Embed Size (px)
Citation preview

Recovery: Recovery: The Experience and the The Experience and the
EvidenceEvidenceby Patricia E. Deegan, Ph.D.by Patricia E. Deegan, Ph.D.
http://www.patdeegan.comhttp://www.patdeegan.com
Pat Deegan PhD & Associates, LLC © 2003

Pat
Family
Friends
Values&Beliefs
Spirituality
Class Politics
Wo
rk
Cul
ture
SexualityHopes&Dreams
How I am Seen By Others And Understand Myself
Before Being Diagnosed with Mental Illness

MentalIllness
Spirituality HopesandDreams
Work
Beliefs &Values
FriendsCulture
Sexuality
How I am Seen By Others After Being Diagnosed With Mental Illness

Some of My Recovery Some of My Recovery StrategiesStrategies
No street drugsNo street drugs
Tolerant environmentTolerant environment
Relationships with people who Relationships with people who cared about me and who I cared forcared about me and who I cared for
Spirituality and finding meaning in Spirituality and finding meaning in my sufferingmy suffering

Some of My Recovery Some of My Recovery StrategiesStrategies
A sense of purpose and A sense of purpose and direction; daring to have a dreamdirection; daring to have a dream
RoutineRoutine
Day at a time, hour at a time, Day at a time, hour at a time,
minutes at a timeminutes at a time
Study, learn and workStudy, learn and work

Recovery Strategies (cont’d)Recovery Strategies (cont’d)
A willingness to do psychotherapy to work A willingness to do psychotherapy to work through trauma historythrough trauma history
Meeting others in recovery and learning Meeting others in recovery and learning not to be ashamednot to be ashamed
Some of My Self-Care Some of My Self-Care StrategiesStrategies
How to avoid delusional thinkingHow to avoid delusional thinking How to cope with voicesHow to cope with voices How to cope with anxietyHow to cope with anxiety How to rest, pace myself, sleepHow to rest, pace myself, sleep The importance of physical exerciseThe importance of physical exercise Prayer, meditationPrayer, meditation Sensory dietSensory diet

Using your own voiceUsing your own voiceSome research suggests that using your own Some research suggests that using your own voice can make distressing voices go away.voice can make distressing voices go away.
Possible techniques include:Possible techniques include: speaking to someone when voices start upspeaking to someone when voices start up humming or singing quietly to yourselfhumming or singing quietly to yourself counting under your breathcounting under your breath repeating a mantra to yourself such as repeating a mantra to yourself such as I am I am safe, I am okaysafe, I am okay reading out loudreading out loud

Using EarplugsUsing Earplugs
Some people have found that using an earplug in one ear Some people have found that using an earplug in one ear can greatly reduce or eliminate distressing voices.can greatly reduce or eliminate distressing voices.
In this technique you will need an earplug. They can be In this technique you will need an earplug. They can be purchased at the drugstore.purchased at the drugstore.
Each time the voices start up, put earplug in left ear. See Each time the voices start up, put earplug in left ear. See what happens. Sometimes the voices stop altogether. what happens. Sometimes the voices stop altogether. Sometimes they stop only when you take the earplug out. Sometimes they stop only when you take the earplug out. Sometimes you have to try the earplug in your right ear. Sometimes you have to try the earplug in your right ear.

Using EarplugsUsing Earplugs(continued)(continued)
You will have to experiment with this You will have to experiment with this technique to see what works for you. You technique to see what works for you. You may have to keep trying for a week or more may have to keep trying for a week or more in order to get results. The good news is that in order to get results. The good news is that in some studies, over half the people who in some studies, over half the people who tried this got some relief, and for several tried this got some relief, and for several people the voices disappeared completely for people the voices disappeared completely for several months.several months.

Listening to Listening to HeadphonesHeadphones
Listening to talk or music through headphones can bring Listening to talk or music through headphones can bring temporary relief.temporary relief.
The key to this technique is not how loud you play the The key to this technique is not how loud you play the music, but that you really like the music and actively music, but that you really like the music and actively listen to it.listen to it.
Be Creative! Try listening to a sports broadcast or radio Be Creative! Try listening to a sports broadcast or radio talk show. Some people have made tapes in which they talk show. Some people have made tapes in which they describe really happy places and events in theirs lives.describe really happy places and events in theirs lives.

