Embed Size (px)
Citation preview

Pharmacol. Ther. Vol. 79, No. 1, pp. 1–53, 1998Copyright © 1998 Elsevier Science Inc.
ISSN 0163-7258/98 $19.00PII S0163-7258(98)00008-4
Associate Editor: P. Winstanley
Severe Falciparum Malaria in Children: Current Understandingof Pathophysiology and Supportive Treatment
Charles R. J. C. Newton*
‡
and Sanjeev Krishna
†‡
*NEUROSCIENCE’S UNIT, INSTITUTE OF CHILD HEALTH, WOLFSON CENTRE, MECKLENBURGH SQUARE, LONDON WC1N 2AP, UK
†
DIVISION OF INFECTIOUS DISEASES, DEPARTMENT OF CELL AND MOLECULAR SCIENCES,ST. GEORGE’S HOSPITAL MEDICAL SCHOOL, CRANMER TERRACE, LONDON SW17 0RE, UK
ABSTRACT. Severe falciparum malaria is one of the most lethal parasitic infections in the world and isresponsible for more than one million deaths in African children per year. Changes to management over thelast 40 years have not improved survival. A reduction in the mortality and morbidity may only come about bya better understanding of the pathophysiological processes that are responsible for severe disease and thatdetermine the outcome before antimalarials have had time to work. This review discusses potential adjunctivetherapies for severe malaria that are under development following such detailed clinical and pathophysiological
studies.
pharmacol. ther.
79(1):1–53, 1998.
© 1998 Elsevier Science Inc.
KEY WORDS.
Falciparum malaria, pathophysiology, children, adjunct therapy.
CONTENTS1. I
NTRODUCTION
. . . . . . . . . . . . . . . 22. D
EVELOPMENT
OF
I
NFECTION
. . . . . . . . 32.1. M
ULTIPLICATIVE
CAPACITY
. . . . . . 32.2. S
EQUESTRATION
OF
PARASITISEDRED
BLOOD
CELLS
. . . . . . . . . . . . 43. P
ATHOLOGY
. . . . . . . . . . . . . . . . . 43.1. P
ATHOLOGY
OF
INFECTION
. . . . . . 43.2. M
ACROSCOPIC
APPEARANCES
. . . . . 53.3. M
ICROSCOPIC
APPEARANCES
. . . . . 53.3.1. V
ASCULAR
CONGESTION
. . . . 53.3.2. R
ING
HAEMORRHAGES
AND
GRANULOMA
FORMATION
. . . . . . . . . . . 53.3.3. C
ELLULAR
ELEMENTS
. . . . . . 63.3.4. P
IGMENT
. . . . . . . . . . . . 63.4. R
ELATIONSHIP
BETWEEN
SEQUESTRATION
AND
CEREBRAL
DISEASE
. . . . . . . . . . . . . . . . . 64. P
ATHOGENESIS
—H
OST
F
ACTORS
. . . . . . 74.1. M
ECHANICAL
HYPOTHESIS
. . . . . . . 74.2. T
OXIN
HYPOTHESIS
. . . . . . . . . . . 84.3. C
YTOKINE
HYPOTHESIS
. . . . . . . . 84.4. O
THER
CYTOKINES
AND
MARKERS
OF
ENDOTHELIAL
CELL
ACTIVATION
. . . 94.5. N
ITRIC
OXIDE
. . . . . . . . . . . . . . 94.6. R
EACTIVE
OXYGEN
SPECIES
. . . . . 104.7. T
HE
PERMEABILITY
HYPOTHESIS
. . . 114.7.1. E
XPERIMENTAL
EVIDENCE
. . 114.7.2. B
LOOD
-
BRAIN
BARRIERIN
HUMANS
. . . . . . . . . . 114.8. T
HE
IMMUNOLOGICAL
HYPOTHESIS
. . . . . . . . . . . . . . 124.8.1. E
XPERIMENTAL
EVIDENCE
. . 124.8.2. C
LINICAL
STUDIES
. . . . . . 125. P
ATHOGENESIS
—P
ARASITE
F
ACTORS
. . 125.1. C
YTOADHERENCE
. . . . . . . . . . . 125.2. R
OSETTING
. . . . . . . . . . . . . . 135.3. R
HEOLOGY
. . . . . . . . . . . . . . 14
6. C
LINICAL
D
EFINITIONS
AND
P
RESENTATIONS
. . . . . . . . . . . . . 146.1. S
EVERE
MALARIA
. . . . . . . . . 146.2. C
EREBRAL
MALARIA
. . . . . . . 166.2.1. D
EFINITION
OF
CEREBRAL
MALARIA
. . . . . . . 166.2.2. C
OMA
SCORES
. . . . . 186.2.3. C
LINICAL
PRESENTATION
OF
CEREBRAL
MALARIA
IN
A
FRICAN
CHILDREN
. . . 186.2.4. N
EUROLOGICAL
SEQUELAE
. . . . . . . 196.3. M
ETABOLIC
ABNORMALITIES
IN
SEVERE
MALARIA
. . . . . . . . . 236.4. S
EVERE
MALARIAL
ANAEMIA
,
JAUNDICE
,
AND
HAEMOLYSIS
. . . 246.5. T
HE
COMMONEST
MODES
OF
PRESENTATION
OF
SEVEREMALARIA
IN
CHILDREN
. . . . . . 246.6. M
ODERATE
MALARIA
. . . . . . . 257. PATHOPHYSIOLOGY . . . . . . . . . . . 25
7.1. FEVER . . . . . . . . . . . . . . . 257.2. COMA . . . . . . . . . . . . . . . 257.3. SEIZURES . . . . . . . . . . . . . 267.4. RAISED INTRACRANIAL
PRESSURE . . . . . . . . . . . . . 267.5. CAUSES OF NEUROLOGICAL
SEQUELAE . . . . . . . . . . . . . 277.5.1. ISCHAEMIA . . . . . . 277.5.2. REACTIVE OXYGEN
SPECIES . . . . . . . . 277.5.3. EXCITOTOXINS . . . . . 277.5.4. APOPTOSIS . . . . . . . 287.5.5. HEMIPARESIS . . . . . . 287.5.6. VISUAL IMPAIRMENT . . 28
7.6. HYPOGLYCAEMIA . . . . . . . . . 297.7. LACTIC ACIDOSIS . . . . . . . . . 307.8. ANAEMIA AND
THROMBOCYTOPAENIA . . . . . . 317.9. ELECTROLYTE ABNORMALITIES
AND FLUID BALANCE . . . . . . . 327.10. RENAL IMPAIRMENT AND ‡ Corresponding authors.

2 C. R. J. C. Newton and S. Krishna
BLACKWATER FEVER . . . . . . . 337.11. SECONDARY INFECTIONS . . . . . 33
8. ANTIMALARIAL TREATMENT . . . . . . 338.1. INTRODUCTION . . . . . . . . . . 338.2. CINCHONA ALKALOIDS . . . . . . 348.3. 4-AMINOQUINOLINES . . . . . . . 358.4. ARTEMISININ DERIVATIVES . . . 35
9. ADJUNCTIVE MEASURES . . . . . . . . 359.1. ANTIPYRETICS . . . . . . . . . . 359.2. ANTICONVULSANTS . . . . . . . 369.3. MEASURES TO REDUCE RAISED
INTRACRANIAL PRESSURE . . . . 379.4. CORRECTION OF
HYPOGLYCAEMIA. . . . . . . . . . 37
9.5. ACIDOSIS . . . . . . . . . . . . . 389.6. ANAEMIA AND EXCHANGE
TRANSFUSION . . . . . . . . . . . 399.7. DESFERRIOXAMINE . . . . . . . . 399.8. ANTI-INFLAMMATORY AGENTS . . 40
9.8.1. CORTICOSTEROIDS . . . 409.9. AGENTS THAT IMPROVE
MICROCIRCULATORY FLOW . . . . 409.9.1. PENTOXIFYLLINE . . . . 409.9.2. MISCELLANEOUS AGENTS . 40
9.10. OTHER AGENTS . . . . . . . . . . 4010. DISCUSSION AND FUTURE STUDIES . . . 40ACKNOWLEDGEMENTS . . . . . . . . . . . . . 41REFERENCES . . . . . . . . . . . . . . . . . . 41
ABBREVIATIONS. BBB, blood-brain barrier; BCS, Blantyre coma score; CM, cerebral malaria; CPP, cerebralperfusion pressure; CSF, cerebrospinal fluid; CT, computerised tomography; CVP, central venous pressure; DAT,direct antiglobulin test; DCA, dichloroacetate; E-selectin, endothelial selectin; ICAM-1, intercellular adhesionmolecule-1; ICP, intracranial pressure; Ig, immunoglobulin; IH, intracranial hypertension; IL, interleukin; iNOS,inducible nitric oxide synthase; NCM, non-cerebral malaria; NO, nitric oxide; NPRBC, nonparasitised red bloodcell; Pfemp-1, Plasmodium falciparum erythrocyte membrane protein-1; PRBC, parasitised red blood cell; ROS,reactive oxygen species; TNF, tumour necrosis factor; TPI, triose phosphate isomerase; VCAM-1, vascular celladhesion molecule-1; WHO, World Health Organisation.
1. INTRODUCTION
Malaria is one of the most common and important parasiticdiseases worldwide. About 40% of the world’s populationlives in malaria-endemic areas (Sturchler, 1990), and malariais responsible for up to 500 million episodes of clinical infec-tion and 2.7 million deaths every year (World Health Organ-isation, 1996). Plasmodium falciparum is the principal causeof severe disease, since the other species of malaria rarelycause death or persistent sequelae. P. falciparum may infecthumans at any time from conception to adulthood. Malarialinfection probably results in 3.5 million low birth-weightinfants every year (Steketee et al., 1996), since an estimated24 million pregnant women live in malaria-endemic areas.Children living in sub-Saharan Africa bear the brunt of thedisease, as they are exposed to malaria frequently after birth,and either die from complications or experience clinical epi-sodes of infection for many years until the slow and capriciousdevelopment of antimalarial immunity (Edington, 1967).This balance between acquisition of immunity and develop-ment of severe disease has continued for thousands of years.
Since the first description of malarial parasites in a suf-ferer by Laveran in Constantine, Algeria in 1880, therehave been considerable advances in the understanding ofdisease mechanisms in malaria (Laveran, 1880; White andHo, 1992). These advances have resulted from detailedstudies in patients, animal models of infection, biochemi-cal, cellular, and molecular investigations. These studieshave illuminated our understanding of disease processes, al-though none have succeeded so far in reducing mortalityfrom severe infection. Mortality from treated severe malariain children is between 5 and 15% (Waller et al., 1995;Marsh et al., 1995), and the current management of severemalaria has changed surprisingly little, in spite of rapid sci-entific advances in malariology.
Measures to eradicate malaria have been ineffective(World Health Organisation, 1993). After the initial suc-
cesses in the 1960s, insecticides have failed to curb trans-mission by anopheline mosquitoes (World Health Organi-sation, 1993). Insecticide-impregnated bednets have reducedmortality and morbidity in malarious areas (Nevill et al.,1996; D’Alessandro et al., 1995c), but their efficacy maynot be sustainable (D’Alessandro et al., 1995b; Greenwood,1997). Results of recent trials with the current generation ofmalaria vaccines have been unimpressive (D’Alessandro etal., 1995a; Alonso et al., 1994), although newer prototypesare under continuous investigation (Stoute et al., 1997; Tar-gett, 1995). Therefore, it probably will require a concertedcombination of measures, including antimalarials, vaccines,and vector control, before a reduction in infection and mortal-ity can be maintained. Furthermore, reducing the transmissionof malaria in an endemic area runs the concomitant risk ofreducing the development of antimalarial immunity in thepopulation. This reduction in “herd immunity” eventuallymay result in the rapid spread of severe infection if controlmeasures fail, so that longer-term study of preventive inter-ventions will be crucial to assessment of their true and sus-tainable worth. The goal of effective prevention is not yetachievable, and consequently, we will still need to managecases of severe malaria in the foreseeable future.
The early effective treatment of falciparum infection iscritical in preventing the progression to severe, life-threat-ening disease. Falciparum malaria has become increasinglyrefractory to chloroquine, the cheapest and most widelyavailable antimalarial (Krishna and White, 1996; Zucker etal., 1996). In Southeast Asia, multidrug resistance is rapidlyspreading (Pukrittayakamee et al., 1994a; White, 1992), in-creasing the likelihood of severe disease. In Africa, wide-spread chloroquine resistance has increased the incidenceof some complications such as anaemia (because of inabilityto cure infections) (Lackritz et al., 1992), and other relatedproblems are anticipated to worsen as higher-grade resis-tance becomes entrenched.

Pathophysiology and Supportive Treatment of Severe Malaria 3
Newer antimalarial treatment regimens testing, for ex-ample, the efficacy of artemether against quinine in chil-dren with severe malaria, have not confirmed any advan-tage for artemether in terms of survival (van Hensbroek etal., 1996a). Yet, in vitro, the artemisinin derivatives aresome of the most rapidly parasiticidal drugs, with the broad-est stage-specificity of action (Murphy et al., 1995b; terKuile et al., 1993), and indeed, in vivo, they clear circulat-ing parasites much faster than other antimalarials (Hienand White, 1993). This observation, that the use of morerapidly parasiticidal drugs may not affect mortality, pointsto alternative directions for further research designed to re-duce mortality in children with malaria. These alternativeapproaches are based on detailed studies of the pathophysi-ology of infection (White and Ho, 1992), and are aimed atreversing or ameliorating those disease processes that maycontribute directly to a fatal outcome, in spite of the rapidadministration of effective antimalarials to the patient.These adjunctive therapies are designed to support severelyill children until the underlying disease can be reversed bythe antimalarial treatment. This review focuses on keypathophysiological observations made in children with se-vere malaria that may guide the eventual development ofsuch adjunctive therapies.
2. DEVELOPMENT OF INFECTION
Clinical symptoms and signs of malaria occur when P. falci-parum-infected erythrocytes multiply asexually (Marchi-afava and Bignami, 1894). The hepatic stages and gameto-
cytes are asymptomatic. The cause of P. falciparum’svirulence in comparison with other human parasites is un-known, but its multiplicative capacity and ability to seques-ter in the deep vascular beds are thought to contribute.
2.1. Multiplicative Capacity
The median number of falciparum sporozoites initiating in-fection is 8–15, but this may reach up to 100 sporozoites(White and Ho, 1992). In comparison with other malariaparasites, P. falciparum has a shorter pre-erythrocytic stage(5–7 days), prepatent period (interval between infection andthe appearance of parasites in the erythrocytes), and incuba-tion period (interval between infection and onset of symp-toms). It also produces more merozoites from liver schizontsand after erythrocytic merogony.
Each infecting exo-erythrocytic merozoite can yield upto 36 daughter meronts once the erythrocytic stage of infec-tion is initiated from the liver. Untrammelled multiplica-tion rates in this stage of infection can exceed 10 per cycle,logarithmically expanding the parasite burden in an indi-vidual. Within a few days, a few thousand parasites liber-ated from the liver can progress to a total parasite burden of.1012 parasites in adults (Fig. 1) (White et al., 1992a;White and Krishna, 1989). The threshold of microscopicdetection is reached after 3–4 asexual cycles, and a lethalparasite burden may be reached in another 3–4 cycles.Young children will begin the asexual phase of parasite de-velopment at a higher parasitaemia, as they have a smallerblood volume in which to dilute the merozoites liberated byhepatic merogony (White and Krishna, 1989). Thus, in a
FIGURE 1. Estimates of the in-crease in malaria parasites infect-ing an adult during the exponen-tial growth phase of a relativelysynchronous infection; effectsof sporozoite load and multipli-cation rate on time to reach po-tential lethal parasitaemia (as-suming unchanged clearance andmultiplication rates). Reproducedfrom White and Krishna (1989),with permission of the copyrightholder, Royal Society of Tropi-cal Medicine and Hygiene.

4 C. R. J. C. Newton and S. Krishna
young child with a blood volume of 500 mL, a lethal parasi-taemia could develop in 8 days from hepatic merogony(White et al., 1992a). P. falciparum can invade red cells ofany age, and since more than one merozoite can infect asingle erythrocyte, multiply infected erythrocytes are com-mon in falciparum malaria.
2.2. Sequestration of Parasitised Red Blood Cells
During the first half (24 hr) of the parasite’s life cycle, theparasitised red blood cell (PRBC) is metabolically quies-cent. There is a modest increase in parasite size and the ex-pression of some parasite antigens on the surface of the in-fected erythrocyte. These PRBCs continue to circulate andare visible by microscopic examination of a patient’s blood.By contrast, the remaining 24 hr of development are char-acterised by intense synthetic and metabolic activity (Sher-man, 1979). The PRBCs express molecules on the erythro-cyte surface, which allows the cells to sequester in vascularbeds. These include the expression of a recently identifiedfamily of parasite-encoded genes (the var genes), which areprimarily responsible for increasing the adhesiveness ofPRBCs to host ligands expressed on capillary and post-cap-illary venules (Su et al., 1995). The adhesion of cells infectedwith mature stages of parasites to capillary beds removesmost of them from the circulation, thereby preventing theirdestruction by the spleen. It also allows asexual growth ofthe parasite and division to occur in a favourable hypoxicenvironment, and perhaps allows more efficient invasion oferythrocytes after schizogony (Marsh et al., 1988).
Observations on the age distribution of different stages ofparasite development on admission blood films suggest thata preponderance of more mature forms (.20% trophozoitesor schizonts, for example) is a prognostic indicator for fatal-ity (Silamut and White, 1993). These circulating matureforms easily can be quantitated on peripheral blood filmsand probably represent a fraction of the total sequesteredparasite burden.
At this later developmental stage, there is a surge in theuptake of essential synthetic precursors, such as glucose (upto 25- to 50-fold increase compared with uninfected eryth-rocytes), amino acids, and nucleosides (Elford et al., 1995).The uptake of these metabolites and the disposal of lactate,the principal waste product resulting from the parasite’sanaerobic glycolysis, are mediated through poorly under-stood transport processes (Elford et al., 1995; Kanaani andGinsburg, 1991). These biochemical changes are associatedwith a rapid increase in parasite size, the visible depositionof haemozoin in the PRBC, and subsequently syncytial nu-clear division, which produces daughter merozoites (Leeteand Rubin, 1996). The factors that signal cell rupture whenmultiplication is complete are also not understood, but sub-sequent invasion of red cells takes place within a few min-utes, and the developmental cycle is re-initiated.
Sequestration of PRBCs is thought to give rise to thecomplications of falciparum malaria (White and Ho, 1992),which define severe disease. A consequence of sequestra-
tion is that circulating parasitaemia is not representative ofthe total parasite biomass in the patient. Indeed, the para-sites visible on microscopy have not adhered to host tissuesand are unlikely to be contributing directly to severe symp-toms of disease (White and Krishna, 1989). Furthermore,studies carried out on these circulating parasites, especiallyex vivo studies, may not represent the pathogenic potentialof sequestered parasites. As sequestered parasites are muchmore metabolically active when mature, their increased re-quirements for synthetic precursors, such as glucose and nu-cleosides, may compete directly with the needs of adjacenthost tissue. This potential for metabolic diversion is an im-portant additional consideration in the pathogenesis of se-vere malaria, particularly cerebral malaria (CM).
3. PATHOLOGY
The finding of relatively mature parasites within the deepvascular bed at post mortem was made soon after the dis-covery of the parasite (Marchiafava and Bignami, 1894),and gave rise to the “mechanical” hypothesis for the patho-genesis of severe malaria. This hypothesis has dominatedthe thinking of severe malaria during this century. We willfirst discuss the pathological basis of this theory, describingthe pathology of severe malaria, after which we will furtherdiscuss the mechanistic theory and other theories of thepathogenesis.
3.1. Pathology of Infection
One of the difficulties of interpreting pathological findingshas been heterogeneity in the clinical features of malaria(discussed in Section 6), particularly age-dependent andgeographical disparities. The lack of clinical definition inmost pathological studies has particularly hampered inter-pretation. This review focuses on pathological findings ob-served in CM as a clinically identifiable syndrome of severedisease. Clinico-pathological correlates in severe non-CM(NCM) still require further detailed studies, which shouldbe guided by validated clinical definitions.
Most pathologists have defined cerebral involvement asthe presence of sequestered parasites in the brain (Turner etal., 1994; Aikawa et al., 1980; Edington and Gilles, 1976;Thomas, 1971; Lemercier et al., 1966; Spitz, 1946). How-ever, patients who die of noncerebral complications, e.g.,renal failure, without clinical evidence of cerebral involve-ment, may also have cerebral sequestration (MacPherson etal., 1985). Resolving these apparent discrepancies requirescareful quantitative comparisons of parasite density in cere-bral and other tissues obtained from patients with meticu-lously documented clinical histories. These studies are nowin progress and will be valuable in further establishing thevalidity of the mechanical model for malaria (Turner, 1997).Alternatively, a method of quantitating the total parasiteburden in an individual with malaria would also allow a di-rect test of the mechanical hypothesis, but this has notproved possible by simple methods (Davis et al., 1990a).

