Embed Size (px)
Citation preview

NhlwpaawAtv15a
Titcvtpdplsfsv
M
warAp�vtova
Fsa
oh
7
Relation of N-Terminal Pro–B-TypeNatriuretic Peptide to Severity of
Valvular Aortic StenosisMichael Weber, MD, Roman Arnold, MD, Matthias Rau, MD, Roland Brandt, MD,
Alexander Berkovitsch, PhD, Veselin Mitrovic, MD, and Christian Hamm, MD
(cpcAfTYAeaA
-terminal pro–B-type natriuretic peptide (NT-proBNP)as been shown to be a reliable biochemical marker for
eft ventricular wall stress and is increased in patientsith aortic stenosis (AS). We evaluated the role of NTro-BNP as a biochemical marker in the diagnosis of ASnd whether it contributes to the optimal timing forortic valve replacement (AVR). Included in this studyere 146 patients who had AS, 31 who underwentVR, and 32 who had “normal valve function” (con-
rols). Increased NT pro-BNP was closely linked to se-erity of AS (mild AS 612 � 151 pg/ml, moderate AS,441 � 32 pg/ml, severe AS 2,579 � 13 pg/ml, AVR93 � 148 pg/ml, controls 140 � 27 pg/ml; p <0,01)nd to New York Heart Association functional class
valaNP)
fNthedrr
tichyA
rtic.
ntserr
ereadionlefin
ruelet bp
tYbatcmcdmafsmHm
wscwwmcavawp3wgvoaeim, Germany. E-mail: [email protected].
40 ©2004 by Excerpta Medica, Inc. All rights reserved.The American Journal of Cardiology Vol. 94 September 15, 2004
class I 601 � 116 pg/ml, class II 1,119 � 216 pg/ml,lass III 1,998 � 459 pg/ml, class IV 5,107 � 1,512g/ml; p <0.01). Area under the receiver-operatingharacteristic curve for NT pro-BNP as a predictor forVR was 0.73. Using an optimized cutoff of 550 pg/ml
or NT-proBNP, the positive predictive value was 85%.hus, NT pro-BNP is linked to severity of AS and Nework Heart Association class and is an indication forVR. Therefore, it is a useful biochemical marker tovaluate severity of AS, monitor disease progression atn early stage, and decide on the optimal time forVR. �2004 by Excerpta Medica, Inc.
(Am J Cardiol 2004;94:740–745)
Newnsasable,
ac-y thecho-teded a
etic
m
hyHzsa-
ionswho
NPg toi-
ternalmaluous-ightoverentsure
Leftula
ce
he few data available for patients who havevular aortic stenosis (AS) have shown that
ncreased level of B-type natriuretic peptide orerminal pro–B-type natriuretic peptide (NT pro-BNorrelates with the mean pressure gradient,1 aorticalve area,2 and functional status.3 The objective ohe present study was to evaluate the role ofro-BNP as a potential biochemical marker iniagnosis of AS. For this reason, we conducterospective observational study to analyze the co
ation of NT pro-BNP to different degrees of aortenotic severity, as assessed by echocardiograpunctional class as assessed by New York Heartociation classification and to the indication for aoalve replacement (AVR) according to guidelines
ETHODSPatients: In this prospective study, 146 patie
ho were referred for further evaluation of degentive AS and 31 patients who were referred foegular follow-up visit after AVR because of sevS for �12 months were included. All patients hreserved left ventricular function (ejection fract45%). In addition, 32 patients who had normal
entricular function were included as controls;hese patients, valvular heart disease had beenut by echocardiography and hemodynamically rant coronary artery disease had been ruled oungiography. In all patients, severity of clinical sym
rom the Kerckhoff Heart Center, Bad Nauheim, Germany. Manu-cript received April 14, 2004; revised manuscript received andccepted May 24, 2004.