IMMEDIATE EFFECTIVENESS AND IMMEDIATE EFFECTIVENESS AND LONG TERM USE OF TREATMENT IN LONG TERM USE OF TREATMENT IN
20 CASES20 CASES One or
More Treatment
Ear Plug Subvocal Counting
Tape Player
Patients Attempting Treatment
17 8 13 15
Patients reporting some immediate beneficial effects
16 8 5 14
Patients using treatment long term
11 4 2 7
Nelson, H.E., Thraser, S., Barnes, T.R.E.
British Journal of Medicine
1991, 302, p.327

92 research participants diagnosed with schizophrenia reported 350 individual coping techniques in addition to the 57 strategies that they were asked to rate
• Passive diversion(listening to music)
• Activity(walking)
• Decreasesocialization(being alone)
• Active diversion(playing aninstrument)
• Inactivity(waiting)
• Shifting attention(think aboutsomething else)
• Change ofenvironment(van ride)
• Postural changes(lying down)
• Problem solving
• Increasesocialization(phone call)
• Suppressionof ideas

““From the foregoing it should appear obvious that From the foregoing it should appear obvious that schizophrenic patients are not simply passive victims of their schizophrenic patients are not simply passive victims of their illness.illness.
On the contrary…patients can play an active role in the On the contrary…patients can play an active role in the management of their illness, particularly in the containment of management of their illness, particularly in the containment of its symptoms.its symptoms.
The experience of schizophrenia is evidently a learning The experience of schizophrenia is evidently a learning process in which patients make active attempts to master the process in which patients make active attempts to master the illness and not have it dominate them.”illness and not have it dominate them.”
Vaughn Carr (1988). Patients’ techniques for coping with Vaughn Carr (1988). Patients’ techniques for coping with schizophrenia: An exploratory study. schizophrenia: An exploratory study. British Journal of British Journal of
Medical PsychologyMedical Psychology, 61, 339-352., 61, 339-352.

RecoveryRecovery
A new vision of people as active subjects A new vision of people as active subjects as opposed to passively afflicted objectsas opposed to passively afflicted objects
A self-directed process of healing and A self-directed process of healing and transformationtransformation

Some of My Recovery Some of My Recovery StrategiesStrategies(continued)(continued)
A willingness to take responsibility A willingness to take responsibility for myself and accepting that no one for myself and accepting that no one could do the work of recovery for mecould do the work of recovery for me

The Restitution The Restitution NarrativeNarrative
I was wellI was well I got sickI got sick I sought I sought
professional helpprofessional help I followed I followed
professional adviceprofessional advice I got wellI got well I am back to I am back to
myselfmyself

The Recovery NarrativeThe Recovery Narrative I was well, I got sick, the I was well, I got sick, the
professionals did not professionals did not make me bettermake me better
What do I do now?What do I do now? I can’t go back to who I I can’t go back to who I
once was. Who can I be once was. Who can I be and what can I do?and what can I do?
Transformation of self Transformation of self and discovery of valued and discovery of valued social roles.social roles.
A testament to the A testament to the resilient, struggling selfresilient, struggling self

The Disease Centered ModelThe Disease Centered Model
Professional RoleProfessional Role
1.1. HierarchicalHierarchical
2.2. PaternalPaternal
3.3. In-chargeIn-charge
4.4. Holds the important Holds the important knowledgeknowledge
5.5. Responsible for Responsible for treatmenttreatment
6.6. Disease is focusDisease is focus
Patient RolePatient Role
1.1. SubservientSubservient
2.2. ObedientObedient
3.3. PassivePassive
4.4. Recipient of Recipient of knowledgeknowledge
5.5. Responsible for Responsible for following treatmentfollowing treatment
6.6. Host of diseaseHost of disease
Recovery is Person-Centered Recovery is Person-Centered ModelModel
Professional RoleProfessional Role1.1. Power sharingPower sharing2.2. Exchange Exchange
informationinformation3.3. Shared decision-Shared decision-
makingmaking4.4. Co-investigatorCo-investigator5.5. Professional is Professional is
expert consultant on expert consultant on journeyjourney
Person’s RolePerson’s Role1.1. Personal powerPersonal power2.2. Personal Personal
knowledgeknowledge3.3. Personal Personal
responsibilityresponsibility4.4. Person in context Person in context
of life is focusof life is focus5.5. Person is self-Person is self-
determiningdetermining