Pathophysiology and Supportive Treatment of Severe Malaria 5
Most post-mortem studies [reviewed by Turner (1997)]have been conducted on adults, and in those series that in-clude children, differences between adults and childrenhave not been highlighted. The original autopsy studies inchildren were from Africa (Lemercier et al., 1966; Thomas,1971; Edington and Gilles, 1976), and few have been per-formed elsewhere.
3.2. Macroscopic Appearances
In CM, brains packed with PRBC have a slate-grey discol-oration, which is evident on the cut surfaces of the brain inboth adults (Toro and Roman, 1978; Schmid, 1974; Khanand Durham, 1945; Dhayagude and Purandare, 1943; Thom-son and Annecke, 1926; Aikawa et al., 1980) and children(Thomas, 1971; Lemercier et al., 1966; Edington and Gilles,1976). The colour reflects the presence of malarial pigment(haemazoin). Meningeal vessels are often congested, withsurrounding haemorrhage and some infiltration of leuco-cytes (Spitz, 1946; Khan and Durham, 1945; Dhayagudeand Purandare, 1943; Boonpucknavig and Boonpucknavig,1988; Thomson and Annecke, 1926). Haemorrhages, de-scribed as “punctiform” or “ring haemorrhages,” are a com-mon pathological feature of CM and are distributedthroughout the brain (including the brainstem). They aremore common in children who have had convulsions asso-ciated with CM than in other children (Thomas, 1971).
A recent controversy has been the frequency with whichcerebral oedema complicates CM, and how this swellingmay contribute to mortality. The macroscopic features ofoedema, such as increase in brain weight and compressionof cerebrospinal fluid (CSF) spaces (e.g., gyri, ventricles,and pericisternal spaces), are observed in CM. The brainsof African children (Walker et al., 1992; Edington andGilles, 1976) and adults (Janota and Doshi, 1979; Rigdonand Fletcher, 1945) dying with CM frequently appearedswollen with flattened gyri. Thomas reported macroscopicoedema and an increase in brain weight by more than 10%in 10/13 (77%) Ugandan children with CM (all of whomwere less than 5 years old), with white matter oedema moremarked in the heavier brains (Thomas, 1971). However, ina Nigerian study, only one child had a heavy brain (Walkeret al., 1992), although severe oedema was observed in 5/7(71%) children with CM. Ventricular compression (with-out accompanying oedema) was seen in 79% of childrenwith P. falciparum sequestered in their brains (Lucas et al.,1996), although these children may not have had CM sinceclinical details were lacking. Another study reported the in-cidence of cerebral oedema as similar in adult patients dy-ing of CM and those dying without cerebral disease (Ri-ganti et al., 1990), suggesting that it did not contribute tocerebral disease.
It has often proved difficult to distinguish oedematouschanges seen at post-mortem from those occurring in life,or those arising in the agonal state. Cerebral swelling mayalso occur because of increased blood volume in cerebraltissues (Newton et al., 1991a) due to sequestration and mi-
crovascular obstruction. These changes can cause ventricu-lar compression without associated tissue oedema. In viewof the potential therapeutic implications, the presence ofcerebral oedema and the delineation of its role in causingdeath from CM is an important area for future pathologicalstudies in African children. Studies are in progress to ad-dress some of these issues (T. Taylor, web site: http://www.niaid.gov./ictdr/Blantyre.htm).
3.3. Microscopic Appearances
The earliest microscopic observations have dictated muchof the current thinking about the pathogenesis of severe fal-ciparum malaria. In 1949, Clark observed:
There is intense congestion of the vessels through-out the brain and spinal cord with special promi-nence in the cortical layer of both the cerebrumand cerebellum. These capillaries contain bothparasitised and non-parasitised erythrocytes, de-pending on the terminal degree of parasitaemiaand localisation. Frequently one area of the cortexwill show scattered parasites while other areas willreveal almost complete parasitisation of the eryth-rocytes and no satisfactory explanation for thisphenomenon is available (Clark and Tomlinson,1949).
As discussed in Section 5, molecular explanations for thisphenomenon have emerged recently.
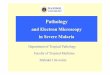
3.3.1. Vascular congestion. Cerebral capillaries and venulesdistended with PRBCs are the microscopic hallmark of se-vere falciparum malaria (Fig. 2). In contrast to the periph-eral blood, all mature stages of the parasite are seen withinthese vessels, both in adults (Spitz, 1946; MacPherson etal., 1985; Cropper, 1908; Aikawa et al., 1980), as well as inAfrican children (Lemercier et al., 1966). The distendedvenules are more prominent in the gray matter, where theyappear evenly distributed. Arteriolar dilatation has beennoted (Dudgeon and Clarke, 1917), although arteriolarconstriction was also described in one study (Polder et al.,1991).
3.3.2. Ring haemorrhages and granuloma formation.Ring haemorrhages contain a blocked central capillary,with an agglutinated mass of PRBCs surrounded by braintissue that is necrotic and contains demyelinated fibres(Spitz, 1946; Boonpucknavig and Boonpucknavig, 1988) ora glial reaction. More recently, it has been suggested thatthe “haemorrhages” are a specific response to blockage of avessel by PRBCs and reperfusion, resulting in the concen-tric pattern of haemorrhage surrounding a necrosed vessel(Turner, 1997), and are, therefore, different from petechialhaemorrhages seen after a variety of hypoxic insults, e.g.,typhus fever (Vietze, 1978). Small malarial granulomata(Dürck’s nodules) are a distinctive pathological feature ofmalaria (Dhayagude and Purandare, 1943; Thomson and

6 C. R. J. C. Newton and S. Krishna
Annecke, 1926) associated with ring haemorrhages. Theyare not found in patients who die shortly after the onset ofsymptoms (Dhayagude and Purandare, 1943), and probablyrepresent a more advanced stage of repair following haem-orrhage in which necrotic tissue has been replaced by neu-roglial cells and microglial tissue (Spitz, 1946; Edingtonand Gilles, 1976; Dhayagude and Purandare, 1943).
The presence of thrombotic lesions in CM is controver-sial. Some authors have described thrombi in the white andgray matter (Dudgeon and Clarke, 1917; Aikawa et al.,1980), often associated with ring haemorrhages or granulo-mata, although they do not contain PRBC (Spitz, 1946). Incontrast, other pathologists have commented on the lack ofevidence for organising thrombi in adult brains (Janota andDoshi, 1979) or in children (Edington and Gilles, 1976).These haemorrhagic deposits do not contain platelets(MacPherson et al., 1985) or fibrin (Dudgeon and Clarke,1917). Since there is no evidence of fibrinolysis in mostcases of severe malaria (Warrell, 1987), these lesions areunlikely to be true thrombi.
3.3.3. Cellular elements. Capillary endothelial cells aredescribed as swollen (Sein et al., 1993; Pongponratn et al.,1991; Fitz-Hugh, 1944), necrotic, or desquamated (Aikawaet al., 1980). These changes appear only in samples takenmore than 5 hr after death (Oo et al., 1987), suggesting that
these features are post-mortem artefacts. The ultrastructureof capillaries appears well preserved, with only a few vesselsshowing patchy degenerative changes (MacPherson et al.,1985). Most pathologists have commented on the lack ofinflammatory cells both in adults (MacPherson et al., 1985;Fitz-Hugh, 1944; Dudgeon and Clarke, 1917) and Africanchildren (Thomas, 1971). However, an accumulation ofmacrophages (with active phagocytosis of PRBCs and pig-ment), neutrophils, and plasma cells has been seen in areasof extravasated PRBCs (Boonpucknavig and Boonpuck-navig, 1988), and has been interpreted as evidence of in-flammation. Some immunofluorescence studies have shownthe deposition of falciparum antigens and anti-falciparumantibody on the cerebral vessels (Aikawa, 1988), often as-sociated with haemorrhages in the white matter (Oo et al.,1987; Nagatake et al., 1992; Boonpucknavig and Boon-pucknavig, 1988), although other studies have not foundevidence of such deposition (Turner et al., 1994; MacPher-son et al., 1985). An increase in leukocytes in the cerebrumwas reported in a single case of CM, but the patient alsohad acquired immunodeficiency syndrome (Porta et al.,1993), which complicates interpretation of these findings.
3.3.4. Pigment. Malarial pigment or crystalline haemo-zoin is present in all erythrocytes that contain mature stagesof parasites. Pigment accumulates in monocytes and mac-rophages in those tissues where there is significant parasi-taemia, including in the peripheral circulation where itspresence is a prognostic indicator (Metzger et al., 1995; Phuet al., 1995). In a rodent model of infection, the longer thepreceding malarial infection, the more pigment is seen inthe reticuloendothelial system (Sullivan and Meshnick,1996). The presence of pigment in the brain of patientswith CM when PRBCs are no longer present implies thatcoma was prolonged, and death ensued even after tissueparasitaemia had begun to clear.
Pigment is composed of sheets of b-haematin, which de-rive from haem polymerisation after haemoglobin break-down by parasites. Most of the metabolised haemoglobin inthe cell contributes to pigment formation (Morrison andJeskey, 1948). Chloroquine, and perhaps other antimalari-als, were thought to interfere with the process of haem po-lymerisation by inhibiting a purported enzyme (Slater andCerami, 1992). More recently it has been shown that poly-merisation can proceed without protein present (Dorn etal., 1995), although parasite histidine-rich protein II accel-erates the process of haemozoin formation (Sullivan et al.,1996). Pigment was believed to be relatively inert and non-toxic, but it can clearly modulate important biological ac-tivities. The quantitation of pigment in human tissueseventually may prove to be as interesting as the quantita-tion of parasites.
3.4. Relationship betweenSequestration and Cerebral Disease
The degree and distribution of sequestered parasites variesaccording to the species of malaria parasite and host. For
FIGURE 2. Cerebral capillary packed with parasitised redblood cells in an African child. Courtesy of Professor S. Lucas.

Pathophysiology and Supportive Treatment of Severe Malaria 7
example, in the night monkey (Aotus trivirgatus), P. falci-parum sequestration affects in descending order myocar-dium, adipose tissue, and skeletal muscle, with no parasitesvisible in the brain (Miller, 1969). This difference in se-questration in animal models and humans is one of the keyfactors that complicates the extrapolation of findings in an-imal models to understanding of human disease.
The first semiquantitative assessment provided light andelectron-microscopic comparisons of samples obtained fromThai adults dying with strictly defined CM (n 5 7) andthose with multi-organ involvement without predominantcerebral symptoms (n 5 6) (MacPherson et al., 1985). Anadvantage of this study was early collection of specimens(~90 min after death), although only needle biopsies wereobtainable, which may have caused a sampling bias in theresults. Nevertheless, statistically significant differenceswere observed between clinical groups. Patients with CMhad more PRBCs and more vessels affected than NCM pa-tients. The degree of sequestration was greatest in thebrain, followed by the heart and then the liver, lung, andkidney, all of which contained larger numbers of PRBCsthan the blood. There was little evidence for haemorrhagicor inflammatory exudation in tissues, immune complexdeposition, or widespread thrombosis. Knobs on PRBCs ap-peared to be the site of attachment to endothelial cells,some of which were swollen.
A subsequent study also carried out in Thailand of 39 adultsconfirmed that the percentage of PRBCs in organs washigher in CM patients than in NCM patients (Pongponratnet al., 1991). Again in the CM group, the sequestration ofPRBCs in the brain was significantly higher than in other or-gans, and there was a strong correlation between peripheralparasitaemia and PRBC sequestration in brain (r 5 0.7031).This organ difference was not seen in the NCM group, al-though some degree of PRBC sequestration was visible in50% of the NCM cases. Interestingly in this study, lung tis-sue contained mononuclear cells rather than parasites.
In another study (Turner et al., 1994), based upon exper-imental observations on in vitro models of cytoadherence, adetailed quantitative analysis of expression of endothelialcell markers in tissues from adult patients (n 5 9) with fatalCM were compared with control patients (n 5 9). Therewas increased expression of intercellular adhesion mole-cule-1 (ICAM-1) and endothelial selectin (E-selectin) oncerebral vessels from malaria patients compared with con-trols. CD36 and thrombospondin staining was sparse in allcerebral tissue. Parasites co-localised to areas expressingICAM-1, CD36, and E-selectin, supporting the notion thatthese molecules may be important vascular ligands in vivo.There was additional evidence of endothelial cell activa-tion in malaria with increased expression of other markerssuch as human leucocyte antigen Class II antigens, butthese changes were not accompanied by increased local ac-cumulation of inflammatory cells. The most marked seques-tration of parasites was in the brain, confirming findingsfrom previous studies. There were also large accumulationsof parasites and pigment in the spleen and liver. The ob-
served increase in expression of receptors in severe malariamay be related to induction by high levels of so-called pro-inflammatory cytokines (see Section 4.3), which are foundin severe, particularly cerebral disease. These findings beginto provide a mechanistic explanation for the developmentof severe malaria, as well as linking the mechanical hypoth-esis with the cytokine hypothesis. A more recent largerpost-mortem study of 50 Vietnamese adults dying of severeand cerebral disease (Turner, 1997), found heterogeneity ofdistribution of parasites within cerebral tissue. Patients dy-ing later in the course of infection did not show sequestra-tion, although pigment was detectable. Some observers havereported that vessels congested with parasites are moreprominent in gray rather than white matter, and also thatthe cerebellum is affected more than other parts of the CNS(Sein et al., 1993).
4. PATHOGENESIS—HOST FACTORS4.1. Mechanical Hypothesis
The mechanical hypothesis assumes that organs will be af-fected in proportion to the overall number of PRBCs se-questered in tissues, as well as their relative proportionswithin different tissue capillary beds. Thus, CM arises be-cause of sequestration of PRBCs in cerebral capillaries andpostcapillary venules, whereas patients who may have simi-lar numbers of sequestered parasites in other tissues, but notthe brain, would not be expected to develop a full-blowncerebral syndrome. Patients, of course, may have other signsof severe disease, as many other organs, particularly theliver and spleen are frequently congested with PRBCs.
The mechanical hypothesis has been questioned by anumber of investigators. The two main objections havebeen the lack of sequestration in some patients with cere-bral symptoms associated with falciparum malaria, and thefact that most patients with CM recover without evidenceof ischaemic damage.
The lack of massive intracerebral sequestration of para-sites in some patients with CM can be rationalised in anumber of ways (Sections 4.3–4.8) (Berendt et al., 1994).Since CM is a diagnosis of exclusion (Section 6.2), otherdiagnoses (e.g., encephalitis) (White et al., 1992b) may nothave been excluded, and the coexistence of factors such ashypoglycaemia may also cause impairment of conscious-ness. Furthermore, the mechanical hypothesis may be un-able to explain why all patients with malaria die. In sometreated cases of malaria and coma, patients have died with-out any parasites visualised on histological examination, al-though changes in host tissues may be similar to those seenin patients dying with parasite-engorged capillaries (Dud-geon and Clarke, 1917). An obvious explanation for thesefindings is that parasites have responded successfully totreatment, but that pathophysiological processes have pro-gressed to an irreversible stage, and resulted in a fatal out-come. There are, however, additional hypotheses that at-tempt to explain severe malaria and more particularly CM,and these are discussed below.

