-
RevisedNationalTuberculosis ControlProgramme
(RNTCP)
Dr.NAVPREETAssistantProf.,Deptt.ofCommunityMedicine
GMCHChandigarh
-
ProblemStatementofTBinIndia
India
accounts
for
nearly
1/4th
of
global
burden
of
TB (2010).
Mortality:
26per1lacpopulation.
Prevalence(old+newcases):256per1lacpopulation.
Incidence(newcasesonly):185per1lacpopulation.
-
MillenniumDevelopmentGoals
Goal
6:
Combat
HIV/AIDS,
malaria
and
other diseases
Target
8:
By
2015,
to
have
halted
and
begun
to reverse
the
incidence
of
malaria
and
other
major
diseases Indicator
23:
between
1990
and
2015
to
halve
prevalenceofTBdiseaseanddeathsduetoTB
Indicator24:todetect70%ofnewinfectiouscasesand
to successfully
treat
85%
of
detected
sputum
positive patients
-
EvolutionofTBControlinIndia
1950s60s ImportantTBresearchatTRCandNTI
1962 NationalTBProgramme(NTP)
1992
ProgrammeReviewonly30%ofpatientsdiagnosed;ofthese,only30%treatedsuccessfully
1993 RNTCP
pilotbegan
1998 RNTCPscaleup
2000 >30%ofcountrycovered
2004 >80%ofcountrycovered
2006 EntirecountrycoveredbyRNTCP
-
NationalTuberculosisControl Programme
NTCPwasstartedin1962withaimtodetectcasesat
theearliest&treatthem.
However, Treatmentsuccessrate
:unacceptablylow
Death&defaultrate
:high
-
NeedForRevisedStartegy
in
1992,
nation
wise
review
was
conducted
with assistanceofSIDA&WHO.
NTPsufferedfrommanagerialweakness Inadequatefunding
OverrelianceonXraysfordiagnosis Frequentinterruptedsuppliesofdrugs
Lowratesoftreatmentcompletion.
In
1993,
GoI
decided
to
give
a
new
thrust
by revitalizingNTP.
RNTCPthusformulated
-
RevisedNational
TuberculosisControlProgramme
ObjectivesofRNTCP:
1.
To
achieve
and
maintain
a
cure
rate
of
at
least
85% amongnewlydetectedinfectious(newsputumsmear
positive)cases
2.Toachieveandmaintaindetectionofatleast70%of
suchcasesinthepopulation.
-
Revisedstrategy:
1.
Augmentation
of
organizational
support
at
centre andstatelevel.
2.
Usesputumtestingasprimarymethodofdiagnosis3.
Standardizedtreatmentregimen
4.
Ensuringregular,uninterruptedsupplyofdrugs5.
Emphasis
on
training,
IEC,
operational
research
&
NGOinvolvement.6.
Increasedbudgetoutlay
-
ComponentsofDOTS:
1.
Political
will
ensures
financial
support
and sustainability.
2.
Case
detection
with
the
help
of
quality
assured sputumsmearmicroscopy.
3.
Regularanduninterruptedsupplyofdrugs
patientwiseboxes
4.
Directlyobservedtreatment
directobservationwhilepatientisgettingtreatment.
5.
Systemicmonitoringandaccountability.
-
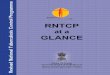
StructureofRNTCPatStatelevel
State TB Cell
District TB Centre
Tuberculosis Unit
Microscopy Centre
DOT Centre
STO, Deputy STOMO, Accountant, IEC Officer, SA, DEO
DTO, MO-DTC, LT, DEO, Driver
MO-TCSTS, STLS
MO, LT
DOT Provider MPW, NGO, PP, Comm Vol
Nodal point for TB control
One/ 5 lakh (2.5 lakh in hilly/ difficult/ tribal area)
One/ lakh (0.5 lakh in hilly/ difficult/ tribal area)
-
RecommendationoftheRNTCPNationalLaboratory
Committee(Oct2008)
Strongly
recommended
that
RNTCP
changes
diagnostic criteriaofSmear+vePTBasbelow:
TB
suspect
is
any
person
with
cough
for
2
weeks,
or more
Number
of
specimen
required
for
diagnosis
is
2,
with oneofthembeingamorningsputum
One
specimen
positive
out
of
the
two
is
enough
to declareapatientasSm+PTB
-
Basisofchanges
The
revised
definition
of
a
new
sputum
smear positivepulmonaryTBcaseisbasedonthepresence
ofatleastoneacidfastbacillus(AFB)inatleastone sputum
sample
in
countries
with
a
well
functioning
EQAsystem. The
reduction
of
the
number
of
specimens
to
be
examined
for
screening
of
TB
cases
from
three
to two,
in
places
where
workload
is
very
high
and
humanresourcesarelimited.
