Embed Size (px)
Citation preview

Scabies And Pediculosis

Scabies Scabies is an itchy rash caused by a little
mite that burrows in the skin surface. The human scabies mite's scientific name is Sarcoptes scabiei var. hominis.

Aetiology
Scabies is caused by the acarus, Sarcoptes scabiei, and is a common world-wide public health problem with an estimated global prevalence of 300 million. The infestation causes considerable discomfort and can lead to secondary infection and complications such as post-streptococcal glomerulonephritis. Scabies spreads in households and environments where there is a high frequency of intimate personal contact.

Microscopic appearance of Sarcoptes scabiei, the parasite
which causes scabies.
Sarcoptes scabiei
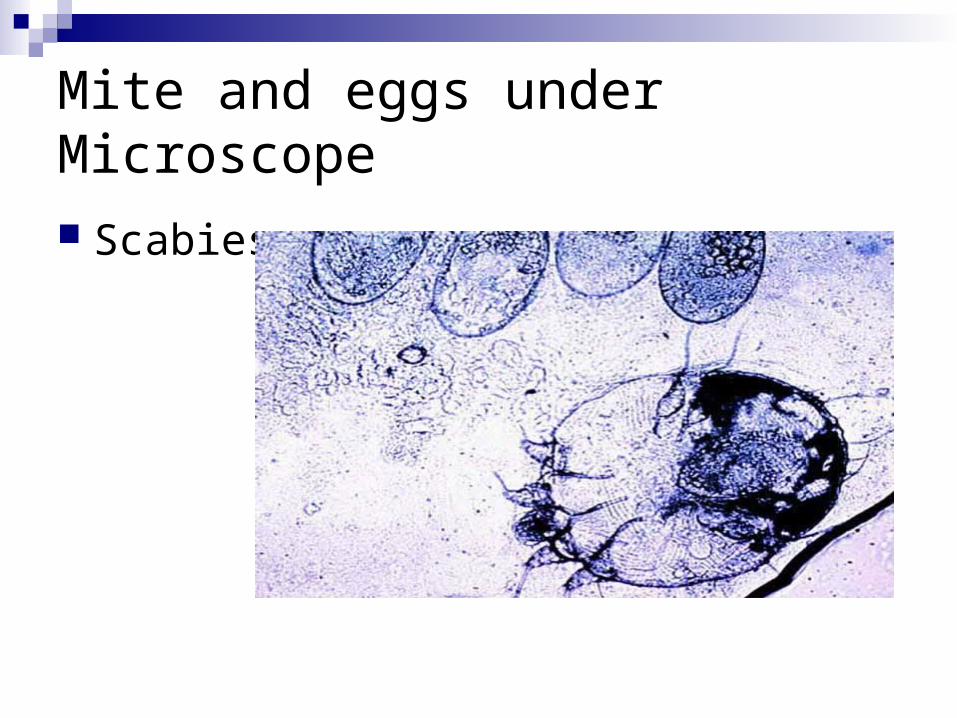
Mite and eggs under Microscope
Scabies

Lesions
Inappropriate application of scabietic treatments can cause considerable irritation in other conditions. In small children the palms and soles can be involved with pustule formation . Involvement of the genital area in boys is pathognomonic. The main symptom is itch . The clinical features include secondary eczematisation elsewhere on the body; the face and scalp are never involved except in the case of infants. Even after successful treatment the itch can continue, and occasionally nodular lesions persist.

Symptoms and Signs Itch
The itching appears a few days after infestation. It may occur within a few hours if the mite is caught a second time. The itch is characteristically more severe at night and affects the trunk and limbs. It does not usually affect the scalp.
Burrows Scabies burrows appear as tiny grey irregular tracks between the fingers and on the wrists. They may also be found in armpits, buttocks, on the penis, insteps and backs of the heels. Microscopic examination of the contents of a burrow may reveal mites, eggs or mite faeces (scybala).
Generalised rash Scabies rash appears as tiny red intensely itchy bumps on the limbs and trunk. It can easily be confused with dermatitis or hives (and may be accompanied by these). The rash of scabies is due to an allergy to the mites and their products and may take several weeks to develop after initial infestation.
Nodules Itchy lumps or nodules in the armpits and groins or along the shaft of the penis are very suggestive of scabies. Nodules may persist for several weeks or longer after successful eradication of living mite.
Acropustulosis Blisters and pustules on the palms and soles are characteristic of scabies in infants.
Secondary infection Impetigo commonly complicates scabies and results in crusting patches and scratched pustules. Cellulitis may also occur, resulting in localised painful swelling and redness, associated with fever.
Scabies only rarely affects the face and scalp. This may be the case in young babies and bedbound elderly patients.

