Embed Size (px)
Citation preview

1
Hematuria in CHildren
The detection of microscopic hematuria in a child’s urine prompts an evaluation for medical renal and uri-nary bladder diseases [1–5]. Macroscopic hematuria is visible to the naked eye, whereas microscopic hematu-ria is usually detected clinically on dipstick testing of urine at a routine examination. Subsequently, hematu-ria is confirmed microscopically with a concentrated urinary sediment specimen. Microscopic hematuria usually requires concentration, while macroscopic hematuria does not. Dipstick sensitivity (100%) and specificity (99%) are quite high and can detect 1–5 RBCs/hpf, which corresponds to a concentration of 5–10 RBCs/μL in urine. Microhematuria in 2–3 uri-nalyses over a 2- to 3-week period prompts further workup. Clinically significant hematuria is usually associated with 5–10 RBCs/μL of urine. As part of well-child care, a screening urinalysis is recommended
by the American Academy of Pediatrics at an initial school physical examination (age 4–5 years) and once during adolescence (11–21 years).
Hematuria may originate from the glomeruli, renal tubules and interstitium, and urinary tract (collecting system, ureters, bladder, urethra), and is associated with many different disease processes (Table 1), medications, or toxins (Table 2) [1–5]. Bright red urine, visible clots, or crystals with intact normal RBCs suggest urinary tract bleeding. Cola-colored urine, RBC casts, and distorted RBCs suggest glomerular disease. Absence of RBCs in urine suggests hemoglobinuria or myoglobinuria.
Macroscopic hematuria in children has an incidence of 1.3 per 1000 [1–5]. Microscopic hematuria is more common (4.1 per 1000 with 4 urine samples; 3.2 per 1000 for girls and 1.4 per 1000 for boys with 5 urine samples). Some epidemiologic studies have noted hematuria prevalence to be as high as 1–2% in 6- to 15-year-olds when 2 or more samples have been obtained [1–5].
Ultrastructural Pathology, 36(1), 1–18, 2012Copyright © 2012 Informa Healthcare USA, Inc.ISSN: 0191-3123 print/1521-0758 onlineDOI: 10.3109/01913123.2011.620731
This presentation represents a lecture handout from a portion of the Basic Tutorial on Pediatric Renal Disease in the Pediatric Section of the Society for Ultrastructural Pathology Biennial Meeting in Richmond, Virginia in July 2010 (UltraPath XV), and as part of the Pediatric Renal Symposium at the Society for Pediatric Pathology Annual Spring Meeting in Washington, DC in March 2010. This paper is designed to provide an overview and introduction to pediatric renal disease associated with hematuria, but not represent an exhaustive detailed review of such entities. The references provide a list of publications with more in-depth coverage of the specific entities than covered in this brief general overview.
Received 28 August 2011; accepted 29 August 2011
Correspondence: John Hicks, 6621 Fannin Street MC1-2261, Department of Pathology, Texas Children’s Hospital, Houston, TX 77030, USA. E-mail: [email protected]
28 August 2011
00 00 0000
29 August 2011
© 2012 Informa Healthcare USA, Inc.
2012
Ultrastructural Pathology
0191-31231521-0758
10.3109/01913123.2011.620731
36
118
1
620731
UUSP
REVIEW
renal diseases associated with Hematuria in Children and adolescents: a Brief tutorial
John Hicks1, Gary Mierau2, Eric Wartchow2, and Karen Eldin1
1Texas Children’s Hospital and Baylor College of Medicine, Houston, Texas, USA and 2The Children’s Hospital, Aurora, Colorado, USA
aBstraCt
The detection of microscopic hematuria in a child’s urine prompts evaluation for renal and urinary bladder causes. Microscopic hematuria identified during a routine physical examination by the pediatrician is much more common than macroscopic hematuria. Persistent microscopic hematuria is particularly worrisome and may require a percutaneous needle core kidney biopsy to determine whether the etiology is secondary to glomerular disease, tubulointerstitial disease, urinary tract infection, urinary tract structural abnormalities, medications, or toxins. This paper reviews the epidemiology, pathologic features, pathogenesis, treatment, and outcome of familial hematuria (Alport syndrome [hereditary nephritis]), thin basement membrane nephropa-thy), IgA nephropathy, Henoch-Schönlein purpura, and acute postinfectious glomerulonephritis.
Keywords: Hematuria, IgA nephropathy, Alport syndrome, thin basement membrane nephropathy, postinfectious nephropathy, familial hematuria
Ultr
astr
uct P
atho
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f T
oron
to o
n 05
/04/
15Fo
r pe
rson
al u
se o
nly.

2 J. Hicks et al.
Ultrastructural Pathology
Persistent hematuria has been reported in 23% of children with microscopic hematuria on 2 initial urine samples who underwent 2 subsequent evaluations after 4–6 months [1–5]. In studies with children with persis-tent hematuria undergoing kidney biopsy, it has been shown that about 65% have either thin basement mem-brane disease or Alport syndrome (hereditary nephritis [1–5]. IgA nephropathy was present in up to 32%. The remaining children tended to have normal or clinically insignificant glomerular findings. Depending on the threshold for performing a renal biopsy, the proportion of normal renal biopsy findings may be much higher, with some clinical studies reporting 28–47% normal findings. Interestingly, the majority of asymptomatic patients with isolated microscopic hematuria who have undergone renal biopsies have normal findings. The most common cause of isolated microscopic hema-turia has been reported to be hypercalciuria (16–30%). It has been suggested that asymptomatic children with isolated microscopic hematuria should not routinely undergo renal biopsy. The combination of hematuria
and proteinuria is concerning for significant renal dis-ease in children.
With children with gross hematuria who have undergone renal biopsies, 30% had glomerular dis-ease, while 30% had normal renal biopsy findings [1–5]. Glomerular diseases included IgA nephropathy (54%), Alport syndrome (25%), and acute postinfec-tious glomerulonephritis (13%). The remaining 40% had nonglomerular-associated hematuria with the most common etiology being hypercalciuria (16%). Urethrorrhagia (14%), hemorrhagic cystitis (12%), uro-lithiasis (5%), and sickle cell trait (3%) were the other causes for gross hematuria.
TABLE 1 Causes of hematuria in children.Glomerular diseases
Recurrent gross hematuriaIgA nephropathy, benign familial hematuria, Alport syndrome
Acute postinfectious glomerulonephritisMembranoproliferative glomerulonephritisLupus glomerulonephritisMembranous glomerulonephritisRapidly progressive glomerulonephritisHenoch-Schönlein purpuraGoodpasture disease
Interstitial and tubular diseasesAcute pyelonephritisAcute interstitial nephritisInfections (mycobacteria)Hematologic conditions (sickle cell disease, coagulopathies,
factor VIII deficiencies, von Willebrand disease, renal vein thrombosis, thrombocytopenia)
Urinary tract diseaseInfection (bacteria, virus [especially adenovirus])Nephrolithiasis and hypercalciuriaStructural and congenital abnormalities (ureteropelvic
junction obstruction)Polycystic kidney diseaseTumorsVascular malformationsUrinary tract polypsTraumaExerciseMedicationsToxinsIdiopathic urethrorrhagia (terminal urethral hematuria,
dysuria in prepubertal males, 90% spontaneous resolution)
TABLE 2 Medications and toxins associated with hematuria on urinalysis.Hemoglobinuria
Carbon monoxideMushroomsNaphthaleneSulfonamidesTin compoundsLeadMethicillinPhenolTurpentineTiclopidine
HematuriaAminoglycosidesAmitriptylineAnticoagulantsAnticonvulsantsAspirinChlorpromazineCyclophosphamideDiureticsPenicillinThorazineTolueneAntiretrovirals (Ritonavir, Indinavir)
Urine ColorDark yellow or orange
Normal concentrated urineRifampin, pyridium
Dark brown or blackMethemoglobinemiaBile pigmentsHomogentisic acid, thymol, melanin, tyrosinosis, alkaptonuriaAlanine, cascara, resorcinol
Red or pink urineRBCs, free hemoglobin, myoglobin, porphyrinsBenzene, chloroquine, desferoxamine, phenazopyridine,
phenolphthaleinBeets, blackberries, red food dyesUratesIron sorbitolIbuprofenNitrofurantoin
Ultr
astr
uct P
atho
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f T
oron
to o
n 05
/04/
15Fo
r pe
rson
al u
se o
nly.

