Embed Size (px)
Citation preview

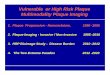
Relationship of Ultrasound Plaque Characteristics to TMPG Following Intracoronary Stenting
Relationship of Ultrasound Plaque Characteristics to TMPG Following Intracoronary Stenting
↓ TMPG Post PCI No Δ or ↑ TMPG p-value
Pre-PCI Plaque Area 12.4 ± 6.3 9.9 ± 4.1 0.047
86%
33%
56%
7%
0%
20%
40%
60%
80%
100%86%
33%
56%
7%
0%
20%
40%
60%
80%
100%
Conclusion:
Soft plaque and presence of lipid core found by IVUS during procedure was associated with impairment of myocardial perfusion even after successful intervention.
Conclusion:
Soft plaque and presence of lipid core found by IVUS during procedure was associated with impairment of myocardial perfusion even after successful intervention.
Pre-Procedure
Soft Plaque
p=0.049
Pre-Procedure
Soft Plaque
p=0.049
Lipid Core
p=0.002
Lipid Core
p=0.002
↓ TMPG↓ TMPG ↓ TMPG↓ TMPGNo Δ or ↑
TMPG
No Δ or ↑
TMPG
No Δ or ↑
TMPG
No Δ or ↑
TMPG
N=15N=15 N=15N=15N=117N=117N=117N=117
Zheng et al, ACC 2004Zheng et al, ACC 2004

Emboli Protection Improves Thrombolysis in Myocardial Infarction Perfusion Score in Saphenous Vein Graft Intervention
Emboli Protection Improves Thrombolysis in Myocardial Infarction Perfusion Score in Saphenous Vein Graft Intervention
Conclusion:Conclusion: Embolic protection as part of SVG-PCI improves TMP score when Embolic protection as part of SVG-PCI improves TMP score when compared to unprotected SVG-PCI. This finding was associated with a decrease in compared to unprotected SVG-PCI. This finding was associated with a decrease in post-procedural MACE.post-procedural MACE.
44%
13%
56%
87%
0%
20%
40%
60%
80%
100%
Unprotected SVG-PCI Protected SVG-PCI
TMP 0,1,2
TMP 3 (p<0.01)Unprotected SVG-PCI
Protected SVG-PCI
p-value
MACE 8.1% 4.2% 0.04
CK (with TMP < 3)
177 U/L 133 U/L 0.07
CK-MB (with TMP < 3)
21 ng/mL 6 ng/mL 0.07
305 patients had a SVG-PCI suitable for EPD; 247 (81%) had an angiogram 305 patients had a SVG-PCI suitable for EPD; 247 (81%) had an angiogram appropriate for TMP evaluation. Of those, 40 (20%) had an EPD deployedappropriate for TMP evaluation. Of those, 40 (20%) had an EPD deployed
Exaire et al, ACC 2004Exaire et al, ACC 2004

Evolution of Thrombolysis in Myocardial Infarction Myocardial Perfusion Grade During Primary Coronary Angioplasty in Acute Myocardial Infarction Predicts
Long-Term Recovery of Left Ventricular Function
Evolution of Thrombolysis in Myocardial Infarction Myocardial Perfusion Grade During Primary Coronary Angioplasty in Acute Myocardial Infarction Predicts
Long-Term Recovery of Left Ventricular Function
Reperfusion Pattern
0/1 to 0/1 (I)n=204
2/3 to 0/1(II)n=11
0/1 to 2 (III)n=133
2/3 to 2 (IV)n=41
0/1 to 3 (V)n=122
2/3 to 3 (VI)n=74
% pts with complete ST resolution
37.3† 36.4† 45.9† 60.9† 52.5† 72.9†
AUC [U/lxh]
3690 ± 1840
3870 ± 1975
2485 ± 882*
2340 ± 837**
2259 ± 954*
2115 ± 810**
EF-24h [%]
42 ± 11†
41 ± 3†
46 ± 9†
45 ± 12†
53 ± 9†
55 ± 8†
EF-6m [%]
39 ± 10†,***
40 ± 3†
45 ± 8†
46 ± 12†
55 ± 9†, ††
59 ± 9†, ***
Conclusion:
Maintaining a high MPG throughout PCI in AMI or achieving a marked MPG improvement are both related to improved ST resolution, smaller areas under the curve for myonecrosis, and better ejection fractions acutely and at 6 month follow-up.
Conclusion:
Maintaining a high MPG throughout PCI in AMI or achieving a marked MPG improvement are both related to improved ST resolution, smaller areas under the curve for myonecrosis, and better ejection fractions acutely and at 6 month follow-up.
Zalewski et al, ACC 2004Zalewski et al, ACC 2004
*p<0.01 vs. I, **p<0.01 vs. II, †p<0.001 among I-VI, ††p<0.001 vs. I-IV, ***p<0.01 vs. EF-24h*p<0.01 vs. I, **p<0.01 vs. II, †p<0.001 among I-VI, ††p<0.001 vs. I-IV, ***p<0.01 vs. EF-24h
AUC: Area under curve of CK-MB release in the first 48 hoursAUC: Area under curve of CK-MB release in the first 48 hours