Recovery Oriented Recovery Oriented PracticePractice
Recognize and end macro and micro-Recognize and end macro and micro-aggression aggression Handcuffed in back of cruisersHandcuffed in back of cruisers Restraint seclusionRestraint seclusion Threats, bribes and coercion Threats, bribes and coercion
Build respectful relationshipsBuild respectful relationships A new approach to establishing professional A new approach to establishing professional
boundariesboundaries A new approach to communication with clients A new approach to communication with clients
both in writing, speaking, and non-verbal formsboth in writing, speaking, and non-verbal forms Support client choice through shared decision Support client choice through shared decision
makingmaking
Pat
Family
Friends
Sexuality
Spirituality
Class Po
litics
Wo
rk
Cul
ture
Hopes&Dreams
Recovery: I am a Person, Not an Illness
Vulnerabilities
M. Bleuler StudyM. Bleuler Study
Sample size: 208 peopleSample size: 208 people Average length of follow-up: 23 yearsAverage length of follow-up: 23 years Rates of significant improvement or Rates of significant improvement or
recovery for schizophrenia:recovery for schizophrenia: 53%53% for multiple admission sample for multiple admission sample 68%68% for first admission sample for first admission sampleEnglish translation of the 1972 study: S.M. Clemens (1978) English translation of the 1972 study: S.M. Clemens (1978) The The
Schizophrenic Disorders: Long-term Patient and Family Studies.Schizophrenic Disorders: Long-term Patient and Family Studies. New Haven, CT: yale University PressNew Haven, CT: yale University Press

Huber et al. StudyHuber et al. Study
Sample size: 502 peopleSample size: 502 people Average length of follow-up: 22 yearsAverage length of follow-up: 22 years Rates of significant improvement or Rates of significant improvement or
recovery for schizophrenia:recovery for schizophrenia: 57%57%
Huber, G., Gross, G., & Schüttler, R. (1979). Huber, G., Gross, G., & Schüttler, R. (1979). Schizophrenie: Verlaufs Schizophrenie: Verlaufs und sozialpsychiatrische Langzeit unter suchü an den 1945 bis und sozialpsychiatrische Langzeit unter suchü an den 1945 bis 1959 in Bonn hospitaliisierten schizophrenen Kranken. 1959 in Bonn hospitaliisierten schizophrenen Kranken. Monographien aus dem Gesamtgebiete der Psychiatrie. Bd. 21. Monographien aus dem Gesamtgebiete der Psychiatrie. Bd. 21. Berlin: Springer:Verlag.Berlin: Springer:Verlag.

Ciompi & Müller StudyCiompi & Müller Study
Sample size: 289Sample size: 289 Average length of follow-up: 37 yearsAverage length of follow-up: 37 years Rates of significant improvement or Rates of significant improvement or
recovery:recovery: 53%53%
Ciompi, L. & Müller,C. (1976). Ciompi, L. & Müller,C. (1976). Lebensweg und Alter der Lebensweg und Alter der Schizophrenen: Eine katanmnestische Longzeitstudie bis ins Schizophrenen: Eine katanmnestische Longzeitstudie bis ins senium.senium. Berlin: Spring-Verlag Berlin: Spring-Verlag
Ciompi, L. (1980). Catamnestic long-term study on the course of life Ciompi, L. (1980). Catamnestic long-term study on the course of life and aging in schizophrenics. and aging in schizophrenics. Schizohrenia Bulletin,6Schizohrenia Bulletin,6(4), 606-618.(4), 606-618.

