Embed Size (px)
Citation preview
Saladin Ch. 22 Respiratory System
Alveoli
Respiratory Processes
• Pulmonary ventilation - Inspiration and expiration
• External respiration - O2 into pulmonary circulation, CO2 out.
• Transport of gases
Respiratory Processes
• Internal respiration - O2 out of capillaries, CO2 in.
• Cellular respiration - metabolic reactions within cells that consume O2 and produce CO2.
Functions
• Gas exchange - O2 in, CO2 out
• Regulation of blood pH
• Sense of smell
• Filtering system for inspired air
Functions
• Sound production for communication
• Heat and water reduction
Respiratory System Components
• Upper Respiratory system = nose, nasal cavity, pharynx and associated structures.
• Lower Respiratory System = larynx, trachea, bronchi and lungs.
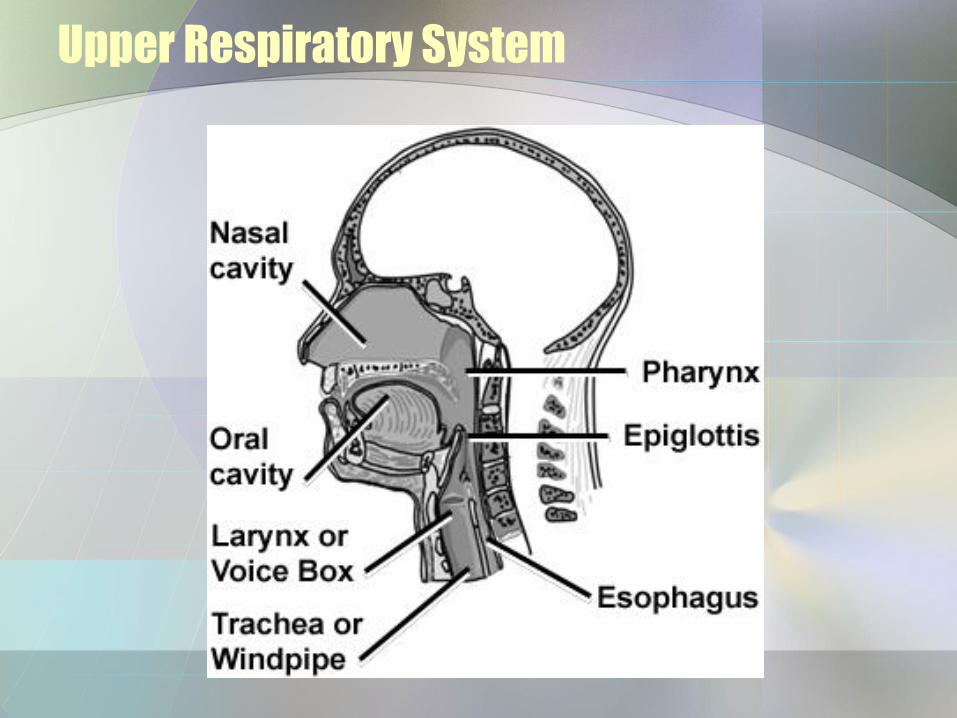
Upper Respiratory System
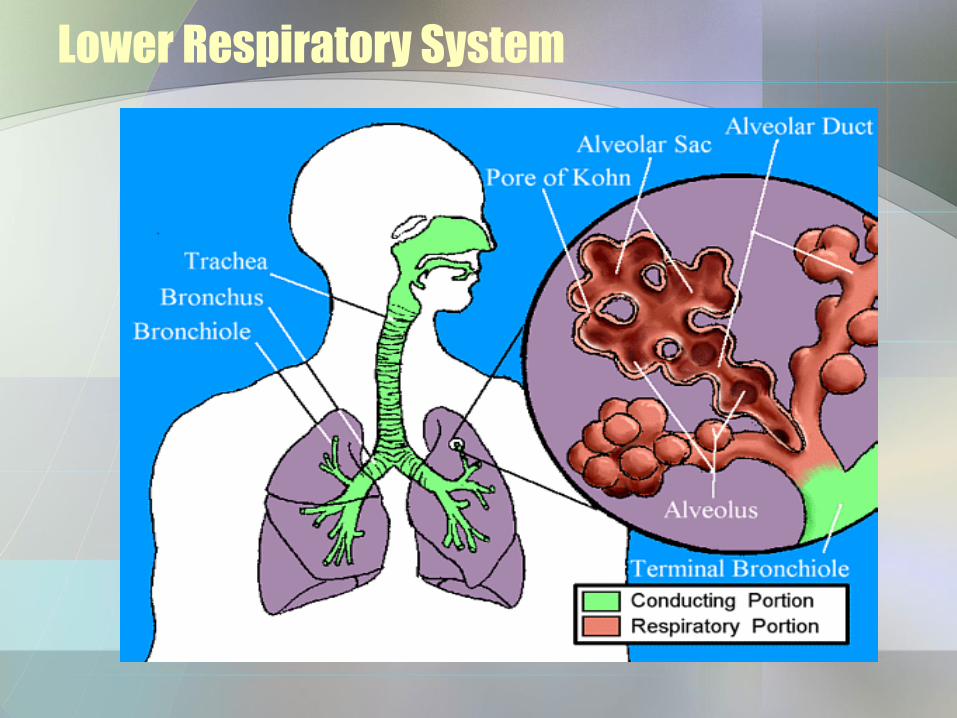
Lower Respiratory System
Respiratory System Components
• Conducting - nose, pharynx, larynx, trachea, bronchi, bronchioles, & terminal bronchioles - filter, warm & moisten air and carry to the respiratory portion.
• Respiratory Portion - tissues within lungs where gas exchange transpires.
Nose
• Functions - warm, moisten, filter air, smell, modifying speech sounds.
• External – Nose – Structures – root, bridge, dorsum
nasi, apex, philtrum.
– Bones - nasal, frontal, and maxilla.
Nose
– Cartilage - septal, lateral nasal and alar.
– External nares - openings into external nasal region from outside.
Nose
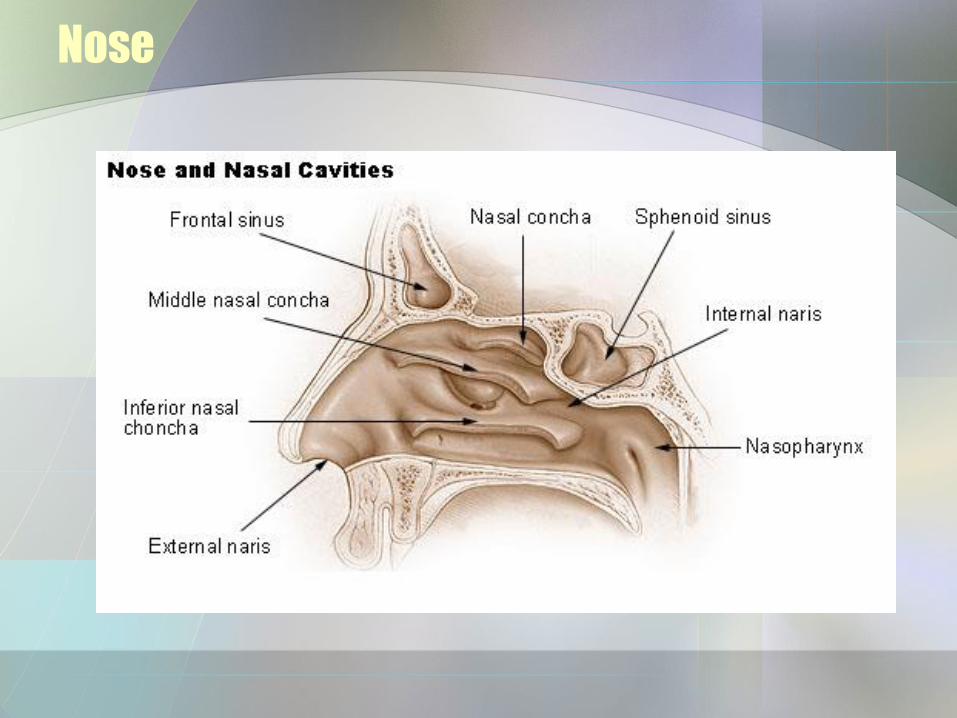
– Nasal cavity - space inside internal nose. Divided into R and L by nasal septum.
•Anterior portion is the vestibule - has nasal hairs.
Nose
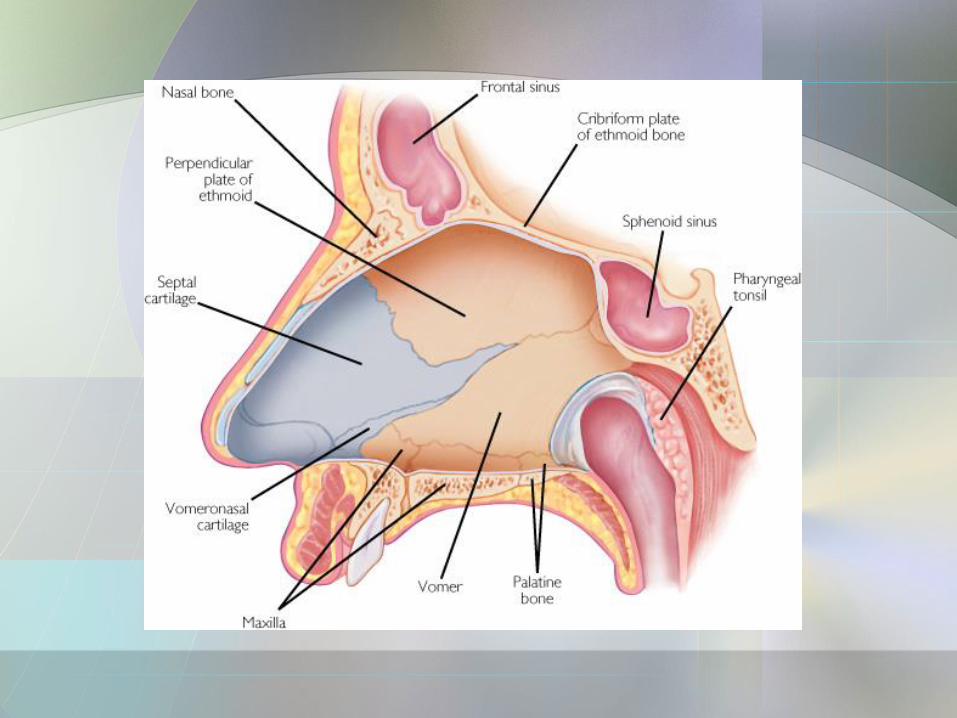
• Internal – nasal cavity
– Bones - ethmoid, maxilla, lacrimal, palatines, nasal conchae.
