Embed Size (px)
Citation preview

Screening for Lung Cancer using Low Dose CT: State of the Art and
Controversies
Philippe GRENIER
University Pierre et Marie Curie (UPMC),Pitié-Salpêtrière Hospital, Paris, FRANCE

Rationale for lung cancer screening
Lung cancer remains the leading cause of cancer-related death among men and women in the world
The 5-year survival rate of 10-15% has been roughly unchanged for the past two decades despite treatment advances
Strauss. Surg Oncol Clin N Am 1999; 8: 747
At diagnosis, most lung cancers are already at advanced stage
Mountain. Chest; 1997.111: 1710

Rationale for lung cancer screening
Early stage lung cancer patients have a much higher 5-year survival rate (between 60 and 80%)
Pisters. J Clin Oncol 2005; 23:3270
Changing smoking habits could reduce lung cancer incidence and deaths
The risk for lung cancer does not decrease for many years after smoking cessation
Cessation programs have long-term cessation rates of only 20% to 35% at one year

Lung Cancer Screening with Chest Radiography with or without
Sputum Cytologic Examination
Some lower-quality evidence (case-control studies) has shown benefit
Higher-quality evidence (randomized controled trials) conducted in the 80’s has not (the screened groups had the same number of death from lung cancer as the control group)
Humphrey. Ann Intern Med 2004; 140:740

Early Lung Cancer Action Project (ELCAP)
1000 asymptomatic volunteers (> 60 yo)
smoking : 45 py (median).
Subjects received both low dose computer tomography (LDCT) and chest radiography (CR)
Non-calcified nodules were detected on 23% of LDCT and 7% of CR
Lung cancer was detected in 2.7% LDCT screens (85% were stage I disease) and in 0.7% CR screens
Henschke. Lancet 1999; 354:99
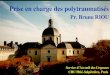
Uncontrolled observational trial

Year 0
Year 1
Year 1+3 months Adenocarcinoma

Year 1+3 months
Year 0
Year1
Adenocarcinoma

Initial 3-month Follow-up
+ 30%
Adenocarcinoma

Uncontrolled studies with LDCT
Study yearsScreening
typeScreening tests
performedPostive testresults (%)
Lung cancer(%)
Stage I disease (%)
Henschke 1999BaselineIncidence
10001184
243.10.9
8567
Nawa 2002BaselineIncidence
79565568
260.50.1
86100
Sone 2001BaselineIncidence
54838303
50.40.6
10086
Sobue 2002BaselineIncidence
16117891
120.80.2
7779
Swensen 2003BaselineIncidence
15202916
511.80.7
66
Diederich 2002 Baseline 817 43 1.3 58
Pastorino 2003 BaselineIncidence
1035994
151.11.1
77

Uncontrolled studies with LDCT
Prevalence rates of lung cancer have varied widely (0.44-1.8%) , due to different risk profiles based on age and smoking disease status,
Stage I or II cancers have been 75% to 100%
High level of non-calcified benign nodules detected (15-51%) with the risks of invasive procedures and futile thoracotomies

False positive rate of screening CT
Definition : number of patients who required further evaluation after CT but did not have cancer
Rate of positive tests in prevalence screening : 15-51 %
Rate of positive tests in incidence screening : 3-12 %
Most are resolved with follow-up CT
5 % - 14 % of those undergoing follow CT were referred to biopsy and most (63 % - 90 %) then received a diagnosis of cancer

False negative rate of screening CT
Nodules were missed in 26 % of patients on annual incidence screening CT scans1
CT sensitivity for detecting nodules is reduced when central versus peripheral, when adjacent to the vessels and when small2
Double reading and CAD may reduce false negative rates3
1 Swensen. Am J respir Crit Care Med 2002; 165: 5082 Rusinek. Radiology 1998; 209:2433 Ko. J Thorac Imaging 2004; 19:136

