Embed Size (px)
Citation preview

Review Article
A c!inical and research protocol for characterizingpatients with hypophosphatasiaChing-Chun Hu, BDS, PhD David L. King, DDS, PhD
Huw F. Thomas, BDS, LDS, MS, PhD James P. Simmer,
H ypophosphatasia is a rare inherited disordercharacterized by a wide spectrum of defects inmineralized tissues. The disease is usually in-
herited as an autosomal recessive trait with a prevalenceof approximately 1/100,000 live births. 1 The clinicalmanifestations are highly variable, ranging from an al-most total lack of skeletal formation to the prematureloss of the permanent anterior teeth. The scarcity ofhypophosphatasia patients and the diversity of theirsymptoms create special challenges for the clinician,who is unlikely to benefit from broad experience withthe disease. These difficulties are compounded by ba-sic science researchers who require standardized andthorough clinical descriptions of affected individuals.It is now possible to characterize the precise mutation(s)at the root of this disorder. To successfully relate theunderlying biochemical deficit to its clinical sequelae,it is necessary to document the complete range of physi-cal signs and symptoms of the hypophosphatasia pa-tient. We anticipate that the next 5 to 10 years will seetremendous progress in identifying mutations under-lying childhood hypophosphatasia. As scientists go onto clone and characterize these mutations, the pediatricdentist must assume an expanded role in diagnosis,clinical description, tissue collection, and referral to ap-propriate genetics or research institutions. Our objec-tives in this report are threefold:
1. To review the basic and clinical science ofhypophosphatasia
2. To heighten awareness among pediat-ric dentists of opportunities to contrib-ute to scientific investigations directedtoward characterizing the physiologi-cal outcomes of specific mutations un-derlying hypophosphatasia
3. To propose a strategy for conductinga thorough clinical examination onhypophosphatasia patients whosemutation(s) may subsequently be char-acterized.
DDS, PhD
The underlying genetic defectand its role in hypophosphatasiaand laboratory diagnosis
Hypophosphatasia is caused by a defect in the gene-encoding, tissue nonspecific alkaline phosphatase(TNSALP), which is also known as liver/bone/kidneyalkaline phosphatase (L/B/K ALP).2 This enzyme ispresent in most tissues and in blood serum,3 with os-teoblasts showing the highest level of activity. 4, s
TNSALP is encoded by a single gene located near thetip of the short arm of chromosome 1.6,7 The gene com-prises more than 50,000 base pairs of DNA.s Its RNAmessage is 2339 nucleotides in length.9, 20 The protein,following removal of a 17 amino acid signal peptide,contains 507 amino acids. Hypophosphatasia occurswhen a single nucleotide in the coding region for theprotein is mutated, causing one of the 507 amino acidsto change.
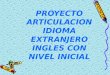
TNSALP functions principally as a phosphomo-noesterase.11,12 In humans the enzyme cleaves phosphatefrom three known substrates: pyridoxal-5’-phosphate(PLP), pyrophosphate (PPi), and phosphoethanolamine(PEA). The chemical structures of these substrates areprovided in Fig 1. Tissue nonspecific alkaline phos-phatase is anchored at its carboxyl-terminus to theplasma membrane by a phosphatidylinositol-glycanmoiety.13 Its tetrameric structure is oriented so that theactive sites face the extracellular environment. Thisprotein also is present in serum as a functional dimer
0
Pyddoxal 5’-phosphate (PLP)
Phosphoethanolamine (PEA) Pyrophosphate (PPi)
Fig 1. TNSALP substrates: pyridoxal-5’-phosphate, phosphoethano-lamine, and pyrophosphate.
Pediatric Dentistry- 18:1, 1996 American Academy of Pediatric Dentistry 17

following cleavage of its membrane attachment by aspecific phospholipase.I4 A reduction in serum alkalinephosphatase activity along with elevated serum andurine levels of TNSALP substrates forms the basis forlaboratory tests to diagnose hypophosphatasia as wellas unaffected carriers of the disease.