Address for reprints: Michael Weber, MD, Department of Cardi-logy, Kerckhoff Heart Center, Benekestraße 2-8, 61231 Bad Nau-
-n-
T
ae-
, tos-
-a
t
led-y
-
oms was assessed and graded according to theork Heart Association classification by physicialinded to NT pro-BNP values. Medical history wssessed based on patients’ reports or, if avail
heir medical records. Patients were categorizedording to aortic stenotic severity as assessed bean transvalvular pressure gradient obtained e
ardiographically. Although no universally accepefinition exists, many investigators have suggestean transvalvular pressure gradient of�50 mm Hgs a criterion for severe AS.4,5 Therefore, we used th
ollowing values for the grading of aortic stenoeverity: a mean transvalvular pressure gradient�30m Hg was considered mild AS (AS I), 30 to 50 mg was considered moderate AS (AS II), and�50m Hg was considered severe AS (AS III).Echocardiography: Transthoracic echocardiograp
as performed with an Agilent Sonos 1.75- to 3.5-Mcanner (Phillips Medical Ultrasound, Andover, Mashusetts) that used harmonic imaging. All examinatere done by an experienced echocardiographeras blinded to the clinical results and NT pro-Beasurements. A complete examination accordin
urrent guidelines6 was performed. Left ventricular dmeter was assessed in M-mode in the left parasiew. Ejection fraction was visually assessed. Maxind mean aortic velocities were assessed by continave Doppler echocardiography from the apical or rarasternal view. Transaortic velocity was averagedcycles in sinus rhythm and over 7 cycles in patiho had atrial fibrillation. Maximum and mean pressradients were calculated with the built-in software.entricular mass was calculated according to the formf Devereux and Reichek7 and indexed to body surfa
rea. In 76 patients who had AS, transesophageal echo-0002-9149/04/$–see front matterdoi:10.1016/j.amjcard.2004.05.055

TABLE 1 Baseline Characteristics
VariableControls(n � 32)
Mean Transvalvular Pressure Gradient (mm Hg)
AVR(n � 31) p Value
�30(n � 26)
30–50(n � 29)
�50(n � 91)
Men/women 19/13 13/13 15/14 46/45 21/10 0.49Age (yrs) 62 (57–63) 71 (65–74) 73 (67–74) 72 (68–72) 69 (66–72) �0.01Creatinine (mg/dl) 0.85 (0.78–0.91) 0.99 (0.90–1.06) 0.98 (0.88–1.06) 0.86 (0.85–0.94) 0.94 (0.87–1.07) 0.05Body mass index (kg/m2) 28.7 (27.4–30) 28.2 (27.5–30.2) 28 (26.9–29.1) 26.8 (26.6–28.1) 26.1 (25.1–27.5) 0.021Episodes of CHF 0 0 3 (10%) 10 (11%) 0 0.01Syncope 0 0 2 (7%) 4 (4%) 0 0.17Atrial fibrillation 0 (0%) 3 (12%) 3 (10%) 13 (14%) 4 (13%) 0.28New York Heart Association class
0/I 10 (31%) 14 (54%) 4 (14%) 10 (11%) 23 (74%)II 14 (44%) 11 (42%) 13 (45%) 30 (33%) 8 (26%) �0.01III 8 (25%) 1 (4%) 8 (28%) 39 (43%) 0IV 0 0 4 (14%) 12 (13%) 0
Coronary artery bypass grafting 0 6 (23%) 1 (3%) 5 (5%) 12 (39%) �0.01Percutaneous coronary intervention 9 (28%) 5 (19%) 1 (3%) 7 (8%) 0 0.04Acute myocardial infarction 5 (16%) 3 (12%) 3 (10)% 5 (5%) 0 0.12Diabetes mellitus 5 (16%) 8 (31%) 4 (14%) 19 (21%) 5 (16%) 0.41Hypertension 25 (78%) 21 (81%) 26 (90%) 61 (67%) 20 (65%) 0.06Smoker 6 (19%) 0 4 (14%) 12 (13%) 4 (13%) 0.27Hyperlipidemia 21 (66%) 15 (58%) 9 (31%) 30 (33%) 15 (48%) 0.07Left ventricular mass (g) 155 (148–202) 205 (180–233) 246 (213–288) 248 (240–271) 188 (168–233) �0.01Left ventricular mass index (g/m2) 81 (72–96) 102 (96–122) 129 (114–152) 133 (128–144) 99 (89–123) �0.01Mean transvalvular gradient (mm Hg) �5 16.5 (14–19) 37 (35–48) 59 (58–59) 14 (13–18) �0.01Peak transvalvular gradient (mm Hg) �10 29 (24–34) 60 (55–76) 94 (91–102) 21 (23–32) �0.01Aortic valvular area (cm2) ND 1.5 (1.1–1.8) 0.9 (0.84–0.96) 0.65 (0.62–0.69) ND �0.01
CHF � congestive heart failure; ND � not determined.