– Internal nares - openings from internal nasal region into pharynx.
– Ducts from paranasal sinuses, & nasolacrimal glands enter here.
Nose
– Superior, middle & inferior meatuses.
• Formed by coverings over the nasal conchae.
•Mucous membranes - olfactory epithelium in superior.
Nose
– Erectile tissue – inferior concha – swells and closes nostrils – alternates a couple of time per hour to allow for recovery from drying.
– Pseudostratified columnar epithelium with goblet cells - sweep and weep.
Nose
Pharynx
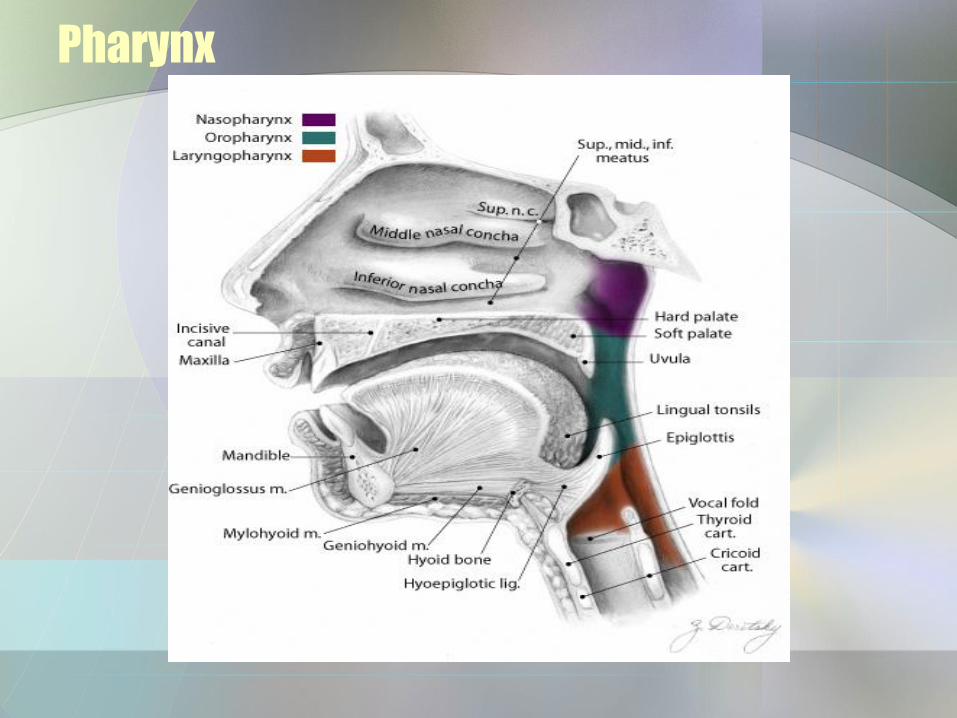
• Throat - from internal nares to cricoid cartilage [most inferior of laryngeal cartilages].
• Skeletal muscle wall lined with mucus membranes. 3 regions.
Pharynx
Pharynx
• Nasopharynx- from nasal cavity to plane of soft palate.
– Pseudostratified columnar epithelium.
– 5 openings - 2 internal nares, 2 auditory (Eustachian tubes), opening into oropharynx.
Pharynx
– Receives air from nares & mucus packets of trash to be removed.
– Also helps equalize ear pressure via the Eustachian tubes.
– Pharyngeal tonsils [adenoids] trap & destroy pathogens.
Pharynx
• Oropharynx - from nasopharynx to epiglottis.
– Common passageway for food, drink & air - digestive & respiratory.
– Stratified squamous epithelium - to withstand food abrasion.
– Lingual & palatine tonsils.
Pharynx
• Laryngopharynx - connects esophagus to voice box.
– Stratified squamous epithelium.
– Epiglottis to larynx.
Larynx
• Connects pharynx to trachea - C4-C6 region.
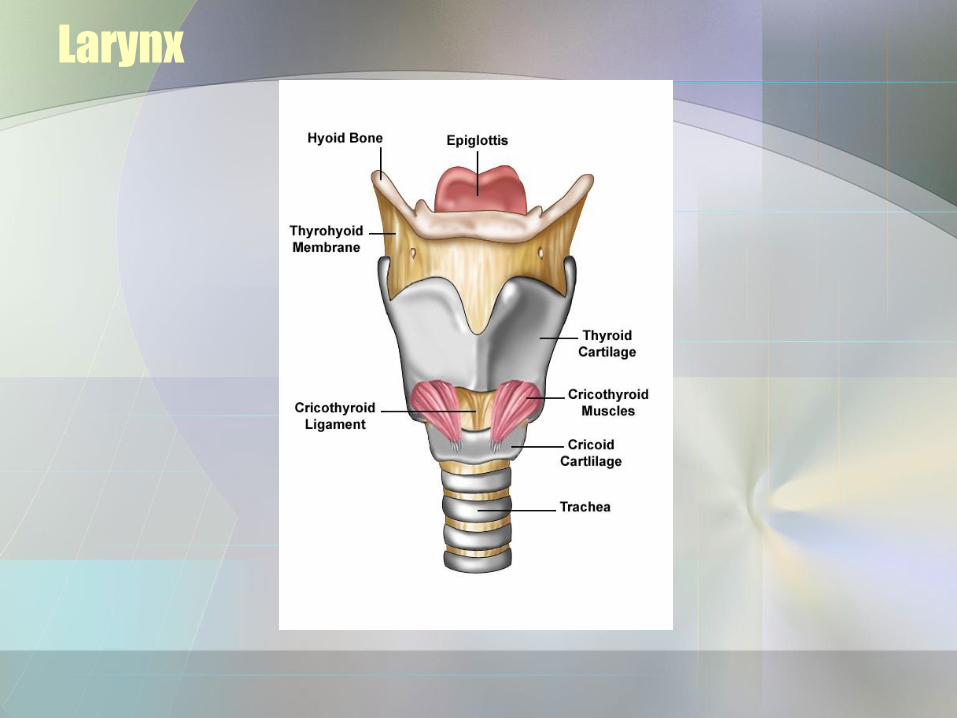
• From top to Bottom:
– Hyoid bone
– Thyrohyoid membrane
Larynx
• Epiglottis/glottis:
– Epiglottis attached to thyroid cartilage.
– Covers glottis (vocal cords & opening between) during swallowing - to prevent stuff from going the wrong way.
Larynx
Larynx
• Linings:
– Above larynx = non-keratinized stratified squamous.
– Below -pseudostratified columnar with cilia and goblet cells.
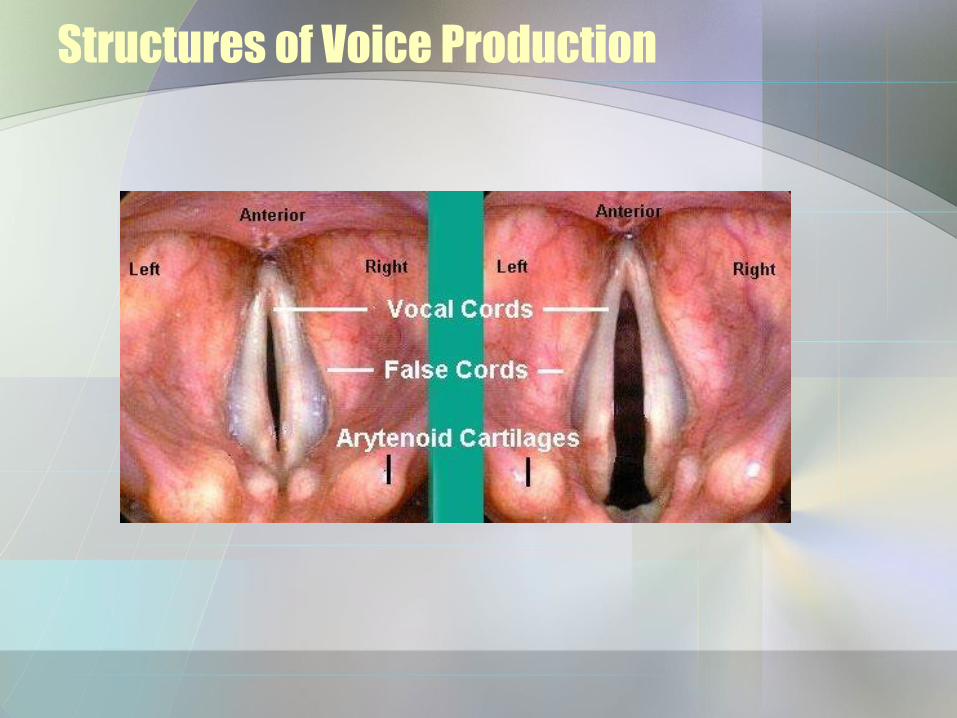
Structures of Voice Production
• Vestibular folds [false vocal cords -
superior] - hold breath in thoracic cavity by bringing folds together.
Structures of Voice Production
• Vocal folds [true vocal cords]
– Bands of elastic ligaments stretched between pieces of cartilage - like guitar strings.
– Skeletal muscles move the vocal folds into & out of the air stream & tighten or loosen the "strings“.
– More air - more volume.
Structures of Voice Production
Structures of Voice Production
• Shorter strings produce higher pitch.
– Men tend to have longer, thicker "strings" thus lower voices.
• Shape of the resonating chamber affects intonation, etc. - like with any instrument.
– Cheeks, tongue, lips etc. contribute.