Pyridoxal-5’-phosphate (PLP) is a derivative of 6that functions as a coenzyme with enzymes that de-grade glycogen. It also participates in a wide range oftransformations on amino acids including transamina-tions, decarboxylations, deaminations, racemizations,and aldol cleavages.15 PLP is unable to traverse theplasma membrane while phosphorylated. TNSALPmay act as an ectoenzyme to dephosphorylate PLP,facilitating its entry into cells26
Pyrophosphate (PPi) is a potent inhibitor of biomin-eralization27 TNSALP removes this inhibitor and gen-erates phosphate, a component of calcium hydroxya-patite. Pyrophosphate is a byproduct of manybiosynthetic reactions. Cleavage of PPi can drive sucha reaction forward by removing a reaction product28An increased concentration of PPi can be detected inthe urine19 and serum2°, 21 of individuals with reducedALP activity.
Phosphoethanolamine (PEA) is incorporated intomembranes as phosphatidylethanolamine (plasmalo-gen) or phosphatidylethanolamine(cephalin) whose structures are pro-vided in Fig 2. 22 Plasmalogens consti-tute as much as 10% of the phospholip-ids of brain and muscle cells. Anincreased concentration of PEA can be Perinatal
detected in the urine23-25 and serum16 of Perinatalindividuals with reduced ALP activity.
The three substrates accumulate in Infantilepatients with a defective allele of InfantileTNSALP, even if they do not presentwith clinical hypophosphatasia. El- Infantileevated levels can be detected in eitherthe serum or urine and provide a
Infantilemethod to identify unaffected carriers(heterozygotes), or to confirm a diagno-sis of hypophosphatasia when clinicalmanifestations are present.26
PLP, PPi, and PEA are intermediates in diverse, andapparently unrelated, biochemical pathways. The si-multaneous loss of capacity to metabolize all three sub-strates could perturb widespread molecular processes.Sorting out the chain of events that begins with a spe-cific TNSALP catalytic deficit and ends with a clinicaloutcome such as premature tooth loss, rickets, or cran-iostenosis is daunting, but is precisely what must beaccomplished to characterize hypophosphatasia at themolecular level. In special circumstances, it may be pos-sible to isolate the downstream effects of a loss ofTNSALP function with respect to a single substrate.
An isolated case of pseudohypophosphatasia hasbeen reported. 27 The patient presented withhypophosphatasia-like symptoms in the absence of re-duced TNSALP activity. Subsequent investigations de-termined that the TNSALP of this patient had lost ac-tivity for pyridoxal-5’-phosphate only while the activitywith other substrates was normal. 28, 29 Thereforehypophosphatasia was the correct diagnosis. The al-tered amino acid residue may participate in PLP bind-ing but has not been characterized.
Ten-point mutations that lead to perinatal or infan-tile hypophosphatasia have been reported and are listedin the Table. The most severe forms of hypo-phosphatasia are recessive and usually are lethal at or
II
Onset Survival TNSALP Mutation Substitutions Reference
Died at birth G 1177 to A Gly 317 to Asp 47
Died at birth G 388 to C Arg 54 to Pro 38A 796 to C Gln 190 to Pro
Died at 3 months G 711 to A Ala 162 to Thr 51
Died at 6 months C 387 to T Arg 54 to Cys 38A 1057 to C Asp 277 to Ala
Died at 8 months G 747 to A Glu 174 to Lys 38A 1309 to T Asp 361 to Val
Pneumonia & C 274 to T Ala 16 to Val 38rickets at 6 months T 1482 to C Tyr 419 to Hisbut near normalat 9 years old
0 CH~-- O--CH=CH--R~R, ~ 0 ~CH"’ ’I l ..........................
~ ...............................: ................ .............................
Phosphatidalethanolamine (Plasmalogen)
o
0
iH2-- O--C-- ....
Phosphatidylethanolamine (Cephalin)
Fig 2. Membrane phospholipids containing phosphoenthanolamine. The phosphoenthanolamine side chains are boxed.
