-
8/3/2019 Resusitation in Trauma
1/51
ITACCSCURRENT PRACTICE GUIDELINES FOR
RESUSCITATION OF HAEMORRHAGIC
TRAUMA PATIENT
Dr. Sanghamitramishra
Asso. Prof
Dept. of Anaesthesiology and Critical Care
-
8/3/2019 Resusitation in Trauma
2/51
Traumatic injury remains the leading cause of
potentiallypreventable death under the age of fourty.
In addition, 50 million people globally are estimated to
beinjured ordisabled every year.
Although only a minority of patients present with
haemodynamicinstability, these patients have a significant chance
of dying
The cause of instability must be recognized and corrected
quicklyby using a systematic approach
-
8/3/2019 Resusitation in Trauma
3/51
Once the clinician has made the diagnosis of acute blood
loss,several
issues become important.
Traditional dogma suggests thatrestoration of forward flow by
crystalloid
resuscitation followed by blood is optimal therapy. However,
increases in blood
pressure produced by fluid may, in fact, increase blood loss by
displacing the
hemostatic clot that was formed at the time of hypotension.
However, there are now data to suggest that sustained
hypotension
produces a more injurious shock insult than do multiple episodes
of
shock and resuscitation. Thus, the clinician must estimate
the
degree of hemorrhage, the depth of shock, and the time to
definitive
hemostasis when making a decision.
-
8/3/2019 Resusitation in Trauma
4/51
Approximately 12 to 16 hours following
resuscitation, the relationship changes between
base deficit and anion gap versus serum lactate,and anion gap
and base deficit no longer correlatewith lactate.
During this time, one must directly measureserum lactate as it
cannot be inferred from either ofthe other two measurements.
When resuscitation decisions are based onthese parameters,
therapy will be inappropriatealmost 50% of the time.
-
8/3/2019 Resusitation in Trauma
5/51
Clearly, achieving hemostasis is the most important part
ofresuscitating the trauma victim. Resuscitation efforts will
not besuccessful until blood loss is arrested.
Regardless of the resuscitation decision, patients
whodemonstrate ongoing bleeding require definitive hemostasis.
Serial blood gas determinations and/or central venousoxygen
saturation determination may be very helpful indetermining whether
blood loss is continuing.
-
8/3/2019 Resusitation in Trauma
6/51
Hypoperfusion is a common complication after injury.Early
recognition of bleeding is key to the optimal care
of trauma patients.Normally vital signs underestimate the degree
of
physiologic deficit.Limited crystalloid resuscitation is prudent
initially, at
least until blood loss is controlled.New technology may soon be
available to help with the
diagnosis of hemorrhage.Early use of fresh-frozen plasma is
probably wise in
patients with severe hemorrhage using blood and plasma ina 1:1
ratio.
The use of factor VIIa requires further work before itsrole is
clearly elucidated. It can be lifesaving in selectedpatients.
-
8/3/2019 Resusitation in Trauma
7/51
Learning Objectives:
1) To learn the definition of shockand the common subtypes.
2) To understand the clinicaldiagnosis and progression of
shock.
3) To learn the pathophysiology of shockat the cellular, tissue,
organ, andwhole body level
-
8/3/2019 Resusitation in Trauma
8/51
Shock is the systemic disease that results
from any process that impairs the systemic
delivery of oxygen to the cells of the body, orthat prevents its
normal uptake and utilization.
Hemorrhage with decreased cardiac outputis the most common cause
of shock intrauma patients, although it is not unusual forshock to
result from a combination of events.
-
8/3/2019 Resusitation in Trauma
9/51
Causes of Shock in the Trauma Patient
Cause Pathophysiology
Lost airway or Inability of oxygen to reach
pulmonary injury the circulation
Tension pneumothorax Diminished blood return tothe heart
Cardiac tamponade Diminished blood return to the heart
Hemorrhage Inadequate oxygen carrying capacityInadequate
intravascular volume
Cardiac injury Inadequate pump function
Spinal cord injury Inappropriate vasodilatation
Inadequate pump function
Poisoning Direct failure of cellular metabolismInappropriate
vasodilatation
Sepsis Direct failure of cellular metabolismInappropriate
vasodilatation
-
8/3/2019 Resusitation in Trauma
10/51
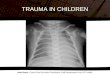
Stages and outcomes from traumatic shock. Curve A represents
compensated shock. Curve B is acute decompensated shock.