Relationship Between Time to Reperfusion, ST-Segment Resolution, Myocardial Blush Scores and Mortality With Primary Percutaneous Coronary Intervention
for Acute Myocardial Infarction: Results from the CADILLAC Trial
Relationship Between Time to Reperfusion, ST-Segment Resolution, Myocardial Blush Scores and Mortality With Primary Percutaneous Coronary Intervention
for Acute Myocardial Infarction: Results from the CADILLAC Trial
Conclusion:Conclusion: Early time to reperfusion is associated with a greater likelihood of Early time to reperfusion is associated with a greater likelihood of successful microvascular reperfusion after primary PCI.successful microvascular reperfusion after primary PCI.
Brodie et al, ACC 2004Brodie et al, ACC 2004
55%53%
44%
64%
68%
47%
30%
35%
40%
45%
50%
55%
60%
65%
70%
<3 hrs 3-6 hrs >6 hrs
Grade 2/3 MB (p=0.007)
Complete STR* (p=0.0002)*Defined as >70%
•The CADILLAC Trial randomized 2,082 pts with AMI to The CADILLAC Trial randomized 2,082 pts with AMI to PTCA vs. stenting +/- abciximabPTCA vs. stenting +/- abciximab
•Complete STR was associated with a higher frequency Complete STR was associated with a higher frequency of Grade 2/3 MB (56% vs. 40%, p=0.0007)of Grade 2/3 MB (56% vs. 40%, p=0.0007)
•40% of pts with poor STR had good blush scores40% of pts with poor STR had good blush scores
•44% of pts with complete STR had poor blush 44% of pts with complete STR had poor blush scoresscores
•One year mortality was lowest with optimum One year mortality was lowest with optimum microvascular reperfusion (complete STR and Grade microvascular reperfusion (complete STR and Grade 2/3 MB) and highest with poor microvascular 2/3 MB) and highest with poor microvascular reperfusion (0.6% vs. 9.9%, p=0.006)reperfusion (0.6% vs. 9.9%, p=0.006)

Coronary Blood Flow Velocity and Myocardial Perfusion With Balloon Occlusion and Filter-Based Distal Protection Devices in Saphenous Vein Graft
Stenting: Early Experience of Two Centers
Coronary Blood Flow Velocity and Myocardial Perfusion With Balloon Occlusion and Filter-Based Distal Protection Devices in Saphenous Vein Graft
Stenting: Early Experience of Two Centers
Halkin et al, ACC 2004Halkin et al, ACC 2004
Balloonn=57
Filtersn=57
p-value
Final TFCg (ostium to anastomosis)
14.3 21.3 <0.01
∆ TFCn (anastomosis to distal landmark)
6.5 1.5 <0.05
Final TFC 26.0 34.0 0.05
∆ Final TFC 17.4 6.6 <0.05
Measurements done before placement of DPD, and post retrieval.Measurements done before placement of DPD, and post retrieval.
Myocardial blush graded 0-3 using the Zwolle methodology.Myocardial blush graded 0-3 using the Zwolle methodology.
Difference in TIMI 3 Flow, Baseline Blush 3, Baseline TFCg, Difference in TIMI 3 Flow, Baseline Blush 3, Baseline TFCg, ∆TFCg, Baseline TFCn, Final TFCn, and Baseline TFC not ∆TFCg, Baseline TFCn, Final TFCn, and Baseline TFC not statistically significant.statistically significant.
Conclusion:Conclusion: Balloon occlusion and aspiration DPD enhance myocardial Balloon occlusion and aspiration DPD enhance myocardial perfusion compared to filter-based DPDs.perfusion compared to filter-based DPDs.
66%
46%
30%
35%
40%
45%
50%
55%
60%
65%
70%
N=57N=57 N=57N=57
BalloonBalloon FiltersFilters
Final Grade 3 Blush
p=0.05
Final Grade 3 Blush
p=0.05