18 American Academy of Pediatric Dentistry Pediatric Dentistry - 18:1, 1996

near birth. 3° While the specific mutations underlyingchildhood and adult hypophosphatasia are yet to becharacterized, they are known to involve the TNSALPgene. The procedures for identifying these mutationsare the same as those that have achieved so muchprogress in characterizing the lethal forms,sl To achievesimilar advances in our understanding of childhoodand adult hypophosphatasia, it is necessary for clini-cians to bring their patients to the attention of the re-search community by making a detailed case study oftheir clinical presentation. In the following sections thesigns and symptoms likely to be encountered in ahypophos-phatasia patient are discussed along withsuggestions for how they can be discerned in a clinicalexamination.
The clinical manifestationsof TNSALP mutations
Hypophosphatasia is classified according to the agewhen symptoms first appear (for reviews seel,31). Whyclinical manifestations segregate according to age ofonset is unknown. As a general rule the earlier the ap-pearance of disease the greater the severity. Appar-ently, diverse point mutations result in heterogeneousamino acid substitutions in the alkaline phosphataseprotein. The altered proteins display a spectrum offunctional changes that range from complete activityto complete loss of activity. Mutants displaying no ac-tivity should affect all alkaline phosphatase-dependentdevelopment and result in extreme symptoms that areobserved earlier. A minor loss of TNSALP functionmay affect only processes that are the most alkalinephosphatase dependent, which happen to occur laterin development. The four clinical varieties ofhypophosphatasia are perinatal, infantile, childhood,and adult onset.1, 31
Perinatal hypophosphatasia occurs in utero with theinfant being stillborn or expiring a few days after birth.These individuals exhibit dramatic skeletal deformi-ties. 32-34 Diagnosis is based upon radiographic findings.
Infantile hypophosphatasia has similar skeletal de-formities as the lethal form, only far less severe. Symp-toms are usually noticed within the first 6 months post-natal. The infant feeds poorly and fails to gain weight,3s,36 and may present with a flail chest and pneumonia. Eye
signs include blue sclerae, harlequin orbits, and patho-logic lid retraction.37 Wide fontanelles and cranial su-tures may be observed, or alternatively the fontanellesmay be obliterated with subsequent craniostenosis.37
The disorder is fatal in about half of fhe cases.1 Child-hood survivors can range from few symptoms38 to pre-mature fusion of all cranial sutures with prominent scal-loping of the inner table of the skull, premature toothloss, and generalized osteopenia and ossification defectswith bowing deformities of the long bones .39
Childhood hypophosphatasia is often diagnosed firstby the dentist.4° The child may have rickets, a small stat-ure, and a waddling gate. The periodontal ligament
does not form properly possibly due to a partial or com-plete lack of cementum formation.41 Both parents ofhypophosphatasia children, although clinically unaf-fected, are likely to exhibit a raised urinary concentra-tion of pyrophosphate and reduced serum alkalinephosphatase activity. 42 Lundgren et al. published an ex-cellent retrospective study that provides a differentialdiagnosis for hypophosphatasia, assesses various pa-rameters for their reliability in making a diagnosis, andsuggests a diagnostic strategy. Clinical and radiologicdeformities of the legs were the most consistent find-ing, followed by non-leg bony deformities and the pre-mature loss of anterior primary teeth. The exfoliatedteeth were fully rooted and displayed cementum apla-sia. A histological examination of prematurely mobileprimary teeth was recommended as a diagnostic tool.