Oncedecompensation has occurred, three outcomes are possible: Curve
Crepresents subacute reversible shock (the patient survives). Curve
D issubacute irreversible shock (the patient dies of multiple organ
systemfailure). Curve E is acute irreversible shock (the patient
dies ofhemorrhage and cardiovascular collapse).
O
xygendelivery/
D
emand
-
8/3/2019 Resusitation in Trauma
11/51
After establishing a secure airway andensuring adequate
oxygenation and ventilation,
the highest priority in the management of theinjured patient is
to control hemorrhage.Because patients may bleed from multiple
sitessimultaneously, it is imperative that a strategybe devised to
identify and control all possiblesources of hemorrhage.
The control of hemorrhage is amultidisciplinary endeavor
involving traumasurgeons, orthopaedic surgeons, radiologists,and
anesthesiolo ists.
-
8/3/2019 Resusitation in Trauma
12/51
Blood Loss in Trauma
Site Potential volume
External (roadway or floor) Exsanguination possible
Thorax Greater than 1.5 L per
hemithorax
Peritoneal cavity Exsanguination possible
Pelvis and retroperitoneum Exsanguination possible
Long bone fractures Tibia/Humerus, 750 mL;
Femur, 1,500 mL
-
8/3/2019 Resusitation in Trauma
13/51
General Management of the Bleeding Patient
There must be a rapid and thorough search of the five
possible
locations for blood loss following injury.
The clinical pathophysiology of hemorrhage is made manifest
bytachycardia,hypotension, oliguria, and decreased mental
status.
Aggressive means must be taken to stop blood loss and
reversehypotension in order to prevent acidosis,coagulopathy,&
hypothermia.Increasing depth and duration of hypotension has been
shown to besignificantly associated with mortality.
Worsening base deficit results in statistically greater
transfusion volumes,coagulopathy, and organ dysfunction. Clot
formation time in healthy volunteersis significantly impaired by
acidosis and the effects are reversed by buffering.Hypothermia also
prolongs clotting times and causes platelet dysfunction.
-
8/3/2019 Resusitation in Trauma
14/51
Coagulation factors are lost from circulation, consumed
bycoagulation, and exhibit reduced activity because of
hypothermia,acidosis, and dilution with asanguinous fluid.
Prophylactic administration of fresh-frozen plasma (FFP)
orplatelets in the absence of clinical bleeding is
notwarranted.However, there is a growing emphasis on the need
for
earlier use of FFP before coagulation factors decline to
criticallevels in patients with significant bleeding.
With ongoing bleeding in severe trauma, FFP and packed redblood
cells (PRBCs) should be administered in a1:1 ratio. It iseasy to
get behind in this process, because it takes 20 to 30minutes for
FFP to thaw before administration.
The platelet count should be kept at a minimum of 50,000 per
Microliter.
-
8/3/2019 Resusitation in Trauma
15/51
At laparotomy (or any operation following injury) it is
absolutely necessary tocontrol hemorrhage in the most rapid fashion
possible.
After hemorrhage is controlled, gastrointestinal contamination
is nextaddressed.
The bloody vicious cycle (coagulopathy, hypothermia, and
metabolic acidosis)should compel the trauma team to use adamage
control approach.
The primary objectives of damage control are to arrest bleeding,
limit
gastrointestinal contamination, and enclose the abdomen to
protect viscera and limitprotein loss.
Subsequent operations are required to remove laparotomy sponges
used fortamponade, restore gastrointestinal continuity if required,
and to attempt abdominalwall closure when the patients condition is
more acceptable.
Damage control orthopaedics, using external fixation, reduces
operative timeand blood loss, and does not hinder definitive
osteosynthesis conversion.