Pediatric Renal Disease with Hematuria 3
© 2012 Informa Healthcare USA, Inc.
Familial Hematuria
epidemiology, Genetics, and Clinical Features
Thin basement membrane nephropathy (TBMN, benign familial hematuria) and hereditary nephritis (Alport syndrome [AS]) are the major forms of familial hematuria, and account for 30–50% of children with glomerular-based hematuria referred to pediatric neph-rologists [6–25]. As noted previously, hematuria may be caused by other inherited conditions (polycystic kidney disease, hypercalciuria). Mutations in type IV collagen occur in many Alport syndrome patients and in about 50% of those with thin basement membrane nephropathy (Table 3). Less common forms of familial hematuria include Epstein and Fechtner syndromes, which are caused by nonmuscle myosin heavy-chain IIA mutations (MYH9 gene).
X-linked Alport syndrome accounts for 80–85% of AS cases, with autosomal recessive AS making up 15% [6,8–10,12,14–16,18–21,23–25]. Autosomal domi-nant AS comprises the remaining 1–5% of cases due to heterozygous mutations in COL4A3 or COL4A4 genes. The majority of those with heterozygous mutations in COL4A3 or Col4A4 genes have a form of familial hema-turia that is most often not progressive and is consid-ered to be TBMN. Molecular diagnosis is complicated by the fact that there are several hundred mutations in the COL4A5 gene in X-lined AS. There are several dozen mutations in COL4A3 and COL4A4 genes in AS with either autosomal dominant or recessive inheritance and TBMN. Mutations include missense, nonsense, splicing, and deletion mutations. The diagnostic criteria for AS (hereditary nephritis) and TBMN are listed in Table 4.
Persistent hematuria is the hallmark of AS (hereditary nephritis) and occurs in 100% of boys and 95–100% of girls with either X-linked or autosomal recessive AS [7,8, 10,11,15,16,18,19,22,24,25]. The onset of hematuria with affected boys occurs in infancy. Occasionally, blood-stained diapers may be the first sign of AS. Some chil-dren have nearly continuous gross hematuria; whereas, others have episodic gross hematuria. Only 10–15% of children with X-linked AS have de novo mutations.
Therefore, the majority of X-linked AS children will have one parent with hematuria. With autosomal recessive AS, both parents are heterozygous carriers for either a COL4A3 or a COL4A gene mutation. Hematuria is seen in about 50% of carrier parents. It is possible that both, one, or neither parent(s) of an affected child with autosomal recessive AS will have hematuria.
Over time, deafness develops in 80–90% of males with X-linked AS, and in a similar percentage of males and females with autosomal recessive AS [7,8,11,15–19,22,25]. Deafness may not have developed when the child was first evaluated for AS. Usually, hearing deficits are detected in late childhood. The classic characteristics for hearing loss in AS are that (1) it is not present at birth; (2) it is bilateral with symmetric onset and sever-ity; (3) it initially affects high-frequency wavelengths (2000–8000 Hz); and (4) it gradually involves conversa-tional speech wavelengths.
Ocular abnormalities occur in 40% of males with X-linked AS [8,11,15,16,18,19,25]. A distinctive macul-opathy comprised of white to yellow flecks around the macula occurs in 20% of affected males. These perimac-ular flecks increase with age. Protrusion of the central region of the lens into the anterior chamber (anterior lenticonus) is characteristic of AS and found in 20% of affected males. This is not typically identified until adolescence or early adulthood. Corneal endothelial vesicles (posterior polymorphous dystrophy) and recur-rent corneal erosion may occur and be quite painful. About 15% of X-linked AS females have maculopathy, but rarely have anterior lenticonus. Autosomal recessive AS patients may have similar ocular abnormalities.
Smooth muscle tumors (leiomyomata) occur in a small number of families with X-linked AS [7–9,11,16–19,25].
TABLE 3 Familial hematuria mutations.Alport syndrome Gene ProteinX-linked (Xq22) Col4A5 α5(IV)Autosomal dominant (2q35-37) Col4A3 α3(IV) Col4A4 α4(IV)Autosomal recessive (2q35-37) Col4A3 α3(IV) Col4A4 α4(IV)Thin basement membrane nephropathy Autosomal dominant (2q35-37) Col4A3 α3(IV) Col4A4 α4(IV)Epstein & Fechtner syndromes Autosomal dominant (22q11.2)
MYH9
Nonmuscle myosin heavychain IIA
TABLE 4 Familial hematuria: diagnostic criteria.Alport syndrome (at least two diagnostic criteria required)
Family history of hematuria progressing to end-stage renal disease
Characteristic glomerular basement membrane lamellations and/or basket-weaving
Progressive high-frequency sensorineural deafnessAnterior lenticonus or perimacular retinal flecks
(maculopathy)Absent or decreased glomerular basement membrane
type IV collagen [α3(IV), α4(IV), α5(IV) chains] by immunocytochemistry
Absent or decreased epidermal basement membrane type IV collagen α5(IV) chain
Mutations in COL4A3, COL4A4 or COL4A5 genesThin basement membrane nephropathy (benign familial hematuria)
Isolated hematuria with normal kidney function, urine pro-tein excretion and blood pressure
Family history of hematuria consistent with autosomal dominant inheritance
Negative family history of kidney failure or extrarenal manifestations
Renal biopsy may be used to confirm diagnosisDiffuse attenuation of glomerular basement membrane
Ultr
astr
uct P
atho
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f T
oron
to o
n 05
/04/
15Fo
r pe
rson
al u
se o
nly.

4 J. Hicks et al.
Ultrastructural Pathology
Typically, these tumors are seen in the esophagus and tracheobronchial tree. Additionally, affected females may have external genitalia smooth muscle tumors. The smooth muscle tumors are due to large deletions that span the adjacent 5’ ends of the COL4A5 and COL4A6 genes on the X chromosome (Alport syndrome-associ-ated diffuse leiomyomatosis complex).
The noncollagen disorders associated with MYH9 gene mutations, Epstein and Fechtner syndromes, also have progressive nephropathy, deafness, ocular changes, and thickening of the glomerular basement membranes, simi-lar to AS [6–8,11,12,15–19,21,23–25]. In addition, Epstein syndrome has thrombocytopenia and giant platelets, while Fechtner syndrome has thrombocytopenia, giant platelets, and May-Hegglin anomaly with granulocytes.
Pathology Findings
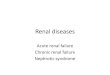
In children, AS and TBMN may have similar features on light, immunofluorescence, and electron microscopy, as detailed in Tables 5–7 [10–12,14–19,21–25]. However, with evaluation of a variety of antibodies to α chains of type IV collagen, separation of AS and TBMN is possible, as will be discussed later in this section. With AS-affected males, mesangial proliferation and interstitial fibrosis with foam cells will be seen over time (Figure 1). Progression to focal segmental glomerular sclerosis (FSGS) and global sclerosis with interstitial fibrosis occurs as a late phase of disease (Table 5, Figure 2). A history of familial hematuria in a child with mesangial proliferation or FSGS suggests the diagnosis of AS (hereditary nephritis). With female AS
a b
c
e
d
f
FIGURE 1 Alport syndrome (hereditary nephritis). (A, B) Glomeruli with mild increase in mesangial cells with no segmental lesions or crescents and no tubular atrophy (A: H&E; B: PAS). (C) Proximal tubules with erythrocytes in their lumens corresponds to clinical feature of hematuria (H&E). (D) Interstitial foam cells may be seen in Alport syndrome, although nonspecific (H&E). (E) Basket-weaving (lamellations) of the glomerular basement membranes is a hallmark of Alport syndrome (transmission electron microscopy). (F) Thin glomerular basement mem-branes (top membrane) and basket-weaving of glomerular basement membranes may be present (transmission electron microscopy).
Ultr
astr
uct P
atho
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f T
oron
to o
n 05
/04/
15Fo
r pe
rson
al u
se o
nly.

Pediatric Renal Disease with Hematuria 5
© 2012 Informa Healthcare USA, Inc.
carriers and TBMN-affected individuals, kidney biopsies are typically normal on routine light and immunofluores-cence microscopy (Figures 1 and 3). Electron microscopy holds the key to differentiating AS from TBMN in children
with hematuria, as illustrated in Figures 1–3. With TBMN, there is diffuse glomerular basement membrane attenua-tion (thinning) of the lamina densa (Figure 3, Table 6). The endothelial cells and visceral epithelial cells (podocytes) are intact. These features are similar with both AS and TBMN in young children. The diagnostic ultrastructural characteristics for AS are (1) thickening of the basement membrane; (2) lamellation (splitting, basket-weaving) of the lamina densa into multiple strands that enclose electron-lucent areas and may contain electron-dense particles; (3) scalloping of epithelial aspects of the GBM; and (4) partial to complete effacement of foot processes in areas of GBM thickening. With X-linked AS males, these features occur during childhood and increase progres-sively with age. With AS females, the GBM thickening varies from focal to diffuse and may or may not progress with age.
With hereditary nephritis, the ultrastructural features vary depending on the stage of the disease [10–12,14–19,21–25]. In the early phase of Alport syndrome, there may be only diffuse thinning of the basement mem-branes, raising a concern for thin basement membrane nephropathy or Alport syndrome. At a later phase, the glomerular basement membranes become thickened and possess lamellations with a more typical splitting of the membranes. The lamellations may not involve all areas
a b
c
FIGURE 2 Alport syndrome (hereditary nephritis). (A) Diffuse mesangial capillary proliferation with the glomeruli and tubular atrophy with casts may be present (H&E); (B) Later phase of Alport syndrome may present with glomeruli undergoing global sclerosis, intersti-tial fibrosis and tubular atrophy (H&E); (C) Basket-weaving of glomerular basement membranes may also be identified with later stage Alport syndrome (transmission electron microscopy).
TABLE 5 phases of Alport syndrome.Phases I II III IVClinical features
Hematuria + + + +Proteinuria – + + +GFR NL NL Low ESRD
Histopathology (light microscopy) Mesangial proliferation – + NA NAFSGS – +/– + NAGlobal sclerosis – – +/– +
Interstitium (light & electron microscopy) Normal + + – –Fibrosis – – + +
Glomeruli (electron microscopy) GBM mostly thin + – – –GBM thickened – + + NAFoot process fusion – + + NASclerosis – – – +
Note. GFR, glomerular filtration rate; NL, normal; ESRD, end-stage renal disease; NA, not applicable.
Ultr
astr
uct P
atho
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f T
oron
to o
n 05
/04/
15Fo
r pe
rson
al u
se o
nly.

