Embed Size (px)
Citation preview

1
SALIVARY GLAND NEOPLASMS:
Classification, Molecular Insights and Biomarkers
DIANA BELL, M.D.
Associate Professor
Head and Neck Section
SALIVARY GLAND NEOPLASMSSALIVARY GLAND NEOPLASMS
~3300 new cases/year (2.5 per 100,000 U.S.)
5% of all Head & Neck neoplasms
~3300 new cases/year (2.5 per 100,000 U.S.)
5% of all Head & Neck neoplasms
Location:
80% Parotid (20% malignant)
15% Submandibular (50% malignant)
5% minor salivary glands (majority malignant)

2
SALIVARY GLAND NEOPLASMS
Characteristics:
Phenotypic heterogeneity
Variable intra- and intertumoral behavior
Lack of a defined precursor
SALIVARY GLAND NEOPLASMS
Management:
Primary: Surgery ± XRT
Advanced, recurred and metastatic disease: limited options
Efforts are focused on:
understanding of their biology • genetic changes
• chromosomal changes
• epigenetic changes
identifying new targets of potential
therapeutic applications

3
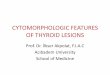
Acinusinter-
calated duct
striated duct excretory
duct Oral cavity
SALIVARY GLAND HISTOGENESIS
Acinic cell Ca Basaloid Tumors Warthin’s MucoepidermoidAdenoid Cystic Ca Oncocytic Salivary Duct Ca
PLGA Tumors AdenocarcinomaMyoepithelial Ca
Epi-myoepithelial CaPleomorphic adenoma
Diagnosis:
FNA
Pathologic examination

4
FNA- indications:
Metastasis
Lymphoma
Infection
Reactive lesions
Planning surgery
FNA- limitations:
Degree of malignancy Basal cell tumors
Ca Ex-PA
Myoepithelial tumors
Oncocytic lesions
Overcalling
FNA- complications:
Infarction
Collapse/ obliteration of cystic lesions and tumors
In doubt:
Core biopsy
Frozen section
Categorical Classification ofSalivary Gland Lesions
Reactive/Developmental Primary Neoplasms Metastasis
Tumor-like Cysts
Benign Malignant

5
Phenotypic Heterogeneity
Acinic cell carcinoma Secretory Carcinoma
(MASC) Adenoid cystic carcinoma Mucoepidermoid carcinoma Polymorphous
adenocarcinoma Epi-myoepithelial
carcinoma Clear cell carcinoma, NOS Hyalinizing clear cell
carcinoma (HCCC) Basal cell adenocarcinoma Sebaceous carcinoma Sebaceous
lymphadenocarcinoma Mucinous adenocarcinoma Cystadenocarcinoma
Oncocytic carcinoma Adenocarcinoma, NOS Myoepithelial carcinoma Carcinoma ex-PA Carcino-sarcoma Squamous carcinoma Small cell carcinoma Large cell neuroendocrine
carcinoma Lymphoepithelial carcinoma Sialoblastoma Intraductal carcinoma Salivary duct carcinoma Metastasizing pleomorphic
adenoma
WHO 2017
Most common SGCs
MEC(30%)
Adenoca NOS / SDCa(20%)
AdCC(25%)
ACC(15%)
A) Low-grade malignancies
low grade MEC
most acinic cell
most PLGA
epi-myoepithelial carcinoma
basal cell adenocarcinoma
most myoepithelial carcinoma

6
B) High-grade malignancies
Solid, AdCC
High-grade MEC
PD/DD Acinic
Salivary duct carcinoma
Carcinosarcoma
Most Ca Ex-PAs (SDCa-exPA)
Incidence of Local Recurrence in Salivary Gland Carcinoma
Diagnosis Recurrence (%)
Adenoid cystic carcinoma 61
Carcinoma ex-PA 60
Adenocarcinoma, NOS 48
Acinic cell carcinoma 15
Mucoepidermoid carcinoma 5
Incidence of LN Metastasis in Salivary Gland Carcinoma
Histology Metastasis (%)
Mucoepidermoid carcinoma 44
Adenocarcinoma, NOS 36
Carcinoma Ex-PA 21
Acinic cell carcinoma 13
Adenoid cystic carcinoma 5