-
8/3/2019 Resusitation in Trauma
16/51
Operating Room Priorities for the InjuredPatient
1. Control of hemorrhage2. Stop gastrointestinal contamination3.
Replace coagulation factors
4. Maintain normothermia and acid-base balance5. Thorough
exploration of abdomen (or other siteof injury) if condition
permits6. Temporary abdominal closure if there is
significant visceral edema7. Timely transfer to intensive care
unit forcontinued resuscitation8. Subsequent operations if
required
-
8/3/2019 Resusitation in Trauma
17/51
Proposed Indications for rFVIIa following Injury
Uncontrolled bleeding despite surgical or radiologic control
of
large-vessel hemorrhageCoagulopathy from exsanguinating
hemorrhage and failure ofconventional medical hemostatic
therapySignificant red blood cell or blood component
transfusion
requirementSuccess of transfusion and medical hemostatic
therapyunlikely to be timely enough to ensure survivalReasonable
hope for meaningful survival if coagulopathyreversedUse in remote
surgical locations where traditional therapy(platelets,
fresh-frozen plasma, cryoprecipitate, rewarming) fortraumatic
coagulopathy is not available
-
8/3/2019 Resusitation in Trauma
18/51
Conditions that Compromise rFVIIa Activity
Revised trauma score
-
8/3/2019 Resusitation in Trauma
19/51
Safe principles for care of the patient with a tourniquetshould
include
(1) used for the shortest time possible and removed at thefirst
available opportunity,
(2) should be deflated for 10 minutes every 2 hours,
(3) use wide cuffs to allow for lower occlusion pressure,
(4) record the time when applied,
(5) Communicate tourniquet use to others down the line in the
careprocess,
(6)should be removed by medical personnel only if bleeding can
bemanaged and resuscitation carried out
-
8/3/2019 Resusitation in Trauma
20/51
Hemorrhage control is a multidisciplinaryendeavor.
Lacerated organs and blood vessels must be resected orrepaired
before the sequelae of hemorrhage ensue.
Medical therapy using blood products, rFVIIa, topical
hemostatic agents, or advanced hemostatic dressings mayalso be
required to help restore, or compensate for, a depletedcoagulation
system.
Numerous methods for hemorrhage control exist, but eachmodality
must be applied to the appropriate situation.
Communication between the surgeon and anesthesiologistmust be of
the highest quality, so that appropriate corrective
actions may be undertaken to preserve life.
-
8/3/2019 Resusitation in Trauma
21/51
Various Drugs Agents That Have Some Efficacyto Reduce Bleeding
and/or Transfusion Burden
Generic Name Pharmacologic ClassAprotinin Natural serine
protease inhibitor
Nafamostat mesylate Synthetic serine proteaseinhibitor
e-Aminocaproic acid Lysine analogue
Tranexamic acid Lysine analogue
Desmopressin Analogue of arginine vasopressin
Recombinant Clotting factor and thrombinactivated factor VII
generator
Hemostatic Drugs in Trauma andOrthopaedic Practice
-
8/3/2019 Resusitation in Trauma
22/51
Hemostatic drugs are useful in excessive generalizedbleeding due
to hyperfibrinolysis, mild hemostatic
defects, or in those patients refusing blood products.
The appropriate drug is most effective when given asprophylaxis
and when adequate doses are given so
that they are not lost with the hemorrhage.
Results of ongoing trials of hemostatic drugs inorthopaedic
surgery and trauma are awaited to betterdetermine their optimal
uses, doses, timing of
administration, and safety.
-
8/3/2019 Resusitation in Trauma
23/51
Fluid and Blood Therapyin Trauma
Initial evaluation of an acutely volume-depleted traumapatient
will include a primary and secondary survey according to
AdvancedTrauma Life Support protocol,an estimate of blood volume
deficit rate of the ongoing blood loss, and
an evaluation of cardiopulmonary reserve and coexisting hepatic
or renaldysfunction.
The major goal in resuscitationis tostop the bleeding,
replete intravascular volume, and restore tissue
oxygenation.
Perfusion pressure and oxygenated blood flow to vitalorgans are
important determinants of outcome.
-
8/3/2019 Resusitation in Trauma
24/51
Management priorities in an acutely bleeding trauma
patientinclude ventilation and oxygenation, assessment of
perfusion,
estimation of volume-replacement requirements, establishment
orverification of adequate intravenous access, measurement of
bloodpressure, placement of electrocardiogram (ECG), pulse oximeter
andcapnograph, and laboratory studies.
Placement of arterial line and close monitoring of systolic
pressurevariability, temperature, urine output, arterial blood
gases, hemoglobin,hematocrit, electrolytes, and parameters of
coagulation is routine inseverely injuredmechanically ventilated
patients.