Pruritus :Causes
Pruritus

Scabies with extensive infestation of Sarcoptes scabiei. scabies

Baby with Scabies Rash

Pustular Eruptions Scabies

Scabies in Childhood
Scabies. Pustules at a common site in a child. Burrows were present but cannot be
seen at this distance.

Affected webspace
Scabies

Scabies

Diagnosis
Diagnosis is made by identifying the scabietic burrow, usually found on the edges of the fingers, toes or sides of the hands and feet. Extraction of the mite using a blunt needle can be difficult but is helpful in ensuring the correct diagnosis, appropriate treatment and compliance. Inappropriate application of scabietic treatments can cause considerable irritation in other conditions. In small children the palms and soles can be involved with pustule formation . Involvement of the genital area in boys is pathognomonic. The main symptom is itch.
The clinical features include secondary eczematisation elsewhere on the body; the face and scalp are never involved except in the case of infants. Even after successful treatment the itch can continue, and occasionally nodular lesions persist.

Burrows
Burrows [Arrows point to mites]

Treatment
Topical treatment of scabies is usual and involves the affected individual and all asymptomatic family members/physical contacts to ensure eradication. Two applications one week apart of an aqueous solution of either permethrin or malathion to the whole body, excluding the head, is usually successful. In some clinical situations such as poor compliance, immunocompromised individuals and heavy infestations (Norwegian scabies), systemic treatment with ivermectin (200 µg/kg) as a single dose would be appropriate.
25% Benzyl benzoate lotion, applied daily for 3 days 5% Permethrin cream, left on for 8-10 hours 0.5% Aqueous malathion lotion, left on for 24 hours

Successful Treatment
To reduce the risk of the treatment failing: Ensure the scabicide is applied to the whole body from
the chin down. Leave it on for the recommended time and reapply it
after washing. Apply the scabicide under fingernails using a soft brush. Obtain antibiotics from your doctor if there is crusting
and secondary infection. Ensure all close contacts are treated whether or not they
are itchy.

Pediculosis Lice Lice are insects that live on human hair and clothing. They are small but can still be seen with the
naked eye. Often they are well camouflaged and reflect the colour of the surroundings, which makes them difficult to see.
The medical term for an infection or infestation with lice is called pediculosis. There are three types of lice that infest humans. Pediculus humanus var. capitis - The head louse Pediculus humanus var. humanus - The body louse. Phthirus pubis - The pubic louse. Lice are insects than live on rather than in the body. They are wingless and have six legs on
which are attached strong claws, which they use to grasp on tightly to hair shafts or clothing fibres.
Head lice, the most common infestation in humans, are colloquially known as cooties and their eggs are called nits. Pubic lice are smaller than the other two species, and have a short body resembling a crab. Hence the name crabs.
Head lice [pediculus humanus capitis] Body lice [pediculus humanus[corporis] Pubic lice [phthirus pubis]
Head Lice
Head lice Head lice have infested humans for thousands
of years. Infestation with lice is quite often inappropriately considered related to poor hygiene and low socio-economic status. In fact people of all walks of life can get infested with lice and the stigma of catching lice is often borne out of ignorance.

Body lice
Infestation with body lice (Pediculus humanus) is uncommon. They tend to infest people in extreme states of poverty or personal neglect. Particularly when clothing is not changed or regular washing is not undertaken.
The eggs of body lice are laid and glued to cloth fibres instead of hair, and the lice feed off the skin. Regular hot washing of clothes and bathing has lead to a decrease in incidence of body lice but during wartime and in some undeveloped countries the condition can still occur.
Body lice in the past have been responsible for spreading diseases such as typhus. However because of the decline in numbers of people infested with body lice this is no longer a significant problem.
Similar insecticides used in the treatment of head lice are used in the treatment of body lice. Hot washing of clothes and bathing should be emphasised.

Pubic Lice
Pubic Lice Pubic lice or crabs are contracted by close contact and are easily
transmitted sexually. The pubic hair is most common site but lice can spread to other
hairy parts of the body including armpit, beard, chest hair and thigh hair. Eyelashes can also be affected.
Pubic louse
Pubic lice infestation results in itching. Blood specks on underclothes and live lice moving in the pubic hair are occasionally noted.