Adult hypophosphatasia is principally associatedwith premature loss of the anterior maxillary and man-dibular teeth with a history of early primary tooth loss.43
Enamel hypoplasia often is observed with prematuretooth loss due to caries.44 Premature fusion of cranialsutures may result in proptosis with elevated intracra-nial pressure and brain damage.4s The precipitation ofcalcium pyrophosphate in the joints can lead tochondrocalcinosis or calcium pyrophosphate depositiondisease (or pseudogout).36,46
Relating specific TNSALP mutationsto their clinical outcomesThe role of the research scientist
The research scientist submits a human researchprotocol, which includes proposed consent forms anda research plan, to an institutional review board. A grantapplication may be sent to appropriate funding agen-cies such as the March of Dimes or the National Insti-tute of Health. Upon approval of the protocol, periph-eral fibroblasts are grown in culture from a skin biopsyobtained from the hypophosphatasia patient. TotalRNA is isolated from these cells and converted to cDNA(or copy DNA) by a process known as reverse transcrip-tion (RT). The cDNA complimentary to the TNSALPmRNA is then amplified by polymerase chain reaction(PCR), cloned, and characterized by DNA sequencing.This DNA sequence is entered into a computer and com-pared with the published sequence for human TNSALP.This procedure identifies the precise mutation(s) affect-ing a proband. The mutation(s) then are linked to thedisease state by allele-specific-oligonucleotide (ASO)hybridization analysis of PCR-amplified genomicDNA.47 In this procedure, the presence or absence of themutant allele is determined for each member of thepedigree and a statistical analysis is performed to mea-sure the correlation of the mutation with the disease.The genomic DNA for this experiment is obtained fromblood samples.
The amino acid sequence of the mutated protein isdeduced from the DNA sequence and compared withthe unmutated or wild-type sequence. The location of
Pediatric Dentistry- 18:1, 1996 American Academy of Pediatric Dentistry 19

the amino acid substitution is compared with proteinsequences of a wide range of alkaline phosphatase ho-mologues and to the three-dimensional structure of E.coli alkaline phosphatase. The level of conservation ofthe substituted amino acid is discerned as well as itslikely effect on protein folding and function. Culturedcells may be induced by recombinant DNA techniquesto express the mutant protein to directly assay forchanges in enzyme function.
While these investigations provide useful data con-cerning the biochemical deficit underlying hypophos-phatasia, investigating the physiology and pathology ofthe disorder requires that this information be relatedback to the clinical symptoms to associate specific mu-tations with their downstream physical effects. Thisnecessitates a thorough clinical investigation usuallyconducted by a pediatric dentist and/or a pediatrician.
The role of the pediatric dentist
The clinician is most likely the first member of theresearch team to meet the patient and make a diagno-sis based upon clinical, radiographic, serum and urineanalyses. A routine description of the physical defectsis made. The quality of this description depends on aprior knowledge of potential symptoms and what testsare needed to identify them. Even if a research effort isnot being considered at this point, the examinationshould be conducted as thoroughly as possible. It maybe at a subsequent recall that the decision is made topursue a research strategy, and prior documentationof findings would enhance the analysis. As medicaltechnology advances, it is plausible that DNA sequencecharacterization of inborn errors of metabolism will be-come a routine laboratory procedure.
The patient should be informed that it is technologi-cally feasible to pinpoint the exact mutation at the rootof the disease. This requires locating an interested re-search group. Blood and urine samples are needed fromeach member of the pedigree, and a punch biopsy isneeded from the proband. No promises or allusionsshould be made to possible personal benefits to patientsor their families. The results of an investigation wouldcontribute to a large body of data that may eventuallylead to improved diagnosis and treatment.
A proposed clinical approach to diagnoseand characterize hypophosphatasia
Hypophosphatasia is caused by point mutations inthe tissue nonspecific alkaline phosphatase gene. Differ-ent amino acid substitutions can variably affect enzymefunction, particularly in the case of a multifunctionalprotein such as TNSALP. Depending upon the impact ofthe amino acid substitution on enzyme function, theclinical manifestations are of variable severity, which isreflected in the age when symptoms first appear. Physi-ological processes that depend on TNSALP activity, suchas cementum formation in the primary and secondarydentitions, occur a t specific times, causing the ages when
symptoms first appear to cluster. This nodal distributionis the basis for the clinical classification. This system cancause confusion however, as patients survive their earlysymptoms and later present with childhood or adulthypophosphatasia. A simple diagnosis of hypophos-phatasia is straightforward and may be adequate undercertain circumstances. The most reliable diagnostic find-ings are clinical and radiologic abnormalities of the legs,phosphoethanolamine in the urine, and reduced serumalkaline phosphatase activity.4°
For the advancement of science and for future im-provements in our understanding and treatment ofhypophosphatasia, we propose the following clinicalapproach be implemented when trying to characterizethe genetic lesion underlying hypophosphatasia. Thisapproach is most applicable for childhood hypo-phosphatasia and can be conducted by a pediatric den-tist. A pediatrician may be consulted if the dentist pre-fers assistance in accomplishing any of the followingprocedures.
