PowerPoint Presentation
Scientific Overview of Angelman Syndrome and Its Social
Implications Chelsea A Coburn, Melissa D Connell, Maureen P Kane,
Jeff Min, and Xueying WangUniversity of Florida, Gainesville, FL
32611
Abstract
Angelman Syndrome (AS) is a neuro-genetic disorder that occurs
in 1 in 15,000 live births 10. Since the initial diagnose by Dr.
Harry Angelman in 1965, scientific advancements enable in depth
analysis of the disorder at the molecular level. The cause of AS
includes uniparental disomy, imprinting defect, and deletion or
mutation of the maternal UBE3A gene on chromosome 15 5. Clinical
and genetic tests are possible using the distinctive behavior
markers displayed by AS patients collectively with sophisticated
technology. There are no known cures for AS, and patients generally
require life-long care; however many symptoms can be controlled by
medication 10. Further scientific breakthroughs and increased
social awareness is crucial in resolving controversial subjects of
AS such as prenatal testing 8. Mendelian
PHENOTYPE/CLINICAL CHARACTERISTICS 1,2Significant developmental
delay with cognitive impairmentOveractive, exuberant, sociable, and
happy demeanorSleep abnormalities, and frequent laughter to minimal
stimulusPresence of hypotonia in body trunk, and hypertonia in
extremitiesSeizures in about 90% of patients, onset in first one to
three yearsLarge wide mouth/teeth, prominent pointy chin with flat
midfaceLife span up to 70 years and behavioral problems improve
with ageAbnormalities in muscle tone lead to stiff and ataxic
METHOD OF INHERITANCEGene of interest: UBE3A gene on chromosome
15Errors, failure to express, or the lack of maternal chromosome
result in ASRecurrence in families: Male with silent mutant
chromosome may pass it to his daughter, whose progeny have 50%
chance of AS
MECHANISM4
90% of AS patients have little or no UBE3A gene expression due
to a deletion of the 15q11 to the 15q13 region on the maternal
chromosome 15. The gene UBE3A codes for an E3-ubiquitin protein
ligase. The function of UBE3A is to tag proteins that need to be
proteolysed by proteasomes. Ubiquitin proteolysis may be involved
with synaptogenesis and long-term memory, thus deletion of the
UBE3A gene may be detrimental to the brains maturation process. The
rest 10-15 % of AS patients, suffer from a mutant UBE3A gene. The
mutations include:Insufficient amount of DNA methylation to induce
expression of UBE3AInheritance of both chromosome 15s from the
father(Uniparental disomy). Uniparental disomy results from
inheritance of both chromosomes from one parent, instead of one
from each. It is possible that chromosome of both parents were
present until the maternal chromosome was pushed out when cell
division occurred; a cell is not feasible if there are three
chromosome 15s present.Mutation of maternal chromosomes.
Responsible for families with more than one AS patients. Japanese
researchers believe there may be a link to mutants in the maternal
chromosomes which turns off the gene expression
Deletions of the 15q11 to 15q13 section of the chromosome 15 and
a mutant chromosome which has a low amount of methylation have been
known to cause the most brutal symptoms such as: poor communication
abilities, more seizures, and microcephaly.
Mechanism Summary7
Molecular
CLINICAL TESTING 5, 11:
GENETIC TESTING 8:
Step 1: Methylation Test: test for methylation pattern present
in AS. Diagnosis is confirmed by positive results on 3 types of
genetic causes.Step 2: FISH test: Test for deletion by chromosomal
study to find small changesStep 3: RFLP analysis : Testing the
lineage of chromosome 15. If only from one parent, then cause of AS
is confirmed to be uniparental disomy. If from two parents, then
the cause is imprinting.Step 4: Imprinting center mutation: precise
changes on chromosome 15. Step 5: UNFE3A Screening: If methylation
test is normal and AS is still suspected, the UNFE3A gene is
screened for small changes. Changes are detected in 20% of AS
patients and 80% of familial AS patients.Step 6: Consider other
possibilities : If none of the above is positive, AS is unlikely,
thought not impossible. Plan for new tests with neurologist Ethical
Legal Social Issues (ELSI):
Is there a cure for AS? NO, but medication can control symptoms
of seizures, behavioral/sleep issues
Is there an increased risk of AS when using assisted
reproductive technology? YES, some reports show increased chance of
imprinting disorders in children conceived using assisted
reproductive technology (ART). It is believed that maternal allele
is more likely to be effected than paternal because of altered
methylation of the female gamete. However, there is not enough of a
risk or evidence to cease use of this technology2
Can people with AS develop to be healthy reproducing adults?