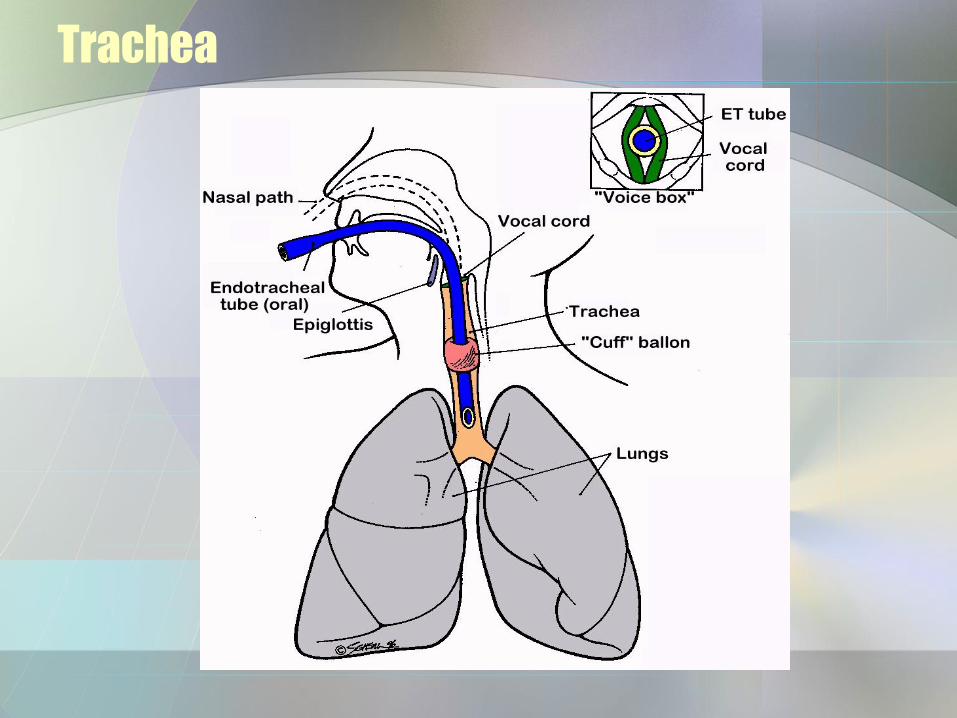
Trachea
• From larynx to fifth thoracic vertebra.
• 12 cm long, 2.3 cm diameter.
• Anterior to esophagus.
• Passageway for air and filters air.

Trachea
Trachea
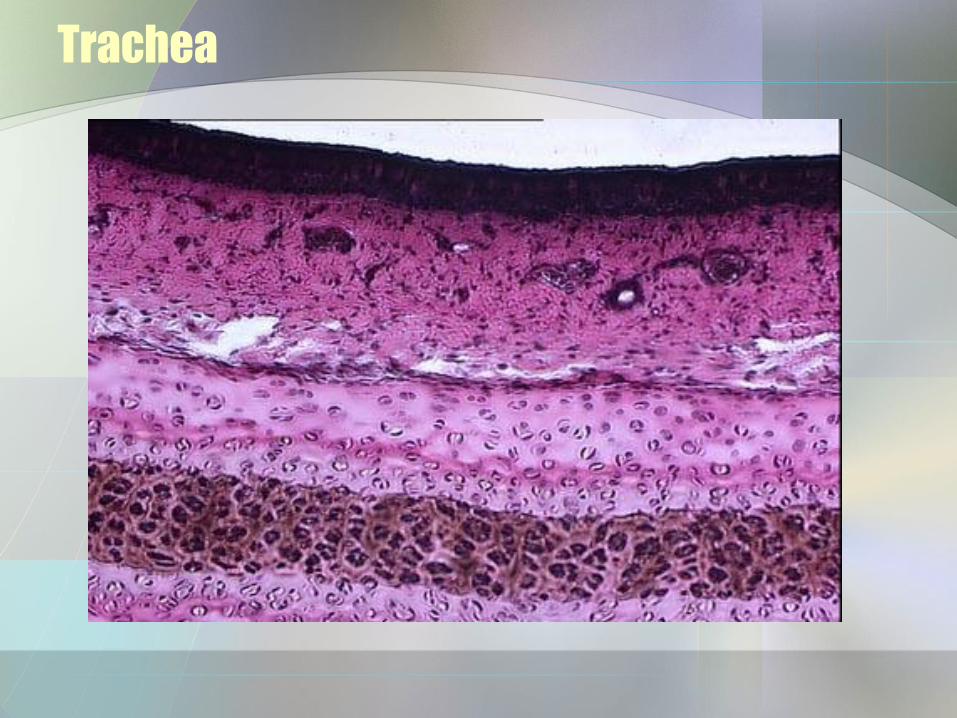
• Layers:
– Mucosa [pseudostratified ciliated columnar epithelium with goblet cells.
– Submucosa - contains ducts and glands; connective tissue & muscle between ends = trachealis muscles.
Trachea
– Adventitia - outer layer - loose connective tissue.
– Cartilagenous layer - 16 to 20 c-shaped rings with transverse smooth.
Trachea
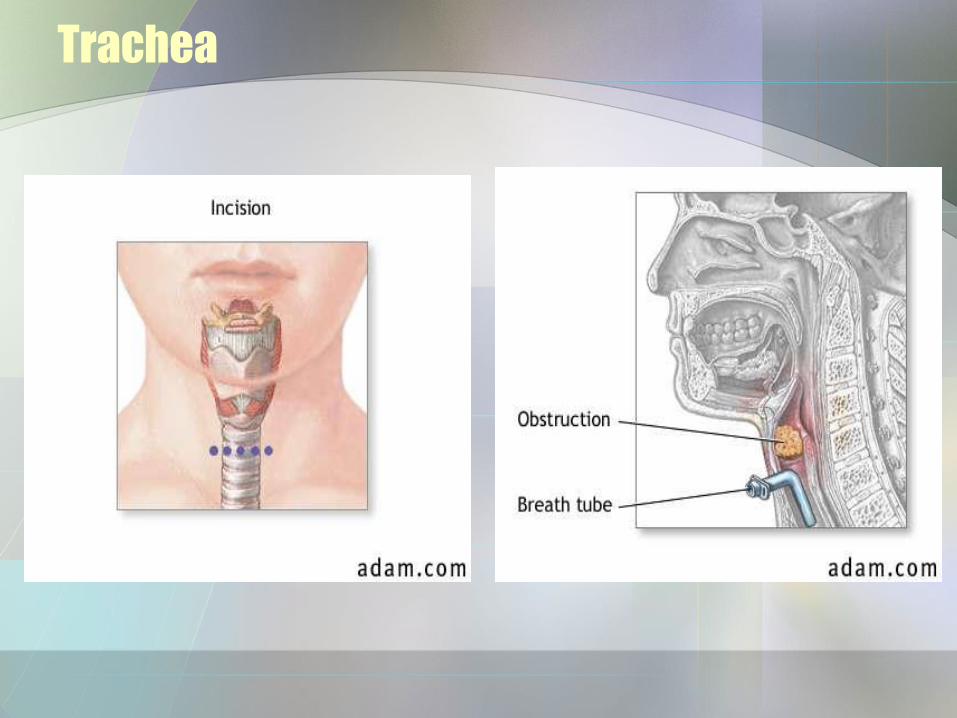
Trachea
• Tracheostomy - incision into trachea just inferior to cricoid cartilage - then place a tube.
• Intubation - the ramrod approach - just shove any obstruction down the tube, then suction out the mess.
Trachea
Trachea
Bronchi
• Trachea branches into R & L primary bronchi.
– Carina - branch point - very sensitive - has cough reflex.
– R is more vertical, shorter & wider - more likely to get inhaled objects.
– L is longer and narrower.
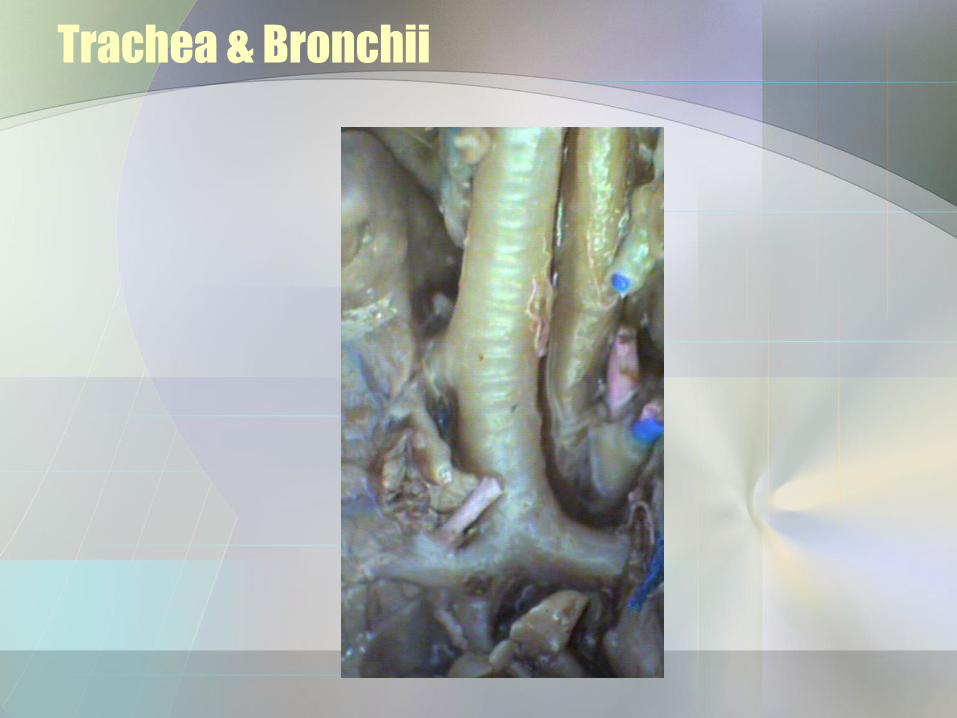
Trachea & Bronchii
Lungs
• External Anatomy Features:
– Base, apex, hilus [where vessels, bronchi, etc. enter each lung].
– Costal surfaces, cardiac notch.
Lungs
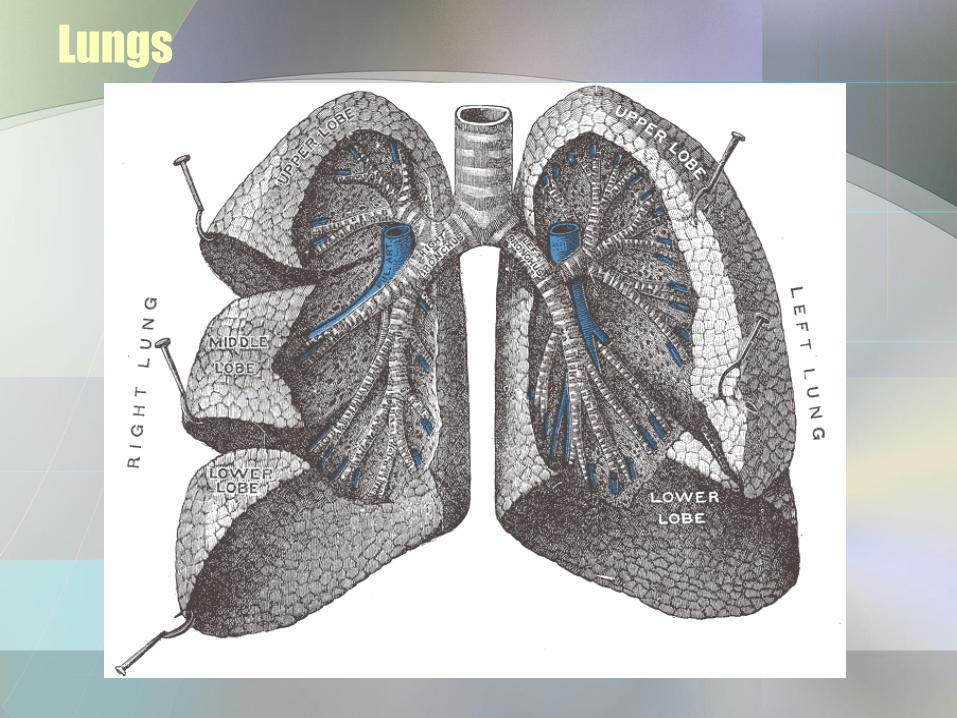
– Fissures - divide the lungs into lobes.