8 C. R. J. C. Newton and S. Krishna
4.2. Toxin Hypothesis
Gaskell and Miller (1920) were the first to propose that pa-tients with malaria died from an overwhelming toxaemia.The kallikrein-kinin system was shown to be important inmurine and simian models of Plasmodium infection (Mae-graith and Fletcher, 1972), but similar evidence in humansis lacking (Warrell, 1987). Clark suggested alternative tox-ins were responsible for the clinical features of severe ma-laria, initially suggesting endotoxins (Clark, 1978), then re-active oxygen species (ROS) (Clark et al., 1986), cytokines(Clark et al., 1987), and nitric oxide (NO) (Clark et al.,1992). Although endotoxins are detectable in patients withfalciparum malaria, they are associated with parasitaemiaand leucocytosis, but not specifically with severe disease,including CM (Usawattanakul et al., 1985; Aung-Kyaw-Zaw et al., 1988). ROS are discussed in Section 4.6. Morerecent studies are attempting to isolate and characterisemalarial material, possibly a glycosylphosphatidylinositolmoiety associated with malarial antigens, which can causerelease of cytokines from host cells (Schofield and Hackett,1993) and up-regulate adhesion ligands (Schofield et al.,1996) and NO (Tachado et al., 1996) (Section 4.5).
4.3. Cytokine Hypothesis
Clark and co-workers suggested that cytokines caused CM(Clark et al., 1991; reviewed in Clark and Rockett, 1994).They suggested that the host overproduction of “pro-inflam-matory” cytokines, such as tumour necrosis factor (TNF)and interleukin (IL)-1, is capable of inducing cerebral syn-dromes in patients with malaria. Localisation of parasites tocertain tissues by sequestration would result in higher localsynthesis and release of these potent mediators, and causemore marked local derangements in function and metabo-lism of tissues than elevations in circulating cytokines.Clearly, in those patients in whom there is no significantsequestration, but cerebral symptoms are still present, othermechanisms would have to be invoked to explain coma.These have not been defined further in the cytokine hy-pothesis.
P. falciparum-infected erythrocytes produce pyrogenicmaterial that triggers the release of TNF (and other cyto-kines) from host mononuclear cells (Kwiatkowski et al.,1989). Merogony (soon after which parasite material is lib-erated in largest quantities into the circulation in vivo) pro-vokes the largest pulses of TNF release in vitro (Kwiat-kowski, 1989). Elevations of TNF result in pyrexia in bothfalciparum (Kwiatkowski et al., 1989) and vivax malaria(Karunaweera et al., 1992). A monoclonal antibody againstTNF attenuates fever in children with CM, confirming theimportance of TNF in causing fever (Kwiatkowski et al.,1993). In the relatively benign vivax malaria (without cere-bral symptoms), very high (up to 3000 pg/mL) TNF levelshave been measured transiently in serum (Karunaweera etal., 1992), suggesting that such high systemic levels do notthemselves cause serious disease. Furthermore, elevations inTNF can exert antiparasitic effects by inhibiting parasite
multiplication and synergising with other factors to pro-duce gametocidal effects (de Naotunne et al., 1993).
Parasite-derived material is responsible for TNF releasefrom host cells (Bate and Kwiatkowski, 1994), and in onestudy, parasites varied in their ability to induce TNF release(Allan et al., 1993). This variation correlated with thesource of the parasites; those obtained from patients withcerebral disease induced more TNF release ex vivo thanthose from patients with uncomplicated disease (Allan etal., 1995). There was considerable overlap in TNF releas-ing activity between disease groups, and ~60% of parasitesisolated from patients grew sufficiently to allow assay (Al-lan et al., 1995). It is possible that TNF may also be an ef-fector arm of some parasite virulence factors if it has a cen-tral role in the pathophysiology of severe malaria.
The consensus that has emerged from a vast literature onexperimental studies on the role of cytokines in malaria isthat the timing and amounts of different cytokines that arereleased, particularly TNF, may be important determinantsof subsequent pathophysiological events and perhaps mor-tality. Thus, increased production of TNF early in malarialinfection may be protective, whereas prolonged, high TNFlevels may be detrimental. This temporal relationship hasbeen difficult to identify in humans. Furthermore, one ofthe difficulties in interpreting immunologically measuredelevations in cytokines, particularly when receptor bindingcan influence the unbound concentrations, is that the bio-logically active moieties (either circulating or local) maynot be represented in these measurements. Thus, bioassaysof circulating cytokines may be more relevant, but are morelaborious to perform.
In African children, circulating cytokines (particularlyTNF) are much higher in severe malaria than controls(Krishna et al., 1994b; Nyakundi et al., 1994; Shaffer et al.,1991; Kwiatkowski et al., 1990; Kern et al., 1989; Grau etal., 1989; Scuderi et al., 1986). In some studies, TNF levelsare correlated with parasitaemia (Nyakundi et al., 1994;Shaffer et al., 1991), but most studies detected higher levelsin children with CM rather than NCM. Based on this cy-tokine theory, studies have focused on TNF in CM to sub-stantiate if elevations in TNF are deleterious. These eleva-tions in TNF may exacerbate the tendency to sequestrationby the up-regulation of host ligand molecules responsiblefor cytoadherence of parasites, especially ICAM-1, vascularcell adhesion molecule-1 (VCAM-1), and E-selectin (seeSection 5.1), increasing mechanical obstruction of cerebralor other blood vessels. As localised TNF production maynot be detected by plasma assays, but nevertheless mayhave important pathophysiological consequences, TNFmeasurements have been carried out on CSF specimensfrom patients with CM, but the results from large series arelacking. Increased TNF may also have consequences on themetabolic status of patients (see Section 7.7) or in thepathophysiology of anaemia (Section 7.8).
Host factors are also important in determining the TNFreleased in response to infection. A TNF-a promoter poly-morphism has been shown to be associated with disease se-

Pathophysiology and Supportive Treatment of Severe Malaria 9
verity in Gambian children (McGuire et al., 1994), with ahomozygous polymorphism at 2308 bp relative to the startof TNF transcription associated with a 7.7-fold increase inthe relative risk of death or neurological sequelae in CM.Other TNF promoter polymorphisms are now the subject ofdetailed assessments in case control studies in malaria, aswell as other diseases. For example, in meningococcal disease,relatively low TNF production assessed ex vivo in first-degreerelatives of patients was associated with a 10-fold increasedrisk of fatal outcome (Westendorp et al., 1997). Interest-ingly, this variation in TNF production was unrelated topolymorphisms at 2308 bp and 2238 bp in the promoter.A further risk factor in meningococcal disease was in-creased production of IL-10, which synergised with the ef-fects of low TNF production, and this was associated with a20-fold increase in the risk of fatality. There is increased IL-10 production in severe malaria associated with elevationsin TNF levels (Anstey et al., 1996), which may contributeto severe disease.
An important test of the central role of TNF, therefore,was undertaken using anti-TNF monoclonal antibodies asadjunctive therapy to either quinine or artemether (in afactorial design) in children with CM, and assessing mortal-ity and neurological sequelae as endpoints (van Hensbroeket al., 1996b). In this largest double-blind placebo con-trolled study of severe malaria in African children, 302children were assigned to receive a mouse monoclonal anti-TNF antibody (B-C7) and 308 received placebo. Mortalitywas similar in the two groups (19.9% vs. 20.8%), adjustedodds ratio 0.9 (95% CI 0.57–1.42). However, residual neu-rological sequelae (assessed at 6 months) were detected in15 (6.8%) survivors in the study group, compared with 5(2.2%) of those receiving placebo, adjusted odds ratio 3.35(95% CI 1.08–10.4). The biological effectiveness of theanti-TNF antibody was confirmed in this study group bythe more rapid decline in rectal temperature in the treat-ment compared with the placebo group. Four hours aftertreatment, mean fall in temperature was 0.68C in the BC-7group compared with 0.28C in placebo (P 5 0.02). Thus, inthis rigorous test designed to establish a causal role in mor-tality due to increased TNF production, neutralisation ofcirculating TNF did not reduce mortality, but did producean appropriate antipyretic effect.
The simplest explanation for these findings is that in-creased circulating TNF associated with CM is an epiphe-nomenon in the complex array of pathophysiological pro-cesses and does not itself increase mortality. Indeed,interfering with elevated TNF levels may be harmful. Al-ternative explanations have been suggested, including thepossibility that antibody prolonged the action of TNF onendothelium by retaining it within the circulation. It mayalso be that the antibody was administered too late in thedisease process, when secondary cascades of mediators hadalready begun exerting their biological effects. In any case,the increased incidence of neurological sequelae after anti-TNF antibody administration suggests that future studiesdesigned to investigate this aspect of pathophysiology must
first overcome the simplest interpretation of these findingsthat increased TNF production is an appropriate responseto malaria infection, and abrogation of this response, there-fore, may be harmful. This interpretation is consistent alsowith the genetic studies reported on meningococcal disease(see above).
4.4. Other Cytokines andMarkers of Endothelial Cell Activation
TNF is recognised as being one of the most important ofthe pro-inflammatory cytokines, and elevations in TNFconcentrations trigger many secondary cytokine cascades insevere malaria. There are associated increases in IL-1 andinterferon-g concentrations, as well as increases in circulat-ing TNF receptors in acute infection. Circulating IL-6(Molyneux et al., 1991) and IL-8 levels (Friedland et al.,1993) are increased in falciparum infection. Interestingly,in relatively uncomplicated infections, IL-8 levels remainedelevated for up to 4 weeks after the acute infection hadbeen cured (Friedland et al., 1993).
Both falciparum and vivax infections are associated withincreases in circulating markers of endothelial cell activa-tion (serum ICAM-1, serum VCAM-1, and serum ELAM-1),and these markers were significantly higher in Gambianchildren with severe falciparum malaria compared with un-complicated infections (Jakobsen et al., 1994). These mark-ers were also elevated in nonimmune subjects, suggestingthat elevations are a consequence of cytokine activation byTNF. However, in a recent study in Gambian children, ma-laria was associated with elevations in circulating ICAM-1levels (which correlated with TNF and IL-1a levels), but el-evations were not related to disease severity (McGuire etal., 1996). Thrombomodulin, another marker of endothe-lial cell damage, was also significantly higher in nonim-mune adults with severe malaria compared with those withuncomplicated infections (Hemmer et al., 1994), and ele-vations were positively correlated with peripheral parasi-taemia and TNF-a levels.
4.5. Nitric Oxide
Since the cytokine hypothesis was first elaborated, NO hasbeen identified as a potential mediator for TNF action. NOis a short-lived, highly reactive molecule that has a widespectrum of biological activities. NO is involved in defenceby killing intracellular microorganisms (Vouldoukis et al.,1995; Wei et al., 1995), in maintaining circulatory status byits action on endothelial cells, and in neurotransmission(Vallance and Collier, 1994). It is produced both constitu-tively in certain tissues and in response to inflammatorystimuli through the action of cytokines that up-regulate thesynthesis of inducible NO synthase (iNOS or NOS2).
Clark et al. (1992) proposed that TNF increased NO pro-duction, which caused the coma of CM. This NO isthought to be produced in cerebral endothelial cells and todiffuse into brain tissue, interfering with neurotransmission(Clark et al., 1992). It may also cause neurological damage

10 C. R. J. C. Newton and S. Krishna
and sequelae by forming peroxynitrite (Lipton et al., 1993),although this was not part of the original hypothesis. An al-ternative suggestion for the role of NO in malaria is that itmay be important in host defence, particularly in intracel-lular killing of parasites. This dual pathogenic or protectiverole for NO is reminiscent of similar roles suggested for cy-tokines, and neither is mutually exclusive. However, testingthese hypotheses is challenging because of the evanescentnature of NO and the inapplicability of results from manyanimal studies to human infection. Instead, indirect mea-sures of increased NO synthesis have been used as markersfor the activity of iNOS. NO is metabolised to nitrate andnitrite, and since these products are stable in plasma andurine, they may be used as endpoints that reflect increasediNOS activity. The effects of diet and renal impairment onnitrate levels have to be taken into account when these in-direct measures are employed (Al Yaman et al., 1997; Pradaand Kremsner, 1997; Anstey et al., 1996). The evidence foran important role of reactive nitrogen intermediates in se-vere and CM vary with the populations that have been ex-amined.
In the largest study to date (Anstey et al., 1996), de-creased NO synthesis was noted in Tanzanian childrenwith CM compared with patients with uncomplicated orsubclinical infections. Changes in plasma TNF profiles wereconsistent with previous reports that progressively higherlevels were associated with increasing disease severity withhighest levels in fatal cases. Levels of the anti-inflammatorycytokine IL-10 were also increased in more severe disease,suggesting a mechanism by which NO synthesis could besuppressed in the patients with CM. In this study, increasedNO synthesis was interpreted as being protective of the de-velopment of cerebral and fatal disease, and, therefore, im-portant in defence rather than as a contributor to cerebralpathology. Some support for this suggestion comes fromwork with desferrioxamine in children with CM, where NOsynthesis was increased in desferrioxamine recipients com-pared with placebo recipients (Thuma et al., 1996).
In contrast, a study from Papua New Guinea noted eleva-tions in reactive nitrogen intermediates in children withCM compared with conscious patients and higher levels infatal cases compared with survivors (Al Yaman et al.,1996). Other smaller studies have also noted an associationbetween elevated levels of circulating nitrogen oxides andsevere malaria. However, African studies have failed to de-tect such an association (Agbenyega et al., 1997; Cot et al.,1994). In Ghanaian children, hyperlactataemia, a meta-bolic marker of disease severity, was not correlated withplasma nitrogen oxide levels, although it was clearly a prog-nostic marker for a fatal outcome and was correlated withdepth of coma (Agbenyega et al., 1997). These findings areillustrated in Fig. 3. In order to assess the intracerebral syn-thesis of nitrogen oxides, which may arise through local dif-fusion of NO if it is produced by cerebral endothelial cells,CSF measurements were performed in a subset of patientswith CM. Again, no elevations in nitrogen oxides were ob-served, suggesting that coma in malaria may not be due toderangements in NO metabolism.
Clearly, further studies are warranted to establish the im-portance of changes in NO metabolism in malaria. How-ever, the balance of evidence suggests that changes associ-ated with severe disease will be harder to establish thanthey have been with cytokines, and the role of NO inpathophysiology and defence is more subtle than resultsfrom plasma and CSF measurements can disentangle.
4.6. Reactive Oxygen Species
Clark et al. (1983) proposed that ROS may play a role inthe pathogenesis of severe malaria. They based this hypoth-esis on experimental studies in which they showed that theROS were produced during malaria infections of mice(Stocker et al., 1984). They also showed that antioxidantsprevent cerebral involvement (Thumwood et al., 1989), in-cluding the breakdown of the blood-brain barrier (BBB)(Thumwood et al., 1988), and attenuated the fall in hae-
FIGURE3. Relationship between(A) admission plasma lactate con-centration and (B) plasma con-centration of nitrogen oxides andthe Blantyre score. s, survi-vors; d, fatal cases. Reproducedfrom Agbenyega et al. (1997),with permission of the copyrightholder, Royal Society of TropicalMedicine and Hygiene, London.

Pathophysiology and Supportive Treatment of Severe Malaria 11
moglobin in mice (Clark and Hunt, 1983). Clark et al.(1986) suggested that extravasated erythrocytes may lead toROS generation, causing coma and damage to local tissues,including the brain.
In humans, there is some evidence that ROS play a rolein the pathogenesis. Monocyte generation of ROS was in-creased in adults with falciparum malaria, especially thosewith severe disease (Descamps Latscha et al., 1987; Dubeyet al., 1991). In Indian children with CM, products of lipidperoxidation were found in the CSF (Das et al., 1991), butthe lack of an assessment of the BBB made this interpreta-tion difficult. In African children, desferrioxamine, an ROSscavenger, appears to reduce the duration of deep coma(Gordeuk et al., 1992), although it has not been shown toimprove the outcome or decrease the incidence of neuro-logical sequelae. Desferrioxamine may act by other mecha-nisms (Section 9.7). Thus, ROS appear to be generated inacute malarial infections, but their role in the pathogenesisof complications is unclear.
4.7. The Permeability Hypothesis
In the 1960s, Maegraith and colleagues proposed that CMwas caused by the stasis of blood secondary to an inflamma-tory state (Maegraith and Fletcher, 1972). They suggestedthat kinins increase the permeability of the BBB, causingan efflux of plasma out of the vessels, thereby concentratingthe red blood cells within the cerebral vasculature and ulti-mately producing stasis of the blood. They based their hy-pothesis on the cerebral oedema found at post mortem inhumans and studies of animals infected with malaria.
4.7.1. Experimental evidence. In the Rhesus monkey(Macaca mulatta), Maegraith and colleagues showed an ef-flux of albumin from the blood into the CSF (Migasena andMaegraith, 1968b), and since albumin is the protein re-sponsible for 75% of the oncotic pressure, they suggestedthat the efflux of protein would draw water into the braininterstitium, causing cerebral oedema. However, they didnot find a significant increase in CSF albumin, but showedthat the protein was transported back into the blood at analmost equally fast rate (Migasena and Maegraith, 1968a).The increase in albumin transport did not appear to be as-sociated with a raised intracranial pressure (ICP), althoughthe pressure was not measured. Furthermore, they showedthat chloroquine and hydrocorticosterone reduced the flowof protein in both directions in the monkeys (Migasena andMaegraith, 1968b; Maegraith and Fletcher, 1972), suggest-ing that the breakdown of the BBB was caused by inflam-mation. These experiments led to the widespread use of ste-roids in human CM (Rees, 1982; Woodruff and Dickinson,1968), an intervention subsequently shown to be inappro-priate (Warrell et al., 1982b).
There are important differences between monkeys dyingof knowlesi malaria and humans with CM. P. knowlesi se-questers preferentially within the liver and the small intes-
tine, with hardly any accumulation within the brain. Thus,despite rising parasite counts, infected monkeys retain con-sciousness until just before death (Anonymous, 1987).
4.7.2. Blood-brain barrier in humans. The BBB is thoughtto be grossly intact, both in African children (Badibanga etal., 1986) and Thai adults (Warrell et al., 1986). In Zairianchildren with CM, the concentrations of CSF albumin, im-munoglobulin (Ig)G, and IgM were not raised comparedwith normal European children, and were significantly lowerthan another group of Zairian children, most of whom hadbacterial meningitis (Badibanga et al., 1986). These find-ings contrast with those in Thai adults with CM, in whom78% had evidence of intrathecal production of IgG (Chapelet al., 1987), although the studies are not directly compara-ble. The use of European controls may not be appropriate,since Kenyan children with febrile convulsions have lowerCSF protein concentrations than European children (Mac-Dougall, 1962). Furthermore, in 101 Kenyan children withCM, 25% had increased CSF protein concentrations(.0.45 g/L), 60% of those who developed permanent se-quelae and all (n 5 5) those who died had high concentra-tions (Newton, 1995). This would suggest that CSF find-ings in African children need to take into considerationthat the BBB is probably impaired and that elevated CSFconcentrations of substances may reflect plasma levels.
In the nonimmune adults, the data are difficult to inter-pret. In adult Thais with CM, the CSF levels of larger pro-teins such as a2-macroglobin were not raised, but theCSF:serum albumin ratio was significantly higher than inBritish controls, although there was no significant differ-ence in the ratios during coma compared with recovery norin fatal cases compared with those who survived (Warrell etal., 1986). Less radiolabelled albumin entered the CSF whilethe patients were unconscious than when they recovered,but the BBB appeared to be more permeable than in Euro-peans. The increase in the CSF:serum ratio of 77bromide re-ported in this study was thought to be caused by hypoxia in-terfering with the active transport of the bromide out of theCSF, but could be explained by an impairment of the BBB.
Warrell and colleagues (1986) suggested that their find-ings, together with normal lumbar puncture CSF pressuresin most patients and the lack of cerebral oedema on com-puterised tomography (CT) scans of adults who survive CM(Looareesuwan et al., 1983), implies that the BBB is grosslyintact in adults. However, these studies do not exclude thepossibility that an abnormal BBB (permeable to smallermolecules) and mild cerebral oedema, not detectable byCT, may contribute to the pathophysiology of CM. Indeed,Davis et al. (1992) have shown that there is an increase inpermeability of the retinal vessels to fluorescein in adultswith acute falciparum malaria, although this finding was as-sociated with biochemical indices of severity, but not thepresence of coma. Recent studies of Kenyan children withsevere malaria have not demonstrated an increased perme-ability of retinal vessels (Hero et al., 1997).

