Embed Size (px)
Citation preview
Recognition and management of Cauda
Equina Syndrome
James BoothConsultant Spine Practitioner
* Cauda Equina first described in 1600
(Andreas Lazarius)-Syndrome not described
until 1934 (Mixter and Barr)
v CE provides innervation to lower limbs,
sphincters, sensory innervation to saddle area and
parasympathetic innervation to bladder and
distal bowel
* L4-5 (57%), L5-S1 (30%), L3-4(13%)
Background to CES
* It occurs as a consequence of the loss of functionof two or more of the eighteen nerve roots whichcomprise the cauda equina (Woolsley & Martin 2003)
* CE nerve roots vulnerable; no Schwann cell cover and due to microvascular system have region of relative hypovascularity
* Nerve roots show mild demyelination after mild cauda equinacompression
* CES is considered a potential emergency within spinal surgery(Fraser et al, 2009)
Background to CES
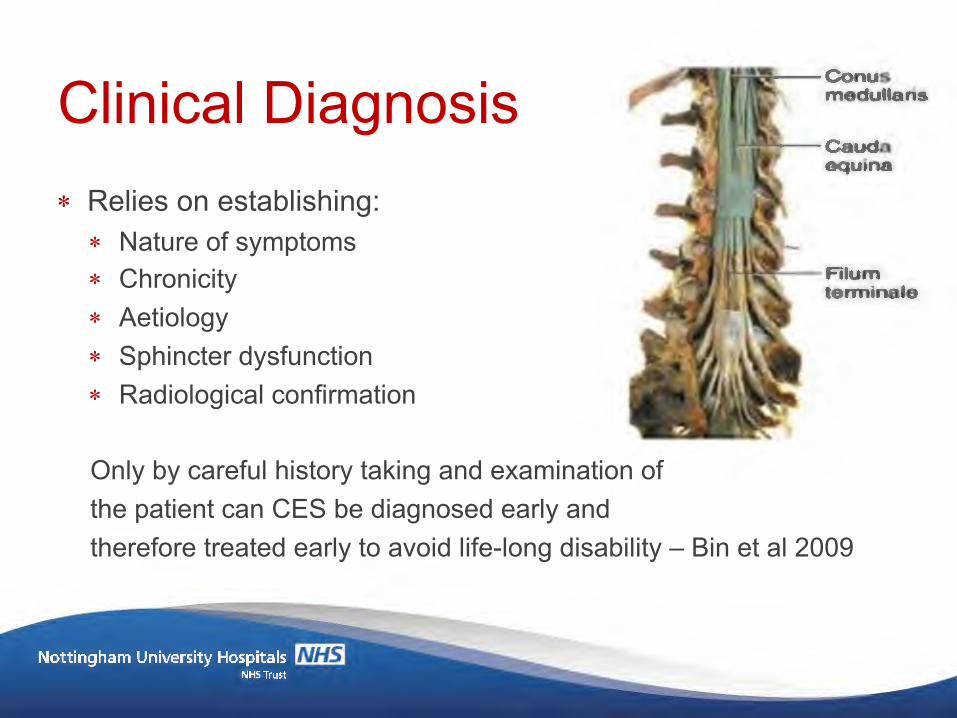
* Relies on establishing:* Nature of symptoms* Chronicity* Aetiology* Sphincter dysfunction* Radiological confirmation
Only by careful history taking and examination ofthe patient can CES be diagnosed early andtherefore treated early to avoid life-long disability – Bin et al 2009
Clinical Diagnosis
* Diagnosis can be challenging and worrying process* Only 10% of suspected CES are confirmed by radiology* There is still no broadly accepted definition or diagnostic
criteria for CES (Fraser et al 2009)* Initial signs and symptoms can be subtle and vague (Bin
et al 2009)
Clinical diagnosis
* One or more of the following must be present in order to make a provisional diagnosis of CES:
* bladder and/or bowel dysfunction* sexual dysfunction* reduced sensation in the saddle area!!!
Definition (Fraser et al 2009)
* Significantly more patients are referred on for further investigation compared with those having a radiologically confirmed diagnosis of CES (Balasubramaniani et al, 2010)
* Retrospective review of 753 consecutive LBP patients;* 14% had saddle anaesthesia* 28% altered bladder and bowel function* 27% bladder and bowel control had changed with the onset
of their LBP…….