The Impact of Myocardial Blush Grade on Clinical Outcomes of Patients Treated With Saphenous Vein Grafts and Thrombotic Native Coronary Arteries: Analysis
From the X-TRACT Trial
The Impact of Myocardial Blush Grade on Clinical Outcomes of Patients Treated With Saphenous Vein Grafts and Thrombotic Native Coronary Arteries: Analysis
From the X-TRACT Trial
Tsuchiya et al, ACC 2004Tsuchiya et al, ACC 2004
Conclusion:Conclusion: Absent myocardial perfusion is an important prognostic marker of 6 Absent myocardial perfusion is an important prognostic marker of 6 month complications even among patients who achieve normal epicardial flow (TIMI month complications even among patients who achieve normal epicardial flow (TIMI 3)3)
6 Month Results
36%
4% 4%
43%45%
1% 3%2%
20%*
15%*13%*
22%*
17%*
1%*
15%*
0%5%
10%15%20%25%30%35%40%45%50%
Non-QMI(p<0.0001)
QMI(p<0.07)
Death(p=0.44)
Death orAny MI
(p<0.0001)
MACE(p<0.0001)
MBG 0/1 MBG 2 MBG 3
Patients with Final TIMI 3
4%
28%
32%
3%2%
21%19%*
14%*
17%*
0%
5%
10%
15%
20%
25%
30%
35%
Death (p=0.37) Death or Any MI(p=0.05)
MACE (p=0.04)
*P<0.05 vs. MBG 0/1*P<0.05 vs. MBG 0/1In the randomized X-TRACT trial, 797 patients underwent PCI to treat diseased SVGs In the randomized X-TRACT trial, 797 patients underwent PCI to treat diseased SVGs (72.4%) and thrombotic native coronary arteries (27.2%)(72.4%) and thrombotic native coronary arteries (27.2%)

Conclusion:Conclusion:
Improved blush grade in UAP patients undergoing PCI is associated with lower Improved blush grade in UAP patients undergoing PCI is associated with lower TnI elevation.TnI elevation.
Improved Myocardial Blush Grade Is Associated With Reduced Troponin I Elevation in Unstable Angina Patients Undergoing Percutaneous Intervention
Improved Myocardial Blush Grade Is Associated With Reduced Troponin I Elevation in Unstable Angina Patients Undergoing Percutaneous Intervention
Prasan et al, ACC 2004Prasan et al, ACC 2004
Troponin I (ug/L)p<0.001
0.11 ± 0.01
0.14 ± 0.01
0.68 ± 0.26
0.34± 0.12
0.00
0.20
0.40
0.60
0.80
1.00
MBG 0 MBG 1 MBG 2 MBG 3
MBG 0n=69
MBG 1n=58
MBG 2n=112
MBG 3n=133
p-value
Death 5 2 3 4 ns
TVR 11 19 18 18 <0.05
372 consecutive UAP treated with PCI were included, none with 372 consecutive UAP treated with PCI were included, none with pre-procedural TnI elevation.pre-procedural TnI elevation.
TnI was measured 24 hours post procedure.TnI was measured 24 hours post procedure.
Patients who did not have TnI elevation were ascribed a value of Patients who did not have TnI elevation were ascribed a value of 0.1 ug/L.0.1 ug/L.
TVR: Target Vessel Revascularization.TVR: Target Vessel Revascularization.
N=69N=69 N=58N=58 N=112N=112 N=133N=133