7
Incidence of Distant Metastasis in Salivary Gland Carcinoma
Histology Metastasis (%)
Adenoid cystic carcinoma 44
Adenocarcinoma, NOS 27
Carcinoma Ex-PA 21
Squamous cell carcinoma 15
Acinic cell carcinoma 14
Mucoepidermoid carcinoma 9
Prognostic Factors in Salivary Gland Carcinoma
Favorable features:
Low-grade histology
Low stage
Parotid location
Unfavorable features:
High-grade histology
High stage
Submandibular location
Cervical LN metastasis
Facial nerve paralysis
Skin involvement
Recurrence
Molecular Testing and Targeted Therapy in Salivary Gland Carcinomas

8
MEC
MUCOEPIDERMOID CARCINOMA
1. Considerable cellular heterogeneity
- epidermoid, intermediate and mucin producing cells
2. Intra- and interobserver variability
- reproducibility of grading schemes
Treatment:
Influenced by conventional clinico-pathologic parameters (age, disease stage, grade).

9
MUCOEPIDERMOID CARCINOMA
3. Uniquely characterized by a specific translocation
t(11; 19) (q12; p13)
Fusion transcript t(11;19)(q21;p13)
mucoepidermoid carcinoma translocated 1
MECT1/ CRTC1 gene at 19p13
AND
mastermind-like gene family MAML2 at 11q21
Fusion transcript t(11;19)(q21;p13) (cont.)
chimeric gene MECT1-MAML2: fuses exon 1 of MECT1 with exons 2–5 of MAML2.
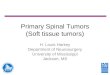
MECT1-MAML2 fusion product disrupts the Notch signaling pathway.
identification of the MECT1 gene product as a potent co-activator for genes that are regulated by cAMP responsive elements (CRE).
MECT1-MAML2 may be disrupting both Notch and CREB signaling pathways to induce tumorigenesis.

10
Copyright ©2006 American Association for Cancer Research
Kaye, F. J. Clin Cancer Res 2006;12:3878-3881
Fusion in MEC
It is generally accepted that more than 50% of this entity manifest the MECT1-MAML2.
Up to 2016
Fusion (+)ve cases showed significantly better survival than
(-)ve cases (?)
MECT1-MAML2 represents a specific prognostic molecular marker in MEC (?)

11
28 patients
90 patients

12
Genomic profiles and MECT1-MAML2 fusion distinguish different subtypes of MEC
fusion (+) MEC significantly lower CNV
fusion (-) MEC multiple genomic imbalances
Fusion in MEC
Represents a distinct mechanism in the development of this entity.
Fusion (+) MEC, regardless of grade, manifest a more stable genome.
Fusion (-) MEC represent a distinctly different pathway characterized by marked genomic instability.

13
Clinical scenarios with potential benefit from CRTC1/MAML2 translocation testing
Diagnostic!
Preoperative
(+)ve CRTC1/MAML2 fusion transcript
Dgn of malignancy on preoperative FNA and bx of a low grade salivary gland neoplasm, in the absence of classic morphology.
Diagnostic
Confirmation of diagnosis of HG MEC and exclusion of MEC mimics (adenosquamous carcinoma, acantholytic SCC, adenoca NOS, SDca).
Confirmation of diagnosis of histologic variants of MEC (e.g., oncocytic), and exclusion of benign MEC mimics (e.g., Warthintumor with mucinous metaplasia).
Confirmation of diagnosis in MEC recurrence or metastasis.
Objective evidence for a separate neoplasm in a patient with multiple synchronous or metachronous tumors withmorphologic overlap (salivary MEC with adenosquamous cell carcinoma of lung).