Reliable Detection
* … only one of these patients had a radiologically confirmed CES that was managed by emergency surgery (Buchanan 2013)
* The cause of these symptoms can be misattributed to CES when the source of the problem may be something less serious
Reliable Detection
* Opioid Salts can cause constipation (e.g. Tramadol, Codeine)
* Anticonvulsants may cause urinary incontinence (e.g. Gabapentin, Pregabalin)
* Antidepressants; retention, sexual dysfunction(e.g. Amitriptyline, Nortriptyline)
Bladder, bowel and sexual dysfunction- Red Herrings
* Stress incontinence
* Pain inhibition* Prostate dysfunction; BPH 30% of 60-69 year olds and
40% of 70-79 year olds
* Erectile dysfunction; (ED) in males with CVD has been reported as high as 65%
Bladder, bowel and sexual dysfunction – Red Herrings
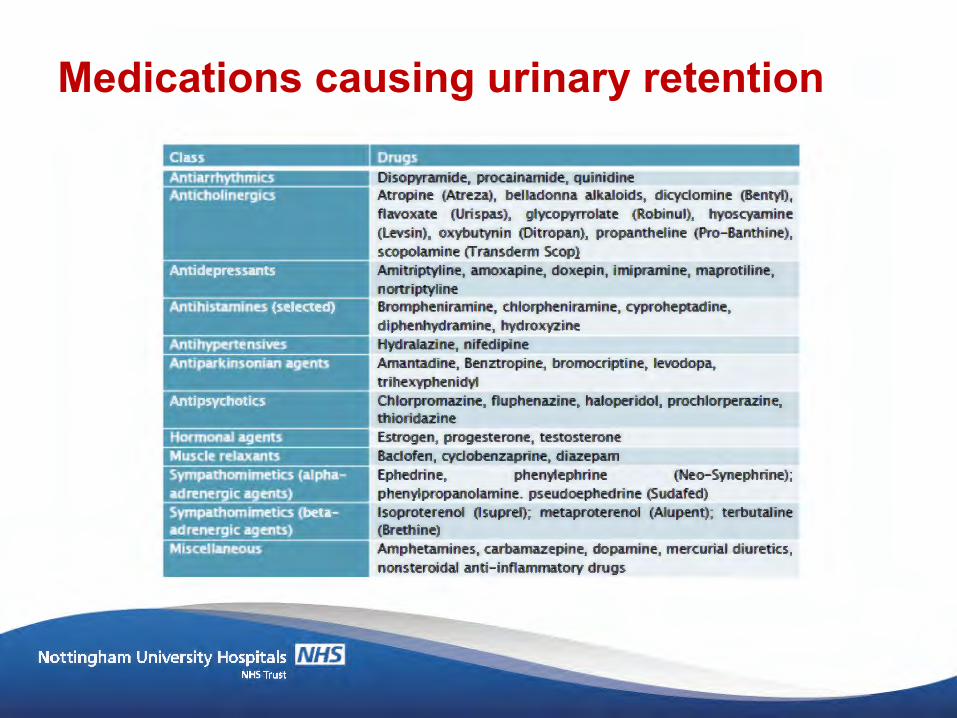
Medications causing urinary retention
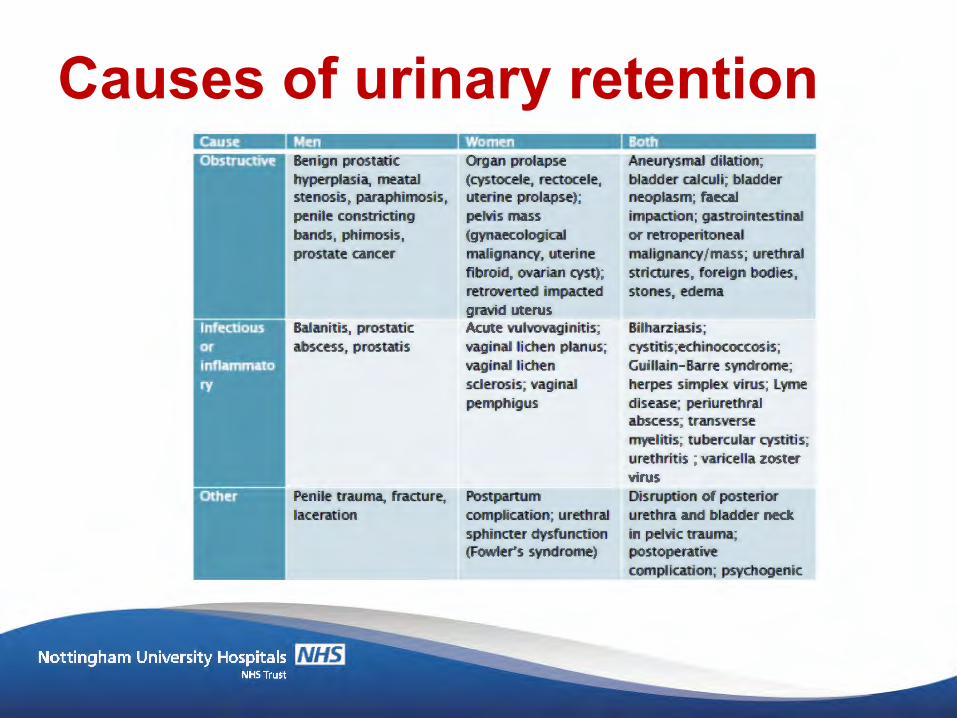
Causes of urinary retention
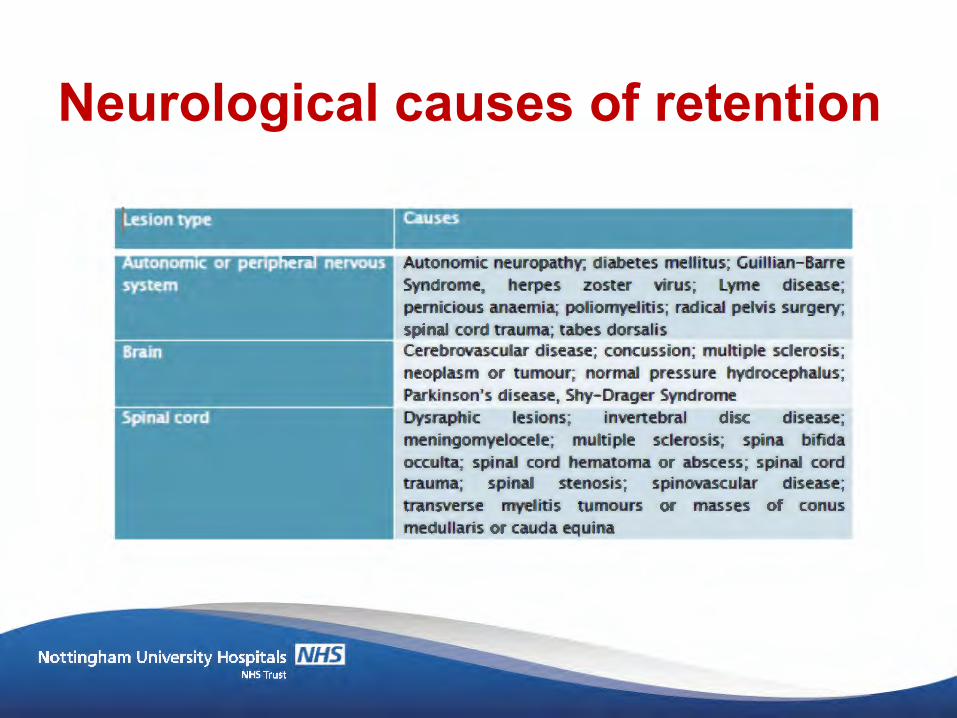
Neurological causes of retention
* Analysis by Korse et al (2013) – 15 studies and 464 patients identified that:* Bladder dysfunction was prevalent in 88.9% of patients with
CES at initial presentation to a healthcare setting* 80.8% of patients complained of saddle anaesthesia during
their initial clinical assessment* Only 47.1% of those with CES had a defaecation
dysfunction at initial presentation
Bladder and bowel Dysfunction
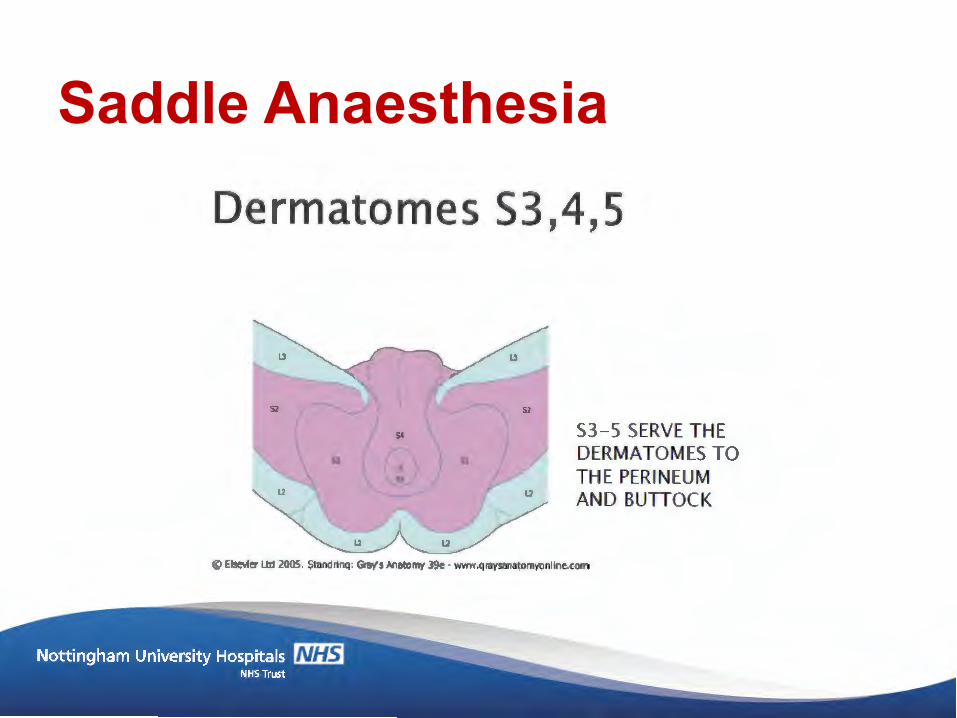
Saddle Anaesthesia
* Incomplete Cauda Equina Syndrome (CESI)* Altered urinary sensation* Loss of desire to void* Need to strain to micturate* Increased frequency of micturition* Increased urgency of micturition
* SURGICAL EMERGENCY
CES – Complete vs Incomplete