Distal Protection Device Was Associated With Better Left Ventricular Function by Improving Microcirculation After Primary Coronary Intervention
Distal Protection Device Was Associated With Better Left Ventricular Function by Improving Microcirculation After Primary Coronary Intervention
PercuSurge® C Group p-value
LV Ejection Fraction 52% ± 9% 45% ± 10% 0.01
PercuSurge: Use of PercuSurgePercuSurge: Use of PercuSurge® distal protection device® distal protection device
C Group: Selected by matching infarct-related artery, pre-angioplasty TIMI flow grade, C Group: Selected by matching infarct-related artery, pre-angioplasty TIMI flow grade, sex, age, and pain-to-balloon time.sex, age, and pain-to-balloon time.
There was no significant difference in death, MI, or TIMI 3 Flow.There was no significant difference in death, MI, or TIMI 3 Flow.
Conclusion:Conclusion:
PercuSurgePercuSurge®® was associated was associated with a better recovery of with a better recovery of myocardial function as well as myocardial function as well as better microcirculatory function at better microcirculatory function at 30 days after primary angioplasty.30 days after primary angioplasty.
62%
76%
30%
47%
0%
10%
20%
30%
40%
50%
60%
70%
80%
Percu-SurgePercu-Surge
C GroupC Group Percu-SurgePercu-Surge
C GroupC Group
N=30N=30 N=29N=29 N=30N=30 N=29N=29
Grade 3 Blush
p=0.04
Grade 3 Blush
p=0.04
Early STR
p=0.02
Early STR
p=0.02
Rhee et al, ACC 2004Rhee et al, ACC 2004

Percutaneous Coronary Intervention With Distal Protection Device Preserves Left Ventricular Function in Patients With Acute Anterior Myocardial InfarctionPercutaneous Coronary Intervention With Distal Protection Device Preserves
Left Ventricular Function in Patients With Acute Anterior Myocardial Infarction
Nakamura et al, ACC 2004Nakamura et al, ACC 2004
Conclusion:Conclusion: PCI with the PercuSurge GuardWire® could not only restore epicardial PCI with the PercuSurge GuardWire® could not only restore epicardial coronary flow and myocardial perfusion, but also preserve left ventricular function in coronary flow and myocardial perfusion, but also preserve left ventricular function in anterior AMI.anterior AMI.
28
35
15
20
25
30
35
40
46%
20%
0%
10%
20%
30%
40%
50%
60%
70%
327
455
0
50
100
150
200
250
300
350
400
450
500
cTFC
p=0.030
cTFC
p=0.030MBG 3
p=0.029
MBG 3
p=0.029
Peak CK Myocardial Fraction Level
p=0.043
Peak CK Myocardial Fraction Level
p=0.043
GW Protection
GW Protection
ControlControl GW Protection
GW Protection
ControlControl GW Protection
GW Protection
ControlControl
N=42N=42 N=30N=30 N=42N=42 N=30N=30 N=42N=42 N=30N=30

Impact of Angioplasty with Distal Protection Device on Myocardial Reperfusion
Impact of Angioplasty with Distal Protection Device on Myocardial Reperfusion
GuardWire Plus™
No Distal Protection
p-value
cTFC 23.7 ± 10.3 33.7 ± 20.6 0.04
LVEF* 51.2% ± 14.5%
46.7% ± 12.2%
0.02
Severity Score
5.6 ± 6.3 10.3 ± 7.3 0.01
Patients within 12 hours after onset of AMI were enrolled and Patients within 12 hours after onset of AMI were enrolled and randomly assigned.randomly assigned.
*Thallium-201 Myocardial Scintigraphy*Thallium-201 Myocardial Scintigraphy
Conclusion:Conclusion: Use of this distal protection device during PCI in patients with AMI was Use of this distal protection device during PCI in patients with AMI was associated with a significant improvement of coronary reperfusion compared with associated with a significant improvement of coronary reperfusion compared with conventional PCI.conventional PCI.
71%
79%
35%
50%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Guard-Wire
Guard-Wire
No Distal ProtectionNo Distal
Protection
N=34N=34 N=30N=30 N=34N=34 N=30N=30
Grade 3 Blush
p=0.02
Grade 3 Blush
p=0.02
Early STR
p=0.03
Early STR
p=0.03
Guard-Wire
Guard-Wire
No Distal ProtectionNo Distal
Protection
Nanasato et al, ACC 2004Nanasato et al, ACC 2004