1. Patient and family history. A pedigree is estab-lished. Family members with clinical hypo-phosphatasia are noted along their ages of onset,and the extent of their symptoms. Dental recordsare obtained to document premature loss of teeth.Blood and urine analyses from each member ofthe pedigree are used to establish the carrier sta-tus of unaffected members.42 Identifying carriershelps to determine if one or both alleles are likelyto be mutated in the patients withhypophosphatasia. This information revealswhether the pattern of inheritance is dominant orrecessive, which is used in genetic counseling.
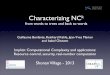
2. Physical examination. The patient’s height andweight are recorded. Subsequent measurementsestablish a chronology that is used for monitor-ing growth potential. A thorough dental exami-nation with panorex (or periapical radiographs)should look for premature loss of primary teeth,widened pulp chambers, and enamel hypoplasia.The gait and shape of legs are examined. Radio-graphs of the legs are taken when abnormalities,such as bowing are suspected. The shape of thehead is noted with lateral and anterior-posteriorcephalograms used to evaluate the size of the fon-tanelles and ossification of the sutures. Chest x-rays can help document a deviated sternum andmalformed vertebra. Examples of these diagnos-tic radiographs are shown in Fig 3.
3. Tissue collection. Hypermobile, fully rooted teethare extracted, placed in formalin, and sent for his-tological examination of the cementum. Under lo-cal lidocaine anesthesia, a 4-mm punch biopsy istaken from the upper arm, one-third of the dis-tance from the shoulder to the elbow, on the lat-eral aspect.48 The biopsy is placed in ice coldHank’s balanced salt solution (GIBCO/BRL,
20 American Academy of Pediatric Dentistry Pediatric Dentistry - 18:1, 1996

Fig 3. Diagnostic radiographs. Lateral (a), and frontal (c) views of the head, a dental panorex, chest (d) and long bone (e)radiographs are used to detect skeletal deformities associated with hypophosphatasia.
Gaithersburg, MD), and immediately shipped tothe genetics laboratory for cloning of the TNSALPmRNA. (The Hank's solution is a standard labo-ratory item and can be obtained from the researchteam.)
4. Blood (10 cc) and urine samples. The clinicianorders blood and urine collected from all of theavailable members of the pedigree. Thesesamples are obtained in the morning prior to thefirst meal.49 Serum calcium and alkaline phos-phatase activity are determined. Fasting samplesare used to avoid measuring the transient intes-tinal alkaline phosphatase activity that appearsafter eating. PEA and PLP levels are measured inboth urine and serum. The Mayo Clinic (Roches-ter, MN) can perform these tests. PPi analyses arenot offered by commercial laboratories. These re-sults establish the diagnosis and determine if uti-
lization of all three substrates is affected. Bloodcells are frozen and stored for the subsequent iso-lation of genomic DNA.