12 C. R. J. C. Newton and S. Krishna
4.8. The Immunological Hypothesis
In the 1950s, immunological mechanisms were invoked toexplain the low incidence of CM in malnourished Africanchildren since it was thought that they were immunodefi-cient (Edington, 1967). The effectiveness of chloroquine intreating CM was also partly attributed to its anti-inflamma-tory nature (Maegraith, 1969). Furthermore, immunologi-cal mechanisms have been invoked to explain the rela-tively late peak incidence of CM in children living inendemic areas, despite the fact that these children havebeen exposed to malaria prior to the development of thiscomplication.
4.8.1. Experimental evidence. Experimental work in the1960s demonstrated that golden hamsters that had a neo-natal thymectomy (Wright, 1968) or those that were givenantithymocyte serum were resistant to P. berghei infections(Wright et al., 1971). During the last decade, Grau and col-leagues (1989) have developed a murine model of CNS in-volvement using P. berghei ANKA in genetically susceptiblemice. Initially, they showed that CD41 T-cells were essen-tial for the development of neurovascular lesions (Grau etal., 1986) and then went on to demonstrate that T-cell-dependent macrophage activation led to the release of cy-tokines, including TNF, which mediated the developmentof these lesions (Grau et al., 1987a). Also, they showed thatcyclosporin prevented the development of neurological com-plications in mice (Grau et al., 1987b). There are funda-mental differences between rodent models of CNS involve-ment and humans with CM. In rodents, monocytes are theprincipal cells that adhere to the endothelium, with littlesequestration of PRBC. Igs are consistently deposited onthe cerebral endothelium in mice, but not in humans. Comais not a prominent feature of murine malaria; rather, theneurological manifestations are limb paralysis, deviation ofthe head, ataxia, and convulsions (Grau et al., 1989).
4.8.2. Clinical studies. Although immunological mecha-nisms are favoured mainly by experimentalists, they havealso been proposed by some investigators studying humanCM. Malaria infections induce cellular and humoral im-mune responses in humans, and proliferative glomerulone-phritis, a manifestation of immunological disease, has beenreported in falciparum malaria (Boonpucknavig and Boon-pucknavig, 1988). Based upon pathologic specimens ofadults dying in South America, Toro and Roman (1978)suggested that CM is a form of disseminated vasculomyelin-opathy resulting from a CNS hyperergic reaction to a mas-sive antigenic challenge during a falciparum infection. Theperivascular inflammatory response, however, is not a fea-ture of CM, and the other features of a disseminated vascu-lomyelinopathy that are commonly seen in CM are not spe-cific and could also arise from terminal hypoxia (Warrell,1987). The more specific features of disseminated vasculo-myelinopathy were not found in all patients. An increase in
circulating immune complexes and the depletion of com-plement occurs in severe falciparum malaria, and in somestudies, is more common in CM than NCM (Warrell,1987). As mentioned in Section 3.3.3, immune complexdisposition on the cerebral vessels is not a consistent fea-ture of CM (Boonpucknavig and Boonpucknavig, 1988;MacPherson et al., 1985). Anti-inflammatory agents, suchas steroids (Hoffman et al., 1988; Warrell et al., 1982a), Ig(Taylor et al., 1992), or the immunosuppressive agent cy-closporin A (Warrell et al., 1990), have not been shown tobe beneficial in humans with CM.
5. PATHOGENESIS—PARASITE FACTORS
The macroscopic consequences of falciparum infection havebeen recognised for over a century, but the cellular and mo-lecular mechanisms that give rise to the fundamental patho-physiological process of sequestration have only begun to un-ravel in the past few years. Infection with P. falciparumchanges the host red cell in many and profound ways. Oneof these is by altering the surface property of infected cells tomake it “sticky.” This increased adhesiveness manifests itselfin ways that can be studied in laboratory models designed torepresent the in vivo microenvironment of the PRBC. How-ever, there is considerable functional redundancy in the par-asite and host-encoded factors that mediate the attachmentof PRBCs to other cells, making study of such mechanismsnot straightforward. Parasites can be selected to exhibit in-creased (or decreased) rosetting and cytoadherence pheno-types relatively easily in vitro, suggesting that similar pheno-typic plasticity may be important during the few cycles ofmultiplication necessary to produce a severe infection in anindividual. Furthermore, demonstrating a potential patho-genic mechanism in vitro is only the first step in assessing itseventual in vivo importance. The principal mechanismsthat are responsible for parasite virulence, the capacity toharm the host, are discussed in the following sections.
5.1. Cytoadherence
Understanding of the mechanisms of cytoadherence ofPRBCs to endothelial cells has grown from observationsmade at post-mortem in malaria patients to the develop-ment of in vitro models that have helped to identify hostligands, and eventually to the characterisation of responsi-ble parasite genes that are expressed at the erythrocyte sur-face. These more recent studies have reconciled the phe-nomenon of antigenic variation with the heterogeneity ofparasite-encoded adhesion molecules expressed in asexualstages of development, and now allow for more detailedstudies on their roles in pathogenesis of disease.
Cytoadherence describes the property of PRBCs to stickto nonerythrocytic cells or cell lines, and is the key patho-physiological process that distinguishes falciparum fromother human malarias. Cytoadherence depends on a highmolecular mass family of proteins encoded by var genes inP. falciparum. These var-encoded proteins [the P. falciparum

Pathophysiology and Supportive Treatment of Severe Malaria 13
erythrocyte membrane protein-1 (Pfemp-1) family] are ex-pressed on the surface of the infected erythrocyte and varyin molecular mass (between 200,000 and 350,000 Mr) (Smith,J. D. et al., 1995; Baruch et al., 1995) in parallel with parasitestrain-specific antigenic variation. They are also responsiblefor agglutination of infected cells when exposed to strain-specific antibodies. These immunological properties helpedto confirm the relationship between the var gene family identi-fied during the hunt for the chloroquine-resistance gene andthe properties of culture-adapted parasite clones varying intheir cytoadherence and rosetting phenotypes, as well as intheir variant surface antigens (Smith, J. D. et al., 1995).
Interestingly, sequence analysis of var genes shows a 2-exonstructure (with an approximately 1-kb intron), which, whentranslated, contains degenerately homologous domains, withsimilarity to previously identified proteins implicated in theinvasion of erythrocytes (Adams et al., 1992). These regionsof the var genes contain cystein-rich motifs similar to theDuffy-binding protein of P. vivax responsible for red cell in-vasion and, therefore, have been called “Duffy binding like”regions (Su et al., 1995). Thus, entry into red cells, antigenicvariation, and evasion of host clearance by cytoadherenceare probably all properties mediated by similar primary se-quences. Antigenic variation in a cloned parasite line is de-tectable at a rate of ~2.4% per asexual generation (Robertset al., 1992). It has been estimated that there are up to ~150copies of the var gene family in the haploid genome of falci-parum, accounting for between 2 and 6% of the whole para-site genome underlining the potential functional redundancyand significance of these gene products for the parasite.
Pfemp-1 is localised primarily to parasite-induced “knobs”on the surface of red cells. These knobs are small (60–100nm in diameter) electron-dense structures consisting ofsubmembranous accretions of parasite proteins, such as his-tidine-rich protein-1 and the mature parasite-infectederythrocyte surface antigen protein (Howard et al., 1990).Knobs form the supramolecular structures that allow appo-sition to host ligands on endothelial cells, and fine “pro-cesses” are visible on electron microscopy that span theseputative attachment sites. However, not all natural infec-tions are associated with knobs, and parasite clones isolatedin vitro can still bind without knobs, suggesting that knobscontribute to, but are not essential for, the process of cyto-adherence (Petersen et al., 1989). PRBCs can bind to a va-riety of host cells, such as monocytes, neutrophils, andplatelets, confirming the phenotypic heterogeneity of cyto-adherence. A number of studies have attempted to identifythe host ligands both in in vitro models of cytoadherenceand in vivo by immunocytochemical techniques.
Initially studies used endothelial cells and subsequently,the amelanotic C32 melanoma cell line as an in vitro modelfor cytoadherence (Sharma, 1991). Studies using mono-clonal antibodies to a variety of ligands established thatCD36 (formally platelet glycoprotein 4) was a potential en-dothelial cell ligand for PRBC. Subsequently, a variety ofother host molecules were also identified as potentialligands, including ICAM-1, VCAM, and E-selectin (Sec-
tion 4.4) (Turner, 1997). Some of these molecules havebeen assayed in heterologous expression systems and conferupon expressing cells the ability specifically to attach toPRBCs. Many of these potential ligands are inducible or areup-regulated when endothelial cells are exposed to appro-priate cytokine stimuli (Section 4.3). The importantligands in vivo in severe infection have only been studied ina small number of cases, primarily in adult patients, so thekey mediators of cytoadherence in African children dyingof severe malaria have yet to be identified.
5.2. Rosetting
Rosetting is the phenomenon observed when PRBCs con-taining relatively mature stages of parasites (those with pig-ment visible with light microscopy) become surroundedand bound to non-PRBCs (NPRBCs) (Udomsangpetch etal., 1989). Rosettes commonly consist of up to 10 NPRBCs,but may be much larger (“giant rosettes”). At first sight, theformation of rosettes is puzzling because it may competewith the process of cytoadherence, which sequesters para-sites from the circulation (indeed, in laboratory studies, it isnecessary to disrupt rosettes to measure binding to celllines). However, rosetting can also be viewed as a mecha-nism for increasing the chances of parasites multiplying bysurrounding them with NPRBCs for reinvasion in the nextreplicative cycle (Wahlgren et al., 1991). This view is notshared by all investigators (Pasvol et al., 1995).
Rosetting has many features in common with cytoadher-ence, such as the parasite-stage specificity of expression ofthe phenotype, dependency on divalent cations, and sensi-tivity to trypsin. There are, however, also important differ-ences, such as disruption of rosettes (but not of cytoadher-ence) by heparin and antibodies from patients with malariaand the lack of positive correlation between the two adhe-sive properties in parasitised erythrocytes obtained from pa-tients (Ho et al., 1991). Certain blood groups (A/AB orB/AB) favour rosetting over others (blood group O), andthis observation has been used to explain the relative pro-tection of patients with blood group O from CM. The dogmathat only sequestering species of malaria (P. falciparum,P. fragile, and P. chabaudi) form rosettes recently has beenchallenged by the observations that P. vivax and P. ovalecan also form rosettes (Angus et al., 1996; Udomsangpetchet al., 1995). Thus, the rosetting phenotype may be neces-sary, but is not sufficient, to cause severe malaria, and rela-tionship of this phenotype to cytoadherence is not clear.
In ex vivo assays, the mean number of parasites that formedrosettes was significantly higher in isolates from Gambianchildren with CM (n 5 48, 31.7%) compared with thosefrom uncomplicated malaria (11.4%, P , 0.00000001), andthe rosettes were much larger in the cerebral group (Treuti-ger et al., 1992). Rosetting was not related to parasite den-sity. Autologous (and some heterologous) testing of serasuggested that disruption of rosettes by sera from CM pa-tients was less efficient than sera from uncomplicated cases.In a smaller subset of isolates, no correlation was observed

14 C. R. J. C. Newton and S. Krishna
between disease severity and capacity to bind to melanomacells in vitro. Studies on adults in Thailand (Ho et al., 1991)and children in Papua New Guinea have not found similarrelationships between rosetting and disease severity (Al Ya-man et al., 1995). The Thai study observed an inverse cor-relation between rosetting frequency and cytoadherence toC32 melanoma cell lines, but may have been too small todetect a difference in rosetting between groups of differingdisease severity. In Papua New Guinea, although there wasno association with disease severity or inhibition of roset-ting by autologous sera in uncomplicated cases, an associa-tion between blood group AB and rosetting was observed(Al Yaman et al., 1995). Another study from Kenya hasconfirmed that increased rosetting is a feature of severe ma-laria and is underrepresented in patients with blood groupO (Rowe et al., 1995). Haemoglobinopathies, such as sicklecell disease and thalassaemia, may also impair rosettingability, the latter because of microcytosis (Carlson et al.,1994). A variety of sulphated glycoconjugates disrupt ro-settes with varying degrees of effectiveness dependent onthe parasite isolates tested (Rogerson et al., 1994). Roset-ting is resistant to metabolic inhibitors (Carlson, 1993).The identification of parasite-encoded molecules responsi-ble for rosetting, following the recent successes with theisolation of the var gene family, undoubtedly will help toclarify the sometimes conflicting experimental observationson this phenomenon. Both rosetting and cytoadherence al-ter the rheological characteristics of PRBC in laboratorymodels of flow (Kaul et al., 1991). These alterations are dis-cussed in the next section.
5.3. Rheology
Early studies of P. knowlesi PRBCs showed infection in-creased resistance to flow through 5-m polycarbonatesieves, and obstructed pores at high parasitaemia. Infectionwas also associated with a decrease in red cell deformability,and these changes were suggested to contribute to the de-velopment of microcirculatory obstruction (Miller et al.,1971). Subsequently, more sophisticated studies have con-firmed that there is a stage-dependent decrease in the de-formability of red cells as P. falciparum matures (Nash et al.,1989), and that mature parasites require correspondinglylarger pressures (4- to 6-fold, compared with controls) to al-low entry of PRBCs into small (3 m) capillaries. Thesechanges could reduce the circulatory flow in downstream(postcapillary) venules, and contribute to other pathophys-iologically important processes such as cytoadherence. Themolecular basis for adhesion at physiological flow rates hasalso been studied in cultured cell receptors (Wick andLouis, 1991; Nash et al., 1992), but relating changes ex vivoto patient’s clinical status is not straightforward (Cooke etal., 1993, 1995). Recently, reduction in red cell deformabil-ity assessed using ektacytometry has been shown to bestrongly associated with a fatal outcome in severe malaria(Dondorp et al., 1997).
6. CLINICALDEFINITIONS AND PRESENTATIONS6.1. Severe Malaria
The parasite and host features that determine why a childwho has been living in a malaria-endemic area and who islikely to have had extensive previous exposure to infectionprogresses to develop severe disease are still largely unde-fined. The clinical manifestations of severe malaria are de-termined by the degree of immunity in the affected child, aswell as genotypic predispositions. African children growingup in endemic areas are exposed to malaria from infancy,and in some areas, may receive up to 100 infected bites peryear (Mbogo et al., 1993). However, the relationship be-tween malaria transmission and severe disease is complex,and the manifestations of severe disease vary with region(Snow et al., 1997). Initially, the children are protected bymaternal factors (e.g., transplacental acquisition of mater-nal antibodies) and intrinsic factors (e.g., foetal haemoglo-bin). The protective effect of these factors, however, beginsto wane during the first 6 months, so that severe diseaseleading to death is maximal between the ages of 1 and 4years and is more likely in younger children. Thereafter, thechildren acquire immunity, so that adults who have livedcontinuously in endemic areas rarely develop severe dis-ease. In contrast, children and adults who have not beenexposed to malaria previously can rapidly develop severedisease after exposure.
Severe malaria is a spectrum of clinical syndromes uni-fied by the single causative organism P. falciparum. It can beoperationally defined as any malaria syndrome that is asso-ciated with a high mortality (.5%), even after appropriatehospital treatment. The clinical spectrum of severe malaria isdifferent in African children growing up in malaria-endemicareas compared with nonimmune adults (Table 1). The rea-sons for these differences are not clear, although they appearto be related to exposure to malaria rather than age, sincenonimmune children have similar features to nonimmuneadults. The clinical picture, however, is changing, as inSoutheast Asia jaundice is seen less frequently (Lalloo etal., 1996). This review largely concentrates on the clinicalpicture of African children since most of the recent workhas been conducted on this group, who bear the brunt of thedisease worldwide. Two studies have reported the admission ofchildren to units in North America, but the number of chil-dren with severe disease was too small to make meaningfulcomparisons (McCaslin et al., 1994; Lynk and Gold, 1989).
In African children, the commonest presenting syn-dromes associated with significant mortality are CM; recur-rent convulsions; metabolic dysfunction, which manifestsitself as hypoglycaemia or lactic acidosis; or symptomaticanaemia. Children with the greatest risk of mortality can beidentified as those with impaired consciousness or respira-tory distress. Although severe anaemia is a common causeof admission, if blood transfusions are given quickly tothose with cardiorespiratory distress, the mortality is low(Fig. 4). The age distribution of these syndromes is differ-

Pathophysiology and Supportive Treatment of Severe Malaria 15
ent, so that severe anaemia affects younger children thanCM, with respiratory distress overlapping both syndromes(Fig. 5). These syndromes are discussed in greater detail inSections 6.2–6.4.
Children who present with severe malaria often have rel-atively short histories of illness, emphasising the rapiditywith which illness may progress. Parents accompanyingtheir children to hospital typically report fever beginning1–3 days prior to admission, with neurological manifesta-tions often beginning within 12 hr of admission (Musoke,1966; Schmutzhard and Gerstenbrand, 1984; Waller et al.,1995; Gordeuk et al., 1992; Molyneux et al., 1989b). Chil-dren with severe anaemia may present with longer histories,although acute decompensation, manifesting as respiratorydistress, often precipitates admission to hospital. Mostdeaths from severe malaria occur within 24 hr of startingtreatment (Waller et al., 1995; Krishna et al., 1994b;Walker et al., 1992; Newton et al., 1991a; Marsh et al.,1995; Molyneux et al., 1989b) (Fig. 6), and most of thosewho survive make full recoveries within 48 hr of startingtreatment (Krishna et al., 1994b; Waller et al., 1995;Walker et al., 1992; Gordeuk et al., 1992; Molyneux et al.,1989b).
The syndrome of CM is clinically discrete and relativelyeasily identified and, therefore, has been the subject of mostof the published studies on severe malaria. However, it isimportant to appreciate that CM is one of the commonestmanifestations of severe disease, but that severe malaria isnot synonymous with CM. It is only within the past fewyears that metabolic derangements have been identifiedand subsequently incorporated into the definition of severedisease. Clinical syndromes of severe malaria exhibit signif-
icant overlap (Fig. 4), and CM is frequently complicated bylactic acidosis and/or hypoglycaemia. In cases where lactatelevels or acid-base status cannot be assessed, clinical signsof respiratory distress suggest severe disease and are oftenassociated with underlying acidosis. These clinical corre-
TABLE 1. WHO Criteria for Severe Falciparum Malaria: Comparison of African Children and Papua New Guinean Adults Admitted to Hospital
African children(Marsh et al., 1995)
Nonimmune adults(Lalloo et al., 1996)
Prevalence Mortality Prevalence Mortality
Defining criteriaComa 10.0 16.8 17.1 41.7Severe anaemia 17.6 4.7 10 0Respiratory distress 13.7 13.9 — —Hypoglycaemia 13.2 21.7 5.7 75Circulatory collapse 0.4 71.4 0 —Renal failure 0.1 0 22.9 37.5Spontaneous bleeding 0.1 0 0.1 100Haemoglobinaemia 0.1 50.0 0.1 0Acidosis 63.6 21.4 NA NARepeated convulsions 18.3 6.8 0.3 0
Supporting criteriaImpaired consciousness 8.2 6.0 37.1 11.5Jaundice 4.7 11.9 45.7 25Prostration 12.2 5.2 — —Hyperpyrexia 10.6 1.6 20 7.1Hyperparasitaemia 8.9 4.3 40 28.6
NA, not applicable.
FIGURE 4. Prevalence, overlap, and mortality for the majorclinical syndromes of severe malaria in 1844 children present-ing to Kilifi District Hospital, Kenya. Mortality is given as apercentage of the total number. Adapted from Marsh et al.(1995), with permission of the copyright holder, MassachusettsMedical Society, Boston.

16 C. R. J. C. Newton and S. Krishna
lates of severe malaria have been recognised for decades(Guignard, 1965), although they have been more formallyassessed recently (Waller et al., 1995; Marsh et al., 1995).
Multi-organ involvement is relatively uncommon inchildren compared with adults with severe disease. In ourexperience, none have required renal replacement therapyfor significant impairment, and severe jaundice is uncom-mon unless it is associated with haemolysis. Pulmonary in-volvement has not been studied in detail in children, and thedistinction between secondary infection and oedema requiresmore detailed examination. In a study of 180 children, 25of whom died of severe malaria, the principal clinical causesof death were identified and summarised in Fig. 7.
Recognition of severe malaria is, therefore, of paramountimportance in determining subsequent management deci-sions such as the use of a loading dose of quinine and thefrequency of post-admission monitoring for complications
such as hypoglycaemia. Whilst there is no single clinical orlaboratory marker that adequately identifies all patientswith severe disease, most high-risk patients are identifiedusing a combination of clinical and laboratory criteria.These criteria are summarised in the following sections.
6.2. Cerebral Malaria
CM is a syndrome of impairment of consciousness associ-ated with a falciparum malaria infection. Impairment ofconsciousness caused by other species of malaria have beendescribed, but in these case reports, other causes of an en-cephalopathy have not been excluded and rigorous post-mortem studies are lacking.
6.2.1. Definition of cerebral malaria. There are no patho-gnomonic pathological features that differentiate CM from
FIGURE 5. Ages of 1844 Ken-yan children admitted with CM,respiratory distress, and severeanaemia to Kilifi District Hos-pital, Kenya. Data from Marshet al. (1995).
FIGURE6. Cumulative percen-tage survival of 2155 childrenadmitted to three African hospi-tals with severe falciparummalaria (Molyneux et al., 1989b;Marsh et al., 1995; Waller etal., 1995).