Angiographically Apparent Thrombus After Fibrinolytic Administration Is Associated With Impaired Epicardial Flow and Myocardial Perfusion in ST
Elevation Myocardial Infarction Patients with Open Arteries
Angiographically Apparent Thrombus After Fibrinolytic Administration Is Associated With Impaired Epicardial Flow and Myocardial Perfusion in ST
Elevation Myocardial Infarction Patients with Open Arteries
Conclusion:Conclusion:
Angiographically-apparent Angiographically-apparent thrombus after fibrinolytic thrombus after fibrinolytic administration is administration is independently associated independently associated with slower epicardial flow with slower epicardial flow and impaired myocardial and impaired myocardial perfusion, despite a patent perfusion, despite a patent epicardial artery.epicardial artery.
Kirtane, Karmpaliotis et al, ACC 2004Kirtane, Karmpaliotis et al, ACC 2004
Residual Thrombus
No Residual Thrombus
p-value Multivariate† OR
p-value
TFG 3n=929
69.3% 73.2% 0.03 N/A
CTFC (frames)n=907
34 31 0.0003 N/A0.01
TMPG 2/3n=929
57.0% 68.0% 0.001 0.710.027
††Multivariate regression models incorporating age, time-to-treatment, gender, history Multivariate regression models incorporating age, time-to-treatment, gender, history of hypercholesterolemia, LAD culprit location, reference segment diameter, percent of hypercholesterolemia, LAD culprit location, reference segment diameter, percent stenosis of the culprit lesion, lesion length, and TFG 3.stenosis of the culprit lesion, lesion length, and TFG 3.
Clinical & angiographic data were analyzed from 929 patients with open arteries Clinical & angiographic data were analyzed from 929 patients with open arteries enrolled in the TIMI 14, 20, 23, and 24 trials in STEMI.enrolled in the TIMI 14, 20, 23, and 24 trials in STEMI.

Distinct Modes of Cardiovascular Death Associated With Impaired Epicardial and Myocardial Perfusion Following Fibrinolysis for ST Elevation Myoardial
Infarction
Distinct Modes of Cardiovascular Death Associated With Impaired Epicardial and Myocardial Perfusion Following Fibrinolysis for ST Elevation Myoardial
Infarction
Conclusion:Conclusion:
Impairment of epicardial and myocardial perfusion were associated with Impairment of epicardial and myocardial perfusion were associated with cardiovascular mortality. Angiographic features differed among causes of death.cardiovascular mortality. Angiographic features differed among causes of death.
Wiviott et al, ACC 2004Wiviott et al, ACC 2004
Cardiac Death (Compared to Survivors)
p-value
Less likely to have TFG 2-3 <0.001
Less likely to have TMPG 2-3 0.004
Higher CTFC (68 vs. 52) <0.001
3 Vessel CAD 0.001
Thrombus 0.001
3683 patients from an angiographic database STEMI 3683 patients from an angiographic database STEMI fibrinolysis trials were analyzed. 180 deaths (4.9%) fibrinolysis trials were analyzed. 180 deaths (4.9%) were observed.were observed.
Cause of Death
%
CHF/Shock 22%
Stroke/ICH 18%
Dysrhythmia 16%
Cardiac Rupture
13%
MI 12%
Other Cardiac
7%
Hemorrhage 3%

Objective Evaluation of Tissue Level Perfusion Using Parametric Analysis of Myocardial Blush Kinetics
Objective Evaluation of Tissue Level Perfusion Using Parametric Analysis of Myocardial Blush Kinetics
Conclusion:Conclusion:
Parametric imaging can be used Parametric imaging can be used to objectively analyze tissue level to objectively analyze tissue level perfusion following percutaneous perfusion following percutaneous intervention. This approach may intervention. This approach may be used to gauge reperfusion be used to gauge reperfusion strategies in acute coronary strategies in acute coronary syndromes. syndromes.
Kuecherer et al, ACC 2004Kuecherer et al, ACC 2004
Successful Reperfusion
Unsuccessful Reperfusion
Tmax (cycles from dye injection)
8.6 ± 3.4 5.6 ± 1.1
Wash-in (grey levels/cycle)
6.0 ± 3.0 17.2 ± 8.2
Wash-out (gray levels/cycle)
3.8 ± 0.8 12.6 ± 6.3
Method:Method:
Developed and tested a computer assisted procedure Developed and tested a computer assisted procedure to visualize and objectively quantitate both temporal to visualize and objectively quantitate both temporal and spatial spread of myocardial blush in 8 normals and spatial spread of myocardial blush in 8 normals (mean age 61 years) and in 34 patients (mean age 65 (mean age 61 years) and in 34 patients (mean age 65 years), defining 4 different parameters for each years), defining 4 different parameters for each intensity profile that were displayed as color coded intensity profile that were displayed as color coded maps: maximal intensity (Gmax), time to maximal maps: maximal intensity (Gmax), time to maximal intensity (Tmax), maximal upslope (Imax) and maximal intensity (Tmax), maximal upslope (Imax) and maximal downslope (Dmax).downslope (Dmax).