Pediculus humanus capitis
[Head louse]

Phthirus Pubis
Pubic louse

Pruritic infestation on the Scalp
Dermatitis

Pediculosis
Mortality/Morbidity: Morbidity results from the severe itching that is caused by lice infestation. Mortality may occur from infectious diseases transmitted by the body louse.
Race: Blacks have a lower incidence of infestation by the head louse but may experience scalp infestation by P pubis.
Sex: Males and females are equally at risk for infestation. Age: Lice affect all age groups. Body lice are indiscriminate in
regard to the age of their host. Head lice are common in young school children but much less common after puberty. Pubic lice infest body and pubic hair. Prepubescent scalp infestation by P pubis may occur in individuals with short, thick, curly scalp hair.

Clinical
History: Patients may come to the attention of a health care provider after
discovering lice or nits. Parents and teachers typically make the initial diagnosis of head louse infestation. In the case of head lice, a school nurse usually discovers infestation, or a generic letter is sent home to parents indicating that they should inspect their children for lice.
Pruritus is the most common symptom of infestation. Children often have trouble sleeping because of intense pruritus at night when lice are feeding.
Children with infestation may be asymptomatic. Routine nit inspections by school nurses are standard in many parts of the United States.

Clinical Physical: Manifestations of head louse infestation include scalp pruritus, occipital
lymphadenopathy, and impetigo. Examination of the scalp reveals excoriations, dark specks of louse dung, nits, and adult lice. The heaviest infestation typically is in the retroauricular scalp. Pruritus commonly leads to excoriation, secondary bacterial infection, and regional lymph node enlargement. A generalized exanthem rarely accompanies louse infestation (pityriasis rosealike pediculid).
Pediculosis capitis: Although head lice may be found on any part of the scalp, they most commonly are found in the retroauricular scalp. Eggs depend on body warmth to incubate, so nits are attached to the hair shafts just above the level of the scalp. Human scalp hair grows at a rate of approximately 0.37 mm/d. Nits found several millimeters from the scalp are nonviable empty egg cases. They indicate chronic infestation.
Pediculosis corporis: Body lice infest the seams of clothing and take blood meals at night. Nits are found in the seams, not on human hairs. Maculae ceruleae, the hemosiderin-stained purpuric spots where lice have fed, suggest the diagnosis of body louse infestation.
Pediculosis pubis: Pubic lice and nits generally are plainly visible throughout the pubic hair, extending onto adjacent hairy areas of the body. Eyelash nits are a manifestation of pubic louse infestation, not head louse infestation.

Lab studies Lab Studies:
The identification of adult lice or nits is diagnostic. The presence of bruiselike bites or dark specks of louse dung suggest the diagnosis of louse infestation.
Lice move rapidly. A helpful technique is to fasten a piece of transparent adhesive tape to the infested areas. Lice stick to the tape. The tape then becomes a convenient coverslip for a microscopic slide.
Mature lice are approximately the size of a sesame seed (3-4 mm) with an elongated body, 3 pairs of legs, and narrow anterior mouthparts. Wide crablike bodies and claws distinguish pubic lice. Nits are approximately 1 mm in length, transparent, and flasklike in appearance.
Nits and lice fluoresce with a Wood light. Properly evaluating persons who have been raped is essential. Evidence should be collected in
such a way as to avoid contamination and to ensure a legal chain of custody. Human DNA can now be identified in the amount of blood present in a pubic louse. Lice recovered after an attack have the potential to provide evidence valuable in securing a convictionOther Tests:
Evaluate individuals with pubic lice for other STDs. Evaluations may include serologic testing for syphilis and AIDS, culture for gonorrhea, and antigen testing for chlamydia.
Histologic Findings: Louse bites demonstrate intradermal hemorrhage and a polymorphous wedge-shaped infiltrate rich in eosinophils

Medical Care
Medical Care: Reinfestation occurs unless louse infestation is addressed as a community-wide problem. Management must include examination of all individuals exposed and treatment of all those who are infested. Education has been shown to reduce the number of lice infestations in schools. “No nit” policies exclude many children from the classroom, but they have not been shown to reduce the number of lice infestations.
Fomite control is essential. Hats lined up on pegs or placed in adjacent cubbyholes provide an avenue for spread of the infestation. Cubbyholes can be sprayed with a permethrin spray or other insecticide, but the most effective method is for each child to "ground his or her clothing" (ie, hat, coat, scarves) under each individual chair or desk. Common cloakrooms may suggest an antiquated charm, but they should be viewed as merely antiquated and a site for spread of the infestation.
Combs, brushes, and headbands should not be shared. Shaving of hair is effective but not socially acceptable in most societies. Young nits do not have a nervous system and are immune to neurotoxic pediculicides.