Pathophysiology and Supportive Treatment of Severe Malaria 17
NCM (Section 3). Furthermore, consciousness can be de-pressed by a variety of pathophysiological processes, includ-ing seizures [either nonconvulsive status or post-ictal states(Crawley et al., 1996; Kirkham, 1991)], metabolic derange-ments [e.g., severe acidosis (Allen et al., 1996a)], and bythe systemic effects of the infection [e.g., fever or hy-ponatraemia (Arieff and Griggs, 1994)]. To exclude sys-temic causes of impaired consciousness and make studies ofCM comparable, Warrell and colleagues (1982a) originallyproposed a strict definition of CM based upon the responseto a painful stimulus. This definition, slightly modified by apanel of experts at the World Health Organisation (WHO)(Warrell et al., 1990), is now widely accepted.
CM exists in a patient who:
• is unable to localise a painful stimulus• has peripheral asexual falciparum parasitaemia• has no other causes of an encephalopathy
The inability to localise a painful stimulus was chosen fortwo reasons. First, because it is associated with sufficientlydeep coma as to exclude systemic effects of infection, andsecond, because it is a sign that can be reliably elicited(Newton et al., 1997a). Lesser degrees of CNS dysfunction(confusion, stupor) are frequently caused by falciparum in-fection and should also be managed as severe malaria. Toexclude patients with uncomplicated falciparum infectionand a complicating febrile seizure who are unrousable post-ictally, the child should be reassessed at least 30 min after aseizure. Warrell and colleagues originally stipulated thatthis assessment period should be after 6 hr, based on experi-ence with adults, but this has now been shortened to 30min since children often regain consciousness after febrileseizures within this time (Warrell, 1989). Our own observa-tions also suggest that recovery 30 min following a febrile
seizure is common, but children with malaria often have aprolonged post-ictal state after long or multiple seizures(Crawley et al., 1996). More than one seizure in a child withfalciparum infection is indicative of significant cerebral in-volvement, as these children frequently progress to coma.
Asexual falciparum parasitaemia is a sine qua non of se-vere infection, since the liver stages and gametocytes donot contribute to symptoms. However, this definition doesnot include cases of blood slide-negative CM (Walker etal., 1992; Gopinathan and Subramanian, 1986; Edingtonand Gilles, 1976), i.e., malaria patients who have profoundCNS disturbance, without asexual parasites detectable inthe peripheral blood, but sequestered parasites found in thebrain at post-mortem. The commonest cause of slide-nega-tive falciparum malaria is pretreatment with antimalarials(White et al., 1992b), which remove circulating evidenceof infection, but not the parasites sequestered in tissues. Inthese cases, the diagnosis may be suspected by rapid re-sponse to continuing antimalarial therapy, although this isrelatively imprecise, or confirmed by finding sequesteredparasites in the brain at post-mortem. It is likely that as theuse of artemisinin derivatives becomes more widespread,slide-negative malaria will be observed more commonly, sincethis class of antimalarial clears circulating parasites rapidly.
Since a considerable proportion (up to 90%) of childrenliving in endemic areas are infected with P. falciparum, butare asymptomatic, children admitted with other encephalo-pathies, which require exclusion (e.g., encephalitis or Reye’ssyndrome), may have a concomitant peripheral parasi-taemia and thus, be misdiagnosed as having CM. This hasled to inclusion of quantitative assessment of parasitaemiato establish the probability of malaria as a cause of symp-toms in a patient. The parasitaemia cutoffs that have beenused range from 2000 to 20,000/mL, depending on the geo-graphical area and the criteria used for establishing positivepredictive values for infection. However, most of thesestudies are community-based case-control studies and,therefore, are inapplicable to children who present to hos-pital with signs of moderate or severe malaria (as opposedto children presenting with uncomplicated infection). Thismay be particularly important in complicated falciparummalaria when a low peripheral parasite count may not re-flect the parasites sequestered in the deep vascular beds.Thus, the absolute parasitaemia per se is not particularlyuseful in discriminating severe from uncomplicated or mod-erate malaria, and any patient who presents with symptomsof severe disease and the presence of asexual P. falciparumparasitaemia, therefore, must be managed as a case of severemalaria. The stages of parasite development on a peripheralblood film may be a more important parameter to assess insevere infections (Cropper, 1908). The importance of de-tecting these mature stages recently has been emphasisedby studies that show that .20% mature stages in the pres-ence of a high parasitaemia (pigmented trophozoites orlater) is associated with a significantly higher mortalitythan patients who do not have such a high proportion oflate stages (Silamut and White, 1993).
FIGURE 7. Causes of death in 25 Gambian children withsevere malaria. The causes of death were classified according tothe following criteria: CM, highest BCS <2, no biochemicalevidence of lactic acidosis, pulmonary complications, or sepsis;lactic acidosis, plasma lactate >5 mmol/L, BCS .2 after admis-sion, and no evidence of pulmonary complications or sepsis; pul-monary complications, chest examination revealed signscompatible with infection or oedema; sepsis, proven by bloodculture. Reproduced from Waller et al. (1995), with permissionof the copyright holder, University of Chicago Press, Chicago.

18 C. R. J. C. Newton and S. Krishna
The exclusion of other causes of coma is determined by acareful history and by the available investigative facilities.In most hospitals in malaria-endemic areas, this entails theexclusion of other CNS infections (by obtaining clear andculture-negative CSF) and hypoglycaemia (either by per-forming a blood glucose estimation or observing the clinicalresponse to glucose administration). The CSF needs to beexamined in all children presenting with CM, since thiscondition cannot be differentiated clinically from bacterialmeningitis (Wright et al., 1993), but the timing of the lum-bar puncture is controversial (Greenwood, 1991; White,1991; Kirkham et al., 1991; Kwiatkowski et al., 1991;Coulter, 1991). If examination is delayed or not possible,then children should empirically be managed with both an-timalarial and antibacterial therapy (to cover the possibilityof meningitis) and the diagnosis confirmed when permissi-ble. Drug toxicity may confuse the clinical picture of CM ,but clearly the presence of parasites dictates immediate an-timalarial treatment. Other causes of encephalopathy, e.g.,encephalitis without a pleocytosis or Reye’s syndrome, can-not be confidently excluded.
6.2.2. Coma scores. The inability to localise a painfulstimulus identifies patients who are deeply unconscious, butnot those with more subtle neurological impairments. Asummated Glasgow coma score less than 8 (Table 2) hasbeen proposed as part of the definition of CM, instead ofthe inability to localise pain (Leaver et al., 1990). How-ever, this criterion is not applicable to children since chil-dren do not have the same range of summated scores (New-ton et al., 1990) and thus, it has not been widely accepted.Molyneux and Taylor developed the Blantyre coma score(BCS) for the assessment of young Malawian children withCM (Molyneux et al., 1989b). The BCS is based upon theGlasgow coma scale (Table 2), but measures different re-sponses. In particular, the eye responses do not take intoconsideration that some children may be blind and that di-rected eye responses can be caused by primitive subcortical
reflexes (Plum and Posner, 1980) or seizures (Crawley et al.,1996). Likewise, withdrawal from a painful stimulus may bea spinal reflex requiring little cortical involvement andthus, is not a useful sign in assessing the depth of coma. Fur-thermore, there are considerable differences between clini-cians in assessing this scale, particularly the verbal compo-nent, which will limit its use (Newton et al., 1997a).Despite these reservations, however, this scale appears toassess the overall degree of compromise due to falciparummalaria, and can be used to predict mortality, rather thanthe neurological complications (Newton et al., 1997a). TheBCS is used by many researchers who define CM in chil-dren as a summated score of 2 or less: a total that is mostlyderived from a motor and verbal score of 1 each and thus, isequivalent to the strict WHO definition. Other researchersinclude children with scores of 4 or less to define CM; how-ever, this score would not exclude systemic effects and isnot directly comparable with the strict WHO definition.
These definitions do not account for the fact that veryyoung children may not have acquired the ability to loca-lise pain and thus, may not satisfy the formal definition forcoma, but nonetheless may be comatose. Thus, the defini-tion of CM should be restricted to children over 8 months,until more appropriate criteria are found for younger chil-dren (Newton et al., 1997a). Overall, the WHO criteria of-fer a pragmatic definition that can be used for research andin the management of children older than 8 months. Comascores may be useful in categorising the severity of CM, buttheir use as a criterion for diagnosis needs to be consideredcarefully.
6.2.3. Clinical presentation of cerebral malaria in Africanchildren. The clinical presentation of CM has features of adiffuse metabolic encephalopathy, as described by Plum andPosner (1980). The pathological basis of this picture hasbeen discussed in Section 3 and its pathophysiology is dis-cussed in Section 7.
TABLE 2. Blantyre and Glasgow Coma Scales
Blantyre coma scale (Molyneux et al., 1989a)
Glasgow coma scale (Teasdale and Jennett, 1974)
Verbal 2. Appropriate cry 5. Able to give name and age1. Inappropriate cry or moan 4. Recognisable and relevant words0. No cry 3. Incomprehensible, but complex vocalisation
2. Cry or grunt1. No response
Motor 2. Localises pain 6. Obeys commands1. Withdrawal from pain 5. Localises pain0. Nonspecific or no response to pain 4. Withdrawal from pain
3. Flexes to pain2. Extends to pain1. No response
Eye 1. Directed eye movements 4. Spontaneous eye opening0. Not directed 3. Opens eyes to voice
2. Opens eyes to pain1. No eye opening

Pathophysiology and Supportive Treatment of Severe Malaria 19
African children usually present in coma with an almostinvariable 2- to 3-day history of fever (Rey et al., 1966;Molyneux et al., 1989b; Maguire, 1983; Ikpatt et al., 1990;Commey et al., 1980). Alterations in conscious level rangefrom drowsiness and/or convulsions to deep coma andbrainstem abnormalities (Musoke, 1966; Schmutzhard andGerstenbrand, 1984; Waller et al., 1995; Newton et al.,1991a; Walker et al., 1992; Molyneux et al., 1989b). Fiftyto 80% of children have a history of convulsions (Schmutz-hard and Gerstenbrand, 1984; Molyneux et al., 1989b;Maguire, 1983; Ikpatt et al., 1990; Commey et al., 1980),one of which often precipitates coma (White and Looaree-suwan, 1987; Warrell et al., 1990; Edington and Gilles,1976). Seizures are witnessed at presentation in up to 50–80% of African children with CM (Table 3). If seizures per-sist after admission and particularly if they are prolonged orresistant to anticonvulsants, they are associated with thedevelopment of neurological sequelae (Bondi, 1992) ordeath (Kirkham et al., 1994; Brewster et al., 1990; Moly-neux et al., 1989b). Occasionally, we have also observedboth children and adults presenting with bizarre behaviouraldisturbances, such as confusion, clouding of consciousness,and stereotyped behaviour, such as tongue protrusion. Of-ten, these symptoms progress rapidly to coma, soon afterthe initiation of antimalarial therapy.
Children with CM frequently develop abnormal postures(decorticate rigidity, decerebrate rigidity, opisthotonos),pupillary changes, absent corneal reflexes, abnormal respi-ratory rhythms (Kussmaul, Cheyne-Stokes, periodic ap-noea), and gaze abnormalities (eyes wide open, conjugategaze deviation, nystagmus) (Newton et al., 1998). Signs offrontal lobe release are often seen. Other brainstem signs,including dysconjugate and conjugate eye signs, and decer-ebrate posturing movements (all of which may representseizure activity), occur in about one-third of children(Schmutzhard and Gerstenbrand, 1984; Molyneux et al.,1989b; Gelfand, 1973). Retinal haemorrhages are presentin 6–36% of African children during admission (Newton etal., 1991b; Molyneux et al., 1989b; Kayembe et al., 1980).Haemorrhages are associated with a high mortality in adults(Looareesuwan et al., 1983), but in children, they do not ap-pear to have prognostic significance (Kayembe et al., 1980).In both groups, they resolve without long-term visual de-fects (Kayembe et al., 1980; Bell et al., 1976). Papilloedemais present in between 2 and 12.5% of children (Newton etal., 1991a; Molyneux et al., 1989a; Kayembe et al., 1980),and was associated with increased opening pressures onCSF examination (Lewallen et al., 1993). Papilloedema andretinal oedema outside the vascular arcades were both inde-pendent indicators of fatal outcome in children.
CSF examination is useful not only in excluding infec-tions that may mimic CM, but also in providing measure-ments of CSF lactate concentrations, which are one of thebest independent prognostic indicators of fatality (Krishnaet al., 1994b; White et al., 1985, 1987a). In children, CSFlactate (and glucose) concentrations are correlated withplasma levels, are not associated with a history of convul-
sions, and concentrations of lactate .4.5 mmol/L predict aparticularly high mortality. In comparison with acute bac-terial meningitis, the CSF glucose concentration is higherand the protein lower (Table 4). The CSF in CM should beclear (no more than 100 lymphocytes/mm3) and 25% haveelevated protein levels. There are no elevations in CSF cre-atinine phosphokinase levels in cerebral disease (Miller etal., 1989b). These findings are discussed more fully in Sec-tion 4.5.
In African research settings, the mortality rate for strictlydefined CM is 18.6% (95% CI 16.3–21.0) (see Table 3).There are no series large enough to give a true estimate ofmortality in children treated in developed countries.
6.2.4. Neurological sequelae. Neurological damage hasonly been recently recognised as a common sequela of CMin African children (Brewster et al., 1990). In nonimmuneadults, neurological sequelae are uncommon, although avariety of postmalarial syndromes have been described(Newton and Warrell, 1998). Although most neurologicalsequelae follow an episode of CM, neurological deficits canbe found in children with seizures without sustained loss ofconsciousness (C. R. J. C. Newton, personal observation).The studies of neurological sequelae are often difficult tointerpret since the definition of the severe falciparum ma-laria, the thoroughness of the examinations, and the extentof follow-up varies considerably, so that the incidence alsovaries considerably (Table 5). Recent studies of Africanchildren with CM (van Hensbroek et al., 1996a; Marsh etal., 1995; Bondi, 1992; Brewster et al., 1990; Molyneux etal., 1989a), which used similar criteria for the definition ofCM, report an incidence of neurological sequelae rate to be10.9% (95% CI 8.3–13.5% of survivors).
6.2.4.1. Factors predisposing to sequelae. In African chil-dren, the development of sequelae is associated with pro-tracted seizures (van Hensbroek et al., 1996a; Brewster etal., 1990; Bondi, 1992), deep coma (van Hensbroek et al.,1997), prolonged coma (Sanohko et al., 1968; Brewster etal., 1990; Bondi, 1992; van Hensbroek et al., 1997), andanaemia in some studies (Brewster et al., 1990), but not inothers (Bondi, 1992). Other smaller studies have shown anassociation between the development of sequelae andpathophysiological processes such as raised ICP (Newton etal., 1997b). Most of these factors are also associated withdeath, and may simply reflect the severity of the underlyinginsult, rather than a specific neuropathogenic process. Thediverse pattern of neurological damage detected clinicallyand by CT suggests that there are likely to be a variety,probably interacting, of mechanisms responsible for neuro-logical damage.
6.2.4.2. Patterns of sequelae. In the studies of Africanchildren, there is a difference between the sequelae foundon discharge and those that persist (Table 5). About 50–84% of children recovered completely, usually within thefirst 6 months after discharge, and 9–55% had recovered 18months after discharge, although this may be an overesti-

20 C. R. J. C. Newton and S. Krishna
TA
BL
E3.
Sum
mar
y of
Fea
ture
s of
CM
in C
hild
ren
Aut
hor,
yea
rC
ount
ryN
umbe
rof
cas
esM
ean
age
(yea
rs)
Hyp
ogly
caem
ia(%
)P
aras
ite
coun
t(/
mL
)Se
izur
es(%
)T
reat
men
tM
ean
dura
tion
of c
oma
(hr)
Neu
rolo
gica
lse
quel
ae (
%)
Mor
talit
y(%
)M
orta
lity
,24
hr
(%)
Rot
he, 1
956
Ken
ya97
Q, C
22A
rmen
gaud
et a
l., 1
962
Sene
gal
88Q
or C
1425
Gui
gnar
d, 1
965
Mad
agas
car
6077
C0
38R
ey e
t al.,
196
6Se
nega
l22
74.
365
Q31
Mus
oke,
196
6U
gand
a20
C34
530
83Sa
nohk
o et
al.,
196
8Se
nega
l34
3Q
/C21
9Le
mer
cier
et a
l., 1
969
Sene
gal
235
3Q
/C5
9B
erne
r, 19
75M
alaw
i39
2C
328
Om
anga
et a
l., 1
977
Zair
e12
13.
787
C1
Q3
440
Com
mey
et a
l., 1
980
Gha
na43
4.5
100
C36
55
Stac
e et
al.,
198
2PN
G68
5.1
Q4
6Sc
hmut
zhar
d an
d G
erst
enbr
and,
198
4T
anza
nia
6695
C17
18A
hmad
and
Riv
er, 1
986
Indi
a30
7C
,24
320
Ber
nadi
no e
t al.,
198
6A
ngol
a25
43
3500
20Q
/C27
Tra
pe e
t al.,
198
7C
ongo
140
2864
Tha
pa e
t al.,
198
8In
dia
4060
Q1
C0
33T
aylo
r et a
l., 1
988
Mal
awi
953.
320
250,
000
78Q
3611
11M
olyn
eux
et a
l., 1
989b
Mal
awi
131
3.6
3714
7,91
0–22
9,08
782
Q31
915
70G
rau
et a
l., 1
989
Mal
awi
555.
318
273,
400
95Q
204
18B
rew
ster
et a
l., 1
990
The
Gam
bia
377
1815
C9
16Ik
patt
et a
l., 1
990
Nig
eria
754.
857
C/Q
020
Kaw
o et
al.,
199
0T
anza
nia
110
3.8
210,
000
C13
2567
Car
lson
et a
l., 1
990
The
Gam
bia
361.
811
19,9
60Q
030
Kw
iatk
owsk
i et a
l., 1
990
The
Gam
bia
24C
25N
eequ
aye
et a
l., 1
991
Gha
na11
35
275
C34
84
New
ton
et a
l., 1
991a
Ken
ya61
3.25
2884
Q20
100
Pasv
ol e
t al.,
199
1K
enya
493.
46
297,
000
94Q
1510
16W
olf-
Gou
ld e
t al.,
199
1G
hana
204.
8C
10G
orde
uk e
t al.,
199
2Za
mbi
a83
2.8
45,0
0081
Q68
219
Wal
ker e
t al.,
199
2N
iger
ia61
5.7
2693
C51
1618
7B
ondi
, 199
2N
iger
ia78
5.2
2367
C68
1421
Tay
lor e
t al.,
199
3M
alaw
i65
2.8
1515
8,48
988
Q o
r AM
14(Q
), 8
(AM
)11
11C
arm
e et
al.,
199
3C
ongo
170
Q9
1564
Wal
ker e
t al.,
199
3N
iger
ia25
3A
M40
.112
1229
3Q
36.7
721
Wri
ght e
t al.,
199
3Li
beri
a97
266
Q16
Kw
iatk
owsk
i et a
l., 1
993
The
Gam
bia
414
740
,000
C24
1229
58A
kped
e et
al.,
199
3N
iger
ia31
3.3
22.6

Pathophysiology and Supportive Treatment of Severe Malaria 21N
ewto
n et
al.,
199
4K
enya
143.
228
1200
–1,1
08,8
0093
Q o
r AM
.11
129
0So
lom
on e
t al.,
199
4M
ozam
biqu
e19
2.9
2617
,400
84Q
1110
0W
atta
nago
on et
al.,
199
4T
haila
nd96
6.5
55Q
22D
elor
on e
t al.,
199
4B
urun
di31
28.6
11,9
20Q
22O
lum
ese
et a
l., 1
995
Nig
eria
2411
,379
RD
4667
8974
NR
D12
Mar
sh e
t al.,
199
5K
enya
185
16.8
di P
erri
et a
l., 1
995
Bur
undi
305.
126
.673
.3Q
468
16.7
265.
626
.965
.4Q
1P
67.
70
Bro
wn,
199
5PN
G17
50
88Q
618
Mab
eza
et a
l., 1
995
Zam
bia
129
2.9
1368
,700
93va
n H
ensb
roek
, 199
6T
he G
ambi
a28
83.
822
.355
,471
28.1
Q20
225
.221
.5z
7028
84
26.3
57,1
0638
.5A
M26
221
20.5
z70
Alle
n et
al.,
199
6bPN
G75
3.7
1067
6053
Q6.
18.
583
n 5
4677
3319
2079
1709
3133
1401
3199
4439
Wei
ghte
d m
ean
53.
819
.939
,198
156
.832
.310
.918
.6W
eigh
ted
95%
CI
3.5–
4.2
16.1
–23.
618
,857
–81,
486
46.1
–67.
423
.4–4
1.1
8.3–
13.5
16.3
–21
1G
eom
etri
c m
ean.
2P
5 0
.046
. C
alcu
lati
ons o
f wei
ghte
d m
eans
and
con
fiden
ce in
terv
als w
ere
carr
ied
out i
n ST
AT
A w
itho
ut in
clud
ing
rang
es.
C, c
hlor
oqui
ne; Q
, qui
nine
; AM
, art
emet
her;
PNG
, Pap
ua N
ew G
uine
a; R
D, r
espi
rato
ry d
istr
ess;
NR
D, n
o re
spir
ator
y di
stre
ss; P
, pen
toxi
fylli
ne.
Mod
ified
from
Wal
ler e
t al.
(199
5).