Consideration is given to use of additional monitors (e.g.,
central venouscatheter, pulmonary artery catheter, transesophageal
echocardiography)and provision of anesthesia as needed.
-
8/3/2019 Resusitation in Trauma
25/51
Estimation of Blood VolumeDeficit in Trauma Patients
Site Volume (mL)
Unilateral hemothorax 3,000
Hemoperitoneum with abdominal distention 2,0005,000
Full-thickness soft tissue defect, 5 cm 3 500
Pelvic fracture 1,5002,000
Femur fracture 8001,200
Tibia fracture 350650
Smaller fracture sites 100500
-
8/3/2019 Resusitation in Trauma
26/51
Timing and Aggressiveness ofFluid Resuscitation
Early aggressive fluid resuscitation aimed at restoration of
normalhaemodynamicsl eads to increased duration and volume
ofbleeding and decreased survival.
The proposed mechanisms include dilution of clotting
factors,decreased blood viscosity, and blow-out of hemostatic plugs
withincreasing blood pressure .
Hypotensive resuscitation, where the rate of fluid infusion
iscarefully titrated to a predetermined level of
lower-than-normal
blood pressure, has been advocated in patients who are
notpregnant and do not have traumatic head injury.
-
8/3/2019 Resusitation in Trauma
27/51
Consequently, in uncontrolled hemorrhagic shock,resuscitation is
aimed at restoration of radial arterypulse, restoration of mental
function, and systolic
blood pressure of 80 mm Hg, until the bleeding issurgically
controlled.
Higher blood pressures (systolic blood pressure>100 mm Hg,
mean arterial pressure >70 mm Hg)
are generally sought in head-injured and inpregnant
patients.
This approach provides satisfactory resuscitation of
the trauma patient until surgical control of bleedingis
achieved.
-
8/3/2019 Resusitation in Trauma
28/51
Disadvantages of Immediate Fluid
ResuscitationDecreased blood viscosity
Blow-out of hemostatic plug
Dilution of coagulation factors
Increased blood loss
Delayed transport to definitive care
Asanguinous Fluid Options for Trauma
-
8/3/2019 Resusitation in Trauma
29/51
Asanguinous Fluid Options for Trauma.
Lactated Ringers (LR) Preferred isotonic crystalloid solution
for most trauma resuscitations. Do not mixwith blood or use in
blood lines because LR contains calcium.0.9% Saline Preferred
isotonic crystalloid solution for head trauma. Only solution used
in blood transfusionlines and to dilute pRBCs. May cause
hyperchloremic metabolic acidosis (with normal anion gap) due
toexcess chloride displacing serum HCO3.
HespanHigh-molecular-weight hetastarch. Hextend (6% hetastarch
High-molecular-weighthetastarch. HalfNot recommended because of
adverse effects on(6% hetastarch in 0.9% saline) Half-life, 30
hours. Abandoned at authors institution-life, 30 hours. Less
coagulopathy and platelet dysfunctionin balanced electrolyte
solution) compared with Hespan. Maximum dose, 1015 mL/kgLow- and
medium-molecular- Colloid solutions with less coagulopathy and
platelet dysfunction comparedwith high-molecularweight
hetastarch weight hetastarch. Low-molecular-weight hetastarch
associated with improved muscle oxygentension, lower markers of
inflammation, and endothelial activation compared with LR.
Availablein Europe and Canada. Not currently available in United
States.Albumin (5%) Little effect on coagulation. May pass into
interstitial compartment if impaired vascularintegritywith
resultant endothelial swelling and impaired microcirculatory
perfusion. Increased mortalityafter head trauma in SAFE study (vs.
0.9% saline).46Dextrans and gelatins Colloid solutions largely
abandoned in United States because of negative effects on
coagulationand potential for anaphylaxis and hypersensitivity
reactionsHypertonic saline Variety of solutions/concentrations. May
be combined with colloid to prolong duration ofaction.Efficiently
restores intravascular volume and decreases extravascular volume
and tissue edema.Decreases ICP and increases CPP. Especially
advantageous in prehospital situations and in headtrauma with
refractory increased ICP. Not associated with improved neurologic
outcomes
-
8/3/2019 Resusitation in Trauma
30/51
There is controversy concerning which intravenous
solutionsshould be used for resuscitation .