6 J. Hicks et al.
Ultrastructural Pathology
of the glomerulus, but may involve segments of the capil-lary loops or only some capillaries. This imparts alternat-ing areas of thin basement membranes with lamellated, thickened basement membranes. At the fully developed stage of Alport syndrome, the entire glomerular basement membrane is affected, resulting in irregular contours to the outer portion of the membrane as well as the lamina densa and lamina rara interna and externa. Electron-lucent areas are present between the lamellations and contain electron-dense, fine granular, mottled material (20–90 nm). The glomerular basement membranes may be ruptured in areas and these rupture sites contain invaginations of the visceral epithelial cell (podocytes) and endothelial cell processes. Electron-dense deposits are unusual in heredi-tary nephritis, but focal minute paramesangial deposits may be seen occasionally. Rarely are there focal minute intramembranous deposits. At an ultrastructural level, males tend to have more severe disease than females and the onset of disease and progression of disease occurs at an earlier age. There are certain kindred with clinically typical Alport syndrome hereditary that have only thin basement membranes even at advanced clinical stages of the disease. Electron microscopic examination of a kidney biopsy in a child with persistent hematuria may provide the first diagnostic features that define the renal disease as hereditary nephritis. Similarly, thin basement mem-brane nephropathy may be first diagnosed with electron microscopy.
Immunostaining with antibodies against α3(IV), α4(IV), and α5(IV) type IV collagen chains may be of util-ity in questionable cases (Table 7) [8–10,12, 14–19,21–25]. It should be noted that several of the immunostains and immunofluorescent antibody studies are only available at certain institutions and in research laboratories pro-viding such services. Normal basement membranes in the glomeruli, Bowman’s capsule, and tubules exist as α3α4α5(IV) type IV collagen heterotrimers. Mutations in both alleles of COL4A3 or COL4A4 in autosomal recessive AS frequently lead to complete absence of
a b
FIGURE 3 Thin basement membrane nephropathy. (A) Glomeruli may show only a focal increase in mesangial cells (H&E). (B) Markedly thin glomerular basement membranes for the child’s age in a diffuse pattern are the hallmark for thin basement membrane nephropathy (transmission electron microscopy).
TABLE 6 Glomerular basement membrane thickness in children.
Age (years)Normal ranges
Males FemalesBirth 135–253 nm 137–251 nm1 146–273 nm 146–267 nm2 156–292 nm 154–283 nm3 167–312 nm 163–299 nm4 177–332 nm 172–315 nm5 188–351 nm 180–331 nm6 198–371 nm 189–347 nm7 209–391 nm 198–363 nm8 219–410 nm 206–379 nm>9 230–430 nm 215–395 nmMean Glomerular Basement Membrane Thickness Birth 194 nm 194 nm >9 years of age 330 nm 305 nmAFIP/ARP: General thin basement membrane guideline Adults <250 nm Children <200 nm AFIP/ARP: Average Basement Membrane ThicknessBirth 169 ± 20 nm 2 years of age 245 ± 49 nm Adult female 320 ± 40 nm Adult male 370 ± 49 nm Note. AFIP/ARP, Armed Forces Institute of Pathology/American Registry of Pathology.
Thin Basement Membrane Nephropathy Diagnostic Criteria (Benign Familial Hematuria):
1. Average of 30 measurements of glomerular basement mem-brane (GBM) thickness is below the lower limit of normal range for child’s age and gender.
2. 50% or more of individual GBM measurements are below the lower limit of the normal range for child’s age and gender.
3. Widespread lamellation (splitting) of GBM is not present, but may be very localized.
4. Indirect immunofluorescence for α3(IV) and α5(IV) show no evidence of Alport syndrome.
5. No family history of renal failure or extrarenal manifestations.
Ultr
astr
uct P
atho
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f T
oron
to o
n 05
/04/
15Fo
r pe
rson
al u
se o
nly.

Pediatric Renal Disease with Hematuria 7
© 2012 Informa Healthcare USA, Inc.
α3α4α5(IV) heterotrimers. This also results in loss of α3α4α5(IV) heterotrimers in the cochlear and ocular basement membranes. In addition, the α5(IV) chain is a component of the α5α5α6(IV) heterotrimer, which is present in Bowman’s capsule (BC), distal (dTBM) and collecting duct tubule basement membranes, and the epidermal basement membranes. In X-linked AS males, COL4A5 mutations results in loss of both the α3α4α5(IV) heterotrimer and the α5α5α6(IV) heterotrimer. With autosomal recessive AS, mutations in COL4A3 and COL4A4 do not affect the expression of α5α5α6(IV) het-erotrimer, and this trimer will be present in Bowman’s capsule (BC), distal and collecting duct tubule basement membranes, and the epidermal basement membranes (EpiBM) in this type of AS affected patients.
In 80% of X-linked AS males, kidney basement membranes will exhibit complete absence or markedly reduced immunostaining of antibodies against α3, α4, and α5(IV) chains [6–8,12,14–17,19, 20,23]. The epider-mal basement membranes will be negative for antibody against the α5(IV) chain. Between 60 and 70% of X-linked AS females will have a mosaic pattern with both renal and epidermal basement membranes. Autosomal reces-sive AS results in GBMs being negative for antibodies against α3, α4, α5(IV) chains. Bowman’s capsule, distal and proximal tubule basement membranes, and epider-mal basement membranes will be positive for α5(IV) chains. With tubular basement membrane nephropathy, type IV collagen staining is normal in the kidney and skin. Also, it should be noted that autosomal dominant AS will have normal staining for type IV collagen chains in the kidney and skin. Normal type IV collagen stain-ing does not absolutely eliminate AS a diagnosis. In patients with hematuria, normal urine protein excretion, a negative family history of renal failure and extrarenal manifestation, and diffuse GBM thinning, normal type IV collagen staining support the diagnosis of TBMN (benign familial hematuria).
Molecular diagnostic tests (sequence analysis, dele-tion analysis, mutation scanning) can be performed because COL4A3, COL4A4, and COL4A5 genes have been sequenced. Identification of mutations in X-linked and autosomal recessive AS can be made quite fre-quently. Information regarding molecular diagnostic service may be found at www.genereviews.org.
natural History of as and tBmn renal disease
X-linked AS males will develop proteinuria, progres-sive renal insufficiency, and end-stage renal disease [7,8,10,12,15–19,21,25]. End-stage renal disease is reached by 60% at age 20 years and 90% by 40 years of age. The progression rate is influenced by the COL4A5 mutation type. By age 40 years, 80–90% will have sen-sorineural hearing loss. X-linked AS females develop end-stage renal disease to a lesser extent than their male counterparts. End-stage renal disease is reached by 12% by age 40 years, 30% at age 60 years, and 40% at age 80 years.
Molecular genetic findings have provided certain correlations with risk for disease manifestations in X-linked AS [6–8,20,21,23]. Large rearrangements and nonsense and frameshift mutations lead to ESRD in 50% by age 20 years and 90% by age 30 years. Splice-site mutations lead to ESRD in 50% by age 25 years and 70% by age 30 years. Missense mutations lead to ESRD in 50% by age 30 years. Nonglycine missense mutations and glycine mutations in the 3’ portion of COL4A5 lead to earlier ESRD than glycine missense mutations in the 5’ portion.
TBMN is characterized by persistent microscopic hematuria identified in childhood, but in some this may be intermittent and not detected until adult-hood [7–9,14,16,19,21,24]. The hematuria is lifelong. Upper respiratory infections may be associated with episodic gross hematuria. TBMN differs from AS in that (1) it rarely is associated with extrarenal mani-festations; (2) proteinuria, hypertension, and progres-sion to end-stage renal disease are unusual; and (3) both genders are affected. It should also be noted that TBMN may be seen in combination with several other glomerular diseases, including IgA nephropathy and FSGS.
treatment of as
The treatment of AS is directed toward controlling hypertension and proteinuria with angiotensin-con-verting enzyme (ACE) inhibitors [7,8,12,15,16,19,25]. The efficacy in slowing progression to end-stage renal disease with ACE inhibitors is uncertain. No therapy is required for TBMN, because this is a nonprogressive renal disease.
TABLE 7 Collagen type IV immunostaining in Alport syndrome (AS). GBM BC dTBM EpiBMNormal (males/females) α3, α4, α5(IV) chains Present Present Present Absent α5, α6(IV) chains Absent Present Present PresentX-linked AS males α3, α4, α5(IV) chains Absent Absent Absent Absent α5, α6(IV) chains Absent Absent Absent AbsentX-linked AS females α3, α4, α5(IV) chains Mosaic Mosaic Mosaic Absent α5, α6(IV) chains Absent Mosaic Mosaic MosaicAutosomal recessive AS (males/female)
α3, α4, α5(IV) chains Absent Absent Absent Absent α5, α6(IV) chains Absent Present Present PresentNote. GBM, glomerular basement membrane; BC, Bowman’s capsule; dTBM, distal tubule basement membrane; EpiBM, epidermal basement membrane.
Ultr
astr
uct P
atho
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f T
oron
to o
n 05
/04/
15Fo
r pe
rson
al u
se o
nly.