VALVU
LAR
HEA
RTD
ISEASE/
NT
PRO-BN
PFO
RTH
EA
SSESSMEN
TO
FA
ORTIC
STENO
SIS741

ca
pi
TpBiM
sptagccwatccogavmuuofa
R
2
1�1p
Fa
Fpf
Fth
7
ardiography was performed and aortic valve area wasssessed by planimetry.
NT pro-BNP measurement: Venous blood from allatients was taken from an antecubital vein and placedn tubes filled with ethylenediaminetetraacetic acid.
IGURE 1. NT pro-BNP levels according to severity of AS. Valuesre shown as mean � SEM.
IGURE 2. Correlation of NT pro-BNP to the mean transvalvularressure gradient (TPG). Values for NT pro-BNP are log-trans-ormed.
IGURE 3. NT pro-BNP levels according to functional status (Newion [NYHA] class) of the entire study population (black bars) andad severe AS (gray bars). Values are shown as mean � SEM.
t
42 THE AMERICAN JOURNAL OF CARDIOLOGY� VOL. 94
he specimens were centrifuged for �1 hour, andlasma was frozen at �80°C until analysis. NT pro-NP was measured by an electrochemiluminescence
mmunoassay (Elecsys proBNP, Roche Diagnostics,annheim, Germany).Statistical analysis: Values for NT pro-BNP are pre-
ented as mean � SEM. For statistical analysis of NTro-BNP values, the Mann-Whitney test (2 groups) andhe Kruskal-Wallis test (n groups) were used. For thenalysis of patients’ baseline characteristics, a t test (2roups) or analysis of variance (n groups) was used forontinuous variables and a chi-square test was used forategorical variables. Multivariate regression analysisas performed to evaluate the relation of the variables of
ge, gender, creatinine, body mass index, ejection frac-ion, left ventricular mass, New York Heart Associationlass, and NT pro-BNP to severity of AS. Pearson’sorrelation coefficient was calculated for the associationf logarithmically transferred NT pro-BNP to pressureradient and to left ventricular mass index and for thessociation of left ventricular mass index to mean trans-alvular pressure gradient. To evaluate the test perfor-ance of NT pro-BNP as a predictor of AVR, the area
nder the receiver-operating characteristic curve wassed. An optimal cut-off level was derived from analysesf the receiver-operating characteristic curve. SPSS 10.0or Windows (SPSS, Inc., Chicago, Illinois) was used forll statistical analyses.
ESULTSAccording to the previously described definition,
6 patients were classified as having mild AS (AS I),29 patients as having moderate AS(AS II), and 91 patients as havingsevere AS (AS III). Thirty-one pa-tients had AVR, and 32 patientsserved as controls. Patients’ detailedbaseline characteristics are listed inTable 1. There was no differenceacross groups with respect to gender.The controls were younger, but therewas no difference among patientswith different severities of AS withrespect to age. Patients with severeAS were in a higher New York HeartAssociation class and had more fre-quent episodes of congestive heartfailure. There were no differences incardiovascular risk factors. Renalfunction, measured by serum creati-nine, was normal in most patients butdecreased (serum creatinine �106�mol/L) in 18 patients, with a max-imum of 150 �mol/L.
NT pro-BNP was higher in patientswho had aortic valvular disease than incontrols (AS I 612 � 151 pg/ml, AS II
,441 � 32 pg/ml, AS III 2,579 � 13 pg/ml; AVR 593148 pg/ml, controls 140 � 27 pg/ml; p �0.01; Figure
), with a positive correlation to a mean transvalvularressure gradient (r � 0.39, p �0.01; Figure 2) and peak
k Heart Associa-atients who
Yorof p
ransvalvular pressure gradient (r � 0.04, p �0.01).