5. Recall. The patients are recalled annually to docu-ment progression of the disease.
Conclusion
Hypophosphatasia is both rare and heterogeneous.This presents the clinician and scientist with specialchallenges and opportunities. By relating specificTNSALP defects to thorough clinical descriptions, thephysiology of alkaline phosphatase activity will be bet-ter understood. Childhood- and adult-onsethypophosphatasia often present a dominant pattern ofinheritance while more severe forms are recessive.Simple laboratory tests of unaffected parents can de-termine carrier status and improve our understanding
Pediatric Dentistry - 18:1,1996 American Academy of Pediatric Dentistry 21

of the mode of inheritance of hypophosphatasia. Al-
though the severity of hypophosphatasia in patientsfrom a given pedigree usually is similar, in some in-
stances the phenotype varies, s° This variability appearsto increase in individuals displaying a later onset ofsymptoms.B6 As the specific mutations in assorted in-
dividuals are characterized, the extent of environmen-
tal influences can be better assessed. Knowledge ofthese effects may form the basis for dietary and thera-peutic interventions that minimize the clinical course
of hypophosphatasia.
Dr. Hu is assistant professor, Dr. King is professor, Dr. Thomas isprofessor and chairman, and Dr. Simmer is assistant professor, allat the University of Texas School of Dentistry, Health Science Cen-ter at San Antonio, Department of Pediatric Dentistry.
1. Fraser D: Hypophosphatasia. Amer J Med 22:730--46, 1957.2. Rasmussen H, Bartter FC: The metabolic basis of inherited
disease. New York: McGraw-Hill, 1978, pp 1340-50.3. Goldstein DJ, Rogers CE, Harris H: Expression of alkaline
phosphatase loci in mammalian tissues. Proc Natl Acad SciUSA 77:2857~0, 1980.
4. Doty SB, Schofield BH: Enzyme histochemistry of bone andcartilage cells. Prog Histochem Cytochem 8:1-38, 1976.
5. Rodan GA, Rodan SB: Expression of the osteoblasticphenotype. Amsterdam: Elsevier Science Publishers, 1983,pp 244-85.
6. Smith M, Weiss MJ, Griffin CA, Murray JC, Buetow KH,Emanuel BS, Henthorn PS, Harris H: Regional assignment ofthe gene for human liver/bone/kidney alkaline phosphataseto chromosome lp36.1~p34. Genomics 2:139-43, 1988.
7. Greenberg CR, Evans JA, McKendry-Smith S, Redekopp S,Haworth JC, Mulivor R, Chodirker BN: Infantilehypophosphatasia: localization within chromosome regionlp36.1-34 and prenatal diagnosis using linked DNA mark-ers. Am J Hum Genet 46:286-92, 1990.
8. Weiss MJ, Ray K, Henthorn PS, Lamb B, Kadesch T, HarrisH: Structure of the human liver/bone/kidney alkaline phos~phatase gene. J Biol Chem 263:12002-10, 1988.
9. Weiss MJ, Henthorn PS, Lafferty MA, Slaughter C, RaduchaM, Harris H: Isolation and characterization of a cDNA en-coding a human liver/bone/kidney-type alkaline phos-phatase. Proc Natl Acad Sci USA 83:7182-86, 1986.
10. Kishi F, Matsuura S, Kajii T: Nucleotide sequence of the hu-man liver-type alkaline phosphatase cDNA. Nucleic AcidsRes. 17:2129, 1989.
11. Coleman JE: Structure and mechanism of alkaline phos-phatase. Annu Rev Biophys Biomol Struct 21:441-83, 1992.
12. Kim EE, Wyckoff HW: Reaction mechanism of alkaline phos-phatase based on crystal structures. J Mol Bio1218:449-64,1991.
13, Jemmerson R, Low MG: Phosphatidylinositol anchor ofHeLa cell alkaline phosphatase. Biochemistry 26:5703-9,1987.
14. Hawrylak K, Stinson RA: The solubilisation of tetrameric al-kaline phosphatase from human liver and its conversion intovarious forms by phosphatidylinositol phospholipase C orproteolysis. J Biol Chem 263:14368-373, 1988.
15. Stryer L: Biochemistry, 3rd Ed. New York: WH Freeman andCo, 1988, pp 452, 496-99.
16. Whyte MP, Mahuren JD, Vrabel LA, Coburn SP: Markedlyincreased circulating pyridoxal-5’-phosphate levels inhypophosphatasia. Alkaline phosphatase acts in vitamin B6metabolism. J Clin Invest 76:752-56, 1985.