* Complete Cauda Equina Syndrome (CESR)* Painless urinary retention* Lack of awareness of need to void* Overflow incontinence (dribbling)* Anorectal continence lost* Penile erection may be achieved at times* Ejaculation weak or lost
* SURGICAL EMERGENCY WINDOW GONE
CES – Complete vs Incomplete
* Symptoms* Back pain (86%)* Perineal numbness (86%)* Unilateral sciatica (57%)* Loss of urinary sensation (46%)
Common Presentation (Ng 2004)
* Signs* Bilateral loss of perineal sensation (53%)* Unilateral loss of perineal sensation (31%)* Unilateral absent ankle jerk (40%)* Absent anal tone (38%)
Common Presentation (Ng 2004)
* “I am going to ask you some really important questions”
* Patients report that some questions do not appear to have face validity when they are in a lot of pain i.e. What has my bladder got to do with my severe back pain? My sexual function normal??
* Explain time frame and seriousness* Chronology is critical – is the picture changing?
Framing your questions
* Loss of feeling/pins and needles between your inner thighs or genitals* Numbness in or around your back passage or buttocks* Altered feeling when using toilet paper to wipe yourself* Difficulty when you try to urinate* Loss of sensation when you pass urine* Leaking urine or recent need to use pads* Difficulty to stop or control your flow of urine* Not knowing when your bladder is either full or empty* Inability to stop a bowel movement or leaking* Loss of sensation when you pass a bowel motion* Change in ability to achieve an erection or ejaculate* Loss of sensation in genitals during sexual intercourse* Bilateral leg pain
CES – Warning Signs