-
RevisedCategories
Treatmen tgroups
Typeofpatient Regimen
Intensive phase(IP)
Continuation phase(CP)
New(CatI)
NewsputumsmearpositiveNewsputumsmearnegativeNewextrapulmonaryNewothers
2H3R3Z3E3
4H3R3
Previously treated
(CatII)
SmearpositiverelapseSmearpositivefailureSmearpositivetreatment
afterdefaultOthers
2H3R3Z3E3
S3/1H3R3Z3E3
5H3R3E3
-
QualityAssurance
RNTCPLabnetworkhasthreelevels: NationalReferenceLaboratories
NTIBangalore TRCChennai LRSNewDelhi
IntermediateReferenceLaboratories Statelevel
NetworkofDesignatedMicroscopyCenters(>11,000)
Includesmicroscopycentersinmedicalcolleges
OneDMCcoversapopulationofabout1lakh
Providequalityassuredacidfastsputumsmearmicroscopy
services
-
RNTCPExternalQualityAssessment
Components
Paneltesting Onsiteevaluation
Randomblindedrecheckingofroutineslides
-
ExternalQualityAssessmentactivitiesofRNTCP
-
ReportingProcedure
-
HIV&TB
HIV
coinfection
strongest
known
risk
factor
for
the progressionoflatentTBinfectiontoactiveTBdisease
Estimated710%annualriskofreactivation,with60%lifetime risk
(cf.
10%
lifetime
risk
in
TB
infected,
nonHIV
infected
individual) Conversely,
TB
amongst
the
most
common
causes
of
morbidityandmortalityinpeoplelivingwithHIV/AIDS
Immune
response
to
TB
bacilli
increases
HIV
replication leadingtoarapidprogressionofHIVdisease
Optimal
access
to
DOTS
will
significantly
reduce
morbidity andmortalityinPLWHA
-
TB/HIVcollaborativeactivities
TB/HIV
Action
Plan
implemented
by
RNTCP
and
NACP jointly,focusingon:
Trainingofserviceproviders
Servicedeliverylinkages(ICTCRNTCPCrossreferrals) Monitoring
Information,Education,andCommunication
Implementationstarted: in
2001,
in
6
high
HIV
prevalent
States
(population
311
million) expanded
in
2004,
to
8
additional
States
(population
323
million)
-
TB/HIVcollaboratingactivities
National,
State
and
District
level
coordination
committees
to monitorlinkages
Guidelinesandtrainingmaterialdevelopedjointly
OngoingtrainingofstaffonTB/HIV Crossreferral
between
ICTC
and
DOTS
services
developed,
pilotedandimplemented InvolvementofNGOsandPPs
CollaborativeIECactivities Jointmonitoringofactivities
-
TreatmentofTBinHIV
TBcanbesuccessfullytreatedeveninHIVinfectedpts.
But,cannotalonepreventpeoplefromdyingofAIDS
InadditiontoTBtreatment,ARTandCPTneededforthose eligible
DOTSisthetreatmentofchoice IntermittentSCCiseffective
NationalpolicyistoprovideRNTCPCatItonewcasesand
CatIItoretreatmentcases
Higher
relapse
rates
have
been
observed
especially
in
those treatedwithnonRifampicincontainingregimen
Whethertruerelapseorreinfection?