YES, mutation of chromosome 15 does not affect the reproduction
system
Is it possible for an AS person to have children with AS? YES,
there is one reported case of a women with AS having a daughter
with AS 9
What would happen if a woman with AS has a child? This is
decision that needed to be made on a patient to patient basis Women
with AS may not handle the physical/hormonal changes of pregnancy
10-Person with AS may not be fit for parenthood due to the need of
assistance -Adoption is an option that could be considered if a
child is conceived
Can prenatal testing be done to accurately determine if child
will develop AS?YES, identification of the mutation or maternal
methylation pattern in a fetus is possible. It can be used with
successive pregnancies after having a child with AS. However, the
ethical issue lies with the decision of what to do when parents are
told they will have a child with AS. If parents consider
termination options, then they have to deal with legal and moral
issues of abortion. 3 ReferenceButler MG. Genomic imprinting
disorders in humans: a mini-review. J Assist Reprod Genet 21 Oct.
2009.Carter MO, James HS Jr. Imprinting Disorders and Assisted
Reproductive Technology. Seminars in Reproductive Medicine 27.5
(2009): 418-428.Cassidy S, Schwartz S. Prader-Willi and Angelman
Syndromes: Disorders of Genomic Imprinting Medicine 77.2 (1998):
140-151.Dan B. Angelman Syndrome: Current Understanding and
Research Prospects. Epilepsia 50.11 (2009): 23312339. Dittrich B,
Robinson WP, Knoblauch H, et al. Molecular diagnosis of the
Prader-Willi and Angelman syndromes by detection of
parent-of-origin specific DNA methylation in 15q11-13. Human
Genetics 90.3 (1992): 313-315.Genetic Diagnostic Testing. Angelman
Syndrome Foundation. 29 Nov. 2009. <
http://www.angelman.org/stay-informed/facts-about-angelman-syndrome---7th-edition/genetics-of-as/genetic-diagnostic-testing/>Genetic
Mechanisms that Cause AS. Angelman Syndrome Foundation. 29 Nov.
2009. James H, Clayton-Smith J. Genetic Testing For Angelman
Syndrome. Angelman Syndrome. InternAnalysis. 29 Nov. 2009. <
http://www.armyofangels.org/angeltest.htm>Lossie AC, Driscoll
DJ. Transmission of Angelman syndrome by an affected mother. Genet
Med 1.6 (1999): 262-6.Stay Informed. Angelman Syndrome Foundation.
29 Nov. 2009. <
http://www.angelman.org/stay-informed/>Williams CA, Beaudet AL,
Clayton-Smith J, et al. Angelman syndrome 2005: updated consensus
for diagnostic criteria. Am J Med Genet A 140.5 (2006):
413-8.Williams C A. Neurological aspects of the Angelman syndrome.
Brain and Development, 27.2 (2005): 88-94.
DiscussionSyndrome is gaining world wide attention through
representation from parents of the patients. The increasing
awareness and the establishment of support groups for care takers
widens the social circle for individuals with AS. However, many
individuals are falsely diagnosed with cerebral palsy or autism3.
Future studies will allow scientists and doctors to gain a deeper
understanding of the molecular mechanisms of the disease, and
consequently decrease the number of misdiagnosis. It is expected
that further research in the field of gene therapy will lead to a
possible cure for AS in the future4.
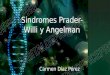
Figure 1. Four mechanisms which lead to AS. 7100%Frequent
laughter/smile; happy demeanor; excitable personality, Uplifted
hand-flapping/waving movements; hyper motor behaviorDelayed
developmentMovement/balance disorder, with tremors in limbsLacking
in verbal skills with stronger receptive
communication80%Disproportionate growth in head
circumferenceSeizuresAbnormal EEG patterns 1020-80%Frequent
drooling; protruding tongueAttraction to/fascination with
waterIncreased sensitivity to heatAbnormal sleep wake cycles and
diminished need for sleep
Figure 2. Six steps of testing in diagnosing AS 6Deletion of
maternal UBE3A (68%)Mutation of maternal UBE3A(13%)Uniparental
disomy (3%)Imprinting defect (6%)1