* Determined by the clinical setting* If you suspect – refer* Only perform PR/Bladder scan if within scope* Make it clear if you have concerns regarding CES* Supporting documentation incl:* Relevant history* Neurological exam - motor
- sensory- reflexes- long tract signs (clonus, babinski etc)- neural tension signs
Clinical Assessment
* Influenced by multiple factors, aetiology, speed of onset, duration of compression, degree of neurological deficit, signs and symptom & spinal level
* Severity of bladder dysfunction at the time of surgery is key factor to bladder function recovery
Prognosis
* Clock begins at the onset of urinary or bowel dysfunction* Early bowel dysfunction poor prognosis* CES presenting to A&E only 19% had bilateral sciatica,
lower limb weakness, saddle anaesthesia and sphincter tone disturbance ie. Good surgical opportunity(Jalloh, 2007)
Surgical Window
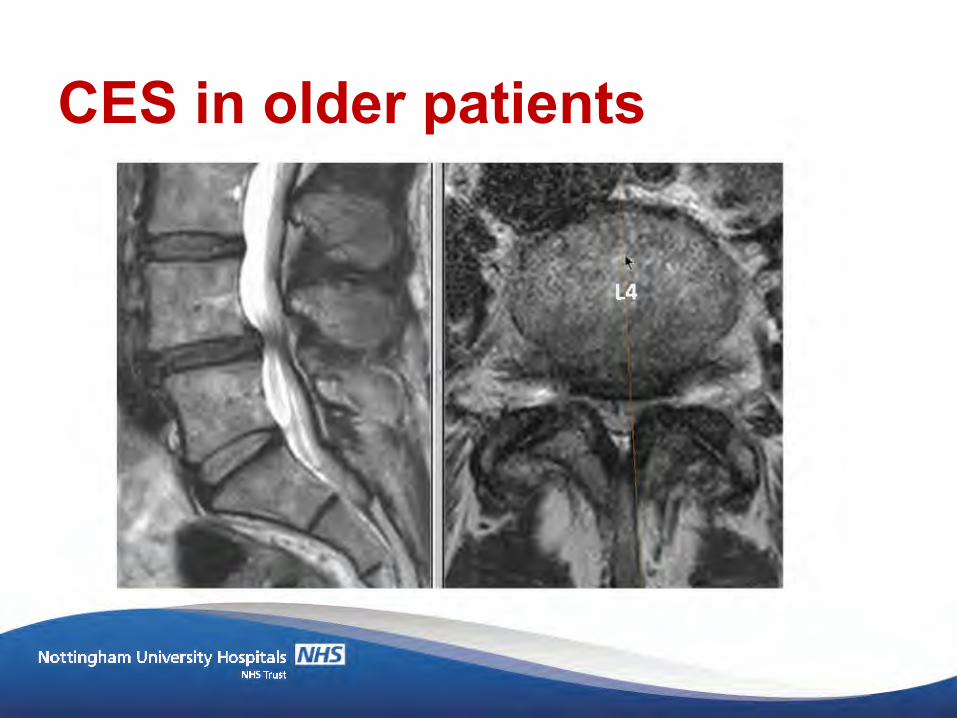
* Lumbar spine stenosis (LSS) results from degenerative
changes in spine and is common (Kalichman 2009)
* 45-60% of over 65s have MRI evidence of LSS (Haig
2006)
* Sx vary from mild, intermittent leg discomfort to severe
and disabling pain, sensory and motor dysfucntion
(Genevay & Atlas 2010)
* Attributed to transient ischaemia of CE nerves by
combination of mechanical pressure, intraneural root
oedema and venous congestion (Pronin 2019)
CES in older patients
CES in older patients

CES in older patients
* Differs from acute CES presentation in <50s * Canal compromised by combination of disc, FJA and
LFH* Sx in LSS has a dynamic component, dependant on
posture (Kobayashi 2014)* Typical presentation – increasing LBP
* Increasing LBP* Insidious onset uni/bilat LL sensory disturbance* With or without motor weakness
CES in older patients