SEPTEMBER 15, 2004

mAHN(cps1Iewt
av
Httti(At
tvsAchtstA22
s
w1wpa3h2
vags(
Fa
Fs
Patients who had severe AS and those who hadild or moderate AS were in higher New York Heartssociation classes (chi-square �0.01; Table 1).igher NT pro-BNP levels were closely linked toew York Heart Association class in all patients
class I 601 � 116 pg/ml, class II 1,119 � 216 pg/ml,lass III 1,998 � 459 pg/ml, class IV 5,107 � 1,512g/ml; p �0.01) and in patients whose AS was clas-ified as severe (class I 1,467 � 395 pg/ml, class II,793 � 459 pg/ml, class III 2,641 � 628 pg/ml, classV 5,273 � 1,936 pg/ml; p �0.05; Figure 3). How-ver, there was no difference in NT pro-BNP levelsith respect to duration (�6 or �6 months) of symp-
oms (1,810 � 287 vs 1,626 � 337 pg/ml; p � 0.67).In a multivariate regression analysis, we included
ge, creatinine, body mass index, ejection fraction, left
IGURE 4. Receiver-operating characteristic curve of sensitivitynd specificity for NT pro-BNP to predict an indication for AVR.
IGURE 5. NT pro-BNP levels with respect to gender and severityhown as mean � SEM.
entricular mass index, gender, rhythm, New York F
VALVULAR HEART DISEASE/N
eart Association class, and NT pro-BNP level. Inhis analysis, NT pro-BNP was independently relatedo severity of AS, as were New York Heart Associa-ion class, left ventricular mass index, body massndex, and ejection fraction. However, NT pro-BNPchi-square 33.25, p �0.01) and New York Heartssociation class (chi-square 54.10, p �0.01) were
he strongest predictors for severe AS.In 105 patients, valvular surgery was proposed by the
reating physician who was blinded to NT pro-BNPalues, and 84 of these patients fulfilled the criterion forurgical AVR according to recommendations of themerican College of Cardiology/American Heart Asso-
iation Task Force Report.8 NT pro-BNP levels wereigh in patients who had been recommended for surgicalherapy (surgery recommended 2,485 � 371 pg/ml andurgery not recommended 768 � 186 pg/ml, respec-ively; p �0.01) and in patients who had an indication forVR according to the guidelines (surgery indicated,677 � 459 pg/ml and surgery not indicated 1,090 �14 pg/ml, respectively; p �0.01). Analysis of the re-
ceiver-operating characteristic curvefor NT pro-BNP as a predictor for theindication of AVR showed an area un-der the curve of 0.73 (95% confidenceinterval 0.636 to 0.814, p �0.001; Fig-ure 4). Using an optimized cut-offlevel of 550 pg/ml derived from thereceiver-operating characteristic curvefor NT pro-BNP as a predictor for theindication of surgical AVR, sensitivitywas 71%, specificity was 68%, posi-tive predictive value was 85%, andnegative predictive value was 48%,with a total test efficiency of 71%.
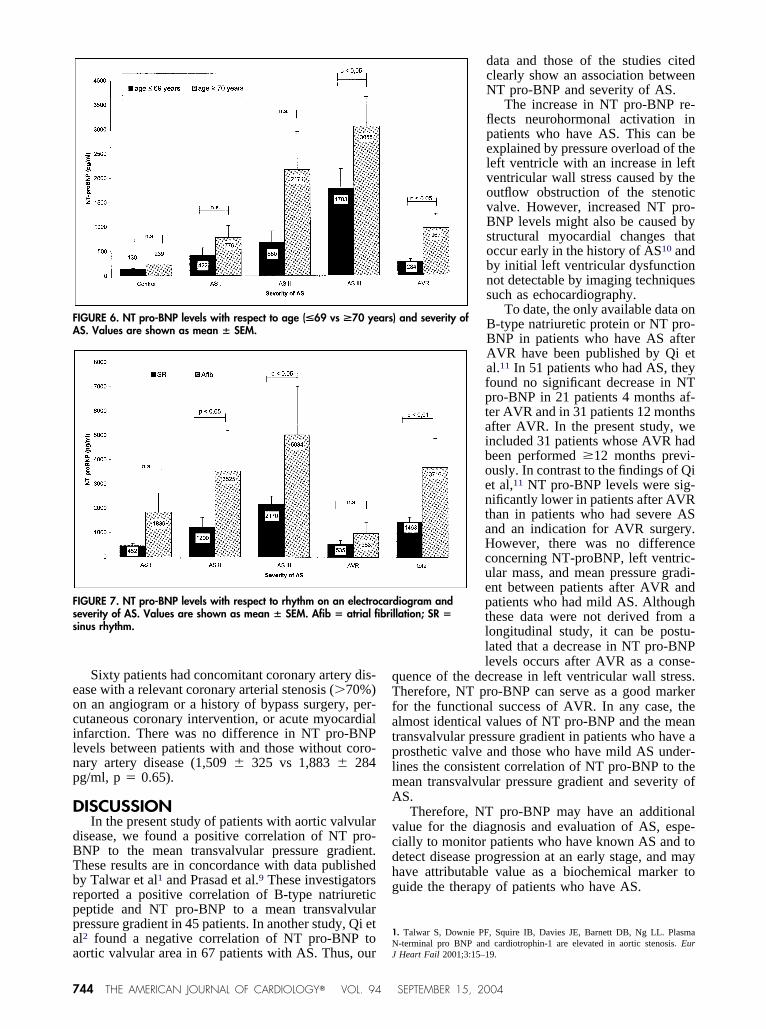