Computer Aided Diagnosis: Detection and Nodule growth assessment on follow-up CT

Strategy for indeterminate nodule(more than 50 y.o. smoker)
Size
Alternative: FDG-PETor contrast enhanced CT
4 - 8 mm
CT Follow-up*3-6, 6-9, 9-12, 12-24
months
< 4 mm
CT Follow-up*12 months
> 8 mm
Biopsyor resection
+
Biopsy or resection
-
McMahon. Radiology. 2005 ; 237: 395-400

Survival of patients with stage I lung cancer detected on CT screening
31,567 asymptomatic persons at risk for lung cancer were screened using LDCT (1993-2005)
412/484 (85%) had clinical stage I lung cancer and estimated 10-year survival rate was 88%
Among 302/412 who underwent surgical resection within 1 month after diagnosis, the 10-year survival rate was 92%
The 8 participants with clinical stage I who did not receive treatment died within 5 years after diagnosis
Henschke. N Engl J Med. 2006; 355:1763

Are Increasing 5-Year Survival Rates Evidence of Success Against Cancer?
Welch. JAMA; 2000; 283:2975
There is little correlation between the change in 5-year survival for a specific tumor and the change in tumor-related mortality
The change in 5-year survival is positively correlated with the change in the tumor incidence rate

Uncontrolled studies with LDCT
Lung cancer can be diagnosed at a significantly earlier stage with CT screening.
However whether this will translate to a mortality benefit is unclear

CT Screening for Lung Cancer:Five-year Prospective Experience
1520 individuals with high risk for lung cancer
68 lung cancers diagnosed (31 initial, 34 subsequent,3 interval) 28 subsequent cases of non-small cell cancers were detected, of which 17 (61%) were stage I tumors
No difference in the observed incidence lung cancer mortality rate to a historic benchmark
2.8 vs 2.0 per 1000 person-years
Swensen. Radiology: 2005; 235: 259

CT Screening and Lung Cancer Outcomes
Bach. JAMA: 2007; 297: 953
Longitudinal analysis of 3246 individuals current or former smokers screened for lung cancer in academic centers with a follow-up of 3.9 years
Comparison of predicted with observed number of new lung cancer cases, lung cancer resections, advanced lung cancer cases, and deaths from lung cancer

CT Screening and Lung Cancer Outcomes
144 individuals diagnosed with lung cancer compared with 44.5 expected cases (RR, 3.2; P<.001)
109 had a lung resection compared with 10.9 expected cases (RR, 10; P<.001)
No evidence of decline in the number of diagnoses of advanced lung cancers (42 vs 33.4 expected cases) or deaths from lung cancer (38 observed and 38.8 expected; RR, 1; P= .9)
Bach. JAMA: 2007; 297: 953

Good :extend quality years of life (QALY)reduce mortality from the tumor
Harm :complications of the screening testsconsequences of false positive diagnoses
Cancer screening programmes :should do more good than harm
at a financial cost acceptable to society

Survival timeSurvival time
Survival timeSurvival time
Lead-Time BiasLead-Time Bias
TimeTime
TimeTime
Screened groupScreened group
Control group Symptoms DiagnosisControl group Symptoms Diagnosis PatientPatient
confirmed diesconfirmed dies
DiagnosisDiagnosisconfirmedconfirmed
Lead timeLead time
PatientPatient diesdies

TimeTime
Length-Time BiasLength-Time Bias
SymptomsSymptoms
SymptomsSymptoms
SymptomsSymptomsTumorTumor
detectabledetectable
TumorTumordetectabledetectable
TumorTumordetectabledetectable
Onset of Onset of tumortumor
Onset of Onset of tumortumor
Onset of Onset of tumortumorAggressive tumorsAggressive tumors
Indolent tumorsIndolent tumors