During hemorrhage, a compensatory increase inreabsorption of
fluid into capillaries partially restores theintravascular
compartment, but depletes the interstitialspace.
To replete the intravascular and interstitial
compartments,crystalloid solutions such as isotonic 0.9% saline or
lactatedRingers (LR) solution are traditionally used.
Glucose-containing solutions are avoided becausehyperglycemia is
associated with aggravation of centralnervous system injuryand
increased mortality, especially intrauma patients.
-
8/3/2019 Resusitation in Trauma
31/51
The effects of crystalloid solutions on the coagulation
system are complex.
With hemodilution up to 20 to40%crystalloids produce
ahypercoagulable state because of dilution of
anticoagulant factors such as antithrombin and byplatelet
activation.
After 60% hemodilution, both crystalloids and colloidsproduce a
hypocoagulable state.
-
8/3/2019 Resusitation in Trauma
32/51
One unit of packed RBCs will usually increase thehematocrit by
approximately 3% or the hemoglobin by 1
g/dL in a 70-kg nonbleeding adult
If 50% to 75% of the patient's blood volume has been
replaced with type 0 blood (e.g., approximately 10 unitsof red
cells in an average size adult patient), one shouldcontinue to
administer type O red cells. Otherwise, riskof a major cross-match
reaction increases because thepatient may have received enough
anti-A or anti-B
antibodies to precipitate hemolysis if A, B, or AB unitsare
subsequently given.
-
8/3/2019 Resusitation in Trauma
33/51
Approach to Transfusing Red Blood Cells (RBCs)Based on the
American Society of AnesthesiologistPractice Guidelines and Review
of the Literature. Transfuse RBCs if hemoglobin 10 g/dL Decision to
transfuse RBCs should be individualizedbased on:
1. Presence of organ ischemia (e.g., altered mental
status,myocardial ischemia, acidosis, low mixed venous
oxygensaturation)2. Rate of bleeding
3. Magnitude of bleeding4. Intravascular volume status5.
Cardiopulmonary reserve
Coagulation Factors and Platelets
-
8/3/2019 Resusitation in Trauma
34/51
Coagulation Factors and Platelets
Two units of fresh-frozen plasma (1015 mL/kg) will achieve30%
factor activity in most adults
The primary cause of bleeding after trauma is surgical, while
thesecond leading cause is hypothermia and dilutional
coagulopathy
Cryoprecipitate and factor concentrates may be indicated
tocorrect specific factor deficiencies. Cryoprecipitate is rich
infibrinogen as well as factors VIII, XIII, and von Willebrand
factor.
Thrombocytopenia is treated with platelet concentrates
Platelet transfusions are usually indicated in the presence of
clinicalbleeding and a platelet count
-
8/3/2019 Resusitation in Trauma
35/51
COAGULATION MONITERING
PT
APTT
FIBRINOGEN
FDP
THROMBOELASTOGRAM
-
8/3/2019 Resusitation in Trauma
36/51
Definitions of MassiveTransfusion
One blood volume loss in 24 hours (equivalent to 10
units of whole blood )
Four or more units replaced in 1 hour with
continuingbleeding
50% blood volume loss in 3 hours (equivalent to 5 unitsof whole
blood)
50 units lost in 48 hours
20 units lost in 24 hours
Blood loss exceeding 150 mL/min.
-
8/3/2019 Resusitation in Trauma
37/51
The adverse effects of hypothermia in the trauma
patientinclude
major coagulation derangements, peripheral vasoconstriction,
metabolic
acidosis, compensatory increased oxygen requirements during
rewarming,and impaired immune response.