8 J. Hicks et al.
Ultrastructural Pathology
renal transplantation in as
Graft survivals in AS patients are similar to those for patients with ESRD due to congenital urinary tract anomalies [7,13,15,16,17,19,25]. Avoidance of a donation by an affected family member (female carrier) is impor-tant. The transplanted AS patient needs to be followed for development of post-transplant anti-GBM nephritis, especially during the first year. This condition affects up to 5–15% of transplanted AS patients, and may result in quite rapid graft loss. Surveillance includes frequent serum creatinine and serial monitoring for anti-GBM antibodies. The majority of patients who experience post-transplant anti-GBM nephritis have antibodies against the α5(IV) type IV collagen chain, but antibod-ies against α3(IV) and α4(IV) type IV collagen chains may develop depending on the AS type. Unfortunately, commercial ELISA testing has a low sensitivity to anti-α5(IV) antibodies. A negative ELISA test may not be reassuring in these patients. Most clinicians have a low threshold for a renal biopsy in these patients.
iga nePHroPatHy
epidemiology and Clinical Features
IgA nephropathy (IgAN) is the most common glom-erulonephritis throughout the world, with Japan and Korea having the highest prevalence [4,26–29]. In Japan, IgAN represents about 50% of newly diagnosed glom-erulonephritis cases and accounts for about 40% of end-stage renal disease cases. Interestingly, subclinical (cryptic) IgAN in Japan has been shown to be present on the basis of discovering that 16% of renal biopsies from living related kidney donors have IgAN. In con-trast, IgAN accounts for 10% of glomerulonephritis cases in the United States and 30% of cases in Western Europe. IgAN has a higher prevalence among Zuni and Manitoba Native Americans and Australian aborigines. It is uncommon in central Africa and the Indian sub-continent. It appears that there is certain genetic/ethnic predisposition to IgAN.
The peak incidence of IgAN is between the second and third decades [4,26–29]. There is a male predisposi-tion (2 M:1 F). Asymptomatic urine testing will identify 30–40% of patients with IgAN based on hematuria and lack of significant proteinuria. Renal biopsy findings in 50% of patients with asymptomatic hematuria who undergo biopsy result in a diagnosis of IgAN. The remainder are either normal or may have TBMN and less commonly AS. With IgAN, it is rare for proteinuria to be present in the absence of hematuria. Only 5% of IgAN patients have nephrotic syndrome; but when pres-ent, nephrotic syndrome is more common in children and adolescents. During the course of IgAN disease, there may be development of nephrotic-range proteinu-ria. Acute renal failure occurs in <5% of cases in 2 forms.
IgAN acute renal failure may occur due to acute severe immunologic and inflammatory injury resulting in cres-cent formation. This may be the primary presentation in some patients. IgAN acute renal failure can also occur due to heavy glomerular hematuria with mild glomeru-lar injury, but with tubular occlusion and severe tubular damage. This is a reversible type of injury and renal function recovers with supportive therapy.
Initial IgAN diagnosis of older patients is usually accompanied by proteinuria, renal dysfunction, and hypertension [4,26–29]. IgAN rarely presents with malignant hypertension. Such patients are presumed to have long-standing, undiagnosed IgAN that was not detected either due to lack of obvious hematuria or lack of routine urinalysis screening.
Clinical presentation is often associated with devel-opment of painless hematuria and may be concurrent with viral pharyngitis, gastroenteritis, or pneumonia [4,26–29]. About one-third of IgAN patients present with gross hematuria and renal dysfunction. Although about 40% of IgAN patients may experience transient renal failure and gross hematuria, the vast majority com-pletely recover their renal function. IgAN patients with intermittent gross hematuria tend to not develop pro-teinuria and have a good overall prognosis. Although IgAN is generally considered a “benign” glomeru-lonephritis, 20–40% of patients progress to end-stage renal disease within 20 years. From the first symptom presentation, it has been calculated that 1.5% of IgAN patients will reach ESRD per year. Clinical risk factors associated with progressive IgAN are hypertension, proteinuria >1.0 g/24 h, male gender, and persistent microscopic hematuria. IgAN also has a high recurrence rate (50–60%) in renal allografts (Table 8).
TABLE 8 IgAN prognostic markers at initial presentationClinical features Pathology featuresPoor prognosis Poor prognosis– Increased age – Light microscopy– Duration of symptoms – Capsular adhesions & crescents– Severity of proteinuria – Glomerulosclerosis– Hypertension – Tubular atrophy– Renal impairment –Interstitial fibrosis– Increased body mass index –Vascular wall thickening – ImmunofluorescenceGood prognosis – Capillary loop IgA deposits– Recurrent macroscopic
hematuria – Only IgA deposits
– Electron microscopy – MesangiolysisNo impact on prognosis – GBM abnormalities– Gender – Ethnicity Good prognosis– Serum IgA level – Minimal light microscopic
abnormalities No impact on prognosis – Intensity of IgA deposits – Co-deposition of IgG, IgM or C3
Ultr
astr
uct P
atho
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f T
oron
to o
n 05
/04/
15Fo
r pe
rson
al u
se o
nly.

Pediatric Renal Disease with Hematuria 9
© 2012 Informa Healthcare USA, Inc.
A genetic basis for IgAN is supported by link-based analyses of familial forms of the disease. Familial forms of IgAN account for 10–15% of cases [26–29]. Certain chro-mosomal loci have been identified in these familial forms (2q36, 3p24-23, 4q26-31, 6q22-23 [IGAN1], 17q12-22); however, no causal genes have been identified to date. Other candidates gene loci for IgAN include selectin E and L genes (SELE and SELL) at chromosomal locus 1q24-25. IgAN susceptibility variant alleles are polymeric Ig receptor gene (1q31-31), HLA-DRA (6p21.3), GNB3 (G protein β3 subunit, 12p13), IGHMBP2 (immunoglobu-lin μ-binding protein 2, 11q13.2-13.4), TNFα (6p21.3), IFNλ (12q14), TGFβ1 (19q13.1), C1GALT1, SCB1A1, and SERPINB7 (megsin, 18q21.3) genes. Single nucle-otide polymorphism (SNP) analyses (partial genome scan of 80,000 SNPs) have identified certain genes that are strongly associated with IgAN. These include PIGR (polymeric immunoglobulin receptor gene) and immuno-globulin μ-binding protein 2 (IGHMBP2, 11q13.2-13.4).
Pathology Findings
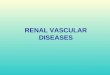
The hallmark of IgAN is mesangial deposition of IgA by immunofluorescence (Figure 4). IgA deposition in the mesangium is usually diffuse and global. IgA is occasionally seen in the capillary membranes, and this
is associated with a worse prognosis. IgA is the domi-nant or co-dominant immunoglobulin deposited. C3 is almost always present. IgG and IgM are frequently detected also. IgA as the only immunoglobulin present occurs in only about 15% of cases. Electron microscopy demonstrates the electron-dense deposits usually in a paramesangial, as well as mesangial distribution. Often even with diffuse IgA immunofluorescence, electron-dense deposits are difficult to identify. This is because the electron-dense deposits in the paramesangial regions may be subtle and blend in with the mesangial matrix, making their identification extremely difficult. Another complicating factor in identifying electron-dense deposits is the cyclical nature of this disorder and variation in the amount and extent of electron-dense deposits. Although the deposits in IgA nephropathy are classically described as paramesangial, deposits may be seen in the subendothelial locations, extending from the mesangial areas when capillary proliferation is present. This can also be seen as interposition. On occa-sion, subepithelial and/or intramembranous deposits may be present. The variability in ultrastructural find-ings emphasizes the need to correlate the light, immu-nofluorescence, and electron microscopic findings, as well as clinical features, in rendering a final diagnosis. Finally, thin glomerular basement membranes may also be present.
a
c
b
FIGURE 4 IgA nephropathy. (A) Typically, the kidney biopsy shows normal glomeruli and tubulointerstitial compartments (H&E). (B) Immunofluorescence demonstrates IgA reactivity with a mesangial pattern (direct immunofluorescence, IgA antibody). (C) Electron-dense deposits corresponding to the IgA reactivity are seen in a paramesangial and mesangial pattern in the glomeruli (transmission electron microscopy).
Ultr
astr
uct P
atho
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f T
oron
to o
n 05
/04/
15Fo
r pe
rson
al u
se o
nly.