14
AdCC
AdCC- what is new in biological markers?
Cytogenetics and CGH
MYB Oncogene
Kit and EGFR in AdCC
DNA Methylation in AdCC
Xenograft Models
Cancer Stem-like Cells

15
c-kit 70-90%
EGFR 20-60%
Cell dependent expression:
c-kit (ductal epithelial cells), and
EGFR (myoepithelial cells)
Studies of Chromosome 6q Alterations
Reference Total no. of ADCC
Deletion No. Translocation No.
Sandros et al 11 6q22-q24 5 t(6;14)(q22;q11) 1
Mark et al. 2 - 0 - 0
Highashi et al. 2 - 0 t(6;9)(q21-22;p13-21),t(X;6)(p22;q23)
2
Lopez -Gines et al. 1 6q23 1 - 0
Jin et al. 2 6q21 1 t(6;9)(q21-22;p13-21) 1
Hrynchak et al. 2 - 0 t(6;9)(q23;q22) 1
Martins et al. 3 - 0 t(6;9)(q23-25;p22-24) 1
Nordkvist et al. 10 6q21 1 t(6;9)(q23;p21) 2
El-Naggar et al. 1 - 0 t(6;15)(q25-15) 1
Martins et al. 3 6q23add 9p22
0 t(6;12)(p21;q13) 2
Bell et al. 1 - 0 t(6;14)(q25;q13) 1

16
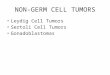
G-Banding
SKY Analysis
MYB Oncogene
chr6 q23
NFIB
p23‐22.3chr9
MYB exon1‐ 8 NFIB exon12
1 2 3 4 5 6 7 8 9
10
11 12 13 14 15 16
MYB
main
break point
12345678
91011
12 main
break point
15 variants
t(6; 9) (q22-23; p23-24) with fusion transcript involving MYB and NFIB

17
Identification of the
MYB-NFIB Fusion and
Therapeutic Applications
RT-PCR, FISH, IHC
Few therapeutic options available
that directly target MYB.
1. Reports of DNA vaccines and antisense
MYB oligonucleotides - potential role in
the treatment of AdCC.
2. Therapies directed against MYB-NFIB
transcriptional downstream targets may
prove more feasible.
3. Various antibodies and inhibitors BCL2,
FGF2, MYC, and COX-2, as potential
chemotherapeutic agents; their efficacy
in AdCC requires further investigation.
18 NOTCH1 mutations identified in 15 patients
Ferrarotto R et al, J Clin Oncol, 2016
IHC for NICD1 to evaluate pathway activation: 40/72 (56%) were +
NOTCH1 mutations in AdCC

18
Adenoid Cystic Carcinoma (AdCC)
Morris LGT et al, JAMA Oncology, 2016
NOTCH1 mutations define a distinct disease phenotype
Stage I-III Stage IVA-C
NOTCH1 mut vs. wt:
86% vs. 46% stage IV (P=0.02)
79% vs. 38% solid (P<0.001)
Ferrarotto R et al, J Clin Oncol, 2016
Tubular Cribriform Solid
(HYALINIZING) CLEAR CELL CARCINOMA(HCCC)

19
t(12;22)(q21;q26) EWSR1-ATF180-90 %
SECRETORY CARCINOMA OF SALIVARY GLANDS
(MASC)
t(12;15(p13;q25)ETV6-NTRK3
Secretory Carcinoma of Salivary Gland
Morphology and genetics similar to secretory carcinoma of
the breast
43-93% harbors the fusion of the transcriptional regulator
(ETV6) with membrane receptor kinase (NTRK3)
ETV6-NTRK3 encodes a chimeric TK with potent transforming
activity in fibroblasts
PKC Ras/MAPK PI3K
Differentiation & Survival

20
LOXO-101 (Larotectinib), a TRKA/B/C inhibitor, in patients with NTRK fusions
Hyman DM et al, ASCO Annual Meeting, 2017
ORR: 76%
LOXO-101 (Larotectinib), a TRKA/B/C inhibitor, in patients with NTRK fusions
Hyman DM et al, ASCO Annual Meeting, 2017
POLYMORPHOUS ADENOCARCINOMA (PLGA)
Site: Minor salivary glands, palate, buccal mucosa
Growth:“eye of the storm”, tubular, trabecular, papillary, solid, cribriform
Nuclear features: vesicular and ovoid nuclei
Clinical: cervical LN mets very rare
Tissue invasion: PNI
Molecular alterations: Hotspot activating PRKD1 somatic point mutation (E710D)

