Embed Size (px)
Citation preview

Shepherd Center:A Catastrophic Care Hospital
The Jane Woodruff Pavilion

Acute Management of SCI&
Prevention of Secondary Complications
Joycelyn Craig, BSN, RN, CRRN
SCI Nurse Education Manager

FACTS & STATISTICSModel SCI Care System Data, Archives of Physical and Medical Rehabilitation, January 2008
PREVALENCE in US
• 227,080 - 300,938 living with SCI
• 12,000 annually
AGE
• 24% are between the ages of 16-30
• 55% are between the ages of 31-45
• 11.5% are older than 60
GENDER
• 77.8% are males

Model Systems• National SCI database
– NSCI Statistical Center
– www.spinalcord.uab.edu
• Independent and collaborative research
• Resources to individuals with SCI, family and caregivers, health care professionals and the general public– www.shepherd.org
– www.pva.org

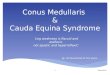
SPINAL CORD INJURY
An injury to the
spinal cord at any
level between the
foramen magnum
and the cauda
equina, from any
cause.

CERVICAL: 7 Bones-8 Nerves

Cervical NervesC1
C2
C3
C4
C5
C6
C7
C8
Neck
Shoulder Shrug,
Neck, Diaphragm
Shoulder Muscles
Front Arm Muscles
Wrist Muscles,
Shoulder Muscles
Lower Arms, Fingers

THORACIC: 12 Bones-12 Nerves

Thoracic Nerves
T1
T2 thru T6
T7 thru T12
Hand
Middle part of the
body (trunk), chest
and stomach area
Coughing and
laughing muscles

LUMBAR: 5 Bones-5 Nerves

Lumbar
L1
L2
L3
L4
L5
Hips
Knees
Top of Foot and
Ankle

SACRAL: 1 Bone-5 Nerves

SacralS1
S2
S3
S4
S5
Legs
Feet
Bowel & Bladder
Sex Organs

CLASSIFICATION of SCI
ASIA• A – E
• most widely accepted
• “neurologic” basis

ASIA CLASSIFICATIONS
ASIA A = no motor or sensory function is preserved in the sacral segments S4-S5.
ASIA B = sensory but not motor function is preserved below the neurological level and includes the sacral segments S4-S5
ASIA C = motor is preserved below the neurological level, and most of the key muscles below the neuro level have a muscle grade < 3.
ASIA D = motor function is preserved below the neurological level, and at least half of key muscles below the neurological level have a muscle grade =or > 3.
ASIA E = NORMAL motor and sensory testing.

CLASSIFICATION of SCI
• Complete SCI = no motor or sensory
function below the LOI.
• Incomplete SCI = any sensation present
and/or any motor function below the LOI.

INCOMPLETE SYNDROMES• Brown-Sequard
• Central Cord
• Anterior Cord
• Posterior Cord
• Conus Medullaris
• Cauda Equina
• Mixed (combination of 2 of above)

INCOMPLETE SYNDROMES
Brown Sequard: damage to one side of cord– ipsilateral
paralysis, loss proprioception
– contralateral loss of pain and temperature

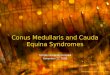
INCOMPLETE SYNDROMES
Central cord:
damage to central
part of cord
– greater weakness
in arms verses legs
– sacral sensation

INCOMPLETE SYNDROMES
POSTERIOR
CORDLesion within
posterior 1/3 of cord
Sensory and motor function intact
Loss of proprioception
ANTERIOR
CORDLesion within
anterior 2/3 of cord
Paralysis with loss of pain and temperature
Proprioception intact

MECHANISM OF INJURY
The CNS, of which the spinal cord is a part, is
extremely fragile.
Even slight pressure on the spinal cord from
the primary injury or from the secondary
injury in the form of swelling or infection or
bruising, can result in permanent and severe
neurologic injury.

Spinal Cord

Nursing
• Prevention of Secondary Injury
• Spinal stabilization
• Proactive Prevention of Medical Complications

FIRST ---Immobilize
THEN-Assess & Test

Within 3 hours of the injury:
• Solumedrol 30 mg/kg IV as a bolus dose
• over 15-60 minutes, then 5.4 mg/kg/hr for 23-24 hours.
Within 8 hours of the injury:
• Solumedrol 30 mg/kg IV as a bolus dose over 15-60 minutes, then 5.4 mg/kg/hr for 47-48 hours.
• Monitor blood glucose
High Dose Solumedrol Protocol

Spinal Stabilization
Goals:
• Prevent further damage to the spinal cord.
• Provide means for early mobilization.

Cervical Traction: Gardner-Wells Tongs• Proper alignment until surgery.
• Constant traction force at all times. Ensure that weights hang freely.
• Pin-site care with soap and water every shift.
• Log rolls

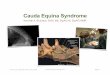
Halo Vest
• A device that is used for unstable cervical injuries that are in alignment.
• Skin care.
• Patient safety.

Cervical Fusion and Wiring• Anterior and/or Posterior Fusion
• Hard collar to be worn at all times
• post-op, for 6 weeks.
• Skin.