22 C. R. J. C. Newton and S. Krishna
mate, since the follow-up was incomplete in some of thesestudies and children with severe sequelae often die at homefrom an intercurrent illness. Other sequelae, e.g., epilepsyor behavioural difficulties, may develop after discharge andpersist. However, some children with major sequelaeshowed dramatic resolution, particularly if they had corticalblindness.
Ataxia, common on discharge, rapidly improves over aperiod of weeks. The cause of the ataxia is not clear, sincemost children do not have the features of cerebellar in-volvement. It may be caused by muscle weakness followingdamage by cytokines, depletion of glycogen, or even para-site sequestration in the muscles (Miller et al., 1989b).
Although clearly definable neurological deficits are nowwell recognised, the importance of more subtle defects,manifesting as speech and behavioural difficulties, is be-coming increasingly recognised. Psychoses with visual andauditory hallucinations have been reported in some African
children (Sowunmi, 1993). The incidence of cognitive im-pairments is also not known. A case control study of 36Gambian children who recovered from CM without anyneurological deficits showed that cases may have had im-paired balance, but there were no significant impairmentsof memory, perception, reasoning, learning, visiomotor co-ordination, dexterity, or manual speed (Muntendam et al.,1996). This study, however, only compared the results ofsingle test scores that have a large standard deviation andthus, are unlikely to detect significant differences (and,therefore, subject to Type II error). Furthermore, there wereno tests of long-term memory, and language was not ade-quately measured. Recent studies from Kenya suggest thatchildren have difficulties in attention, expressive language,and behaviour following CM.
The pattern of neurological sequelae in adults is differentfrom children (Newton and Warrell, 1998). There are nostudies of nonimmune children, but they may have similar
TABLE 4. CSF Findings in CM and Acute Bacterial Meningitis
CM(White et al., 1987a; Newton, 1995)
Acute bacterial meningitis(Eross et al., 1981; Bonadio, 1992)
Appearance Clear CloudyWhite cell count (3109/L) ,1001 .100
neutrophils .1 3 109/L NR 99%Opening CSF pressure (mm Hg) 1.8–7.1 15 (4–70)Glucose (mmol/L) 2.0–5.6 ,1–3.8
,2.2 mmol/L 8% 81%Lactate (mmol/L) 2.4–.10 3.9–.10.0Protein (g/L) 0.39 (0–4.0) 1.3–3.0
.0.45 g/L 25% 60%
1CM is usually defined as ,10 white blood cells.NR, not reported.
TABLE 5. Incidence and Pattern of Neurological Sequelae Following CM
Malawi(Molyneux
et al., 1989b)
Gambia(Brewster
et al., 1990)Nigeria
(Bondi, 1992)
Kenya (Murphy
et al., 1996)1
Gambia (van Hensbroek,
1997)2 Total
Number studied 131 308 72 160 6243 1295Survivors 111 265 62 134 490 1062Sequelae/number followed up (%) 12 (11%) 35 (13%) 11 (18%)Sequelae detected 1 month after discharge 7 (6%) — — 13 (10%) 114 (24%)Persistent sequelae NR 11/23 NR 20/452Duration of follow-up NR 6 months 12–16 months NR 18 monthsAtaxia 3 6 [NR] NR 3 13 [3] 25/1000Monoparesis/hemiparesis 4 23 [6] 4 [2] 3 11 [4] 44/1066Severe deficit 5 9 [2] 1 [1] 5 NR 20/578Hearing impairment NR NR 2 [1] 6 5 [3] 13/666Visual impairment NR 11 [2] 3 [0] 5 3 [2] 22/931Dyphasia/dysarthria NR 9 [2] 3 [0] 7 7 [4] 20/931Behavioural difficulties NR 2 [NR] NR 1 8 [4] 11/865Cognitive deficit NR NR 1 [1] 4 4 [3] 9/931Epilepsy NR NR [3] 1 [1] NR
5 [1]6/797
1Examined 7 days after discharge.2Sequelae assessed 1 month after discharge.3Two patients were re-admitted (with convulsions and parasitaemia) within 48 hr of initial discharge.NR, not reported; [ ], persistent sequelae.

Pathophysiology and Supportive Treatment of Severe Malaria 23
patterns of damage as the adults. In adults, sequelae are notconfined to CM, but are often associated with laboratoryevidence of severe disease. The major deficits are isolatedcranial nerve lesions, mononeuritis multiplex, polyneurop-athy, extrapyramidal tremor, and other cerebellar signs (deSilva et al., 1992; White and Looareesuwan, 1987). Someadults have transient psychosis or delirium during recovery,whilst others develop focal epilepsy, sometimes associatedwith transient tomographic opacities in the brain (Looaree-suwan et al., 1983). More recently, a postmalarial syn-drome, consisting of confusion, convulsions, and tremor,associated strongly with mefloquine treatment in SoutheastAsia has been described (Nguyen et al., 1996).
6.3. Metabolic Abnormalities in Severe Malaria
Hypoglycaemia and lactic acidosis both frequently co-existand are also complications of CM (Krishna et al., 1994b).There are few clinical features that distinguish hypoglycae-mia from other manifestations of malaria, since conven-tional signs, such as decreased consciousness level, sweat-ing, pupillary dilatation, tachycardia, and seizures, arecommon to both CM and hypoglycaemia. Hypoglycaemia(defined as blood or plasma glucose ,2.2 mmol/L), there-fore, should be suspected in all patients who look severelyill, and rapidly excluded using bedside tests such as the BM-stix™ (a colorimetric assay for blood glucose that relies onglucose oxidase). Unfortunately, BMstix™ are not alwaysavailable and are relatively expensive (although their cost-effectiveness can be enhanced by longitudinally cuttingthem into 2 or 3 strips). If diagnosis of hypoglycaemia is un-confirmed or likely to be delayed more than a few minutes,then empirical administration of hypertonic glucose (1 mL/kg, 50% glucose) is indicated. The majority of patients willnot improve dramatically after correction of hypoglycae-mia, indicating that hypoglycaemia is not the main cause ofsymptoms such as coma.
Lactic acidosis (defined as blood or plasma lactate >5mmol/L) may be equally difficult to recognise clinically. Itshould be suspected in any severely ill patient who hasmarkedly abnormal respiratory patterns, such as tachypnoea(.50 respirations/min in children), deep gasping respira-tions, or the use of secondary muscles of respiration (Marshet al., 1995; Krishna et al., 1994b). In Kenyan children,“respiratory distress” was defined as alar flaring, chest reces-sion (intercostal or subcostal), the use of accessory muscles ofrespiration, or abnormally deep (acidotic) breathing, whilst“severe respiratory distress” was used for children with chestrecession or abnormally deep breathing (Marsh et al., 1995).In this study, respiratory distress was observed in 7% of1844 children admitted with malaria to a district hospital.Half were fully conscious, 19% died (13.9% died with anysymptom of respiratory distress and 24.8% with severe res-piratory distress). In the children with respiratory distress inwhom plasma bicarbonate was measured, 81% were severelyacidotic (plasma bicarbonate concentration ,15 mmol/L).Respiratory distress was not associated with abnormal pul-
monary auscultatory or chest X-ray findings and thus, isprobably a manifestation of a systemic acidosis. Similarconclusions also apply to Gambian children with hyperp-nea, where acidosis is an underlying identifiable cause inz70% (van Hensbroek, 1996). A study of 24 Nigerian chil-dren also identified respiratory distress as a poor prognosticindicator, but a high proportion of children (37.5%) hadcoarse crepitations on auscultation (Olumese et al., 1995).
In nonimmune adults with uncomplicated falciparummalaria, pulmonary involvement, which is mild and asymp-tomatic, is frequent and disappears when the malaria istreated (Gozal, 1992). Community-based studies haveshown that malaria may be associated with interstitial shad-owing on a chest X-ray, independent of lower respiratorytract infections (Byass et al., 1991), although oxygen desat-uration is not a feature of severe malaria in hospitalisedchildren with respiratory symptoms (Taylor et al., 1988).The clinical differentiation of pneumonia- and malaria-associated respiratory abnormalities can be difficult (O’Demp-sey et al., 1993). Also, the nomenclature of the “respiratorysyndrome” is debatable, as respiratory distress suggests aprimary pulmonary pathology, rather than the underlyingacidosis. Hyperpnoea (defined as an increase in depth andrate of breathing) may be more appropriate as it does notpresuppose the underlying cause(s) (Newton et al., 1998).
There are no rapid simple laboratory methods to confirmlactic acidosis when it is suspected on clinical grounds, anddiagnosis currently relies on dedicated equipment that isexpensive. However, manufacturers are developing simplermethods equivalent to the BMstix™ for glucose estima-tions, and these will prove particularly useful in the identi-fication of patients at risk of death with severe malaria. Of avariety of admission clinical and laboratory parameters as-sessed by logistic regression analysis in a Gambian study of115 children with severe malaria, deep coma and the lac-tate/glucose ratio were independently found to be predic-tive of mortality. Figure 8 shows the relationship amonghypoglycaemia, hyperlactataemia, and mortality in thesepatients.
When all clinical and laboratory variables were exam-ined together in a regression model, sustained hyperlacta-taemia (>5 mmol/L 4 hr after admission) proved to be thesingle most sensitive indicator of a fatal outcome, followedby the BCS at 4 hr and presence of hypoglycaemia on ad-mission (Krishna et al., 1994b). In many children, hyper-lactataemia resolves soon after admission, resuscitation,and the start of antimalarial treatment. In a proportion ofchildren, hyperlactataemia remains even after vigorous at-tempts at resuscitation, correction of electrolyte abnormali-ties, and hypoglycaemia (English et al., 1996c; Krishna etal., 1994b). The severity of lactic acidosis in this latter groupis clearly much greater than in children who recover quickly.This is reflected in blood gas measurements made in Malaw-ian children who presented with severe malaria (Taylor etal., 1993). Sustained acidaemia was the most specific indi-cator of a poor prognosis in this group of children, againsuggesting that the buffering capacity of the patient could

24 C. R. J. C. Newton and S. Krishna
not cope with an increased acid load. Approximately 42%(25/60) of children with CM were acidaemic (capillaryblood pH ,7.3) compared with 5% (4/81) with uncompli-cated disease (P , 0.0001), and some had inadequate respi-ratory compensation for the metabolic acidosis. The rela-tive risk of a fatal outcome for acidaemic patients with CMwas 8.5 (95% CI 1.1–64). Acidaemia, attributable to a lac-tic acidosis, was associated with hypoglycaemia, elevatedwhite cell count, and witnessed convulsions. Although lac-tate levels were lower in uncompensated metabolic acidosisthan in those who had partially compensated, this findingprobably represents the inability of some patients with CMto mount an effective ventilatory response to acidosis.
6.4. Severe Malarial Anaemia, Jaundice, and Haemolysis
The incidence of severe malarial anaemia has increasedwith the spread of chloroquine-resistant P. falciparum para-sites across the world (Zucker et al., 1996). Patients mayimprove symptomatically following chloroquine treatment,but unless the parasites are cleared completely, the haemo-globin is lowered and the patient becomes increasingly vul-nerable to a life-threatening anaemia (Bloland et al., 1993).Destruction of PRBCs is an inevitable consequence of P. falci-parum infection and usually produces a fall in haemoglobin.The WHO defines severe malarial anaemia as a haemoglo-bin concentration ,50 g/L (or a haematocrit ,15%) in apatient with a P. falciparum parasitaemia in excess of 10,000trophozoites/mm3 (Warrell et al., 1990), with normocyticindices. However, this definition may not be appropriate inmalarial-endemic areas, since anaemia is common, causedmainly by iron and folate deficiency or haemoglobinopa-thies (Newton et al., 1997d), and children often adjustphysiologically to the low haemoglobin concentrations.Life-threatening anaemia is determined more by the rate of
decrease in haemoglobin than the absolute level of haemo-globin, but children with chronic anaemia may decompen-sate rapidly when challenged with a febrile illness.
The symptoms and signs of life-threatening severe malarialanaemia are those of respiratory distress and hyperdynamiccirculation, which may be caused by the underlying acidosisfrom inadequate oxygenation (English et al., 1997) or im-pairment of cardiac function. The contribution of impairedcardiac function to respiratory distress is not determined.However, most African children with severe falciparummalaria are fluid depleted, and respond well to rapidly ad-ministered blood transfusions (English et al., 1996c).
Malaria is the most common cause of severe anaemia inchildren admitted to hospitals in Africa and is responsiblefor many blood transfusions (Newton et al., 1997d; Slutskeret al., 1994; Greenberg et al., 1989). In children with CM, thelowest haematocrit is reached within the first 24 hr aftertreatment (Molyneux et al., 1989b) and 23% of the childrenrequired blood transfusions during the first 24 hr (Moly-neux et al., 1989b). In some studies, African children withCM who also have severe anaemia (haemoglobin ,50 g/L)are less likely to die (Marsh et al., 1995), but in others aremore likely to die or survive with sequelae (Brewster et al.,1990). They may take longer to recover consciousness (Moly-neux et al., 1989b). Whether severe anaemia contributesdirectly to impaired metabolism (by reducing oxygen deliv-ery) or simply is a marker of severe disease is unclear.
6.5. The Commonest Modes ofPresentation of Severe Malaria in Children
Identifying children with malaria who are at high risk of afatal outcome depends on recognition of clinical signs, aswell as access to laboratory variables. When only simpleclinical criteria and bedside tests are available, then chil-dren who are deeply unconscious, hyperpnoeic, and hy-poglycaemic represent the most severely ill group of pa-tients. If lactate measurements or blood gas data areavailable, then the additional presence of lactic acidosis(lactate >5 mmol/L) or acidaemia (pH ,7.3, or base excess,15 mmol/L) identifies the majority of severely ill children(z80% of whom will die if they have 3 risk factors) (Tayloret al., 1993). However, the largest experience with theseprognostic variables is from Africa, and there may be con-siderable geographic variation in their relative importance.In Papua New Guinea, depth of coma was surprisingly notan important discriminant of a fatal outcome, whereas lac-tic acidosis was in one study (Allen et al., 1996b), but inanother study, deep coma, anaemia, and leucocytosis wereassociated with death (Genton et al., 1997). In our experi-ence with African children, parasitaemia is not a usefulprognostic variable (for reasons discussed in Section 2).The distribution of stages of development on a peripheralblood film may prove to be an additional simple bedsidemarker of severe disease, as in Southeast Asia (Silamut andWhite, 1993), but further studies are needed to confirm theutility of this test in African children. Likewise, the pres-
FIGURE 8. The relationship between venous metabolite con-centrations and mortality of 115 Gambian children with severemalaria: glucose (u), lactate (s) at admission, and lactate after4 hr (d). Reproduced from Krishna et al. (1994), with permis-sion of the copyright holder, Royal Society of Tropical Medicineand Hygiene, London.