•Oblique - in both divides into superior and inferior lobe.
•Horizontal - R only; splits the superior to form a third, medial lobe.
Lungs
Bronchi
• Anatomy:
– Surrounded by incomplete rings of cartilage like trachea.
– Lined with pseudostratified ciliated columnar epithelium.
Bronchi
• Branching:
– Primary bronchus secondary
bronchi - to each lobe - 3 to R & 2 to L.
– Secondary tertiary – to 10 [R] or 8
[L] bronchopulmonary segments per lung.
Bronchi
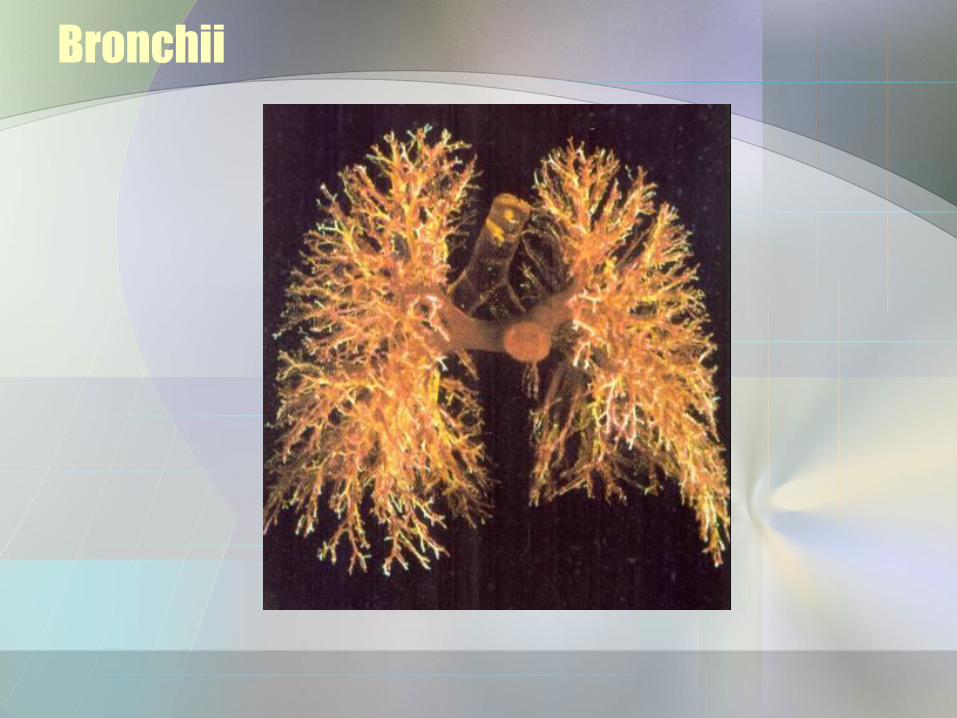
– Tertiary branch to bronchioles that branch to terminal bronchioles, etc.
– Total of 25 branching divisions.
– Pulmonary arteries & branches parallel bronchial tree
Bronchii
Bronchi
• Anatomic changes with branching:
– C cartilage replaced by plates which disappear by bronchiole level.
– With decreased cartilage, smooth muscle increases.
– At bronchiolar level simple cuboidal epithelium replaces pseudostratified ciliated columnar.
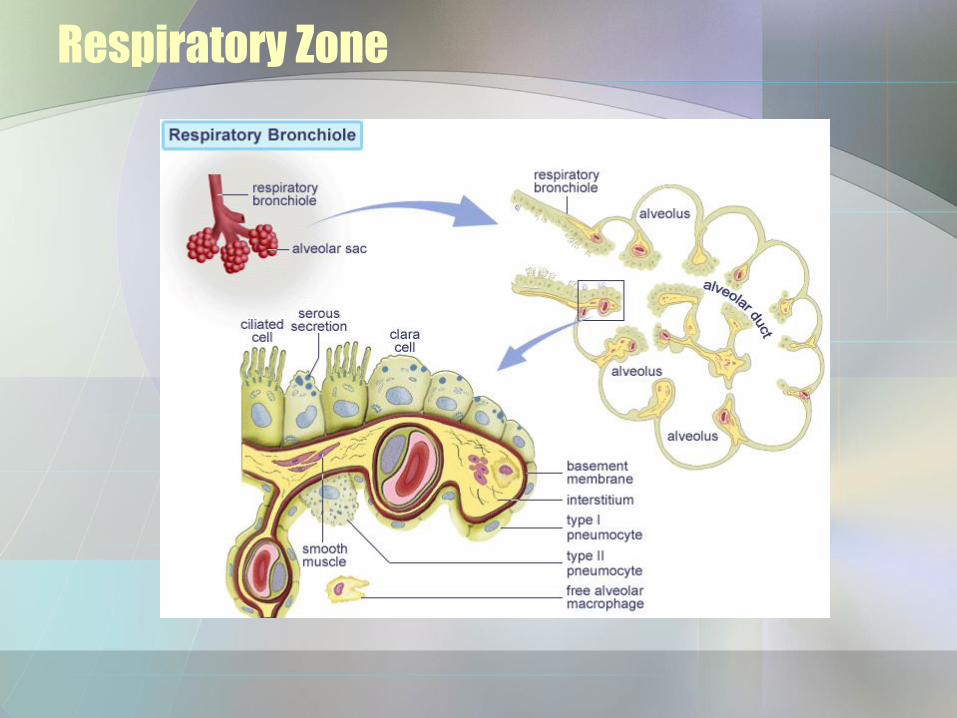
Respiratory Zone
• Alveoli [“cup-shaped”]:
– Simple squamous epithelium = type I alveolar cells - most of the lining.
– Septal cells = type II cells - interspersed with the type I's make surfactant - provides a film for diffusion and reduces surface tension to prevent collapse.
Respiratory Zone
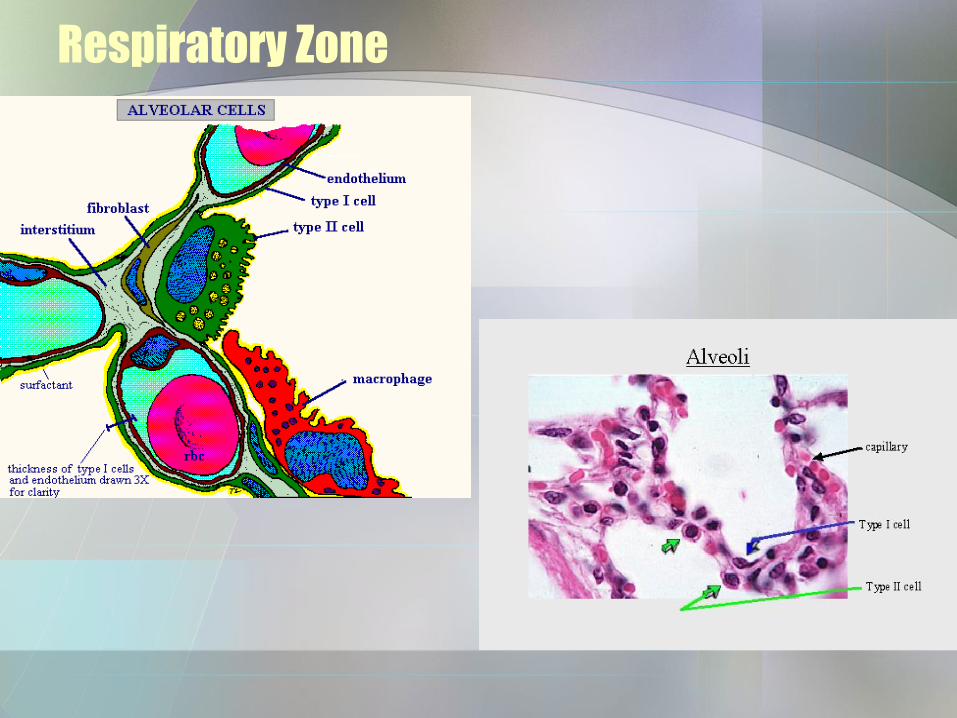
Respiratory Zone
– Alveolar macrophages - trap and dispose of dust and debris.
– Fibroblasts - produce reticular and elastic fibers.
– Alveoli are intimately associated with extensive capillary networks.
Respiratory Zone
Respiratory Zone
• Alveolar-capillary "respiratory membrane“:
–About 0.5 micron thick.
–4 layers:
1 - Alveolar wall - simple squamous, septal cells + macs.
Respiratory Zone
2 - Epithelial basement membrane.
3 - Capillary basement membrane.
4 - Endothelial cells of capillary - simple squamous.
• There are about 300 million alveoli in the lungs with a net surface area of about 70 square meters.

