, until disease progression occurred or a lack of clinical
benefit
Tumor response was assessed by investigators and by independent
radiology review at baseline and every 8 weeks for 1 year, and
every 12 weeks thereafter until disease progression, according to
RECIST v 1.1. First protocol assessment was required at the end of
cycle 2
All response data in this poster are presented based on
independent radiology review (unless otherwise noted); the
waterfall plot is based on investigator assessment
Safety data were recorded until 28 days after the last dose of
larotrectinib and adverse events were graded according to the
Common Terminology Criteria for Adverse Events v 4.0
From the 55 patients in the primary analysis set, 4 adult
patients with previously treated lung adenocarcinoma with an NTRK
gene fusion, detected by molecular profiling from CLIA-certified
laboratories, were identified
Results
Durable responses (ranging from 8.21 to >20.27 months) were
seen in 3 of 4 patients with NSCLC harboring NTRK gene fusions
treated with larotrectinib (Table 1)
In the overall population of 55 patients with TRK fusion
cancers, the majority of adverse events (93%) were grade 1 or 2,
with few grade 3 or 4 events reported (Table 2). Adverse events
leading to dose reduction occurred in only 15% of patients
Larotrectinib was well tolerated in patients with NSCLC, with
the occurrence of primarily grade 1 adverse events reported, except
for one grade 2 adverse event (decreased neutrophil count) noted
across patients
Baseline 2 Months
Figure 5: Durable response in IRF2BP2-NTRK1 fusion
non-small-cell lung cancer
Durable response in ETV6-NTRK3 fusion non-small-cell lung
cancer
Baseline Cycle 4
Figure 6: Durable response in SQSTM1-NTRK1 fusion non-small-cell
lung cancer
Patient 4: SQSTM1-NTRK1 fusion non-small-cell lung cancer
45-year-old female diagnosed with Stage IV NSCLC adenocarcinoma,
with metastases in the liver and mediastinum and symptoms of
hypertrophic osteoarthropathy (HOA)
NTRK fusion gene detected by Paradigm Cancer Diagnostics She had
received previous platinums (cis- and carbo-) and pemetrexed with a
confirmed best response to treatment of SD
Baseline symptoms included arthralgia due to HOA, cough causing
sleep disturbance, and fatigue The patient experienced a rapid
response to larotrectinib 100 mg twice daily, demonstrated by an
improvement in HOA symptoms, cough and fatigue by cycle 1 (Study
Day 8) and complete absence of cough by cycle 3. A partial response
was noted by Study Day 54
The duration of response by investigator assessment was
>12.88 months. She subsequently withdrew consent in order to
pursue alternative non-traditional therapies
Adverse events were primarily grade 1, with one grade 2 event
reported.
DisclosuresA.F.F. received research support from Bayer and Loxo
Oncology and provided consulting to Bayer and Loxo Oncology. A.D.
has provided consulting to Loxo Oncology. M.C.C., N.C.K., S.C-T.,
S.C. and S.I. are employees of Loxo Oncology. S.K. has no conflicts
of interest to disclose.
18002318 Larotrectinib Poster 86x36 inches v16.indd 1 13/09/2018
10:40