NT pro-BNP levels tended to behigher in women than in men, with-out a statistically significant differ-ence (1,852 vs 1,221 pg/ml; p �0.59), and were significantly higherin older patients (median age �69years; 2,251 � 369 vs 792 � 152pg/ml, p �0.01). The tendency to-ward a higher level of NT pro-BNPin older patients was present in all
ubgroups (Figures 5 and 6).Eighty-nine patients who had AS were pretreated
ith an angiotensin-converting enzyme inhibitor and14 patients were pretreated with a � blocker. Thereas no difference in NT pro-BNP levels betweenatients who had been treated with or without anngiotensin-converting enzyme inhibitor (1,534 �50 vs 1,489 � 242 pg/ml, p � 0.51) and those whoad been treated with or without a � blocker (1,554 �54 vs 1,454 � 328 pg/ml, p � 0.44).
Twenty-three of 177 patients who had aortic val-ular disease (AS and AVR) were in atrial fibrillationnd were distributed equally among the different sub-roups. In these patients, NT pro-BNP levels wereignificantly higher than in patients in sinus rhythm3,716 � 1,185 vs 1,463 � 197 pg/ml, p �0.01;
S. Values are
of Aigure 7).
T PRO-BNP FOR THE ASSESSMENT OF AORTIC STENOSIS 743
eocilnp
D
dBTbrppaa
qTfatplmA
vcdhg
1N
FA
Fss
7
Sixty patients had concomitant coronary artery dis-ase with a relevant coronary arterial stenosis (�70%)n an angiogram or a history of bypass surgery, per-utaneous coronary intervention, or acute myocardialnfarction. There was no difference in NT pro-BNPevels between patients with and those without coro-ary artery disease (1,509 � 325 vs 1,883 � 284g/ml, p � 0.65).
ISCUSSIONIn the present study of patients with aortic valvular
isease, we found a positive correlation of NT pro-NP to the mean transvalvular pressure gradient.hese results are in concordance with data publishedy Talwar et al1 and Prasad et al.9 These investigatorseported a positive correlation of B-type natriureticeptide and NT pro-BNP to a mean transvalvularressure gradient in 45 patients. In another study, Qi etl2 found a negative correlation of NT pro-BNP to
IGURE 6. NT pro-BNP levels with respect to age (<69 vs >70 yeS. Values are shown as mean � SEM.
IGURE 7. NT pro-BNP levels with respect to rhythm on an electroeverity of AS. Values are shown as mean � SEM. Afib � atrial fiinus rhythm.
ortic valvular area in 67 patients with AS. Thus, our J
44 THE AMERICAN JOURNAL OF CARDIOLOGY� VOL. 94
data and those of the studies citedclearly show an association betweenNT pro-BNP and severity of AS.
The increase in NT pro-BNP re-flects neurohormonal activation inpatients who have AS. This can beexplained by pressure overload of theleft ventricle with an increase in leftventricular wall stress caused by theoutflow obstruction of the stenoticvalve. However, increased NT pro-BNP levels might also be caused bystructural myocardial changes thatoccur early in the history of AS10 andby initial left ventricular dysfunctionnot detectable by imaging techniquessuch as echocardiography.