Standard coagulation tests are temperature-corrected to 37C and
maynot reflect hypothermia-induced coagulopathy. Hypothermia
impairscoagulation because of slowing of enzymatic rates and
reduced platelet
function.Even worse, different steps in coagulation cascade are
affected to
different degrees, disrupting synchronization of the
cascade.Hypothermia can cause cardiac dysrhythmias and even cardiac
arrest
from electromechanical dissociation, standstill, or
fibrillation, especially with
core temperatures below 30C.Hypothermia also impairs citrate,
lactate, and drug metabolism;
increases blood viscosity; impairs RBC deformability; increases
intracellularpotassium release; and causes a leftward shift of the
oxyhemoglobindissociation curve. A mortality of 100% has been
reported in trauma patientswhose body temperature fell below
32C,
-
8/3/2019 Resusitation in Trauma
38/51
Resuscitation End Points
Within the First 24 Hours afterTrauma
Parameter Value
Mixed venous oxygen tension >35 mm Hg
Mixed venous oxygen saturation >65%
Base deficit > -3 mmol/L
Lactate
-
8/3/2019 Resusitation in Trauma
39/51
-
8/3/2019 Resusitation in Trauma
40/51
Goals for Fluid Resuscitation
Achievement of normovolemia and hemodynamic stability
Correction of major acid-base disturbances
Compensation of fluxes from the
interstitial/intracellularcompartments
Improvements of microvascular blood flow
Prevention of activation of inflammatory cascade system
Normalization of oxygen delivery to tissue cells and cell
metabolism
Prevention of reperfusion injury
-
8/3/2019 Resusitation in Trauma
41/51
capacitance, and positive inotropic effects through direct
actions onmyocardial cells
Hypertonic solutions and hypertonic/hyperoncotic solutions may
improvecardiovascular function on multiple levels: displacement of
tissue fluid into
the blood compartment, direct vasodilatory effects in the
systemic andpulmonary circulation, reduction in venous
Because of the hypertonicity of the solutions,only a small
volume offluid (approximately 4 mL/kg) is necessary to effectively
restore
cardiovascular function (small-volume resuscitation).
-
8/3/2019 Resusitation in Trauma
42/51
Improved microperfusion resulting frominfusion of hypertonic
solutions (small-volume resuscitation).
-
8/3/2019 Resusitation in Trauma
43/51
In inflammatory-related capillary leak, HEShas been reported
tohave occlusiveeffects on damagedcapillaries,subsequently
limitingthe extravasation of fluid. LMW HES may
exert benefical effects on endothelialfunction by stabilization
of fragile cellmembranes or by avoiding endothelial
swelling This may be of benefit in thosetrauma patients
suffering from severeendothelial leakage
-
8/3/2019 Resusitation in Trauma
44/51
-
8/3/2019 Resusitation in Trauma
45/51
Management of bleeding patients with fluids andblood/blood
products
-
8/3/2019 Resusitation in Trauma
46/51
Risks Associated with Allogeneic TransfusionOnset Time Mechanism
Complication
Acute Immunologic Acute
hemolyticAllergic/anaphylactoidTransfusion-related acute lunginjury
(TRALI)FebrileInfectious Bacterial contamination
Metabolic Volume overloadStorage defect-associated injuryDelayed
Immunologic Delayed hemolyticPosttransfusion
purpuraGraft-versus-host diseaseTransfusion-related
immunomodulation (TRIM)Infectious Viruses, parasites,
prionsOncogeneMetabolic Iron overload
-
8/3/2019 Resusitation in Trauma
47/51
these echinocytes do not pass through capillaries in thesame
fashion as do normal,unstored cells
During the storageof a red cell, red cell shape change occurs
due to areduction in intracellular adenosine triphosphate,
sialic
acid, and nitric oxide.
After approximately 14 days of storage, dependent on thestorage
solution, the red cells lose their biconcave disc
shape and become echinocytes
-
8/3/2019 Resusitation in Trauma
48/51
Diagnosis of Transfusion-Related Acute Lung Injury1. No acute
lung injury prior to transfusion
2. Acute lung injury occurs during or within 6 hours
oftransfusion
3. Acute onset of respiratory distress
4. Hypoxemia
5. Bilateral lung infiltrates on chest radiograph
6. No evidence of circulatory overload
7. No other acute lung injury risk factors (septic shock,sepsis,
aspiration, lung contusion, pneumonia, multiple trauma,drug
overdose, burn injury, cardiopulmonary bypass, inhalationinjury,
acute pancreatitis) overload
-
8/3/2019 Resusitation in Trauma
49/51
-
8/3/2019 Resusitation in Trauma
50/51
A DEDICATED TRAUMA TEAM CAN SAVE THIS LIMB
-
8/3/2019 Resusitation in Trauma
51/51