Overdiagnosis and consequent overtreatment
Overdiagnosis bias is the result of slow-growing relatively indolent lung cancers that a patient dies with and not from
The high rate of adenocarcinomas raises the possibility of overdiagnosis
Slow-growing adenocarcinomas (bronchioloalveolar carcinomas or non-invasive adenocarcinomas) that are not lethal may be identified with CT screening
Lindell. Radiology: 2007; 242: 555

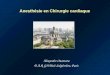
Non solid nodules: malignant causes
Adenocarcinoma
Bronchioloalveolar cell carcinoma
Ground glass opacity

Mixed (part-solid) nodules
Adenocarcinomas

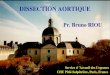
Solid and non-solid nodules: growth rate
Doubling time of nodules from a 3-year screening program for lung cancer*
*Hasegawa. Br J Radiol 2000; 73: 1252
Solid nodules: 189 daysMixed (part-solid) nodules: 457 daysNon solid nodules: 813 days

Curative limited resection for small peripheral lung cancer
146 stage IA peripheral tumors
Type IGGO
90-100 %
Type IIGGO
50-89 %
Type IIIGGO
10-49 %
Type IVGGO
< 10 %
Nodal metastasis 0 0 20 % 24 %
3-year disease-free survival
98 % 98 % 86 % 78 %
Patients with tumor that have GGO ratio > 50 % are regarded to be possible candidates for limited pulmonary resection
Nakata. J Thorac Cardiovasc Surg 2005; 129: 1226

Overdiagnosis: a Substantial Concern in Lung Cancer Screening
Lindell. Radiology: 2007; 242: 555
61 cancers reviewed and 48 assessed for morphologic change
Mean tumor size: 16.4 mm (5.5-52.5 mm)
74% prevalence, 37% incidence detected lung cancers were adenocarcinomas
Mean volume doubling time (VDT) was 518 days
13/48 (27%) cancers had a VDT longer than 400 days (11/13 were in women)

Randomized controlled trials eliminate lead-time and lenght biases
RDZ
Test1e yr
Test2e yr
Test3e yr
Test4e yr
Screened group
Control group

Randomized controlled trials
They are very difficult to set up
Contamination is a major problem
They take a very long time to produce definitive results (enough time to allow for lead time and length biases)
In the interval technology changes and the results may not be relevant when trial finally reports

Lung Cancer Study: a randomized controlled trial (LDCT vs CR)
3,318 tobacco-exposed subjects
Compliance at baseline was 96% in the LDCT arm and 93% in the CR arm
At year one screening compliance was 86% in the LDCT arm and 80% in the CR arm
Gohagan. Chest 2004; 126: 114

NLST: RCT Design
time
0 1 2 3 4 5 6 7 8
53,476High-Risk
Subjects
CT Arm
CXR Arm
Randomize
F/U
T0
T1
T2

The NELSON Trial
15,428 subjects
LDCT screened arm is beeing compared to a control arm without screening
Van Iersel. Int J Cancer 2007; 120:868

Conclusion
Screening for lung cancer with LDCT may increase the rate of lung cancer diagnosis and treatment, but may not meaningfully reduce the risk of advanced lung cancer or death from lung cancer
Until more conclusive data are available, asymptomatic individuals should not be screened outside of clinical research studies

Conclusion
Randomized controlled trials are the only way to reliably determine whether screening does more good than harm
Although expensive and time-consuming, rigorous trials of cancer screening are far more cost-effective than widespread adoption of costly screening interventions that cause more harm than good
Welch. Arch Intern Med; 2007; 167: 2289

Genetic abnormalities and biomarkers of premalignancy or early malignancy
Detection of biomarkers will have profound implications for more precise selection and stratification of population at risk for lung cancer
Field. J Thorac Oncol. 2006; 1:497
Genomic and proteomic methods may offer a much easier mass screening as the first step of a screening strategy
Meyerson. J Clin Oncol. 2005; 23:3219Zhong. Am J Respir Crit Care Med. 2005; 172:1308