10 J. Hicks et al.
Ultrastructural Pathology
The light microscopic appearance of IgAN is quite variable (Figures 4 and 5) [26,27]. The typical appear-ance in the pediatric age group is mesangial hypercellu-larity. Mesangioproliferation is most commonly diffuse and global, but may be focal and segmental. IgAN may be classified as no lesion by light microscopy, mesangio-proliferative (most common), focal proliferative (<50% of glomeruli), diffuse proliferative (>50% of glomeruli), crescentic, and chronic sclerosing. While there are sev-eral other classifications, this classification follows the WHO lupus nephritis system, and is easily understood by nephrologists.
Histopathologic features of poor prognosis in IgAN include (Table 8) [26,27] (1) cellular crescents, (2) endo-capillary proliferation, (3) karyorrhexis, (4) tubuloint-erstitial fibrosis, and (5) glomerulosclerosis. Crescents and endocapillary proliferation have been shown in certain clinical studies to correlate with hypertension at presentation, proteinuria (>1 g), and nephrotic-range proteinuria.
Pathogenesis of igan
IgAN is an immune complex disease process with mesangial deposition of dimeric and polymeric
IgA1 [4,26,27,30,31]. Glomeruli with the greatest amount of IgA deposits have the highest level of inflammatory infiltrates and mesangial proliferation. The mesangial deposits are predominantly polymeric IgA1 secondary to systemic overproduction of IgA1 polymers, possibly in response to infectious agents (such as IgA associated with hepatitic C). There is impaired clearance of the systemic IgA1 by hepatic and myeloid routes. CD89/Fc receptor is used as a method to isolate polymeric IgA1. Interestingly, mesangial cells express CD89/Fc and CD71 receptors, and these receptors may lead to the accumulation of IgA1 deposits. The interaction between IgA1 and CD89/Fc receptor may stimulate proinflam-matory cytokines that lead to mesangial matrix expan-sion and glomerular inflammation. IgAN is associated with increased serum levels of IgA1 in about 50% of affected patients. Serum complement levels are normal, and complement activation is restricted to the kidneys alone.
In addition, abnormal glycosylation of IgA1 occurs and leads to polymeric IgA1 complexes with reduced glycosylation at the hinge region of the molecule [26,27,30,31]. This results in high avidity for binding to mesangial cells. The resultant polymeric IgA1 is more prone to self-aggregation, generation of macro-molecular polymeric IgA1 aggregates, and formation
a
c
b
d
FIGURE 5 IgA nephropathy, variable patterns. (A) Distinct lobular mesangial cellularity and increased mesangial matrix may be seen (PAS stain). (B) Cellular proliferative crescents and tubular atrophy with cast material may also be present (H&E). (C) Immunofluorescence demonstrates an IgA dominant pattern of reactivity (direct immunofluorescence, IgA antibody). (D) Readily identified mesangial and paramesangial electron-dense deposits are present (transmission electron microscopy).
Ultr
astr
uct P
atho
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f T
oron
to o
n 05
/04/
15Fo
r pe
rson
al u
se o
nly.

Pediatric Renal Disease with Hematuria 11
© 2012 Informa Healthcare USA, Inc.
of immune complexes (antigen-antibody complexes with IgG), especially in the mesangium. The lack of glycosylation of serine and threonine near the hinge region of the IgA1 molecule with oligosaccharides (Gal Nac, NANA) is responsible for the polymeric IgA1 complexes that deposit in the mesangium. In addition, IgA1 that lacks terminal sialic acid and galactose units have a high affinity for the extracellular matrix com-ponents fibronectin and type IV collagen, resident in the glomerulus.
Enzymatic removal of all complex oligosaccharides from the hinged region of the IgA molecule from normal individuals significantly enhances mesangial deposition [26,27,30,31]. It has been shown that IgA molecules defi-cient in NANA or Gal Nac are present in the serum of IgAN patients with proliferative disease. Quantitative analyses of kidney biopsies have reported reduced gly-cosylation levels of IgA in patients with active IgAN compared to those with inactive IgAN. It has also been shown that the amount of Gal Nac-deficient IgA1 in the kidney is significantly higher than in the serum of IgAN patients.
It has been proposed that specific glycosyltrans-ferases responsible for the O-glycosylation of IgA1 may have functional abnormalities that lead to the lack of or reduced glycosylation seen in IgAN [26,27,30,31]. β-1-3-Galactosyltranferase (7p14-p13) is a key enzyme that catalyzes the addition of galactose to O-linked glycans. This enzyme has a functional defect in peripheral blood B lymphocytes, tonsillar lymphocytes, and mesangial cells in patients with IgAN. The molecular chaperone of this enzyme (Cosmc, Xq23) may also be a factor in IgAN. Significantly decreased serum mRNA levels of Cosmc have been reported in peripheral blood B cells in IgAN. It is interesting to note that Cosmc lies on the X chromosome, and males are more commonly affected with IgAN.
Reduction in glycosylation at the hinge region of IgA results in the formation of a neoantigen, which allows for formation of IgG autoantibodies against Gal Nac-deficient IgA [26,27,30,31]. This leads to IgG autoantibodies, in addition to Gal Nac-deficient IgA, binding to the CD89/Fc receptor expressed by the mesangial cells. This in turn results in the pro-duction of proinflammatory cytokines, recruitment of circulating inflammatory cells, inflammatory and growth factors, and extracellular matrix components by mesangial cells. Polymeric IgA has been shown to activate the alternate complement pathway via mannose-binding lectin, leading to an additional mechanism to recruit an inflammatory response. Of note is that IgA complexes resolve when donor kid-neys from IgAN patients are transplanted into non-IgAN patients requiring kidney transplantation. This finding supports the idea that the mesangial immune complex deposits are a result of deposition from extra-renal sources, rather than intrarenal or glomerular in situ synthesis.
treatment of igan
There is no specific treatment required for patients with isolated hematuria and minimal to no proteinu-ria [4,26,27,30,31]. Long-term surveillance is required in these patients for assessment of disease progres-sion. Proteinuria of >1 g/24 h is a threshold to identify IgAN patients who are at higher risk for progression. Clinical treatment, as well as entry into clinical trials, is typically based on presence of hypertension, proteinuria 1–3 g/24 h, and reduction in glomerular filtration rate. Treatment for hypertension is usually with medications directed toward the renin–angiotensin system (ACE inhibitors). Treatment of progressive IgAN is targeted toward interfering with the immune and inflammatory processes with corticosteroids, cyclophosphamide, and mycophenolate. Immunosuppressive therapy is desig-nated for sustained proteinuria. Although the initial clinical trial with fish oil supplements demonstrated benefits, subsequent studies failed to show any benefit in treating IgAN. Renal transplantation is performed for those who reach end-stage renal disease. Recurrence of IgAN in the transplanted kidney does occur at a rate of 7–30%. The rate of graft loss after 5–10 years ranges from 3 to 16%.
evolving diagnostic tests for igan
Recently, there have been investigations into tests that may be helpful in diagnosis of IgAN and Henoch-Schönlein Purpura nephritis (HSPN) before a renal biopsy is performed [32]. These include identifying a urinary proteomic pattern and measurement of galactose-deficient IgA1 in serum. A specific IgAN pattern of urinary polypeptide excretion has been detected by capillary electrophoresis coupled with mass spectrometry. Using this diagnostic technique, IgAN patients could be distinguished from normal controls (100% sensitivity, 90% specificity) and from patients with membranous glomerulonephritis (77% sensitivity, 100% specificity). The IgAN pattern has also been identified in pediatric age groups with IgAN and HSPN. Patients with IgAN due to hepatitis C lacked the IgAN pattern.
Serum galactose-deficient IgA1 (Gal-D IgA1) may be detected using a specific lectin-binding assay [26,27,30]. This assay can distinguish IgAN and HSP compared with normal controls and non-IgAN chronic glom-erulonephritis in both adult and pediatric age groups. Of interest is the finding that the serum Gal-D IgA1 levels were not elevated in children with HSP without nephritis or with acute poststreptococcal glomerulo-nephritis compared with normal controls. IgAN and HSPN patients with a current episode of macroscopic hematuria had the highest levels of Gal-D IgA1. IgAN and HSPN patients with no hematuria had the lowest levels among the IgAN group.
Ultr
astr
uct P
atho
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f T
oron
to o
n 05
/04/
15Fo
r pe
rson
al u
se o
nly.

12 J. Hicks et al.
Ultrastructural Pathology
HenoCH-sCHönlein PurPura renal disease: systemiC Form oF iga
nePHroPatHy
epidemiology and Clinical Features
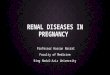
Henoch-Schönlein purpura (HSP) is a systemic disease due to vasculitis involving small vessels (Figure 6) [4,33–39]. Most commonly, HSP affects children between the ages of 3 and 10 years, with 50% of cases occurring before age 5 years. There is a male predisposition (2 M:1 F). The inci-dence of HSP is reported to be 1–2 per 10,000. The clinical manifestations include purpuric skin lesions, abdominal pain, gastrointestinal bleeding, arthropathy, and renal involvement. The most serious long-term complication of HSP is renal involvement, with about one-third of all HSP cases having renal manifestations. This results in isolated hematuria and/or proteinuria in 80% of such cases, and acute nephritis or nephrotic syndrome in 20% of such cases. When renal complications are present, they occur early in the course of HSP (85% by week 4). Persistent renal involvement with hypertension, reduced renal func-tion and nephrotic or nephritic syndrome is seen in 5% of children with isolated hematuria and/or proteinuria and in 20% of children with acute nephritis and/or nephrotic syndrome. Typically, HSP occurs after an upper respiratory infection and is more common from fall through spring.
HSP presents as a classic tetrad: (1) purpuric rash, (2) polyarthralgia, (3) abdominal pain, and (4) renal disease [4,33–38]. The rash is palpable and nonblanching and persists for 3–10 days. The most common sites are the extremities. In children, angioedema may precede the rash. Polyarthralgia occurs in 80% of HSP patients and most commonly involves the knees and ankles. This resolves after a few days. Abdominal pain occurs in about 50% of patients, has a colicky nature, and devel-ops within 1 week of the rash. Nausea, vomiting, and diarrhea with passage of blood and mucus are common gastrointestinal manifestations. Renal disease is seen in 40–50% and is associated with microscopic hematuria, red blood cell casts in the urine, and proteinuria. The
renal symptoms resolve in most cases. As noted pre-viously, about 5% will have progressive renal disease with development of end-stage renal disease in 1% of children with HSP. With HSP in adults, renal involve-ment occurs in 50–80% and progression to renal failure (ESRD) occurs in 10–20%. The most common cause of death is attributed to renal failure (Table 9).
Diagnosis is based on clinical recognition of the HSP tetrad, while eliminating other autoimmune dis-eases (lupus, vasculitis, juvenile rheumatoid arthritis) (Table 10) [4,33,35,37,38]. With HSP, there is only mild leukocytosis with occasional eosinophilia and a normal platelet count. Throat culture for group A hemolytic streptococcus is positive in 10–30%. ASO titers are ele-vated in 20–50%. Although a substantial proportion of children with HSP have evidence for a recent or concur-rent group A hemolytic streptococcal infection, most do not. Elevated serum IgA levels are noted in about 50% of patients. The American Academy of Rheumatology has criteria for HSP diagnosis that include (1) palpable pur-pura, (2) age <20 years at onset of symptoms, (3) bowel angina, and (4) granulocytes in the wall of arterioles or
a b
FIGURE 6 Henoch-Schönlein purpura skin biopsy. (A) Perivascular inflammatory infiltrates involve the superficial and upper dermis (H&E). (B) There is leukocytoclastic vasculitis that is associated with IgA deposits in the vessel walls (H&E).
TABLE 9 Long-term kidney survival rates in pediatric IgA and HSP nephritis
5-year
survival10-year survival
20-year survival
IgA nephritis 94–100% 87–95% 70–89%HSP nephritis 82–95% 78–90% 68–80%
TABLE 10 Clinical manifestations of HSP: comparison of chil-dren vs. adults Children AdultsM:F ratio 1.5 M:1.0 F 1.6 M:1.0 FPurpura 100% 100%Arthritis 70% 62%GI Involvement 66% 46%Renal Involvement 37% 72%Microscopic hematuria 15% 10%Macroscopic hematuria 34% 22%Proteinuria 64% 55%
Ultr
astr
uct P
atho
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f T
oron
to o
n 05
/04/
15Fo
r pe
rson
al u
se o
nly.