Tsuang et al. StudyTsuang et al. Study
Sample size: 186Sample size: 186 Average length of follow-up: 35 yearsAverage length of follow-up: 35 years Rates of significant improvement or Rates of significant improvement or
recovery for schizophrenia:recovery for schizophrenia: 46%46%
Tsuang, M.T., Woolson, R.F., & Fleming, J.A. (1979). Long-term Tsuang, M.T., Woolson, R.F., & Fleming, J.A. (1979). Long-term outcome of major psychoses: 1. Schizophrenia and affective outcome of major psychoses: 1. Schizophrenia and affective disorders compared with psychiatrically symptom-free surgical disorders compared with psychiatrically symptom-free surgical conditions. conditions. Archives of General Psychiatry, 36Archives of General Psychiatry, 36, 1295-1301., 1295-1301.

Harding et al. StudyHarding et al. Study Sample size: 269Sample size: 269 Average length of follow-up: 32 yearsAverage length of follow-up: 32 years Rates of significant improvement or Rates of significant improvement or
recovery for schizophrenia:recovery for schizophrenia: 62-68%62-68%
Harding, C.M., Brooks, G.W., Ashikaga, T., Strauss, J.S., & Breier, A. (1987). The Harding, C.M., Brooks, G.W., Ashikaga, T., Strauss, J.S., & Breier, A. (1987). The Vermont longitudinal study of persons with severe mental illness: 1. Vermont longitudinal study of persons with severe mental illness: 1. methodology, study, sample, and overall status 32 years later. methodology, study, sample, and overall status 32 years later. American Journal American Journal of Psychiatry,of Psychiatry, 144(6), 718-726. 144(6), 718-726.
Harding, C.M., Brooks, G.W., Ashikaa, T., Strauss, J.S., & Breier, A. (1987). The Harding, C.M., Brooks, G.W., Ashikaa, T., Strauss, J.S., & Breier, A. (1987). The Vermont longitudinal study: II. Long-term outcome of subjects who Vermont longitudinal study: II. Long-term outcome of subjects who retrospectively met the criteria for DSM-III schizophrenia. retrospectively met the criteria for DSM-III schizophrenia. American Journal of American Journal of Psychiatry, Psychiatry, 144(6), 727-735.144(6), 727-735.

Ogawa et al. StudyOgawa et al. Study
Sample size: 140Sample size: 140 Average length of follow-up: 22.5 yearsAverage length of follow-up: 22.5 years Rates of significant improvement or Rates of significant improvement or
recovery for schizophrenia:recovery for schizophrenia: 57%57%
Ogawa, K, Miya, M., Watarai, A., Nakazawa, M., Yuasa, S. & Utena, H. Ogawa, K, Miya, M., Watarai, A., Nakazawa, M., Yuasa, S. & Utena, H. (1987). A long-term follow-up study of schizophrenia in Japan with (1987). A long-term follow-up study of schizophrenia in Japan with special reference to the course of social adjustment. special reference to the course of social adjustment. British Journal British Journal of Psychiatry, 151of Psychiatry, 151, 758-765., 758-765.