Respiratory Zone
Respiratory Membrane
PLEURAL MEMBRANES
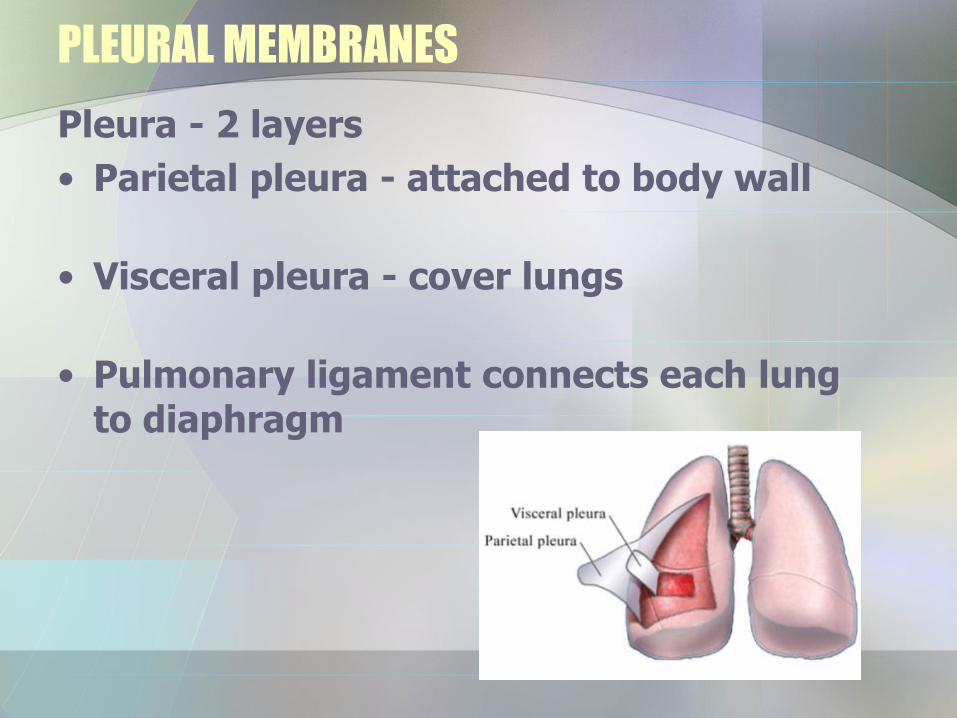
Pleura - 2 layers
• Parietal pleura - attached to body wall
• Visceral pleura - cover lungs
• Pulmonary ligament connects each lung to diaphragm
PLEURAL MEMBRANES
• Between is the pleural cavity containing serous fluid.
• Functions: reduction of friction, creation of pressure gradient, compartmentalization
Pulmonary Ventilation
• Respiratory cycle = 1 inspiration & 1 expiration
• Ventilation requires a pressure difference between outside and inside of lungs
Pulmonary Ventilation
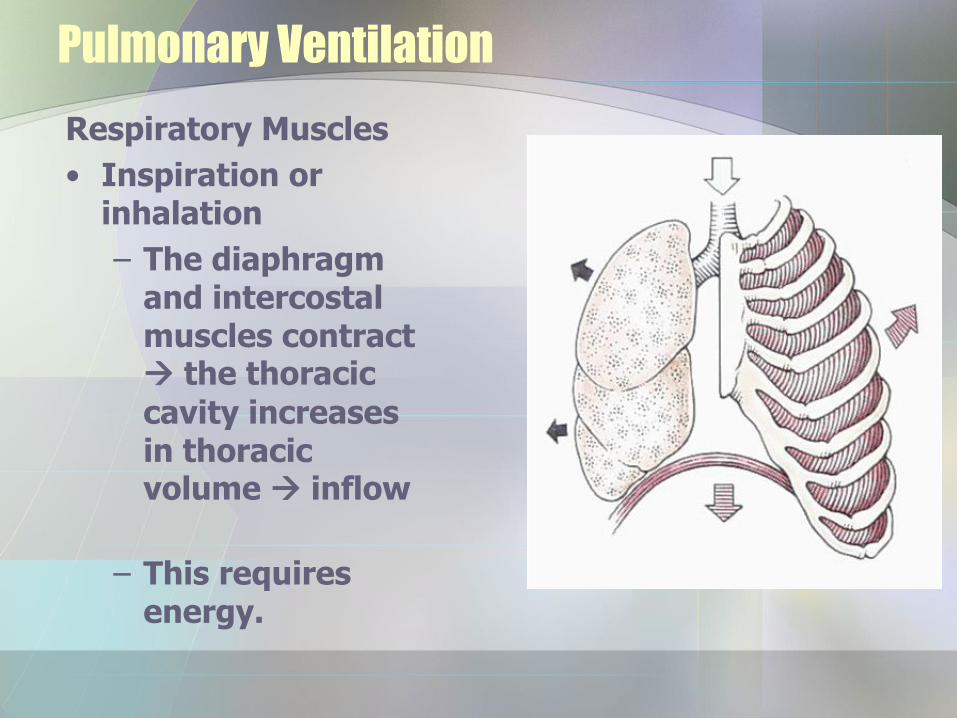
Respiratory Muscles
• Inspiration or inhalation
– The diaphragm and intercostal muscles contract the thoracic
cavity increases in thoracic volume inflow
– This requires energy.
Pulmonary Ventilation
• Expiration or exhaling
– Diaphragm and intercostal muscles relax - passive - no energy input. The thoracic cavity decreases in size outflow
Control of Respiration
• Cortical & brainstem
• Cortical Controls - Cerebral cortex - conscious control - can alter pattern, but cannot kill oneself by holding breath - pCO2 will force inspiratory area to act.
Control of Respiration
Brain stem
• Medulla rhythmicity area [Dorsal Respiratory Group]. – Inspiratory center - fires in a regular
pattern.
– Expiration areas - only kicks with forceful exhalation.
Control of Respiration
• Pons. – Pontine respiratory group
(Pneumotaxic center) - superior pons.
• Inhibitory - limits length of inspiration
•Can result in increased rate of breathing.
Factors Influencing Breathing Rate
Modified in response to changing demands
– Chemoreceptors
•Central - medulla - sample cerebrospinal fluid
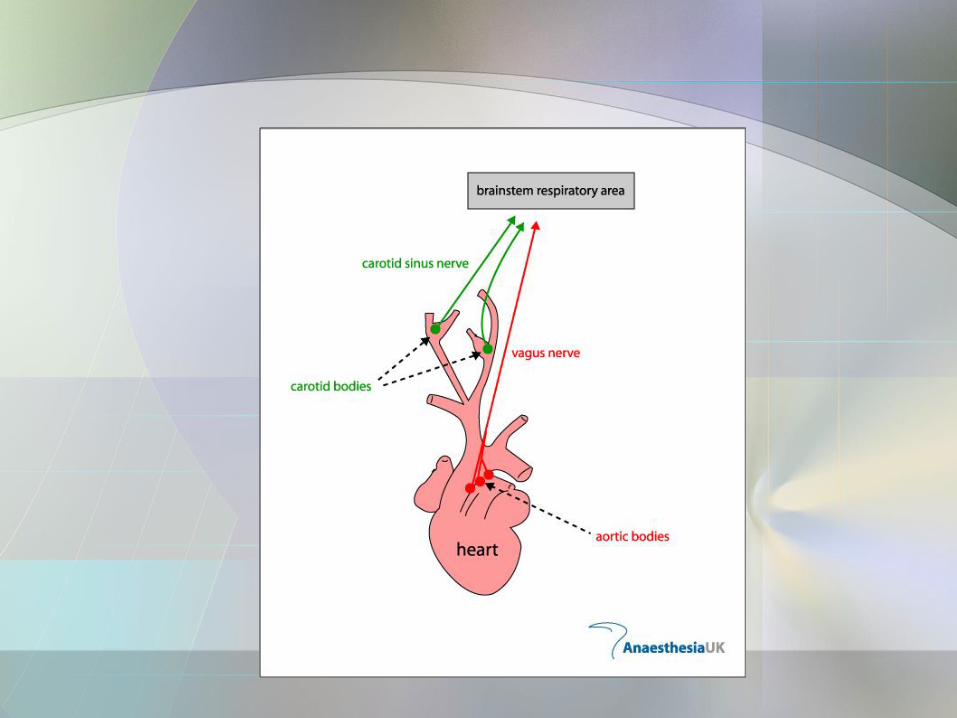
•Peripheral - carotid bodies and aortic bodies -test blood
Factors Influencing Breathing Rate
• Influence of pCO2
– Monitor pCO2 and H+ [peripherals also monitor pO2]
– Send information back to medulla, etc.
– Hypercapnia [increased CO2]
hyperventilation to correct
– Hypocapnia hypoventilation
Factors Influencing Breathing Rate
• Influence of pO2
– low arterial pO2 hypoxic drive
• Influence of arterial pH
– decreased pH inc ventiliation
Factors Influencing Breathing Rate
• Stretch receptors
– Monitor bronchi, etc. smooth muscle
– Hering-Breuer reflex – prevents over-stretching
• Irritants – shallower brathing; apnea
Pressure, Resistance & Airflow
Gas Laws
• Boyle's Law - The pressure of a gas is inversely proportional to the volume of the container.
– Thus, increases in volume produce decreases in pressure and visa versa.
Pressure, Resistance & Airflow
• Charles’ Law – as temperature increases, volume increases.
• Dalton's Law of Partial Pressures - each gas in a mixture exerts its own pressure. The total pressure of the mixture equals the sum of the pressures of each gas present
PO2 = 21% of 760 torr = 160
PCO2 = 0.04% = 0.3 torr
PN2 = 79% of 760 = 597 torr
Pressure, Resistance & Airflow
• Henry's Law -the quantity of a gas that will dissolve in a liquid is proportional to the partial pressure of that gas and its solubility coefficient [assume constant T]
• Solubility coefficients: O2 = 0.024, CO2 = 0.57, N2 = 0.012
Pressure, Resistance & Airflow
• N2 has low solubility under normal atmospheric conditions, so even though it makes up most of the pressure of air, little gets dissolved and taken up.
• N2 narcosis - under pressure - diving for example - more gets dissolved in the water of the alveoli and taken into the blood. When the external pressure drops again, it comes out of solution forming of bubbles = embolus
Pressure & Airflow
• Air flow = pressure difference between alveoli and atmosphere
Resistance
• Atmospheric pressure “drives” respiration. 1atm = 760 torr
• Pressure can be changed by volume changes or by temperature changes.
Pressure & Airflow
• If lung volume ↑, intrapulmonary [inside
lungs] pressure [Boyle’s Law]
• Bulk flow is from areas of high pressure to low.
Inspiration
• General information:
– Normal atmospheric pressure is 760 torr.
– Intrapleural pressure is 756 before inhalation and is always about 4 torr less than the alveolar pressure
Inspiration
• Increase in volume of thorax also increases volume of lungs decreases
the pressure inside the lungs below atmospheric - air flows in from the higher outside pressure to the lower inner.
• Temperature changes in the inspired gases also adds to inflation – Charles’ law – as T increases, V increases.
Inspiration
• Inspiration or inhalation: – The diaphragm & intercostal muscles
contract the thoracic cavity increases in volume.
– The increase in volume decreases the pressure inside the lungs below atmospheric.
– Air flows in from the higher outside pressure to the lower inner.