DruginteractionsbetweenRifampicinandARVs
National
policy
is
to
start
ART
after
completing
antiTB treatment,
or
modify
ART
by
replacing
Nevirapine
with
EfavirenzforthedurationofTBtreatment
-
LikelyimpactofHIVonTBinIndia?
ScenariowithoutRNTCP
HIV
would
increase
TB
prevalence
(by
1%),
incidence
(by 12%),
and
mortality
rates
(by
33%)
between
1990
and
2015
ScenariowithRNTCP
Expect
substantial
reductions
in
prevalence
(by
68%), incidence(by41%),andmortality(by39%)between1990
and2015
Nationally,
RNTCP
should
be
able
to
reverse
the
increases
in
TB
burden duetoHIVbut,toensurethatTBmortalityisreducedby50%or
moreby
2015,
HIVinfected
TB
patients
should
be
provided
with
antiretroviral
therapyinadditiontotherecommendedtreatmentforTB
-
PediatricTuberculosis RelatedtoadultTB
Canoccuratanyage
Diseasedevelopswithinoneyearofinfection Younger,earlier=
disseminated
PTB:EPTB::55:45
PTBpaucibacillary,usuallyspneg
-
TreatmentofPediatricTB DOTS Categorization SAME
Dosesperkgbodyweight Drugs
to
be
made
available
as
combipacks in
patient
wise
boxes,
linked
to
child's
weight
(
610kg,1117kg,
1825kg,26 30kg)
PWB beingmadeavailable PC13yellow(610kg) PC14orange(1117kg)
Prolongationpouches
Pink(1825kg) Gray(2630kg)
-
MDRTBandDOTSPlus
MDRTBisalabdiagnosis,NOTaclinicalone
MDRTBlevelsoflessthan1%to3%innewcasesandof12%
inretreatmentcases.
EmergenceofresistancetoRifampicin
inonly2%ofpatients, despite
a
high
level
(8%)
of
initial
resistance
to
Isoniazid,
eitheraloneorincombinationwithotherantiTB
Quality
assured
laboratory
facility
for
culture
and
Drug SusceptibilityTestmustbeavailable(NB:2 4monthsdelay
beforeDSTresultsseen)
-
RNTCPCatIVtreatmentisa24monthstandardized2ndline
regimengivenunderdailyDOT:
6KmOfxEtoCsZE/18OfxEtoCsE
MDRTBpatientadmittedtoindoorfacilityatDOTSPlussite
forupto1monthfor:
pretreatmentassessment;
initiationofCategoryIVtreatmentafterdecisionofDOTS
Plussitecommittee; monitoringtolerancetotreatmentregimen;
counselingandhealtheducationtopatientandfamily;
developinglinkagestodistrictservices;and contacttracing
-
AchievementsofRNTCP
Treatmentsuccessrate:25%(1998)to88%(2010)
Deathrate:29%(1998)to4%(2010) 662DTCs 2,698TUs 13,039DMCs 1,971NGOs
>10,894Privatepractitioner 297Medicalcolleges
>13,000peripherallaboratories
-
Thanks.
Revised National Tuberculosis Control Programme(RNTCP)Problem
Statement of TB in IndiaMillennium Development GoalsEvolution of TB
Control in IndiaNational Tuberculosis Control ProgrammeNeed For
Revised StartegyRevised National Tuberculosis Control
ProgrammeRevised strategy:Components of DOTS:Structure of RNTCP at
State levelRecommendation of the RNTCP National Laboratory
Committee (Oct 2008)Basis of changesSlide Number 14Revised
CategoriesQuality Assurance RNTCP External Quality
AssessmentExternal Quality Assessment activities of RNTCPReporting
Procedure HIV & TBTB/HIV collaborative activitiesTB/HIV
collaborating activitiesTreatment of TB in HIVLikely impact of HIV
on TB in India?Pediatric TuberculosisSlide Number 26Treatment of
Pediatric TBMDR-TB and DOTS-Plus Slide Number 35Achievements of
RNTCPSlide Number 51