Treatment
Treatment options include Malathion, permethrin cream, and pyrethrins. Less toxic agents are being developed that aim to occlude the respiratory spiracles of the louse and kill via asphPermethrin (Nix, Elimite) -- DOC recommended by most authorities. Resistance probably has developed in many areas. Physicians in some countries select different pediculicides on a rotating basis to discourage development of resistance. Very effective in killing adult lice and nymphs but not as effective in killing nits (eggs). OTC 1% concentration may be insufficient for treatment of pubic lice and for some cases of head lice. The 5% prescription preparation marketed for scabies (Elimite) may be more effective in some cases. One benefit of permethrin is a residual effect in the hair for several hair wash cycles. yxiation.
Pitfalls
Medical/Legal Pitfalls:
Follow manufacturer's instructions for lindane treatment. It may not be suitable for use in patients with a defective cutaneous barrier. Seizure may result from abnormal absorption or gross overuse of the product. Many authors recommend that it not be used as a first-line therapy.
Pyrethrin products are contraindicated for patients with contact allergy to ragweed or turpentine.
Failure to recognize that pubic lice in children may be an indication of sexual abuse is a potential medical/legal pitfall. Children with eyelash nits have been exposed to an adult with pubic lice. This is
not proof of abuse, merely an indication that the child has had contact with an adult with pubic lice.
Pubic lice commonly infest the adult's body hair, as well as pubic hair. Although lice can be transferred easily in the absence of abuse, examine patient
for other signs of abuse

Points To remember Important points on treatment for pubic lice It is important to apply the shampoo to all hairy parts of the body apart from the eyelids and scalp
- from 'neck to knees'. It is easily applied while in the shower. Work thoroughly into lather and leave on for five minutes. Rinse off thoroughly and dry with a towel. Any remaining nits (small white spots attached to hair shaft) should be removed by using a fine
toothed comb. A repeat application is advisable 7 days later. Shampoo should not be applied near the eyes. Lice and nits can be removed by using a pair of
fine forceps. Alternatively petroleum jelly, such as Vaseline can be smeared on the eyelashes twice a day for at least 3 weeks.
Wash underwear and bed linen thoroughly in hot water to prevent recurrences. Sexual partners need to be treated even if they deny itching and do not appear to be infected. You may be at risk of other more serious sexually transmitted infections. It is advisable to attend
your doctor or sexual health clinic for a check-up.
THANKS
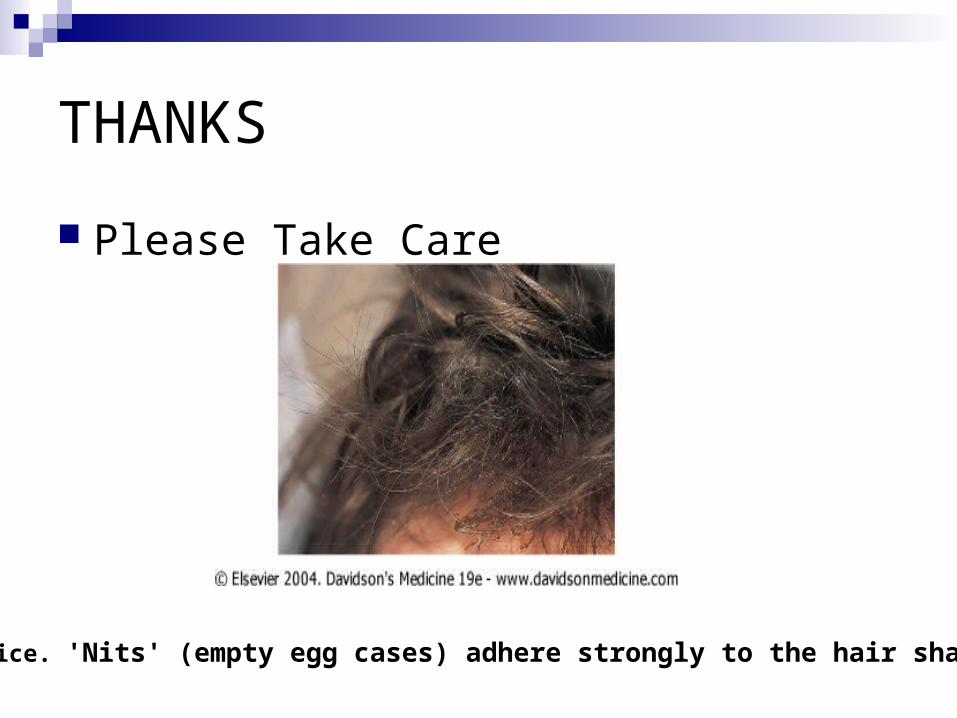
Please Take Care
Head lice. 'Nits' (empty egg cases) adhere strongly to the hair shafts.