Inspiration
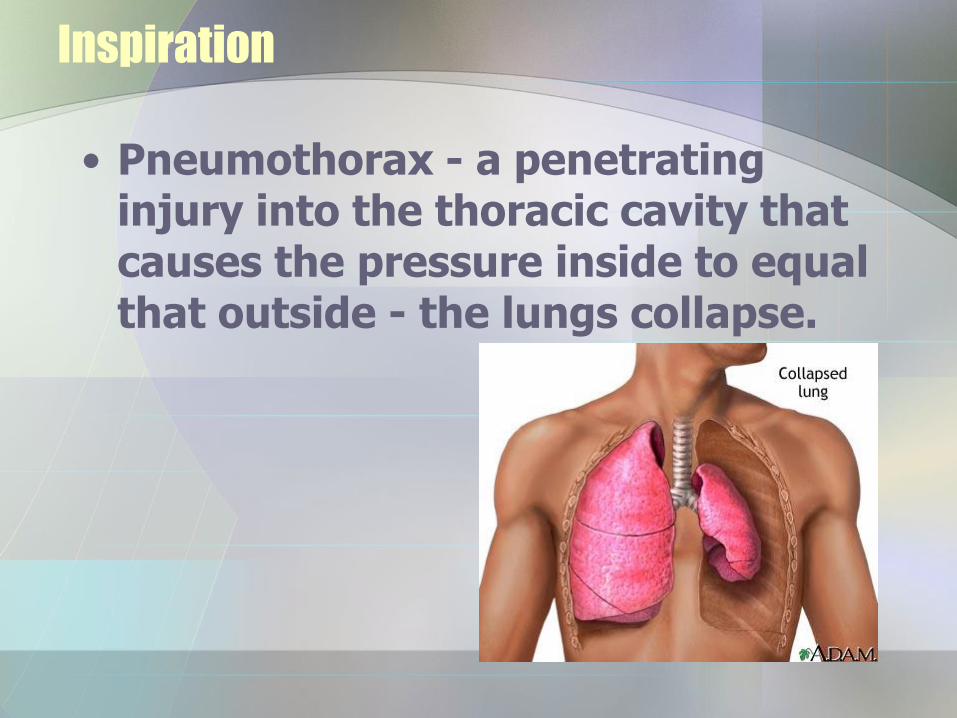
• Pneumothorax - a penetrating injury into the thoracic cavity that causes the pressure inside to equal that outside - the lungs collapse.
Pulmonary Ventilation
Physical Factors Affecting Ventilation:
Resistance of Airways
Air flow = pressure difference between alveoli & atmosphere
Resistance
• Bronchiole constriction or dilation - remember from hemodynamics, resistance is a function of radius.
Pulmonary Ventilation
• Inhaled irritants & inflammatory chemicals can cause airway constriction.
• Also get increased resistance with excessive mucous, tumors, etc.
• Reduce by sympathetic system – epinephrine.
Pulmonary Ventilation
• Pulmonary compliance- ease with which chest and lungs expand
– Affected by elasticity. TB, black lung, etc. decrease
Pulmonary Ventilation
Alveolar Fluid Surface Tension
• An inward directed force that accounts for 2/3 of lung recoil during expiration.
• Keeps the alveoli from collapsing.
Pulmonary Ventilation
• Surfactant
– Produced by the septal cells of the alveoli.
– Makes a fluid layer on the inner surface of the alveoli that decreases surface tension so walls don’t stick together.
Pulmonary Ventilation
– Deficient in Premees –
• IRDS – infant respiratory distress syndrome - At exhalation the alveoli collapse and their walls stick together – effort is required to pull them back apart
Alveolar Ventillation
• Air in conduction system = dead air – can be increased with disease and inability to do gas exchange in a region.
– “normal” dead space = 150mL.
– Normal resting inhalation = 500mL.
– Alveolar ventilation rate = [500 – 150] X 12 breaths per min [resting state]
Alveolar Ventillation
• Alveoli never completely empty - leftover is Residual Volume - air which remains in lungs even after forced exhalation = 1200mL
PULMONARY VOLUMES & CAPACITIES
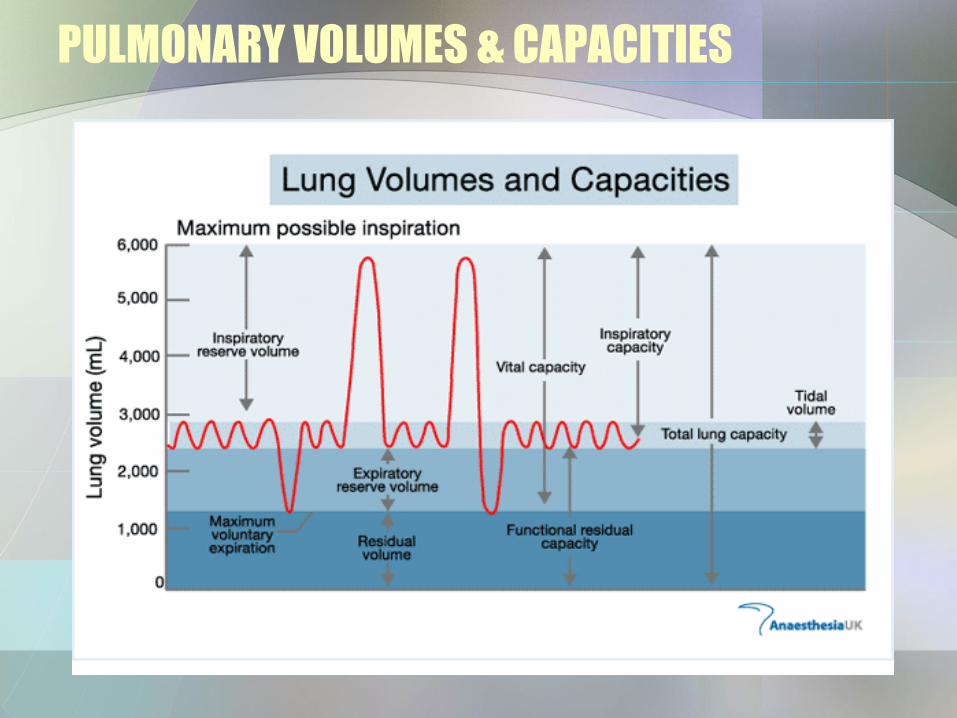
• Tidal Volume - amount of air moved by one breath in & out = 500mL
• Inspiratory Reserve Volume - excess inhaled above normal tidal air flow = 2100-3200mL
PULMONARY VOLUMES & CAPACITIES
• Expiratory Reserve Volume - forcibly exhaled air above normal amount = 1200mL
PULMONARY VOLUMES & CAPACITIES
• Inspiratory Capacity - total inspiratory ability of lung - sum of tidal volume & inspiratory reserve = 2600-3700mL
• Functional Residual Capacity - air not cleared from lungs with normal breath - sum of residual volume & expiratory reserve = 2400mL
PULMONARY VOLUMES & CAPACITIES
• Vital Capacity - amount that can be moved in lungs from normal tidal air with excess inhalation followed by forcible exhalation - sum of inspiratory reserve, tidal volume & expiratory reserve = 4800mL
• Total Lung Capacity - sum of inspiratory reserve, tidal volume, expiratory reserve & residual volume = 6000mL
PULMONARY VOLUMES & CAPACITIES
PULMONARY VOLUMES & CAPACITIES
• Minute Volume of Respiration - total air taken in in 1 minute = 500mL/breath X 12 times/min = 6000mL/min
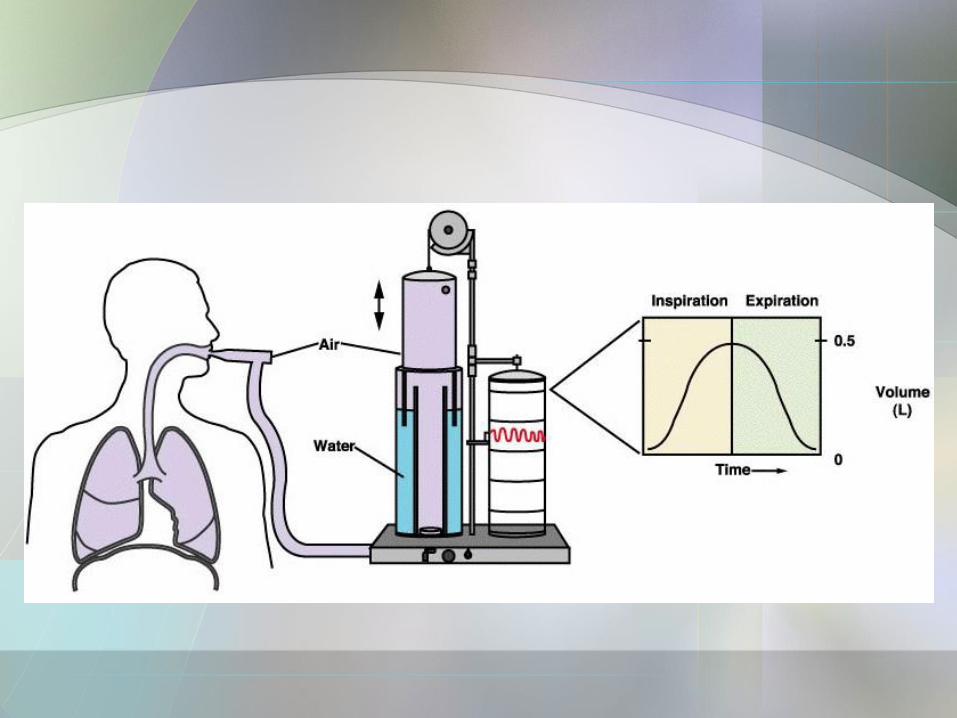
Pulmonary Function Tests
• Spirometer
– Can distinguish obstructive pulmonary disease [increased airway resistance].
•Asthma or chronic bronchitis
– From restrictive disease due to reduction of lung capacity.
• Fibrosis, emphysema, TB
Pulmonary Function Tests
– Obstructive Pulmonary Disease produces increased TLC, FRC and RV
– Restrictive Disease produces decreased VC, TLC, FRC and RV
External Respiration [Gas Exchange]
• Between alveoli & pulmonary caps.
• Gas exchange due to pressure gradient.
• Involves diffusion Press. In blood In alveoli Result
PO2 40 95 O2 goes into blood
PCO2 46 40 CO2 leaves
External Respiration
• Rate depends on: – Partial pressure differences.