Pediatric Renal Disease with Hematuria 13
© 2012 Informa Healthcare USA, Inc.
venules on biopsy. HSP is diagnosed when 2 of the 4 criteria are met (87% sensitivity and specificity).
Other infectious agents reported in association with HSP include Bartonella henselae, Staphylococcus aureus, Helicobacter pylori, Haemophilus parainfluenza, parvovi-rus B19, coxsackie virus, adenovirus, hepatitis A, and hepatitis B [4,33–39]. The association of HSP and IgAN with infectious agents may be due to (1) molecular mimicry with microbes sharing epitopes with human small vessel endothelial cells; (2) bystander activation with pathogen induction of nonspecific inflammation leading to cell injury that reveals sequestered antigens; (3) self-alteration with microbial interaction with ves-sel proteins that result in neoantigen production; and (4) superantigens associated with certain bacteria and viruses that interact and active T cells.
Spontaneous resolution occurs in 95% of children and in 80% of adults [4,34,35,37,38]. About two-thirds of children will resolve HSP within 4 weeks of onset of signs and symptoms. Younger children will have a shorter course and experience fewer recurrences than older patients. At least one HSP recurrence will be noted in 40–60% of patients, and this usually consists of rash and abdominal pain. Recurrence can occur up to 7 years after initial diagnosis. The overall prognosis tends to be good. Forty-four percent of HSP patients who present with nephritic or nephrotic syndrome have hypertension or impaired renal function at long-term follow-up. In comparison, normal renal function is seen in long-term follow-up in 82% of those who present with hematuria with or without mild proteinuria. Long-term follow-up is important because renal failure and hypertension may develop up to 10 years after initial diagnosis. Children who have experienced HSP account for 10% of patients entering into end-stage disease programs.
Pathology Findings
The glomerular pathology is indistinguishable from iso-lated IgA nephropathy as described previously (Figure 7) [35–38]. The most common finding is focal and segmental proliferative glomerulonephritis (60%). Crescents are pres-ent in 40% of biopsies, with 80% of these biopsies show-ing less than 50% of glomeruli with crescents. Interstitial inflammation and fibrosis may also be present and cor-relate with degree of glomerular involvement. Vasculitis in extraglomerular renal vessels is relatively rare, but when it occurs it affects arterioles. The skin lesions in HSP are characterized by leukocytoclastic vasculitis, primar-ily affecting vessels in the upper dermis (Figure 6). IgA deposits are identified within the vessel walls.
Pathogenesis of HsP
The pathogenesis is linked to a variety of IgA abnormali-ties, including (1) increased serum IgA concentration,
(2) IgA circulating immune antigen–antibody complexes, and (3) IgA deposition in vessel walls and renal mesan-gium [4,34–39]. The previous discussion of pathogen-esis of IgAN applies to HSP, as well. There are certain differences between IgAN and HSP with respect to the alterations in IgA1 glycosylation [37,39]. Particularly in children with HSP, it has been shown that the hinge region of IgA1 is deficient in sialic acid, as well as Gal and GalNac. In fact, it has been reported that levels of GalNac-deficient IgA1 and Gal-deficient IgA1 are decreased in patients with HSP nephritis, but there is no difference in IgA1 glycosylation in HSP patients with no nephritis compared with controls.
treatment of HsP
Treatment in HSP is dependent on the extent of disease [4,33,35–38]. With mild symptoms such as rash, mild edema, and arthritis, only supportive care is necessary with possible addition of NSAIDs for arthritis manage-ment. Short-term oral corticosteroids may be used to treat rashes with severe edema, severe colicky abdominal pain, and scrotal or testicular involvement. Intravenous corticosteroids may be instituted for abdominal pain associated with nausea and vomiting and nephrotic range proteinuria. Corticosteroids with immunosup-pressive drugs and plasmapheresis are usually reserved for rapidly progressive glomerulonephritis (crescentic glomerulonephritis) or pulmonary hemorrhage.
Treatment for severe renal involvement may include the following: high-dose corticosteroids either alone or in combination with immunosuppressive drugs (aza-thioprine, cyclophosphamide, cyclosporine); high-dose IV immunoglobulin; plasma exchange/plasmapheresis; corticosteroids with urokinase and warfarin; and even renal transplantation [33,35–38]. It should be noted that corticosteroid therapy does not prevent renal disease progression. Renal biopsy is crucial in assessing the degree of renal involvement and to guide therapy.
Allograft kidneys transplanted for ESRD in HSP patients develop IgAN in about one-third of cases within 5 years [33,35–38]. There is no recurrence of sys-temic vasculitis in these patients. Graft failure will occur in about one-third of those who develop recurrent IgAN in their transplants.
aCute PostinFeCtious GlomerulonePHritis
epidemiology and Clinical Features
Acute postinfectious glomerulonephritis (APIGN) most frequently affects children and is less common in adults (Table 11) [4,40–47]. Most cases occur in 2- to 12-year-old children (80–85%), with the remainder in adults over 40 years of age (5–10%) and children under 2 years of age
Ultr
astr
uct P
atho
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f T
oron
to o
n 05
/04/
15Fo
r pe
rson
al u
se o
nly.

14 J. Hicks et al.
Ultrastructural Pathology
(5%). Most cases of APIGN follow an upper respiratory or cutaneous infection caused by nephritogenic strains of group A beta-hemolytic streptococci (Table 12). In adults, the most frequently associated pathogens are staphylococci and gram-negative organisms. There is a male predilection (2–3 M:1 F). Predisposing factors
a
c
b
d
e
FIGURE 7 Henoch-Schönlein purpura kidney biopsy. (A) Glomerulus with mild increase in mesangial cells (H&E). (B) Glomerulus with mesangiocapillary proliferation with an accentuated lobular pattern (PAS stain). (C) Glomeruli demonstrating segmental (left) and crescentic (right) lesions with a certain degree of interstitial fibrosis (H&E). (D) Mesangial and membranous IgA detected by immuno-fluorescence (direct immunofluorescence, IgA antibody). (E) Electron-dense deposits expand the mesangial region, corresponding to the IgA reactivity identified on immunofluorescence (transmission electron microscopy).
TABLE 11 Acute postinfectious glomerulonephritis: epidemiology Children AdultsIncidence Less-developed countries 24.3/100,000 2.0/100,000 More-developed countries 0.6/100,000 0.3/100,000
Ultr
astr
uct P
atho
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f T
oron
to o
n 05
/04/
15Fo
r pe
rson
al u
se o
nly.