Harrington Rods• For thoracic-lumbar injuries.
• Embedded in the neural arch to provide a distraction force.
• TLSO post operatively for 4-6 weeks.
• Skin.

Rehab Priorities 1st 72 Hours
• Spinal Shock
• Respiratory Intervention
• Skin Protection
• Bowel Function
• Bladder Health
• Early Mobilization

Spinal Shock
• Occurs 30-60 minutes post traumatic SCI
• Can last a few hours to several weeks
• Flaccid paralysis
• Absence of all spinal reflexes below the level of injury.
• Loss of pain, touch, temperature, and pressure.
• Loss of bowel & bladder function.

Spinal Shock
• Bowel-– Initiate suppository and manual evacuation within
24-48 hours.
– Daily bowel program.
– Skin care.
• Bladder-– Foley.
– Perineal skin care.

SKIN• Bed
• Padding & Positioning
• Shearing
• Spasms
• Bony prominences
• Visualize new areas
• Head-to-toe assessments
• Pressure relief
• Turns
• Weight Shifts

EVERY PatientDeserves Their Turn!
• Evaluate to increase 30 min/week
• Skin checks at least twice per shift
• Keep pressure off affected areas

Padding and Positioning
• Protect the skin
• Prevent contractures
• Prevent painful shoulders
• Decrease respiratory complications

Autonomic Nervous System
• ANS Dysfunction
• ANS disruption makes the parasympathetic system dominant.

ANS Dysfunction
• Bradycardia
• Hypotension
• Pneumonia/ Atelactasis
• DVT
• Stress Ulcers/ GI Bleed
• Poikilothermism
• Autonomic Dysreflexia
• Bowel
• Bladder
• Skin

ANS Dysfunction
Bradycardia
• Already decreased due to parasympathetic dominance--the absence of the inhibiting effects of the sympathetic system
• Often due to vagus nerve stimulation
• Can be extreme:– Pre-medicate prior to suctioning
– Pacemaker

ANS Dysfunction
Hypotension
• Parasympathetic dominance resulting in vasodilation.
• Vasoconstrictive therapy: – Dopamine
– Neosynephrine
– Florinef
– Midodrine

ANS DysfunctionPneumonia/Atelectasis
• Leading cause of death in SCI population.
• PS—mucus production increases; bronchial constriction
• Result of immobilization, artificial ventilation, and general anesthesia.
• Interventions:
– Aggressive pulmonary toiletry
– Bronchodilator therapy

ANS DysfunctionDVT/PE
• Result of increased platelet aggregation and common post-op complication
• Intervention:
– Continuous Assessment
– Early Detection
– Prophylactic anticoagulants

ANS DysfunctionGI• PS-increased gastric secretions, motility,
digestion• Gastroduodenal ulcers; GI bleeding• Disruption of CNS, stress response, abdominal
trauma• Interventions:
– Initiate proper delivery of nutrition– Prophylactic meds

ANS DysfunctionPoikilothermism
• Interruption of sympathetic pathways to hypothalamus.
• Loss of sympathetic response below level of injury resulting in the inability to shiver or perspire.
• Warming or cooling blankets.

Temperature control
• NO vasoconstriction, piloerection or heat loss through sweating below level of injury
• Do not over cool or over heat.

ANS Dysfunction
Autonomic Dysreflexia
• Life-threatening.
• Inappropriate reflex action, occurring with injury levels T6 and above.
• Noxious stimuli: distended bladder, full rectal vault, skin issue, infection, ingrown toenail.

ANS Dysfunction
Autonomic Dysreflexia
• S & Sx
– Pounding headache
– BP > 15mm Hg over baseline
– Sweating
– Blotchy/skin redness above LOI
– Nasal congestion

ANS Dysfunction
Autonomic Dysreflexia
• Interventions:– Elevate HOB to 90 degrees
– Remove constrictions: binder, TED hose, etc.
– Assess foley for drainage problems
– Bowel program with nupercaine
– Skin issues

ANS Dysfunction
Autonomic Dysreflexia
• Monitor time
• Monitor BP
• Treat BP-procardia
• Notify MD
• Continue to search for cause
• Monitor BP

ANS DysfunctionBOWEL
• Stool continues to be produced; not evacuated.
• Suppository and rectal clearing.
• Monitor results.
• Consider contrast materials used.
• Skin at risk.

ANS Dysfunction
BLADDER
• Neurogenic Bladder management
• Prevent overdistention, ureterovisical reflux.
• Skin at risk.

ANS Dysfunction
SKIN
• Turns, no less than every 2 hours.
• Visualize new areas with every turn.
• Head-to-toe assessments.

Other Issues to Address
• Impaired physical mobility
• Altered nutrition
• Sexual dysfunction
• Risk or injury r/t sensory deficits
• Altered family processes
• Risk for ineffective individual coping
• Body image disturbance
• Grief, guilt, depression

Family Involvement
Directly related to degree of successful discharge and life planning.
Teach family & caregivers all aspects of care.

Help me be ready for rehab• Prevent skin issues
• Prevent respiratory complications
• Reduce secondary complications
• Anticipate discharge
• Involve the family
• Educate & Explain
• Establish B & B regime

Questions?