– Solubility and molecular weight of gases
• O2 lower mass - diffuses faster
• CO2 is 20X as soluble as O2 in fluid portions of respiratory membrane
• Net effect - CO2 comes out about 20 times faster than O2
External Respiration
– Surface area for gas exchange.
– Diffusion distance
• Thin membrane,
•RBC's in single file
External Respiration
• Ventilation-Perfusion Coupling – air exchange and capillary flow
– Ratio = 4.2 L air/min:5.5 L blood/min = 0.8 normal
– Pulmonary vessels constrict in response to low O2 - opposite of the rest of the circulation - allows blood to bypass regions that are poorly aerated
Gas Transport
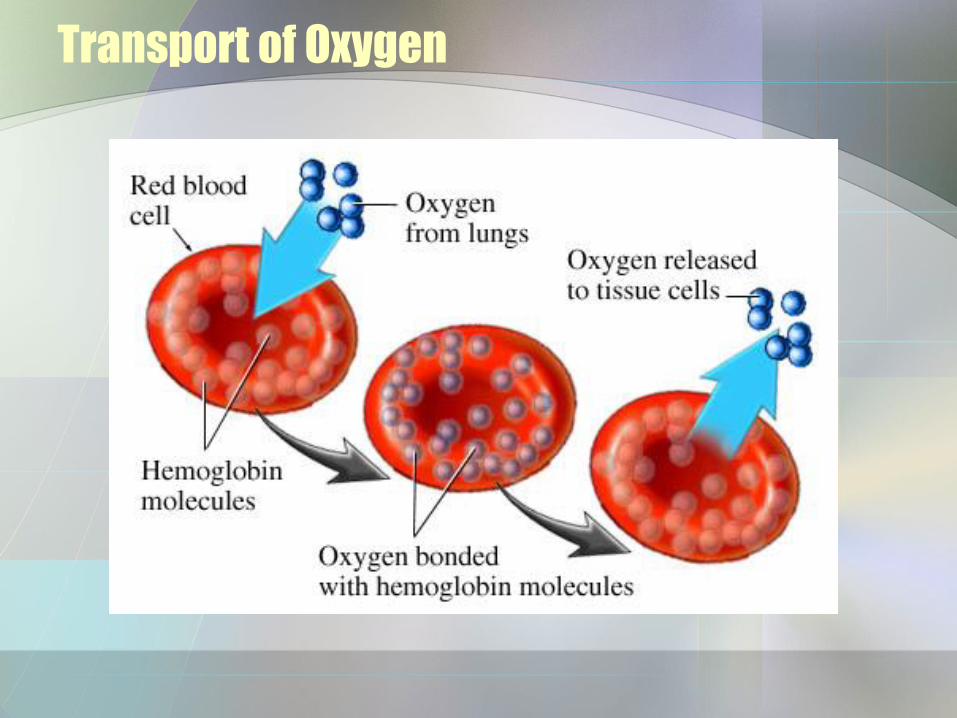
• Transport of oxygen
– 1.5% of what is taken in is carried dissolved in plasma. The rest is bound to hemoglobin (Hgb) reduced Hgb + O2 HgbO2 OxyHgb)
– 100% saturation = 4 molecule of oxygen/ Hgb
Transport of Oxygen
Gas Transport
• Transport of carbon dioxide
– CO2 is transported in blood – 90% carbonic acid
– [CO2 + H2O H2CO3 HCO3- + H+]
– 5% binds hgb, 5% dissolved in blood
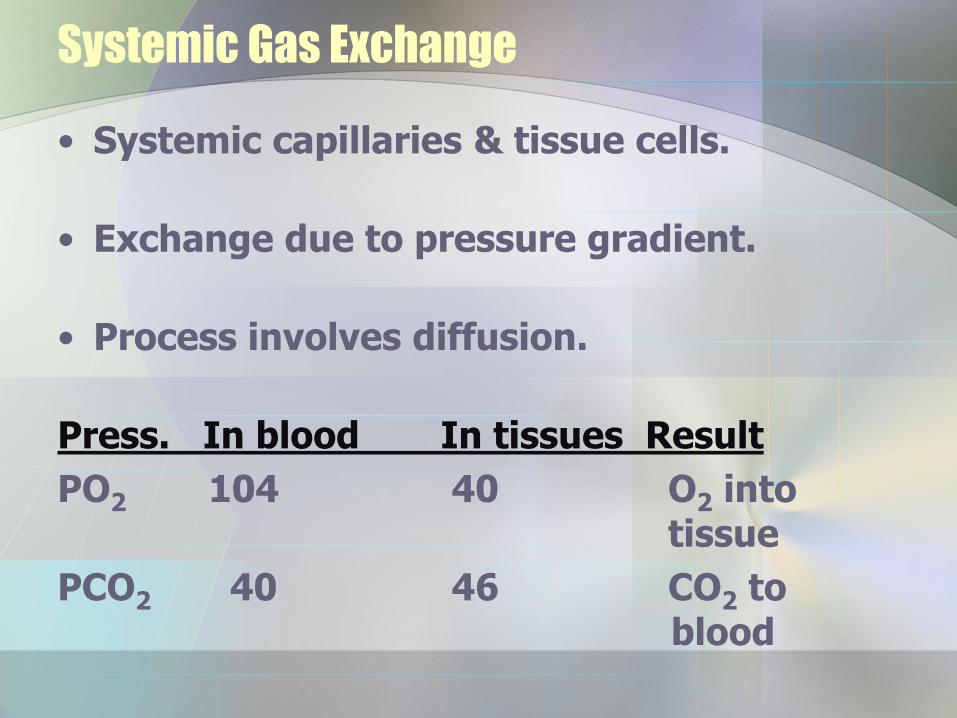
Systemic Gas Exchange
• Systemic capillaries & tissue cells.
• Exchange due to pressure gradient.
• Process involves diffusion.
Press. In blood In tissues Result
PO2 104 40 O2 into tissue
PCO2 40 46 CO2 to blood
CO2 Unloading
• CO2 diffuses into tissue capillaries. Some stays in plasma, some enters RBC's.
• In RBC's some of the CO2 binds to the globin portions of hemoglobin molecules forming carbamino associations.
CO2 Unloading
• The rest of the gas is converted by the enzyme carbonic anhydrase into carbonic acid.
• The acid dissociates into H+ ions and bicarbonate ions [HCO3
-].
• Most bicarbonate is pumped out of rbc in exchange for Cl- ions = chloride Shift
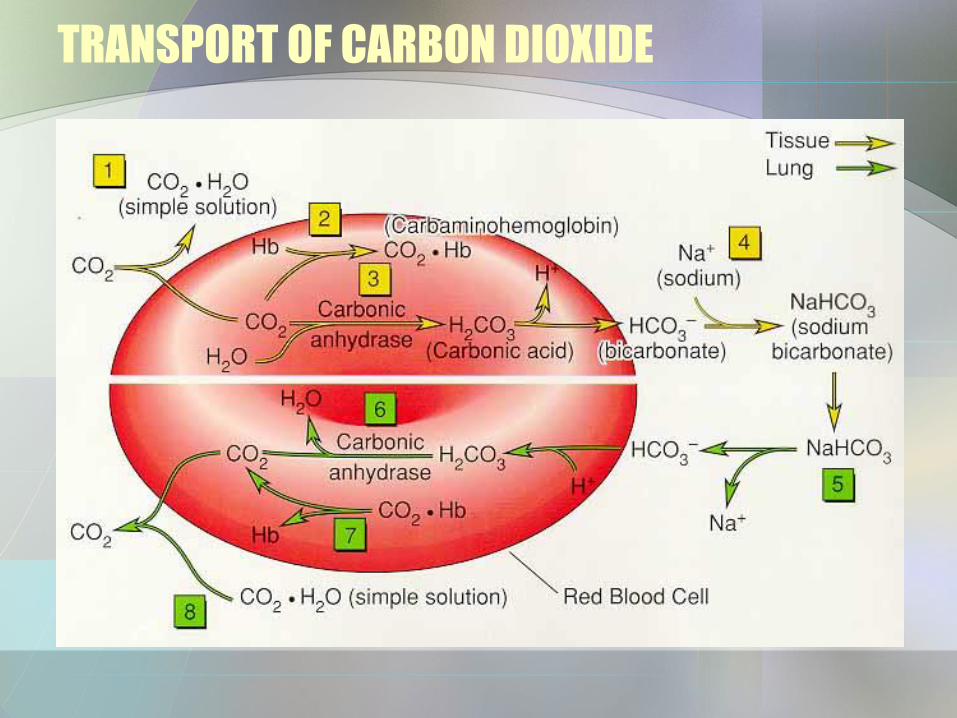
TRANSPORT OF CARBON DIOXIDE
O2 Unloading
• O2 unloading - Pressure gradient;
• H+ reduces O2 affinity of Hgb.
Transport of Oxygen
• Factors affecting uptake and release:
1 - pO2 – Cooperative Binding [positive feedback system].
As more O2 is available, more is
bound to Hb.
As pO2 drops, O2 is released from Hb.
Transport of Oxygen
2 - BPG [2,3biphosphoglycerate - an intermediate product in glycolysis].
Increasing levels mean high metabolism and more O2 is released to tissues.
Transport of Oxygen
3 – Temperature.
Increasing temperature increases release of O2 from Hb.
Transport of Oxygen
4 - Bohr effect [pH].
H+ ions bind to Hb, changing its structure.
This decreases its ability to carry O2,& O2 is released to tissues. Acid is produced during metabolic activities high H+ means high metabolism & high use of O2.
Transport of Oxygen
5 - Haldane Effect – as PO2 decreases and hemoglobin saturation decreases, the amount of CO2 carried by hemoglobin increases. This encourages CO2 exchange
Blood Gases & Respiratory Rhythm
• H+ that accumulate in blood get transferred to CSF – has less buffer, so sees more acid. Receptors respond.
– Acidosis – blood pH below 7.35, Alkylosis – above 7.45
– Slow and shallow breathing increase CO2 in blood, increases acid, decreases pH = respiratory acidosis – respiratory correction = hyperventillation
Blood Gases & Respiratory Rhythm
– Rapid, deep decreases CO2, increases pH = respiratory alkalosis; Corrected by hypoventillation
Blood Gases & Respiratory Rhythm
• Adjustments to Altitude
– Decreased barometric pressure decreased pO2 hyperventilation
– Acclimatization-inc number of erythrocytes
• Adjustments during Exercise
– increased exercise increased
ventilation [pO2, pCO2, pH remain constant]
Transport of Oxygen
Homeostatic Imbalances
• Hypoxia – too little oxygen.
– Anemic – due to low hematocrit or hemoglobin.