Pediatric Renal Disease with Hematuria 15
© 2012 Informa Healthcare USA, Inc.
of APIGN in adults include alcoholism, immunosup-pression, intravenous drug use, chronic illnesses, and diabetes. It should be noted that there has been a decline
in APIGN over the past several decades in industrial-ized countries.
APIGN occurs as an acute nephritic syndrome with sudden onset of edema, hematuria, proteinuria, and hypertension [4,40–47]. The differential diagnostic considerations include those entities listed in Table 13. Serologic evidence should be sought in suspected cases of APIGN, because serologic evidence is more sensitive (94.6%) than a history of recent infection (75.7%) or a positive culture (24.3%).
APIGN tends to be a self-limiting disease that has complete resolution in over 90% of children. In adults, 25% have long-term renal sequelae [4,40–47]. Mortality from APIGN is about 1% and 2% progress to end-stage renal disease, with most being adults. Elderly adults with debilitating conditions (malnutrition, diabetes, chronic illness, alcoholism) and APIGN have a high inci-dence of azotemia (60%), congestive heart failure (40%), and nephrotic-range proteinuria (20%). Death may occur in 20–25% of these patients. In elderly patients with per-sistent proteinuria, 77% develop chronic renal failure. Recent clinical studies have followed children 15–18 years after the acute episode of APIGN in Venezuela [46]. The following were noted: 13.7% with hyperten-sion, 7.2% with albuminuria, 5.4% with hematuria, and 0.9% with increased serum creatinine.
Pathology Findings
The most common pattern of APIGN is acute diffuse proliferative glomerulonephritis (Figure 8) [42,44–46]. This is characterized by numerous neutrophils in glomerular capillaries and endocapillary hypercel-lularity affecting all glomeruli. Crescents are present in the most severe cases, but typically affect less than 50% of glomeruli in the biopsy specimen. Segmental necrosis and capillary thrombosis are uncommon. Trichrome staining may identify large subepithelial immune deposits (subepithelial humps) that are char-acteristic for APIGN. Tubulointerstitial changes in the
TABLE 13 Differential diagnosis of acute glomerulonephritisLow serum complement Normal serum complement
Systemic diseasesSystemic lupus erythematosus Polyarteritis nodosa groupSubacute bacterial endocarditis Hypersensitivity vasculitisVisceral abscess/osteomyelitis Wegener granulomatosisShunt (CSF) nephritis Henoch-Schönlein purpuraCryoglobulinemia Goodpasture syndrome
Renal diseasesAcute postinfectious glomerulonephritis
IgA Nephropathy
Membranoproliferative glomerulonephritis
Rapidly progressive glomerulonephritis
Type I Anti-GBM disease Type II Negative immunofluorescence Immune complex disease
TABLE 12 Infections associated with acute postinfectious glomerulonephritisInfectious syndromes
Skin & throat infections (Streptococcus pyogenes, equi, & constellatus)
Bacterial endocarditis (Staphylococcus aureus & viridans)Pneumonia (Streptococcus pneumoniae, Mycoplasma
pneumoniae)Visceral abscess (dental, deep-seated, osteomyelitis)Shunt nephritis (Staphylococcus epidermidis,
Propionibacterium)Specific bacterial disease
Gram-positive bacteria(Streptococci, Staphylococci, Pneumococci, Enterococci,
Listeria moncytogenes)Gram-negative bacteria (Meningococcus, Neisseria
gonorrhea)Gram-negative coccobacillus (Haemophilus)Gram-negative bacilli
(Salmonella, Klebsiella, Serratia, Yersinia, Proteus, Pseudomonas)
Others (Legionellosis, Brucellosis, Bartonellosis)Mycobacterial, rickettsial, mycoplasmal, chlamydial & spirochetal diseases
Tuberculosis and nontuberculous mycobacterial infectionsSyphilis (Treponema pallidum)Leptospirosis (Leptospira interrogans)Rickettsial diseases (Coxiella burnetti)Mycoplasma pneumoniaeChlamydia pneumoniae
Fungal InfectionsCandida albicansHistoplasma capsulatumCoccidioides immitis
VirusesDNA viruses
Hepatitis B virusHerpesvirus (VZV, EBV, CMV)Parvovirus B19Adenovirus
RNA virusesRetrovirus (HIV)Picornavirus (coxsackievirus, echovirus, hepatitis A virus)Flavivirus (denge virus, measles virus)Paramyxovirus (mumps virus, measle virus)Bunyavirus (hantavirus)Reovirus (rotavirus)
Parasitic infestationsMalariaSchistosomiasisToxoplasmosisFiliariasisTrichinosisHydatid disease (Echinococcus)Ameoebiasis (Entamoeba)
Ultr
astr
uct P
atho
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f T
oron
to o
n 05
/04/
15Fo
r pe
rson
al u
se o
nly.

16 J. Hicks et al.
Ultrastructural Pathology
early phase may be only slight edema and mild peri-glomerular mononuclear infiltrates. In severe cases, there will be a greater degree of edema and inflamma-tory infiltrates, including neutrophils. Tubules often contain red blood cells and occasional neutrophils. Immunofluorescence will reveal coarse granular staining of the glomerular basement membranes and the large subepithelial deposits (humps) with C3 and minor staining with IgG and IgM. The staining pattern may be starry sky-like, garland-like, or mesangial. During the acute phase of APIGN, electron micros-copy reveals large subepithelial deposits (humps) that are characteristic for APIGN. These hump-shaped sub-epithelial deposits tend to be scattered throughout the glomerulus and overlying the glomerular basement membrane. There typically is no reaction or appar-ent change in the adjacent surrounding or underlying basement membrane to the hump-shaped deposits. In addition, scattered areas of subendothelial, subepi-thelial, and mesangial deposits may be present. If a renal biopsy is performed at a later stage of APIGN, classic hump-like deposits are rare. There may be only somewhat resorbed hump-like deposits in the sub-epithelium overlying mesangium. These hump-like deposits have been referred to as “notch” or “waist areas,” resembling the indentation seen with a notch
in the waist area of a belt buckle. With chronic APIGN, deposits are predominantly mesangial with less evi-dent endocapillary proliferation and inflammation. The glomeruli may have only mesangial proliferation or focal membranoproliferative features. Extensive searching for rare partially resorbed hump-like sub-epithelial deposits is helpful in rendering an accurate diagnosis of chronic phase APIGN. Careful attention for MPGN-dense deposit disease should be exercised, since subepithelial humps may occur with this type of MPGN in children as well.
Pathogenesis of aPiGn
The development of APIGN is a complex process that involves cellular immune mechanisms, complement activation, and various nephritogenic bacterial fac-tors [4,40,43–47]. In the early phase of APIGN, mac-rophages and T cells infiltrate the glomeruli in response to chemotactic factors from the complement system. Complement pathway activation occurs via Ig-binding proteins in the streptococcal surface. These Ig-binding proteins interact with C4bP (a C4b-binding protein), extracellular cationic cysteine proteinase (streptococ-cal pyrogenic exotoxin b [SpeB]), and FH and FHL-1
a
d
b
c
FIGURE 8 Acute post-infectious glomerulonephritis. (A) Diffuse mesangiocapillary proliferation with occasional neutrophils noted in the glomerular capillaries (H&E). (B) C3 in a coarse granular pattern highlights the glomerular basement membranes in a garland or starry-sky pattern (direct immunofluorescence, C3 antibody). (C, D) Electron microscopy demonstrates frequent large subepithelial deposits (humps), a hallmark for acute postinfectious glomerulonephritis (transmission electron microscopy).
Ultr
astr
uct P
atho
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f T
oron
to o
n 05
/04/
15Fo
r pe
rson
al u
se o
nly.

Pediatric Renal Disease with Hematuria 17
© 2012 Informa Healthcare USA, Inc.
complement regulatory proteins used for immune eva-sion by streptococci.
The glomeruli and tubulointerstitial regions in APIGN overexpress ICAM-1 and LFA-1, resulting in infiltration by mononuclear cells [40,44,45]. There are also increased levels of IL-6, IL-8, TNFα, and MCP1, which correlate with proteinuria and urinary MCP1 excretion. Infiltrating inflammatory cells play an impor-tant role in the severity of glomerular damage, and the number of leukocytes within the glomeruli correlates with proteinuria.
Nephritogenic streptococci have several factors that participate in the pathogenesis of APIGN (Table 14) [4,40,43–47]. The nephrogenicity of streptococcal NAPlr-GADPH (nephritis-associated plasmin receptor) may be related to its plasmin-binding activity, which in turn induces an inflammatory reaction and glomerular basement membrane degradation via collagenase and matrix metalloproteinase activation. NAPlr-GADPH (nephritis-associated plasmin receptor) colocalizes with plasmin in the glomerulus, but not with IgG or complement. zSpeB/SpeB (zymogen precursor of streptococcal pyogenic exotoxin) may induce immune complex-mediated glomerulonephritis, as SpeB colocal-izes with complement and IgG within the mesangial deposits. SpeB is present in the characteristic subepi-thelial “hump” deposits in APIGN. SpeB, enolase, and streptokinase also bind plasmin similar to NAPlr. Host factors are also important factors in the development of APIGN (HLA-DRW4, HLA-DRB1*03011, eNOS4a/b). A substantial proportion (20–40%) of siblings of patients with sporadic APIGN develop clinical or subclinical nephritis. This familial tendency may be due to “shar-ing” of an infectious agent, as well as the similarity of host factors in family members.
treatment Guidelines for nephritogenic streptococcal infections
A scoring system for streptococcal pharyngitis has been developed (McIsaac score) to increase the accuracy of diagnosis and guide antibiotic prescription [40,42,47]. This has been developed because only 10–20% of patients who present with pharyngitis have a positive group A streptococcal culture. Typically, clinicians may not recognize about 50% of cases and misdiagnosis 20–40% of all pharyngitis as streptococcal in origin. The McIsaac score gives 1 point for each of the following criteria: >38°C temperature; no cough; tender anterior cervical adenopathy; tonsillar swelling or exudates; and age between 3 and 14 years. The sensitivity and specificity for a correct diagnosis are 85 and 92%, respectively. Antibiotic prescription is indicated for a score of 4. Antibiotic prescription is not recommended for a score of 0 or 1. A score of 2 or 3 requires that a culture be obtained and antibiotic treatment initiated if the culture is positive. Patients with APIGN should be treated as if they have an active streptococcal infec-tion. Not only does this treat the affected patient, but it also avoids infecting other household members and close contacts. It has been shown that a milder clinical course may occur with APIGN if antibiotics have been prescribed.
summary
This brief tutorial on pediatric renal disease associ-ated with hematuria illustrates the spectrum of enti-ties that may occur in the pediatric age group as a manifestation of microhematuria and macrohematuria. The spectrum of disease includes familial hematuria (Alport syndrome [hereditary nephritis]) thin basement membrane nephropathy), IgA nephropathy (IgAN), Henoch-Schönlein purpura (HSP), and acute postin-fectious glomerulonephritis (APIGN). Integration of clinical signs and symptoms, biopsy findings from light, immunofluorescence, and electron microscopy, and molecular genetics features (in certain entities) are critical in rendering an accurate diagnosis. It is impor-tant to recognize that certain pediatric renal diseases may have overlapping features and that with exten-sive and detailed examination of the ultrastructure an appropriate diagnosis may be made. Also, depending on whether the biopsy is performed during an early or later stage of the disease, the ultrastructure may become altered and require more intense evaluation of electron microscopic features in order to reveal the underlying disease.
Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
TABLE 14 Streptococcal nephritogenicityMolecular mimicry
Cross-reactivity with streptococcal products and laminin, collagen, GBM, vimentin, and mesangial proteins
Anti-Ig reactivityStreptococcal neuraminidaseStreptococcal Ig-binding receptors
Streptococcal-related glomerular plasmin-binding activityStreptokinasezSpeB/SpeB (zymogen precursor of streptococcal pyogenic
exotoxin B)EnolaseNAPlr-GADPH (nephritis associated plasmin receptor)
Streptococcal nephritogenic antigensM proteinHistone-like proteinsNAPlr-like proteinszSpeB/SpeB
Host factorsHLA-DRW4HLA-DRB1*03011eNOS4a/b
Ultr
astr
uct P
atho
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f T
oron
to o
n 05
/04/
15Fo
r pe
rson
al u
se o
nly.