75%
81%
89%
96%
50%55%60%65%70%75%80%85%90%95%
100%
Impact of Initial Patency of the Infarct Related Vessel on Outcome in Patients With Acute Myocardial Infarction Treated With Primary Angioplasty
Impact of Initial Patency of the Infarct Related Vessel on Outcome in Patients With Acute Myocardial Infarction Treated With Primary Angioplasty
Conclusion:Conclusion:
Not only TIMI 3 flow, but Not only TIMI 3 flow, but any increase in initial any increase in initial TIMI flow of the IRV is TIMI flow of the IRV is associated with a better associated with a better preserved LVEF, preserved LVEF, smaller enzymatic smaller enzymatic infarct size and higher infarct size and higher MBG.MBG.
Ernst et al, ACC 2004Ernst et al, ACC 2004
TIMI 0(65%)
TIMI 1(10%)
TIMI 2(12%)
TIMI 3(13%)
LDHQ48 All MI 1513 ± 1264
1159 ± 1484
1014 ± 956
748 ± 700
LDHQ48 Anterior MI 1816 ± 1404
1601 ± 2126
1115 ± 1064
808 ± 831
LVEF All MI 43% ± 11%
46% ± 11%
44% ± 11%
48% ± 11%
LVEF Anterior MI 36% ± 10%
39% ± 13%
41% ± 11%
46% ± 11%
Angiographic and clinical data of 1702 consecutive patients with acute MI treated with PA.Angiographic and clinical data of 1702 consecutive patients with acute MI treated with PA.
LDHLDHQ48Q48: Enzymatic infarct size as determined by serial measurements of lactate : Enzymatic infarct size as determined by serial measurements of lactate
dehydrogenase up to 48 hours after onset of symptoms.dehydrogenase up to 48 hours after onset of symptoms.
MBG 2/3:

21%
25%
29%
0%
5%
10%
15%
20%
25%
30%
35%
The Role of Collateral Circulation in the Acute Phase of ST-Segment Elevation Myocardial Infarction Treated With Primary Coronary Intervention
The Role of Collateral Circulation in the Acute Phase of ST-Segment Elevation Myocardial Infarction Treated With Primary Coronary Intervention
Conclusion:Conclusion:
Presence of angiographically Presence of angiographically detectable collaterals have a detectable collaterals have a protective effect on protective effect on enzymatic infarct size and enzymatic infarct size and pre- and post-intervention pre- and post-intervention hemodynamic conditions in hemodynamic conditions in patients with acute MI patients with acute MI treated with early PCI, in treated with early PCI, in particular when Rentrop particular when Rentrop grade 2/3 is present and in grade 2/3 is present and in LAD related infarcts.LAD related infarcts.
Elsman et al, ACC 2004Elsman et al, ACC 2004
Collateral Flow Grade 0 1 2/3 p-value
Killip Class ≥2 at Presentation
12% 10% 4% 0.01
Intra Aortic Balloon Pumping Post-PCI
17.2% 12.8% 4.7% 0.0005
LDHQQ48 (U/l) 1947 ± 1553
1893 ± 1549
1221 ± 767
0.001
Between 1994 and 2001, 1074 patients with acute MI treated with early PCI TIMI 0 or 1 Between 1994 and 2001, 1074 patients with acute MI treated with early PCI TIMI 0 or 1 flow at first contrast injection and technically adequate angiograms for collateral flow flow at first contrast injection and technically adequate angiograms for collateral flow were analyzed.were analyzed.
MBG 3: p=0.04

Impaired Myocardial Perfusion Is a Major Explanation of the Poor Outcome Observed in Patients Undergoing Primary Angioplasty for ST-Segment
Elevation Myocardial Infarction and Signs of Heart Failure
Impaired Myocardial Perfusion Is a Major Explanation of the Poor Outcome Observed in Patients Undergoing Primary Angioplasty for ST-Segment
Elevation Myocardial Infarction and Signs of Heart Failure
Conclusion:Conclusion: Patients with ventricular decompensation complicating STEMI Patients with ventricular decompensation complicating STEMI have impaired myocardial perfusion, which may accounts for the poor outcome have impaired myocardial perfusion, which may accounts for the poor outcome observed in these patients.observed in these patients.
De Luca et al, ACC 2004De Luca et al, ACC 2004
Population represented by a Population represented by a cohort of 1548 consecutive cohort of 1548 consecutive patients with STEMI undergoing patients with STEMI undergoing primary angioplasty.primary angioplasty.