DeSisto et al. 1995DeSisto et al. 1995
Sample size: 269Sample size: 269 Average length of follow-up: 35 yearsAverage length of follow-up: 35 years Rates of significant improvement or recovery Rates of significant improvement or recovery
for schizophrenia:for schizophrenia: 49%49%
DeSisto, M., Harding, C.M., Ashikaga, T., McCormick, R., & DeSisto, M., Harding, C.M., Ashikaga, T., McCormick, R., & Brooks, G.W. (1995). The Maine and Vermont three-decade Brooks, G.W. (1995). The Maine and Vermont three-decade studies of serious mental illness: Matched comparison of studies of serious mental illness: Matched comparison of cross-sectional outcome. cross-sectional outcome. British Journal of Psychiatry, 167British Journal of Psychiatry, 167, , 338-342.338-342.
DeSisto, M., Harding, C.M., Ashikaga, T., McCormick, R., & DeSisto, M., Harding, C.M., Ashikaga, T., McCormick, R., & Brooks, G.W. (1995). The Maine and Vermont three decade Brooks, G.W. (1995). The Maine and Vermont three decade studies of serious mental illness: II. Longitudinal course studies of serious mental illness: II. Longitudinal course comparisons. comparisons. British Journal of Psychiatry, 167, British Journal of Psychiatry, 167, 338-342.338-342.
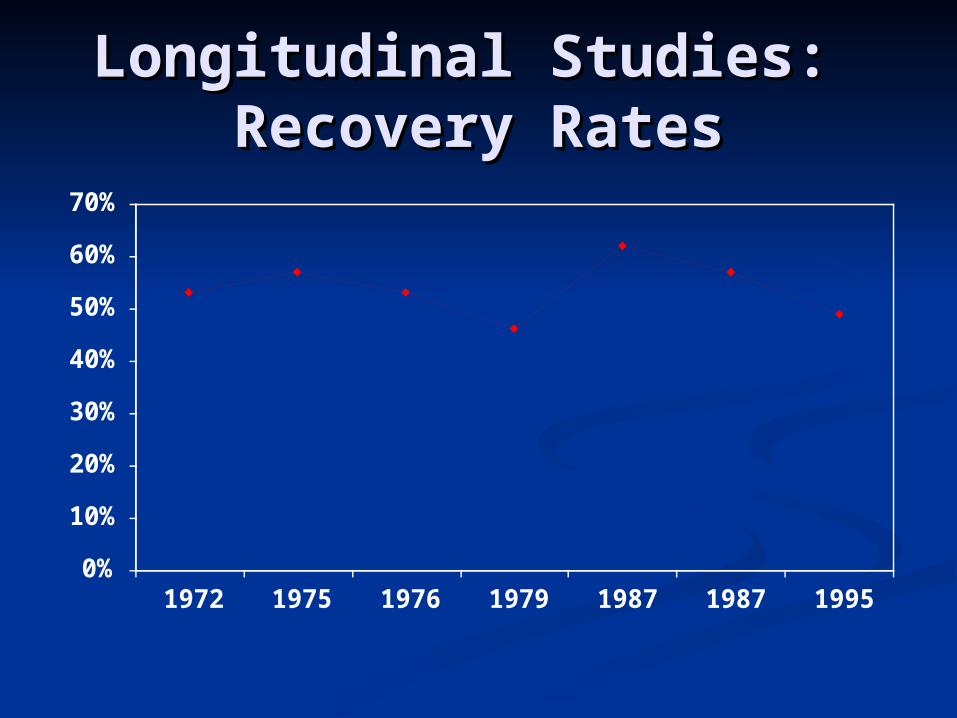
Longitudinal Studies: Longitudinal Studies: Recovery RatesRecovery Rates
0%
10%
20%
30%
40%
50%
60%
70%
1972 1975 1976 1979 1987 1987 1995

Ogawa et al. Study: What was Ogawa et al. Study: What was the outcome for 140 people the outcome for 140 people
diagnosed with schizophrenia?diagnosed with schizophrenia? 74% were “self-supportive in terms 74% were “self-supportive in terms of occupational status.of occupational status. 45% were married.45% were married. 52% lived in their homes.52% lived in their homes. 66% still used psychiatric services.66% still used psychiatric services.

Ogawa et al. Study: What was Ogawa et al. Study: What was the outcome for 140 people the outcome for 140 people
diagnosed with schizophrenia?diagnosed with schizophrenia?47% self supported defined as:47% self supported defined as: Has returned to a level of social Has returned to a level of social functioning similar to that prior to functioning similar to that prior to illnessillness Maintains an independent social Maintains an independent social life with or without asking any advice life with or without asking any advice from psychiatrists or acquaintancesfrom psychiatrists or acquaintancesMaintains a normal family life Maintains a normal family life