18 J. Hicks et al.
Ultrastructural Pathology
reFerenCes
1. Beck L, Salant D: Glomerular and tubulointerstitial diseases. Prim Care Clin Office Pract. 2008;35:265.
2. Meyers K: Evaluation of hematuria in children. Urol Clin N Am. 2004;559.
3. Quigley R: Evaluation of hematuria and proteinuria: how should a pediatrician proceed? Curr Opin Ped. 2008;20:140.
4. Vinen C, Oliveira: Acute glomerulonephritis. Postgrad Med J. 2003;79:206.
5. Youn T, Trachtman H, Gauthier B: Clinical spectrum of gross hematuria in pediatric patients. Clin Pediatr. 2006;45:135.
6. Borza D, Hudson B: Molecular characterization of the target antigens of anti-glomerular basement membrane antibody disease. Semin Immunopathol. 2003;24:345.
7. Carasi C, Van’t Hoff W, Rees L, Risdon R, Trompeter R, Dillon M: Childhood thin GBM disease: review of 22 children with family studies and long-term follow-up. Pediatr Nephrol. 2005;1098.
8. Gubler M: Inherited diseases of the glomerular basement membranes. Nat Clin Pract Nephrol. 2008;4:24.
9. Gross O: Understanding renal disorders as systemic diseases: the fascinating world of basement membranes beyond the glomerulus. Nephrol Dial Transplant. 2008;23:1823.
10. Heidet L, Gubler M: The renal lesions of Alport syndrome. J Am Soc Nephrol. 2009;20:1210.
11. Haas M: Alport syndrome and thin basement membrane nephropathy: a practical approach to diagnosis. Arch Pathol Lab Med. 2009;133:224.
12. Hudson B, Tryggvason K, Sundaramoorthy M, Neilson E: Alport’s syndrome, Goodpasture’s syndrome, and type IV collagen. N Engl J Med. 2003;348:2543.
13. Ivanyi B: A primer on recurrent and de novo glomerulone-phritis in renal allografts. Nat Clin Pract Nephrol. 2008;4:446.
14. Ivanyi B, Pap R, Ondrik Z: Thin basement membrane neph-ropathy. Arch Pathol Lab Med. 2006;130:1533.
15. Kashtan C: Alport syndrome and thin glomerular basement membrane disease. J Am Soc Nephrol. 1998;9:1736.
16. Kashtan C: Familial hematurias: what we know and what we don’t know. Pediatr Nephrol. 2005;20:1027.
17. Kashtan C: Renal transplantation in patients with Alport syn-drome. Pediatr Transplant. 2006;10:651.
18. Kashtan C: Alport syndrome and the X chromosome: implica-tions of a diagnosis of Alport syndrome in females. Nephrol Dial Transplant. 2007;22:1499.
19. Kashtan C: Familial hematuria. Pediatr Nephrol. 2009; 24:1951.
20. Khoshnoodl J, Pedchenko V, Hudson B: Mammalian collagen IV. Microsc Res Tech. 2008;71:357.
21. Kwoh C, Shannon M, Miner J, Shaw A: Pathogenesis of nonimmune glomerulopathies. Annu Rev Pathol Mech Dis. 2006;1:349.
22. Lajoie G: Approach to the diagnosis of thin basement mem-brane nephropathy in females with the use of antibodies to type IV collagen. Arch Pathol Lab Med. 2001;125:631.
23. McKnight A, Currie D, Maxwell A: Unravelling the genetic basis of renal diseases from single gene to multifactorial dis-orders. J Pathol. 2010:220:198.
24. Savige J, Rana K, Tonna S, Buzza M, Dagher H, Wang Y: Thin basement membrane nephropathy. Kidney Int. 2003;64:1169.
25. White R, Raafat F, Milford D, Komianou F, Moghal N: The Alport nephropathy: clinicopathological correlations. Pediatr Nephrol. 2005;897.
26. Barratt J, Feehally J: IgA nephropathy. J Am Soc Nephrol. 2005;16:2088.
27. Tumlin J, Madaio M, Hennigar R: Idiopathic IgA nephropa-thy: pathogenesis, histopathology, and therapeutic options. Clin J Am Soc Nephrol. 2004;2:1054.
28. Beerman I, Novak J, Wyatt R, Julian B, Gharavi A: The genet-ics of IgA nephropathy. Nat Clin Pract Nephrol. 2007;3:325.
29. Maxell P, Wang Y: Genetic studies of IgA nephropathy. Nephron Exp Nephrol. 2006;102;e76.
30. Barratt J, Smith A, Feehally J: The pathogenic role of IgA1 O-linked glycosylation in the pathogenesis of IgA nephropa-thy. Nephrology. 2007:12:275.
31. Barratt J, Smith A, Molyneux K, Feehally J: Immunop-athogenesis of IgAN. Semin Immunopathol. 2007;29:427.
32. Julian BA, Wittke S, Haubitz M, et al. Urinary biomarkers of IgA nephropathy and other IgA-associated renal diseases. World J Urol. 2007;25:467.
33. Chartapisak W, Opastiraku S, Willis I, Craig J, Hodson E. Prevention and treatment of renal disease in Henoch-Schönlein purpura: a systematic review. Arch Dis Child. 2009;94:132.
34. Fervenza F: Henoch-Schonlein purpura nephritis. Int J Dermatol. 2003;42:170.
35. Roberts P, Waller T, Brinker T, Riffe I, Sayre J, Bratton R: Henoch-Schönlein purpura: a review article. South Med J. 2007:100:821.
36. Samarkos M, Loizou S, Vaiopoulos G, Davies K: The clinical spectrum of primary renal vasculitis. Semin Arthritis Rheum. 2005;35:95.
37. Sanders J, Wyatt R: IgA nephropathy and Henoch-Schönlein purpura nephritis. Curr Opin Pediatr. 2008;20:163.
38. Saulsbury F: Epidemiology of Henoch-Schönlein purpura. Cleveland Clin J Med. 69(Suppl II):S11.
39. Yang Y, Chuang Y., Wang L, Huang H, Gershwin M., Chiang B: The immunobiology of Henoch-Schönlein purpura. Autoimmun Rev. 2008;7:179.
40. Ahn S, Ingulli E: Acute poststreptococcal glomerulonephritis: an update. Curr Opin Pediatr. 2008;20:157.
41. Carapetis J, Steer A, Weber K: The global burden of group A streptococcal diseases. Lancet. 2005;5:685.
42. Kanjanabuch T, Kittikowit W, Elam-Ong S: An update on acute postinfectious glomerulonephritis worldwide. Nat Rev Nephrol. 2009;5:259.
43. Nasr S, Markowitz G, Stokes M, Said S, Valeri A, D’Agati V: Acute postinfectious glomerulonephritis in the modern age: experience with 86 adults and review of the literature. Medicine. 2008;87:21.
44. Nordstrand A, Norgren M, Holm S: Pathogenic mechanism of acute post-streptococcal glomerulonephritis. Scand J Infect Dis. 1999;31:523.
45. Rodriguez-Iturbe B, Batsford S: Pathogenesis of poststrep-tococcal glomerulonephritis a century after Clemens von Pirquet. Kidney Int. 2007:71:1094.
46. Rodriguez-Iturbe B, Musser J: The current state of poststrep-tococcal glomerulonephritis. J Am Soc Nephrol. 2008;19:1855.
47. Yoshizawa, N: Acute glomerulonephritis. Int Med. 2000; 39:687.
Ultr
astr
uct P
atho
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f T
oron
to o
n 05
/04/
15Fo
r pe
rson
al u
se o
nly.