To date, the only available data onB-type natriuretic protein or NT pro-BNP in patients who have AS afterAVR have been published by Qi etal.11 In 51 patients who had AS, theyfound no significant decrease in NTpro-BNP in 21 patients 4 months af-ter AVR and in 31 patients 12 monthsafter AVR. In the present study, weincluded 31 patients whose AVR hadbeen performed �12 months previ-ously. In contrast to the findings of Qiet al,11 NT pro-BNP levels were sig-nificantly lower in patients after AVRthan in patients who had severe ASand an indication for AVR surgery.However, there was no differenceconcerning NT-proBNP, left ventric-ular mass, and mean pressure gradi-ent between patients after AVR andpatients who had mild AS. Althoughthese data were not derived from alongitudinal study, it can be postu-lated that a decrease in NT pro-BNPlevels occurs after AVR as a conse-
uence of the decrease in left ventricular wall stress.herefore, NT pro-BNP can serve as a good marker
or the functional success of AVR. In any case, thelmost identical values of NT pro-BNP and the meanransvalvular pressure gradient in patients who have arosthetic valve and those who have mild AS under-ines the consistent correlation of NT pro-BNP to theean transvalvular pressure gradient and severity ofS.
Therefore, NT pro-BNP may have an additionalalue for the diagnosis and evaluation of AS, espe-ially to monitor patients who have known AS and toetect disease progression at an early stage, and mayave attributable value as a biochemical marker touide the therapy of patients who have AS.
. Talwar S, Downie PF, Squire IB, Davies JE, Barnett DB, Ng LL. Plasma-terminal pro BNP and cardiotrophin-1 are elevated in aortic stenosis. Eur
) and severity of
diogram andllation; SR �
ars
carbri
Heart Fail 2001;3:15–19.
SEPTEMBER 15, 2004

2C73Tl465v6FlrFoo
7m8MtrFV9St1vl1C
. Qi W, Mathisen P, Kjekshus J, Simonsen S, Bjornerheim R, Endresen K, Hall. Natriuretic peptides in patients with aortic stenosis. Am Heart J 2001;142:25–732.. Gerber IL, Stewart RA, Legget ME, West TM, French RL, Sutton TM, YandleG, French JK, Richards AM, White HD. Increased plasma natriuretic peptide
evels reflect symptom onset in aortic stenosis. Circulation 2003;107:1884–1890.. Carabello BA. Clinical practice. Aortic stenosis. N Engl J Med 2002;346:677–82.. Stamm RB, Martin RP. Quantification of pressure gradients across stenoticalves by Doppler ultrasound. J Am Coll Cardiol 1983;2:707–718.. Cheitlin MD, Alpert JS, Armstrong WF, Aurigemma GP, Beller GA, BiermanZ, Davidson TW, Davis JL, Douglas PS, Gillam LD, et al. ACC/AHA guide-
ines for the clinical application of echocardiography: executive summary. Aeport of the American College of Cardiology/American Heart Association Taskorce on practice guidelines (Committee on Clinical Application of Echocardi-graphy). Developed in collaboration with the American Society of Echocardi-
graphy. J Am Coll Cardiol 1997;29:862–879. pVALVULAR HEART DISEASE/N
. Devereux RB, Reichek N. Echocardiographic determination of left ventricularass in man. Anatomic validation of the method. Circulation 1977;55:613–618.. Bonow RO, Carabello B, de Leon AC Jr., Edmunds LH Jr., Fedderly BJ, FreedD, Gaasch WH, McKay CR, Nishimura RA, O’Gara PT, et al. Guidelines for
he management of patients with valvular heart disease: executive summary. Aeport of the American College of Cardiology/American Heart Association Taskorce on Practice Guidelines (Committee on Management of Patients withalvular Heart Disease). Circulation 1998;98:1949–1984.. Prasad N, Bridges AB, Lang CC, Clarkson PB, MacLeod C, Pringle TH,truthers AD, MacDonald TM. Brain natriuretic peptide concentrations in pa-
ients with aortic stenosis. Am Heart J 1997;133:477–479.0. Krayenbuehl HP, Hess OM, Monrad ES, Schneider J, Mall G, Turina M. Leftentricular myocardial structure in aortic valve disease before, intermediate, andate after aortic valve replacement. Circulation 1989;79:744–755.1. Qi W, Mathisen P, Kjekshus J, Simonsen S, Endresen K, Bjornerheim R, Hall. The effect of aortic valve replacement on N-terminal natriuretic propeptides in
atients with aortic stenosis. Clin Cardiol 2002;25:174–180.T PRO-BNP FOR THE ASSESSMENT OF AORTIC STENOSIS 745





