Pathophysiology and Supportive Treatment of Severe Malaria 25
ence of pigment in leucocytes was found to be a useful prog-nostic index in Vietnamese adults (Nguyen et al., 1995),and was associated with severe malaria in Gabonese chil-dren (Metzger et al., 1995), but its usefulness remains to beestablished in other areas. Detailed consideration of thepathophysiology of these clinical syndromes is discussed inSection 7 and their management in Section 9.
6.6. Moderate Malaria
Moderate malaria is a disease category that identifies chil-dren who require parenteral treatment, but are unlikely(,10%) to progress to severe disease once appropriate anti-malarial treatment has begun. Patients with moderate ma-laria have none of the defining features of severe disease(no hypoglycaemia, lactic acidosis, coma, or recurrent sei-zures), but have other features that suggest the requirementfor parenteral treatment:
• a history of frequent and/or recent vomiting• drowsiness• obtundation, i.e., an apathetic response to painful stim-
uli such as capillary blood sampling or venepuncture• prostration, i.e., difficulty or inability to suckle, sit up,
stand up, or walk unaided according to the child’s age
Moderate malaria, like severe malaria, does not have apredictable relationship with the level of peripheral asexualparasitaemia or vital signs in individual cases (Sowunmi etal., 1992). Whilst the majority of children with moderatedisease improve rapidly with treatment and are dischargedfrom hospital within 1–2 days, deterioration in clinical sta-tus can occur within a few hours. Apart from the require-ment for parenteral therapy, this potential for rapid diseaseprogression necessitates admission and close observation.However, in-hospital mortality in this category of patientsis by definition low (,3%).
Uncomplicated malaria is infection not associated withany of the features of moderate or severe disease. It mostcommonly presents with fever, and the child is able to tol-erate oral antimalarial medication and can be treated as anoutpatient with an appropriate antimalarial. Mortality isnot anticipated in uncomplicated malaria, providing appro-priate antimalarials have been administered.
7. PATHOPHYSIOLOGY7.1. Fever
Fever is a characteristic feature of falciparum malaria, althoughparasitisation is not inevitably associated with fever. In ma-laria-endemic areas, many children are afebrile despite beingparasitaemic, even with relatively high parasitaemias. Thereis, however, a broad relationship between the level of parasi-taemia and fever in these areas, so that it is possible to deter-mine a threshold of parasitaemia (usually 2000–20,000 para-sites/mL) that has an optimum sensitivity and specificity forthe definition of a clinical episode of malaria (Greenwood,1996; Smith et al., 1995). The relationship is complicated by
the fact that the threshold at which fever occurs appears tobe influenced by age (Greenwood, 1996). Thus, recent stud-ies confirmed older findings that the parasitaemic thresholdfor fever varied by a factor of 5 with age and the threshold washighest in 1- to 2-year-old children (Rogier et al., 1996).
The rise in temperature during malaria infections isthought to be mediated by TNF (Kwiatkowski et al., 1989).TNF is an endogenous pyrogen, acting on the hypothala-mus to reset the set-point for temperature homeostasis. Theablation of fever in children administered anti-TNF mono-clonals supports the importance of TNF as the cause of fe-ver (Kwiatkowski et al., 1993), although the fact that notall fevers are associated with elevations in TNF suggeststhat other mechanisms may also be involved.
The role of fever in the pathophysiology of severe ma-laria is undetermined. Fever may synchronise the stages ofparasites (Kwiatkowski, 1989), promoting the survival ofparasites. In Gambian children with uncomplicated malaria,the increased resting energy expenditure is 37% higher com-pared with when they have recovered, and this is associatedwith a doubling of whole body protein turnover assessed bystable isotope techniques (Berclaz et al., 1996). Elevations inbody temperature are important in increasing energy expen-diture (by between 8.5 and 13.2%/8C), but are not the onlymechanism causing these rises. There is a negative proteinbalance during acute infection, which is reversed 15 daysafter the infection has been treated. Similar studies arelacking in children with severe malaria, but even greaterperturbations of energy expenditure are likely during theacute phases of infection. The role of fever on cerebral me-tabolism is not known and is unlikely to be predicted fromwhole body metabolism in unconscious children (Matthewset al., 1995). The effect of temperature on the brain ispotentially important because increases in temperature pro-mote ischaemic damage to neurons and may contribute to thedevelopment of neurological sequelae in children with CM.
7.2. Coma
The cause of the depressed level of consciousness in falci-parum malaria is unknown. Any theory of causation needs toexplain why coma develops relatively late in the illness inadults, compared with children; the fact that most patientsrecover without any evidence of neurological sequelae; andthat coma is caused by more than one mechanism. Part ofthe difficulty has been the definition of impairment of con-sciousness, since some of the “coma” scales used may notmeasure the depth of coma (Newton et al., 1997a).
Consciousness may be impaired by depression of the re-ticular activating system within the brainstem or a diffuseprocess affecting the cerebrum (Plum and Posner, 1980).Sequestration of PRBC within the cerebral venules, partic-ularly within the brainstem, is the most widely acceptedmechanism. The patchy involvement of blood vessels inthe brain may explain why most patients with CM developa completely reversible coma. The impaired delivery of nu-trients to certain areas of the brain may be compensated for

26 C. R. J. C. Newton and S. Krishna
by normal or increased delivery to microscopically adjacentregions (luxury perfusion), preserving the integrity andfunction of the brain as a whole, in spite of coma. Globalcerebral blood flow is not decreased in adults or childrenwith CM (Newton et al., 1996a; Warrell et al., 1988), butwhether it is appropriate for metabolic demands is un-known. The sequestered parasites may also produce toxins,either directly or stimulate host cells to produce substancesthat interfere with neuronal metabolism.
The common occurrence of seizures may contribute tothe impairment of consciousness, although the contribu-tion is difficult to determine. Subtle seizures and noncon-vulsive status have been documented in Kenyan children(Crawley et al., 1996; Kirkham et al., 1994). In the laterstudy, only half of the children with subtle seizures (i.e.,7.5% of children with CM) appeared to regain conscious-ness within 6 hr of the termination of the electrical activitywith diazepam. Prolonged post-ictal states may also contrib-ute to the impairment of consciousness in other children(Crawley et al., 1996), but there are no specific EEG fea-tures that differentiate a post-ictal state from a rapidly im-proving encephalopathy. The inappropriate administrationof benzodiazepines (intramuscular administration of highdoses) may also contribute to impaired consciousness andapparently prolonged post-ictal states.
In a few children with hypoglycaemia, the conscious levelimproves with the administration of glucose, although mostdo not (Taylor et al., 1988). Other metabolic derangements[e.g., severe acidosis (Allen et al., 1996a)] are associatedwith coma, but whether they are directly responsible for comais unclear. Systemic effects of the infection [e.g., fever orhyponatraemia (Arieff and Griggs, 1994)] may also contrib-ute, although they are unlikely to be responsible for deepcoma. The role of toxins in the pathogenesis of coma requiresfurther investigation. NO may impair neurotransmission,but there is little evidence to support this as a mediator inCM (see Section 4.5). Desferrioxamine, a ROS scavenger,appears to reduce the duration of deep coma (Gordeuk et al.,1992), although the mechanism is unclear. More recently,excitotoxic mechanisms have been invoked (Dobbie et al.,1997), particularly to explain the incidence of seizures.
Thus, it is likely that the impairment of consciousness pro-duced by falciparum malaria is caused by a number of inter-acting mechanisms (Newton et al., 1994) that cannot be eas-ily differentiated from each other, and the contribution ofeach mechanism cannot be easily determined. Further lighton these mechanisms may be shed by specific interventions.
7.3. Seizures
Seizures, particularly those witnessed after admission in chil-dren with CM, are associated with death (Waller et al., 1995;Molyneux et al., 1989b), and prolonged and multiple seizuresare associated with neurological sequelae. The relationshipmay not be causal, since seizures may be a marker of neuro-logical damage rather than the cause. In other encephalo-pathies, seizures often herald the onset of neurological dam-
age, particularly if they are focal in nature. Distinguishingcause from effect clearly has important ramifications, sinceanticonvulsant prophylaxis may prevent seizures, but notneurological damage. Seizures may cause death by aggravat-ing intracranial hypertension (IH) (Newton et al., 1991a),may cause neuronal loss, and may precipitate aspiration ofthe gastric contents into the lungs (Waller et al., 1995).
The cause of the seizures in CM is unclear. Intracranialsequestration of metabolically active parasites is a potentialmechanism, but difficult to investigate. The seizures are un-likely to be simply febrile convulsions (Akpede et al., 1993),since 54% of seizures occurred when the rectal tempera-tures were less than 38.08C, 48% were partial, and over70% were repetitive (Waruiru et al., 1996). Seizures maybe caused by hypoglycaemia and hyponatraemia, althoughstudies of Malawian and Kenyan children have not identi-fied these mechanisms as clinically important in malaria(Crawley et al., 1996; Waruiru et al., 1996; Molyneux et al.,1989b). Other potential mechanisms include toxins, e.g.,NO, excitotoxins, as discussed in Section 7.5.2.
7.4. Raised Intracranial Pressure
Raised ICP is an important cause of poor outcome in paedi-atric encephalopathies, particularly in CNS infections(Goitein et al., 1983). It can cause death by transtentorialherniation or a reduction in cerebral perfusion pressure(CPP), where CPP 5 mean arterial pressure 2 ICP. RaisedICP was thought not to be important in adults with CM,since over 80% of opening CSF pressures were in the nor-mal range, there was no difference in the CSF pressures be-tween those who died and survived (Warrell et al., 1986),and cerebral oedema was probably an agonal event (Looa-reesuwan et al., 1983, 1995). However, opening CSF pres-sures do not predict the maximum ICP when studied inother encephalopathies, and raised ICP may be caused byan increase in cerebral blood volume (Newton et al.,1991a) rather than cerebral oedema. Opening CSF pres-sures are raised in most African children with CM (Lew-allen et al., 1993; Waller et al., 1991; Newton et al.,1991a). The CSF pressures are similar to those found inadults with malaria, but are above the normal range forchildren. Most Kenyan children dying with CM have clini-cal signs compatible with transtentorial herniation (New-ton et al., 1991a), although these signs may be caused byother mechanisms (Kwiatkowski et al., 1991; Kirkham etal., 1991; Newton et al., 1991a). ICP monitoring con-firmed that children deeply unconscious from CM all hadraised ICP (with maximum ICP higher than the upper limitof adults) and that opening ICP did not predict maximumICP (Fig. 9) (Newton et al., 1997b). Furthermore, all chil-dren who developed severe IH (maximum ICP .40 mmHg, minimum CPP ,40 mm Hg) either died or survivedwith severe neurological sequelae. One child, who devel-oped an ICP of 158 mm Hg, died with signs of transtento-rial herniation. In another study, transcranial Doppler stud-ies showed that about one-half of the children dying from

Pathophysiology and Supportive Treatment of Severe Malaria 27
CM had sonographic features of progressive IH, whilst theremainder had sonographic features similar to children whodied of NCM (Newton et al., 1996a).
Transtentorial herniation occurs when there is an ICPgradient established between the contents of the skull andthe spinal cord (Plum and Posner, 1980). This may not applyin CM, where there may be a uniform increase in pressurein the neuraxis due to swelling and, therefore, displacementof cerebral structures is less likely to occur until ICPs becomegrossly elevated. The pathological features of tentorial her-niation, despite being described in the 1930s, have been re-ported infrequently in CM until recently (Section 3.2).
The most likely cause of raised ICP in CM is an increasein cerebral blood volume (Newton et al., 1991a) aggravatedby cytotoxic oedema in those who develop severe neurologi-cal sequelae (Newton et al., 1994). In a CT of Kenyan chil-dren recovering from CM, the scans were normal in mostchildren, but transient brain swelling occurred in childrenwith intermediate IH, and tomographic features of cytotoxicoedema were seen in children who developed severe IH(Newton et al., 1994). There was no evidence of vasogenicoedema or acute hydrocephalus in any of these children.These findings are consistent with observations made in amagnetic resonance imaging study in adults with CM (Looa-reesuwan et al., 1995). Cerebral blood volume could be in-creased by the sequestration of PRBC in the vascular com-partment, either acting as a diffuse space occupying lesion orobstructing venous outflow. Other features of CM, such asseizures, anaemia, and hyperthermia, would also increase ce-rebral blood flow and thus, increase cerebral blood volume.
Thus, raised ICP appears to be a feature of CM in Afri-can children, and severe IH, when it occurs, is associatedwith a poor outcome. Whether IH is a primary pathophysi-ological process remains to be established. Mannitol was ef-fective in lowering the ICP in Kenyan children (Newton etal., 1997b) and may have prevented children with mild de-grees of IH from dying or developing neurological sequelae,but it did not prevent the development of intractable IH inthose children with a poor outcome (Newton et al., 1997b).Further post-mortem studies examining the importance ofherniation, and clinical studies to test the effectiveness ofsubstances to reduce ICP in children with CM, are neededbefore treatment recommendations can be made.
7.5. Causes of Neurological Sequelae
The pathogenesis of neurological damage is likely to be differ-ent from the mechanisms that cause death, since the risk fac-tors are different (Newton, 1995). Death of neuronal tissuesmay be caused by necrosis or apoptosis, with similar or differ-ing pathophysiological processes that lead to these mecha-nisms (Table 6). In Kenyan children with neurological se-quelae, CT scans demonstrate a variety of patterns of damage,suggesting that a number of mechanisms may be responsible.
7.5.1. Ischaemia. Necrosis is caused by a critical reduc-tion in blood supply (ischaemia) or damage by toxins, such
as ROS, NO, or excitoxins. Reduction of cerebral bloodflow has not been associated with diffuse neurological dam-age in either children (Newton et al., 1996a) or adults(Warrell et al., 1988), although these intermittent mea-surements may have missed critical periods of reduced per-fusion. Reduced CPP, however, is strongly associated withsevere neurological sequelae (Newton et al., 1997b), and ifcerebral autoregulation is impaired, cerebral blood flow willbe determined by CPP. Some children with neurological se-quelae have evidence of borderzone infarction (Fig. 10),providing further evidence of reduced cerebral perfusion(Newton et al., 1994), although this is not a consistent fea-ture. Seizures, either prolonged or repetitive, may promoteischaemic damage, although as yet the evidence is lacking(Newton et al., 1997c).
7.5.2. Reactive oxygen species. ROS are generated dur-ing and after hypoxia-ischaemia. These species damage tis-sues by interacting with the polyunsaturated fatty acids ofcellular membranes, damaging proteins and DNA (Siesjo etal., 1989). ROS initiate a vicious cycle of lipid peroxida-tion, which is promoted by the presence of iron and lacticacidosis. This mechanism appears to be important duringreperfusion, particularly after a period of reduced microcir-culatory flow (Hurn et al., 1996) rather than complete is-chaemia, as may occur during the clearance of parasites.These species also promote the formation of NO and mayenhance the damage caused by excitotoxins.
7.5.3. Excitotoxins. Excitotoxins are endogenously pro-duced amino acids, which, under normal conditions, act as ex-
FIGURE 9. Opening ICP and maximum ICP in 23 childrenwho have undergone ICP monitoring. Opening ICP does notpredict maximum ICP. Modified from Newton (1995).

28 C. R. J. C. Newton and S. Krishna
citatory neurotransmitters, but when overproduced, becometoxic to the neuronal cells. The release of excitatory aminoacids is stimulated by hypoxia-ischaemia, hypoglycaemia,and seizures; the latter two are associated with the develop-ment of neurological sequelae in CM. There is no direct ev-idence that the above toxins cause neurological damage inCM, although these substances are difficult to measure, par-ticularly in the brain. The studies that have been conducteddemonstrate the raised concentrations of quinolinic acid,an excitotoxin in the CSF in children with sequelae (Dobbieet al., 1997). These results need to be interpreted within thelight of a possible breakdown in the BBB (Section 4.7.2).
7.5.4. Apoptosis. Apoptosis is the process of programmedcell death that occurs in vertebrates. The cell activates anintrinsic suicide mechanism that leads to characteristicmorphological changes (Fraser and Evan, 1996). It is in-duced by many factors, including TNF, ROS (Baier-Bitter-lich et al., 1995), and proteases. The role of apoptosis inneuronal death remains controversial, and as yet, there isno evidence to suggest apoptosis is responsible for neurolog-ical damage in CM, although this mechanism is difficult toinvestigate noninvasively.
7.5.5. Hemiparesis. Hemiparesis is one of the most com-mon and uniform neurological sequelae, but the cause is un-known. In studies of 10 West African children with hemi-paresis who did not have clearly defined CM (i.e., othercauses of an encephalopathy were not excluded), angiogra-phy demonstrated stenosis abnormalities in 5 children(Omanga et al., 1983; Collomb et al., 1967). Cerebral arteryocclusion was found in 4 children and segmental narrowingof the internal carotid in a further child; 5 children had com-pletely normal angiograms. In Kenyan children with strictlydefined CM, over one-half had a marked asymmetry of bloodflow velocity in the middle cerebral artery, as detected bytranscranial Doppler sonography (Newton et al., 1996a).
In 2 out of 7 children with hemiparesis, no flow could bedetected in the contralateral middle cerebral artery.
In a CT scan study of 12 children who had a residualhemiparesis 3–40 months following CM, 4 had unilateralatrophy, 5 asymmetrical atrophy, and 3 diffuse atrophy(Newton et al., 1996b). All the children with unilateral at-rophy had partial motor seizures and tomographic featuressimilar to those seen in hemiconvulsion-hemiplegia syn-drome after prolonged febrile convulsions (Kataoka et al.,1988). A child with multiple seizure types had severe asym-metrical atrophy. The atrophy was more severe in the pari-eto-occipital regions in 8 children. In none of these scanswas the damage confined to a single basal cranial artery ter-ritory. Furthermore, in an electroencephalographic study ofCM, 66% of seizures were partial, often localised over pari-eto-temporal regions (Crawley et al., 1996), regions thatare not typically borderzone areas. These findings suggestthat hemiparesis in CM may be caused by convulsions, pos-sibly as part of the hemiconvulsive-hemiparesis syndrome.The occlusion of middle cerebral artery found in some chil-dren still requires an explanation since large vessel throm-bosis is not a recognised feature of CM. Underlying ana-tomical abnormalities, disturbances of clotting, or severevasospasm may contribute.
7.5.6. Visual impairment. Cortical visual impairment, de-fined as visual impairment with intact pupillary responsesand normal fundi, is common following CM (Brewster etal., 1990). Although it can occur in isolation followingCM, it is usually associated with evidence of more diffusedamage (Lafaix et al., 1970). Blindness tends to improve,although most children do not recover completely. Thecause of blindness is not clear, although it is often associ-ated with seizures (Olurin, 1970). The occipital area is vul-nerable to hypoxic-ischaemic insults in other encephalopa-thies [e.g., meningitis (Thun-Hohenstein et al., 1992)]. Thisarea is particularly prone to damage following a reductionin cerebral perfusion, possibly because of a difference in the
TABLE 6. Possible Mechanisms for Neurological Damage
Anaemia Impaired delivery of oxygenCytokines Direct toxic effects
Stimulate release of NODiversion of metabolic substances Competition between host and parasites for metabolic substratesHypoglycaemia Impaired delivery of substrateHypoxia Microvascular obstruction
AnaemiaReduced cerebral blood flow
IH Impaired cerebral perfusionHerniation causing compression of posterior cerebral artery
Lactic acidosis Aggravating acidosisNO Formation of peroxynitriteROS Lipid peroxidation
NOSeizures Excitotoxic damage
Mismatch between cerebral metabolism and oxygen supplyRaised ICP

Pathophysiology and Supportive Treatment of Severe Malaria 29
autoregulation of the blood flow in the posterior circula-tion, making it more vulnerable to changes in perfusionpressure. Damage to the thalamic radiations and other ex-tra-striate structures may also occur.
7.6. Hypoglycaemia
Early studies noted that hypoglycaemia was a commoncomplication of malaria infection in humans (Fitz-Hugh,1944) and animals (Mercado and von Brand, 1954). Morerecently, there have been studies of the mechanisms of hy-poglycaemia in animal models of malaria, but findings maynot be directly applicable to human disease processes.
Observations were occasionally made in patients with se-vere disease (Migasena, 1983; Fisher, 1983), but the firstprospective series that identified hypoglycaemia and lacticacidosis in malaria and studied its pathophysiologicalmechanisms was published from Thailand in 1983 (Whiteet al., 1983). Twelve of 151 (8%) adult patients with CMexperienced hypoglycaemia, although 17 patients werestudied overall, including 3 women with otherwise uncom-plicated infection who were pregnant or who had deliveredrecently. The mortality in the hypoglycaemic group was sig-nificantly higher than in patients without hypoglycaemia[8/14 (57%) vs. 27/139 (19.4%), respectively; P 5 0.004],and hypoglycaemic patients had higher parasitaemias andmore severe multi-organ involvement than the remainder.A striking observation was that plasma insulin and C pep-tide levels were inappropriately high during episodes of hy-poglycaemia. In all but one patient, plasma quinine was de-tectable during the episode of hypoglycaemia, and quinineand insulin concentrations were correlated at the first hy-poglycaemic episode. There was an unpredictable clinicalresponse to glucagon or glucose treatment in these patients,although glucagon increased plasma glucose in all patients.
When quinine was infused in normal volunteers, there wasa significant increase in plasma insulin concentrations anda corresponding fall in fasting plasma glucose concentra-tions. These observations confirmed that quinine was re-sponsible for most episodes of hypoglycaemia in these pa-tients, through its capacity to induce hyperinsulinaemia.Pregnancy was identified as a major risk factor for the de-velopment of hypoglycaemia.
These studies in adults subsequently led to an examina-tion of the incidence and mechanisms of hypoglycemia inAfrican children with severe malaria (White et al., 1987b),after 2 index cases presented with hypoglycaemia duringthe course of pharmacokinetic studies on chloroquine. InGambian children who had P. falciparum parasitaemia andrequired parenteral chloroquine treatment, the incidence ofhypoglycaemia was 15/47 (32%), and its presence was pre-dictive of subsequent mortality (White et al., 1987b,c). Hy-poglycaemia was significantly associated with CM (52%had hypoglycaemia in this subgroup), a higher peripheralparasite count, and abnormal liver function tests. In con-trast to Thai adults, insulin levels were appropriately low inhypoglycaemic children, and patients were appropriatelyketotic. A later Sudanese study also found that pregnantwomen were prone to hypoglycaemia without associatedhyperinsulinaemia (Saeed et al., 1990). These observationsare consistent with the rapidity with which starved chil-dren (or pregnant women, or rarely other adults) are proneto deplete glycogen reserves and the inability of chloro-quine to provoke hyperinsulinaemia. They suggest impor-tant differences in the pathogenesis of hypoglycaemia be-tween Southeast Asian adults and patients in Africa.
Since the first reports on hypoglycaemia, many prospec-tive studies have confirmed that children are particularlyprone to develop this complication (Tables 1 and 3), butfew have examined its pathophysiology in detail. In
FIGURE 10. CT scan of childwith CM. (A) acute scan show-ing diffuse brain swelling withextensive hypodensity of the su-perficial watershed areas (arrows)and the basal ganglia. (B) con-valescent scan showing contrastenhancement of the border zone(arrows) between the left mid-dle and posterior cerebral arteryareas. Reproduced from Newtonet al. (1994), with permission ofthe copyright holder, BMJ Pub-lishing Group, London.