– Ischemic – due to poor circulation.
– Histotoxic – due to a ventilation problem.
Transport of Oxygen
Homeostatic Imbalances
• Oxygen toxicity – 100% at > 2.5 atm.
Disorders
• COPD.
– Chronic Obstructive Pulmonary Disease.
– Associated with a history of smoking.
– Labored breathing, frequent coughs & infections.
Disorders
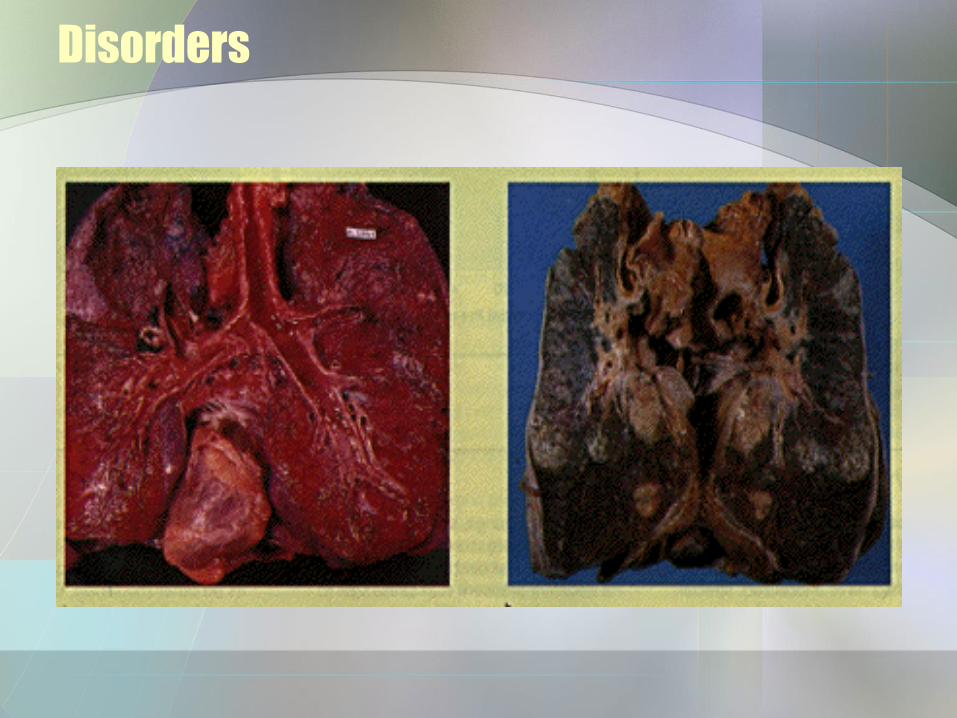
– Most develop respiratory failure.
– Ex. Emphysema - destruction of alveolar walls with loss of exchange surface.
Disorders
Disorders
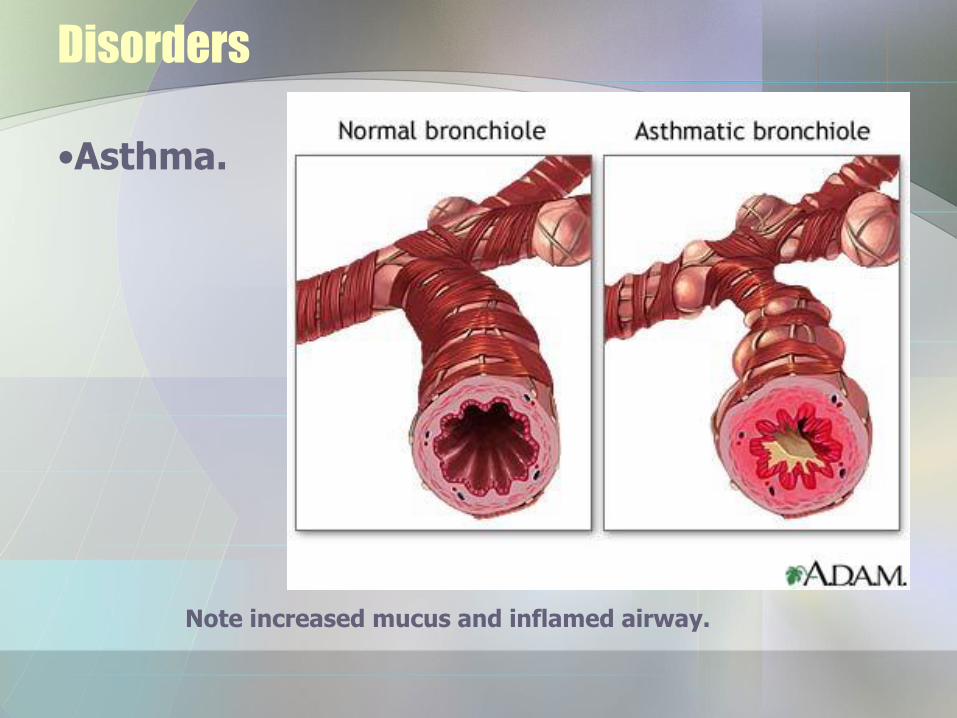
• Asthma – Coughing, wheezing, labored
breathing.
– Inflammation of bronchioles.
– Source – perhaps viral or bacterial.
– Triggers – environmental irritants.
– Some are associated with allergies.
Disorders
•Asthma.
Note increased mucus and inflamed airway.
Disorders
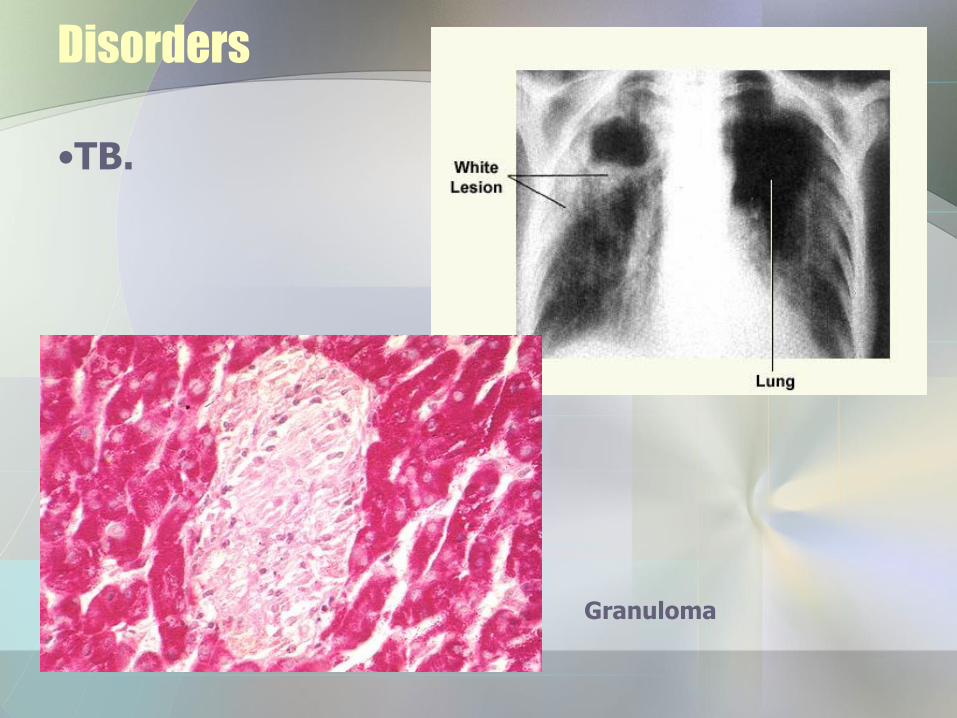
• TB
– Mycobacterium tuberculosis.
– Walling off in enclosed nodules by immune system – tubercle or granuloma.
Disorders
•TB.
Granuloma
Disorders
• Lung Cancer.
– Most common cancer.
– Low survival rate – most die in 1 year.
– Most associated with smoking

Disorders
• Lung Cancer – 3 main types:
•Squamous cell [2-40%] – epithelia of bronchi.
•Adenoma [25-35%] – bronchial glands &alveolar cells.
•Small cell [oat cell] – lymphocyte-like cells in primary bronchi.
•90% originate in large bronchi
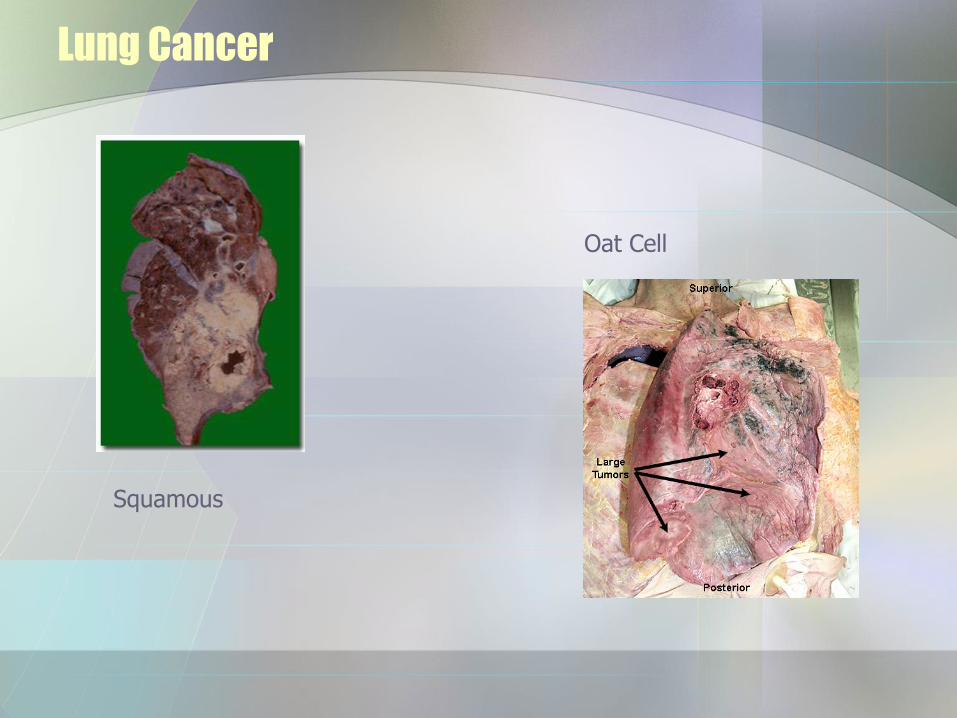
Lung Cancer
Squamous
Oat Cell





