* As well as neurogenic claudicant sx, patients with LSS may also report
* Nocturnal leg cramps (Matsumoto 2009)* Bladder and bowel sx (Inui 2004)* Erectile dysfunction (Gempt 2010)
* Bladder sx particularly common (incomplete emptying, hesitancy, incontinence, nocturia and UTI – be specific when questioning pt
* Reporting of these sx may be vague and inconsistent due to grumbling nature, and pt may think they’re irrelevant as they are ‘age related’ changes
* 57% of >70s have moderate to severe urinary sx with no CES (Lieberman 2018)
CES in older patients
* MRI is gold standard, however sensitivity is HIGH (96%) but specificity is not (68%) for diagnosing LSS (Wassenaar 2012)
* Symptoms and disability correlate poorly with severity of changes seen on MRI (Lurie and Tompkins 2016)
* Weak correlation between severity of stenosis on MRI and bladder dysfunction (Tsai 2010)
* Bladder scan may be of value, but unclear (Venkatesan 2019)
CES in older patients
* Mx is challenging, but as a rule, no urgent need to treat* Monitoring is best as sx may wax and wane over time* Full blown CES is rare in this group
* Do not treat unless new or progressing sx of CES
* Safety netting is important with instructions to seek urgent advice if sx change
CES in older patients
* Plethora of complexities surrounding reliable CES detection from clinical assessment
* The importance and depth of skilled subjective assessment in the screening and exploration of potential red flags in CES cannot be underestimated in clinical practice
* Red flags in LBP should always be taken seriously. * CES is highly litigious condition with delayed diagnosis
causing significant disability and medical costs (£400m/3yrs)
Conclusion
Conclusion
vs