Harding et al. 1987 StudyHarding et al. 1987 Study
Study cohort of 269 people diagnosed with Study cohort of 269 people diagnosed with schizophrenia were bottom 19% in schizophrenia were bottom 19% in functional hierarchy at a state hospitalfunctional hierarchy at a state hospital
Most severely ill sample in world literature Most severely ill sample in world literature on recovery to dateon recovery to date Most in hospital 10+ yearsMost in hospital 10+ years Some could not use eating utensilsSome could not use eating utensils Some barely spokeSome barely spoke

Harding et al. 1987 StudyHarding et al. 1987 Study
Recovery defined as four criteria:Recovery defined as four criteria: Having a social life similar to others in the Having a social life similar to others in the
wider communitywider community Holding a paying job or volunteeringHolding a paying job or volunteering Being symptom freeBeing symptom free Being off of psychiatric medicationsBeing off of psychiatric medications
62% of people diagnosed with 62% of people diagnosed with schizophrenia met 3 of the 4 criteriaschizophrenia met 3 of the 4 criteria

Comparison of Vermont Comparison of Vermont and Maine Studiesand Maine Studies
VermontVermont MH system was MH system was
based on based on rehabilitationrehabilitation
Expectation that Expectation that people would people would become self-become self-sufficient and sufficient and workwork
Expectation that Expectation that people would live people would live in “real” housing in “real” housing
MaineMaine MH system was MH system was
based on based on stabilization modelstabilization model
Expectation that Expectation that people would remain people would remain on benefits for life on benefits for life and could not workand could not work
Expectation that Expectation that people needed to be people needed to be monitored/supervisemonitored/supervised in congregate d in congregate housinghousing

Outcomes for Vermont and Outcomes for Vermont and Maine Research Maine Research
ParticipantsParticipantsResidentialResidential
DomainYears with
statistical differenceVermont
(%)Maine
(%)
Hospital 60-76 13.0 50.0
Independent 60-71 46.4 25.6
Halfway House 60-63 6.2 0.3
Boarding Home 63-71 14.4 3.9

Outcomes for Vermont and Outcomes for Vermont and Maine Research Maine Research
ParticipantsParticipantsWorkWork
DomainYears with
statistical differenceVermont
average (%)Maine
average (%)
Full-time 60-75 30.9 12.7
Part-time 60 7.9 1.8
Unemployed 74, 75, 77-79 41.3 60.2

World Health Organization’s World Health Organization’s
International Study of International Study of SchizophreniaSchizophrenia
Recovery from Psychotic Illness:
A 15-25 year international follow-up study.
Harrison, Hopper, Craig, et.al.
British J. of Psychiatry (2001), 178,
p. 506-517

Conclusions and Clinical Conclusions and Clinical ImplicationsImplications
• Striking heterogeneity in the long-term course of schizophrenia challenges conventional notions of chronicity and therapeutic pessimism
• Evidence of late recovery in a significant minority of subjects should encourage innovative rehabilitation and employment programs in those with long-term illness, despite earlier failures.

Recovery RatesRecovery Rates Panic Disorder: 80%Panic Disorder: 80% Major Depression: 65%Major Depression: 65% Obsessive Compulsive Disorder: 60%Obsessive Compulsive Disorder: 60% Bipolar Disorder: 80%Bipolar Disorder: 80%
National Institute of Mental Health Council:National Institute of Mental Health Council:Health Care Reform for Americans With Severe Mental Health Care Reform for Americans With Severe Mental
IllnessIllnessNational Institute of Mental HealthNational Institute of Mental Health
19931993

Using Empirical Data to Offer Using Empirical Data to Offer HopeHope
Long-term studies have consistently found that Long-term studies have consistently found that half to two-thirds of people diagnosed with major half to two-thirds of people diagnosed with major mental illness go on to a significant or complete mental illness go on to a significant or complete recovery. Data shows that even in the second or recovery. Data shows that even in the second or third decade, a person can still go on to a third decade, a person can still go on to a complete recovery. I believe you can be one of complete recovery. I believe you can be one of the ones to recover.the ones to recover.
I am here to support your journey of recovery.I am here to support your journey of recovery.