21
CRIBRIFORM ADENOCARCINOMA OF MINOR SALIVARY GLAND (CAT)
Site: Minor salivary glands, BOT predominant
Growth:“glomeruloid”, cribriform, tubular, solid
Nuclear features: optically clear (PTC-like)
Clinical: early cervical LN metsbilateral, no DM
Tissue invasion: LVI
Molecular alterations: PRKD1-3translocations, ARID1 A and DDX3Xpartner genes
Molecular tumor markers investigated in salivary gland carcinomas
Target therapies and clinical trials

22
Chromosome
Chromosome
Chromosome
Factors Complicating Clinical Trials Outcome:
Small size
Combined histologies
Variable prior therapies
Variable inclusion criteria
A need for biologically - based target therapy!
Adenoca/ SDCa

23
Mammary
DC
Salivary
DC
SDCa
HER2AR
Salivary Adenocarcinomas/ SDCa
Share in common:
Growth factors and hormonal expressions with breast / prostate Ca

24
Salivary duct carcinoma SDCa is an aggressive adenoca similar to apocrine breast cancer
M:F ratio 4:1, most patients SIII/IV disease (60% N+)
Androgen receptor is overexpressed in ~ 75%
- splice variants in ~ 40%
- FOXA1, FASN mutations
ERBB2 amplifications occur in 20-30%
Genomic alterations in the PI3K/AKT/mTOR
pathway: 54%
Mitani Y et al, Clin Cancer Res, 2014Dalin MG et al, Clin Cancer Res, 2016
Wang K et al, Clin Cancer Res, 2016
Salivary Duct Carcinoma
Mutation burden: 1.7 mut/ Mb
Dalin MG et al, Clin Cancer Res, 2016
Hormonal Expression in SDCa
Positive Negative(2-3) (0+1)
66%70%
25%
0%
20%
40%
60%
80%
100%
AR ERbeta HER-2
Per
cen
t P
osi
tive
35%
EGFR

25
A B
Similar to mammary and prostatic adenocarcinoma:
Hormonal and growth factors expression targeted for therapy
ERb Anti-estrogens (PD98059)
AR Anti-Androgens
Her2neu Trastuzumab (Herceptin)
EGFR Cetuximab, bevacizumab, gefitinib, erlotinib
Markers Agent
New trial concepts are needed
Locati L et al, Ann Oncol, 2003; Piha-Paul S et al, J Clin Oncol, 2011
LHRH agonist +
Bicalutamide
Docetaxel+
Trastuzumab
Sirolimus+
Bevacizumab
AR+
HER2+
PTEN-

26
Molecular Alterations in Salivary Gland Carcinomas
Tumor Type Chromosomal AlterationGene Fusion/
Rearrangement%
MEC t(11:19)(q21; p13)t(11; 15) (q21; q26)
CRTC1-MAML2CRTC3-MAML2
40-80%5
AdCC t(6;9) (q22-23; p23-24)t(8; 9)
MYB-NFIBMYBL1-NFIB
25-8010-20
HCCC t(12;22)(q21;q26) EWSR1-ATF1 80-90
MASC t(12;15)(p13;q25)t(12;X)
ETV6-NTRK3ETV6-RET
95-982-5
PLGA 14q12 Hotspot activating PRKD1 somatic point mutation (E710D)
20
CAT (CASG) t(1;14)(p36.11;q12)t(X;14)(p11.4;q12)
ARID1A-PRKD1DDX3X-PRKD1PRKD2 and PRKD3 rearrangements
241316
SDC 17q21.13q26.32Inv(10)(q11.21q11.22)
HER2 amplificationPIK3 CA mutationNCOA4-RET
20-4020<5
Clinical trials of salivary gland carcinomas based on:
Histologic classification
Molecular and cellular characterization
Biomarker profiling
Needs:
Tissues and cell lines infrastructure
Transgenic animal models
In vitro 3D models
Perspectives