17. Fleish H, Neuman WF: Mechanism of calcification. Role ofcollagen, polyphosphates and phosphatase. Am J Physiol200:1296-1300, 1961.
18. Stryer L: Biochemistry, 3rd Ed. New York: WH Freeman andCo, 1988, pp 456.
19. Russell RG: Excretion of inorganic pyrophosphate inhypophosphatasia. Lancet 2:461-64, 1965.
20. Russell RG, Bisaz S, Donath A, Morgan DB, Fleish H: Inor-ganic pyrophosphate in plasma in normal persons and inpatients with hypophosphatasia, osteogenesis imperfecta,and other disorders of bone. J Clin Invest 50:961-69, 1971.
21. Macfarlane JD, Harinck HI, Bijvoet OL: Hyperphospha-taemia in hypophosphatasia. Neth J Med 28:54142, 1985.
22. Martin Jr DW, Mayes PA, Rodwell VW, Granner DK:Harper’s Review of Biochemistry. Los Altos, CA: LangeMedical Publications, 1985, pp 198-99.
23. McCance RA, Morrison AB, Dent CE: The excretion ofphosphoethanolamine and hypophosphatasia: preliminarycommunication. Lancet 268:131, 1955.
24. Fraser D, Yendt ER, Christie FHE: Metabolic abnormalitiesin hypophosphatasia. Lancet 286, 1955.
25. Rasmussen K: Phosphorylethanolamine and hypophos-phatasia. Danish Med Bull 15:1-112, 1968. (Supp| 2)
26. Sorensen SA, Flodgaard H, Sorensen E: Serum alkalinephosphatase, serum pyrophosphatase, phosphoryle-thanolamine and inorganic pyrophosphate in plasma andurine. A genetic and clinical study of hypophosphatasia.Monogr Hum Genet 10:66-69, 1978.
27. Scriver CR, Cameron D: Pseudohypophosphatasia. N Engl JMed 281:604-6, 1969.
28. Cole DEC, Coburn SP, Salisbury SR, Whyte MP:Pseudohypophosphatasia revisited: Further biochemicalcharacterisation sixteen years later. Am J Hum Genet37:016;12.1, 1985.
29. Cole DE, Salisbury SR, Stinson RA, Coburn SP, Ryan LM,Whyte MP: Increased serum pyridoxal-5’-phosphate inpseudohypophosphatasia [letter]. N Engl J Med 314:992-93,1986.
30. Caswell AM, Whyte MP, Russell RG: Hypophosphatasia andthe extracellular metabolism of inorganic pyrophosphate:clinical and laboratory aspects. Cri~ Rev Clin Lab Sci 28:175-232, 1991.
31. Chapple IL: Hypophosphatasia: dental aspects and mode ofinheritance. J Clin Periodonto120:615-22, 1993.
32. Koslowski K, Sutcliffe J, Barylak A, Harrington G,Kemperdick H, Nolye K, Rheinwein H, Thomas PS, UnieckaW: Hypophosphatasia: review of 24 cases. Pediatric Radiol-ogy 5:103-17, 1976.
33. Ornoy A, Adomian GE, Rimoin DL: Histologic and ultra-structural studies on the mineralization process inhypophosphatasia. Am J Med Genet 22:743-58,1985.
34. Shohat M, Rimoin DL, Gruber HE, Lachman RS: Perinatal le-thal hypophosphatasia; clinical, radiologic and morphologicfindings. Pediatr Radio121:421-27, 1991.
35. Whyte MP, Valdes R Jr, Ryan LM, McAlister WH: Infantilehypophosphatasia: enzyme replacement therapy by intrave-nous infusion of alkaline phosphatase-rich plasma from pa-tients with Paget bone disease. J Pediatr 101:379-86, 1982.
36. Whyte MP, Murphy WA, Fallon MD: Adulthypophosphatasia with chondrocalcinosis and arthropathy.Variable penetrance of hypophosphatasemia in a large Okla-homa kindred. Am J Med 72:631-41, 1982.
37. Brenner RL, Smith JL, Cleveland WW, Bejar RL, Lockhart WJr: Eye signs of hypophosphatasia. Arch Ophthalmo181:614-27, 1969.
38. Henthorn PS, Raducha M, Fedde KN, Lafferty MA, WhyteMP: Different missense mutations at the tissue-nonspecificalkaline phosphatase gene locus in autosomal recessivelyinherited forms of mild and severe hypophosphatasia. ProcNatl Acad Sci USA 89:9924-28, 1992.
39. Moore CA, Ward JC, Rivas ML, Magill HL, Whyte MP: In-fantile hypophosphatasia: autosomal recessive transmission
22 American Academy of Pediatric Dentistry Pediatric Dentistry - 18:1, 1996

to two related sibships. Am J Med Genet 36:15-22, 1990.40. Lundgren T, Westphal O, Bolme P, Modeer T, Noren JG: Ret-
rospective study of children with hypophosphatasia with ref-erence to dental changes. Scand J Dent Res 99:357-64,1991.
41. Macfarlane JD, Swart JG: Dental aspects of hypophosphatasia:a case report, family study, and literature review. Oral SurgOral Med Oral Pathol 67:521-26, 1989.
42. Macfarlane JD, Poorthuis BJ, Mulivor RA, Caswell AM:Raised urinary excretion of inorganic pyrophosphate in as-ymptomatic members of a hypophosphatasia kindred. ClinChim Acta 202:141^18,1991.
43. Wendling D, Cassou M, Guidet M: Hypophosphatasia inadults. Apropos of 2 cases. Rev Rhum Mal Osteoartic 52:43-50,1985. [French with English abstract]
44. Sorensen E, Flodgaard H: Adult hypophosphatasia. ActaMedica Scandinavia 197:357-60,1975.
45. Teree TM, Klein L: Hypophosphatasia: Clinical and metabolicstudies. J Pediat 72:41-50, 1968.
46. Jones AC, Chuck AJ, Arie EA, Green DJ, Doherty M: Dis-eases associated with calcium pyrophosphate deposition
disease. Semin Arthritis Rheum 22:188-202, 1992.47. Greenberg CR, Taylor CL, Haworth JC, Seargeant LE,
Philipps S, Triggs-Raine B, Chodirker BN: A homoallelicGly317—>Asp mutation in ALPL causes the perinatal (le-thal form of hypophosphatasia in Canadian Mennonites.Genomics 17:215-17, 1993.
48. Sly WS, Grubb J: Isolation of fibroblasts from patients. Meth-ods Enzymol 58:444-50,1979.
49. Macfarlane JD, Poorthuis BJ, van de Kamp JJ, Russell RG,Caswell AM: Hypophosphatasia: biochemical screening of aDutch kindred and evidence that urinary excretion of inor-ganic pyrophosphate is a marker for the disease. Clin Chem34:1937-41,1988.
50. Macfarlane JD, Kroon HM, van der Harten JJ: Phenotypicallydissimilar hypophosphatasia in two sibships. Am J MedGenet 42:117-21,1992.
51. Weiss MJ, Cole DE, Ray K, Whyte MP, Lafferty MA, MulivorRA, Harris H: A missense mutation in the human liver/bone/kidney alkaline phosphatase gene causing a lethal form ofhypophosphatasia. Proc Natl Acad Sci USA 85:7666-69,1988.
Future Annual Sessions of the American Academy of Pediatric Dentistry
49tn Annual Session
May 24-28,1996
ChicagoChicago Marriott Hotel
50th Annual Session
May 22-27,1997
PhiladelphiaPhiladelphia Marriott Hotel
51 St Annual Session
May 21-26,1998
San Diego
52nd Annual Session
May27-June1,1999
TorontoSan Diego Marriott Hotel & Marina J Sheraton Centre of Toronto Hotel & Towers
Pediatric Dentistry - 18:1, 1996 American Academy of Pediatric Dentistry 23