30 C. R. J. C. Newton and S. Krishna
Malawi, blood glucose was negatively correlated with theplasma concentrations of the gluconeogenic substrates lac-tate and alanine, but interestingly, not with the length oftime that patients had symptoms or had been fasting (Tay-lor et al., 1988). In this study, quinine was infused withdextrose solution, and patients who were normoglycaemicon admission did not develop hypoglycaemia. Pretreatmenthypoglycaemia was associated with higher mortality and re-current episodes of postadmission hypoglycaemia in somechildren, and a proportion of this group had inappropriateelevations in plasma insulin levels. In survivors, hypogly-caemia was associated with a higher incidence of neurologi-cal sequelae. There is likely to be depletion of glycogen re-serves in the livers of children with severe malaria, but thebiochemical basis of gluconeogenic defects has not beenidentified. Growth hormone concentrations are elevated inhypoglycaemic children, and there is no deficiency inplasma cortisol levels, suggesting appropriate counter-regu-latory homeostatic responses.
In adults with severe malaria, the conversion of galactose(Pukrittayakamee et al., 1991b) or glycerol (Pukrittayakameeet al., 1994b,c) to glucose are not significantly impairedwhen compared with similar rates measured in convales-cence, arguing against gluconeogenic impairment affectingthe enzymes responsible for these relatively proximal syn-thetic pathways. Similar studies have been completed withthe more distal metabolite alanine, and this study will pro-vide a more comprehensive assessment of gluconeogenesisin severe malaria (S. Pukrittayakamee, S. Krishna and N. J.White, unpublished observations). Glucose kinetics mea-sured in pregnancy (Davis et al., 1994) and in adults withuncomplicated (Davis et al., 1990b) and severe infection(Davis et al., 1993) demonstrate increased consumption ofglucose in acute infection. In the latter study, a primed in-fusion of [3-3H]glucose was given to 18 normoglycaemicadults with severe infection, and monitoring of glucose ki-netics carried out before and after quinine treatment. Glu-cose turnover was higher than normal, correlated with oraltemperatures, inversely correlated with plasma glucose levels,and decreased significantly after quinine infusion. Plasma in-sulin values rose significantly after quinine. Postquinineand convalescence glucose turnover rates were similar, butin view of the elevated insulin levels after quinine, hepaticinsulin resistance may be important in the acute phase ofinfection. In adults, peripheral insulin resistance offsets thehypoglycaemic effects of hyperinuslinaemia in acute infec-tion until recovery is taking place when delayed hypogly-caemia becomes a complication.
African children recover much more rapidly than adults,and although delayed hypoglycaemic episodes are morecommon following quinine therapy, compared with otherantimalarials, these may be less problematic than in adults(Krishna et al., 1994b). Admission hypoglycaemia is themore important complication of severe malaria in Africanchildren. In Kenyan children with uncomplicated malaria,basal glucose production did not correlate with alanine, lac-tate, counter-regulatory hormones, or cytokines, but only
plasma glucose production (Dekker et al., 1996), and didnot increase with the infusion of alanine (Dekker et al.,1997). Thus, in this group of children, it appears that en-dogenous glucose production is an important determinantof plasma glucose, in contrast to the findings in adults.
This increased demand for glucose in falciparum malariaresults from many stresses, including the effects of fever andincreased anaerobic glycolysis (which utilises glucose muchless efficiently to produce ATP) by both host tissues andparasitised erythrocytes. Anaerobic glycolysis is discussed inthe following section.
7.7. Lactic Acidosis
Systemic lactic acidosis, like hypoglycaemia, is a metabolicendpoint of many potential causes in severe malaria. Therelative importance of these causes may vary from patientto patient, and broadly reflect both increases in lactate pro-duction and inadequate lactate clearance by normal ho-meostatic mechanisms (Mordes et al., 1996). Lactic acido-sis is one of the best markers of disease severity andmortality in malaria (Krishna et al., 1994b). In normal indi-viduals, gross elevations in plasma lactate occur transientlyin response to anaerobic strenuous exercise. These eleva-tions are a short-term solution to the demand for ATP gen-erated in skeletal muscle, and lactate is rapidly metabolisedfrom peaks of up to 20 mM to basal levels of ~1 mM whenoxygen becomes available to tissues. The production of lac-tate under anaerobic conditions allows glycolysis to con-tinue by maintaining a supply of NAD1, without whichglycolysis will cease. Utilisation of lactate takes place in theliver, kidney, skeletal muscle, and CNS by metabolism viapyruvate. Most pyruvate enters Krebs’ cycle, where it is oxi-dised to CO2 and water, utilising both the accumulated lac-tate anion and the accompanying acidic proton. Withoutthis resolution of lactic acidosis, the buffering capacity of theblood and tissues is exceeded, and lactic acidaemia superveneson lactic acidosis (Stacpoole, 1997). The levels of lactic acidwhere acidaemia is likely to supervene are >5 mM, althoughthere may be significant metabolic dysfunction in patientswith lactate levels below this value. Sustained elevations inplasma lactate, therefore, can be viewed as a marker for in-adequate mitochondrial metabolism of pyruvate, as this isthe principal route whereby lactic acid is cleared in health(Stacpoole, 1997). In severe malaria, it is unlikely that al-ternative routes of lactate utilisation via pyruvate throughsynthetic routes (by conversion to oxaloacetate or acetylcoenzyme A) will be quantitatively important.
Increased lactate production in severe infection can re-sult from many causes. Fever and anaemia themselves in-crease metabolic rates (Stettler et al., 1992). Generalisedseizures cause brief, large bursts of anaerobic glycolysis inmuscle tissue, and can produce severe, if transient, lacticacidosis in otherwise normal adults (Orringer et al., 1977).Their effects are likely to be more severe in malaria wherethere are other derangements in glycolytic pathways, andsome host tissues (such as the brain and muscle) are already

Pathophysiology and Supportive Treatment of Severe Malaria 31
net exporters of lactic acid to the blood. While muscle tis-sue damage is well documented in severe malaria in chil-dren (Miller et al., 1989b) and a higher proportion of chil-dren with abnormal creatine kinase values [12/16 (75%)]have a history of seizures when compared with those whosecreatine kinase values are in the normal range [21/21(50%); P 5 0.076, Fisher’s exact test], there are no studiesthat have prospectively evaluated the contribution of sei-zures to lactic acidosis in malaria in children.
Infected erythrocytes generate 20- to 50-fold lactate (andconsume correspondingly large quantities of glucose) com-pared with NPRBCs (Warrell, 1989). This increased glycoly-sis may not be sufficient to perturb homeostasis in a normalindividual, but it may be more important in severe malariawhere the PRBC are localised to capillaries, and local met-abolic diversion may be more severe. Severe anaemia de-creases the oxygen-carrying capacity of blood, althoughcompensatory mechanisms can restore oxygen delivery totissues. If anaemia develops over a period of days ratherthan hours, then there may also be changes in the oxygen-dissociation curve (Jones and McGregor, 1954) induced byincreased intraerythrocytic synthesis of 2,3-diphosphogly-cerate (Bohr shift), resulting in increased unloading of oxy-gen, although these mechanisms can be blunted in the pres-ence of acidosis (Krishna et al., 1983). Anaemia alsodecreases viscosity, which can increase blood flow to tis-sues, although the increase in cerebral blood flow followinga drop in haemoglobin is caused by a decrease in oxygen-carrying capacity (Brown and Marshall, 1985). These phys-iological adaptations have not yet been examined in severemalaria in humans, although a study in an animal model ofsevere malaria, 31P-NMR studies demonstrated adequatecerebral stores of phosphocreatine, ATP, and pH, in spiteof severe anaemia and lactic acidosis (Krishna et al., 1983).
In adults with severe malaria, adrenaline use, in contrastto dopamine, was associated with a worsening of lactic aci-dosis complicating severe malaria (Day et al., 1996). Inchildren, inotropic support is infrequently required in man-agement, but dopamine would be the preferred inotrope.Chronic salicylate toxicity has been identified in Kenya asa potential cause of lactic acidosis and hypoglycaemia insome children presenting with clinical features of severemalaria (English et al., 1996a). Geographical variations inaccessibility to aspirin and local prescribing habits may alertclinicians to this possible cause, although in Ghana, salicylatesare not used and children presenting with lactic acidosis donot have detectable plasma levels (T. Agbenyega, T. Plancheand S. Krishna, personal observations).
In Thai adults (n 5 8) with malaria and moderate meta-bolic derangement (mean arterial lactate concentrations of3.44 mmol/L and pH values .7.3), lactate kinetics andskeletal muscle lactate metabolism were examined using alactate infusion labelled with a stable isotope (Davis et al.,1996). Quinine treatment did not affect the plasma lactate,pyruvate, or alanine concentrations or arteriovenous differ-ences in these metabolites measured across forearm muscle.Lactate turnover did not change significantly during acute
infection (both before and after quinine treatment) and inconvalescence, although metabolic clearance of lactate wassignificantly lower in acute infection. Lactate turnover inacute infection was correlated with simultaneous arterialplasma lactate concentrations, but no such correlation wasobserved with lactate clearance rates. Lactate release fromskeletal muscle was significantly greater following quinine,and this was much higher than that observed in convales-cence. The observed reduction in lactate clearance in thesepatients accords with observations made in severe malaria,where there is diminished liver blood flow. This reductionin liver blood flow may limit lactate delivery to the liver(Molyneux et al., 1989a), although this is less likely in pa-tients with moderately severe disease (Pukrittayakamee etal., 1994b). Additionally, the liver may have an impairedintrinsic capability to clear lactate in acute infection.
Many of these earlier observations made on lactic acido-sis and malaria have been repeated in a recent Kenyanstudy (English et al., 1997). In this study, a high anion gap(.11) remained in most patients with severe malaria, evenafter accounting for hyperlactataemia, and alternative causesfor this were suggested. Renal impairment was not severe (asestimated by plasma creatinine values) and was associatedwith acidosis, but could not account for the increase in an-ion gap, as organic acids retained by the kidney result in arelatively slowly developing lactic acidosis, usually when re-nal impairment is severe. It is likely that other anions, suchas b-hydroxybutyrate (not picked up by dipstick analysis ofurine) or phosphate or urate, could have contributed to theanion gap, although these were not investigated in thisstudy. In summary, lactic acidosis is an important complica-tion in severe malaria that is difficult to manage, and maycontribute directly to a fatal outcome.
7.8. Anaemia and Thrombocytopaenia
Destruction of PRBC with a fall in haemoglobin is almostan inevitable consequence of falciparum malaria. Severeanaemia can be one of the life-threatening complications ofP. falciparum infections, although in African children, it isassociated with a relatively low mortality on its own (Fig.4), but much higher when associated with CM or acidosis(Marsh et al., 1995).
The anaemia could be caused by many interacting mech-anisms. Removal of erythrocytes by the spleen is an impor-tant mechanism in adults with splenomegaly, in whom thespleen is the major site of erythrocyte destruction after theinstitution of therapy (Looareesuwan et al., 1987). In non-immune adults without CM, using a simple mathematicalmodel, the fall in haematocrit could be described by athree-term equation (Davis et al., 1990a). The initial fall inhaematocrit (during the first few hours) is caused by plasmavolume expansion; a zero-order fall with a mean half-life of25 hr occurred with the fall in parasitaemia and another fallwith a half-life of 43 days is associated with a loss ofNPRBC. However, this model relies on some tenuous as-sumptions, e.g., that the number of PRBC that sequester af-

32 C. R. J. C. Newton and S. Krishna
ter treatment is small, although it is unlikely that quinineused in this study affected sequestration during the initialphases (Watkins et al., 1993). This model has not been ver-ified in adults or children with CM.
Impaired red cell production, manifesting as dyserythro-poiesis in chronic malarial infections (Abdalla et al., 1980),is thought to play a role in the production of severeanaemia in malaria. Dyserythropoiesis is a feature of chronicanaemia caused by P. falciparum in Gambian children (Fig.11), but is not a significant factor in the fall of haemoglobinin acute infections (Abdalla et al., 1980). It is not confinedto children with malaria since it is also found in childrenwith iron deficiency and sickle cell disease (Newton et al.,1997d). In Gambian children and adults with uncompli-cated malaria, the degree of dyserythropoiesis correlateswith the severity of iron deficiency (Abdalla, 1990; Phillipset al., 1986), but in children with severe anaemia, no suchrelationship was found (Newton et al., 1997d). The causeof dyserythropoiesis in these children is not clear. TNF maylead to dyserythropoiesis (Clark and Chaudhri, 1988), al-though there is no clinical evidence to support this asser-tion in Kenyan children (Newton et al., 1997d). In Africanchildren with severe malarial anaemia, erythropoietin levelswere appropriately raised for the haemoglobin concentration(Burchard et al., 1995; Newton et al., 1997d), unlike Thaiadults, in whom erythropoietin levels were inappropriatelylow (Burgmann et al., 1996).
As documented by a positive direct antiglobulin test(DAT), autoimmune haemolysis has been suggested as animportant component of severe malarial anaemia (Facer etal., 1979). Several studies have not found a consistent associ-ation between a positive DAT and parasitaemia (Newton etal., 1997d; Merry et al., 1986; Abdalla et al., 1983; Abdallaand Weatherall, 1982; Greenwood et al., 1978), although inone study, a positive DAT was associated with clinical ma-laria (Abdalla et al., 1983) and in others, it was associatedwith anaemia (Jeje et al., 1983; Facer et al., 1979). One pos-sible mechanism is the production of autoantibodies to triosephosphate isomerase (TPI), a glycolytic enzyme. These anti-bodies are associated with haemolytic anaemia in Epstein-Barr virus infection (Ritter et al., 1990), and the hereditarydeficiency of this erythrocyte enzyme is associated with aneurological syndrome and increased susceptibility to infec-tions. In P. vivax infection, no anti-TPI antibodies were de-tected in 5 patients. However, in 4 of 10 nonimmune patientswith P. falciparum infection, who had biochemical manifes-tations of haemolysis (lactate dehydrogenase .200 U/L andanaemia) continuing for weeks after parasitaemia hadcleared, there was a correlation between anti-TPI antibodytitres and severity of anaemia (Ritter et al., 1993). Reactiva-tion of Epstein-Barr virus infection was only detectable in 1of these 4 patients with anti-TPI antibodies, suggesting thatreactivation is not necessary for this mechanism of autoim-mune haemolysis to operate in malaria. The exact mecha-nism of red cell damage is still unclear, and the significanceof anti-TPI antibodies in the anaemia of malaria in Africanchildren is unknown, but worth exploring.
Thrombocytopaenia commonly accompanies both falci-parum and vivax malaria, and is due to increased consump-tion of platelets during the acute infection with adequatenumbers of megakaryocytes in the bone marrow (Srichaikulet al., 1988; Looareesuwan et al., 1992). Thrombocytopae-nia was associated with elevations in macrophage colony-stimulating factor, which may mediate the increased de-struction (Lee et al., 1997). In some adults, it is associatedwith a specific IgG attached to platelet-bound malaria anti-gen (Kelton et al., 1983). It was more profound in severedisease and was associated with increases in plasma P-selec-tin levels (a marker of endothelial cell activation) (Lee etal., 1997). Although thrombocytopaenia is common andmay be associated with biochemical markers of disseminatedintravascular coagulation, a haemorrhagic diathesis in severemalaria in children is rare. The degree of thrombocytopaeniais frequently mild to moderate (.50 3 109/L), and in Afri-can children, is probably unrelated to disease severity.Changes in platelet aggregability also accompany thromb-ocytopaenia (Srichaikul et al., 1988).
7.9. Electrolyte Abnormalities and Fluid Balance
Hyponatraemia (Na1 ,135 mmol/L) occurs in over half ofthe patients with severe malaria, particularly CM (Englishet al., 1996b). The cause of the hyponatraemia is contro-versial. English and colleagues argued that hyponatraemiaresults from an appropriate hormonal response to the loss ofelectrolyte and fluid in sweat and stool. Yet, the childrenwith most severe hyponatraemia were less dehydrated (lowerurea and less weight gain after treatment). A more recentstudy has shown that some Kenyan children appear to haveinappropriate urinary sodium loss for the plasma sodiumlevel (Sowunmi, 1996a), although osmolality was not mea-sured. Furthermore, at least one child had features of cere-bral salt wasting syndrome, and in both of these studies, uri-nary sodiums are often inappropriately high. Thus, it is
FIGURE 11. Bone marrow aspirate of a Kenyan child withmalarial anaemia, showing malarial pigment (MP) and featuresof dyserythropoiesis, such as karyorrhexis (K) and incompletemitosis (IM). (© C. R. J. C. Newton)

Pathophysiology and Supportive Treatment of Severe Malaria 33
likely that hyponatraemia results from a combination ofmechanisms that include lack of sodium intake, loss of so-dium in body fluids, including sweat and gastrointestinallosses, and inappropriate arginine vasopressin secretion.Whatever the mechanisms, hyponatraemia does not appearto be associated with seizures, neurological damage, ordeath, and consequently, is of little direct clinical signifi-cance. Hypernatraemic dehydration occasionally occurs inAfrican children and is often associated with a poor out-come (C. R. J. C. Newton, personal observations), al-though not studied in detail.
Hypokalaemia (K1 ,3.5 mmol/L) was present in 14% onthe day of admission in survivors, but this increased to 39%the following day. There was speculation that hypokalaemiamay contribute to a variety of complications, such as cardiacdysrhythmias and late respiratory arrest. However, dysrhyth-mias are not important complications of malaria in children(Bethell et al., 1996), although supraventricular ectopic beatscan be observed frequently in some children with severe dis-ease, and a prolonged Q-T interval is seen in acute infections(von Seidlein et al., 1997). Respiratory arrest most commonlyfollows a neurological pattern (with progressive brainstemsigns) rather than a metabolic one. Hyperkalaemia is uncom-mon in severe childhood malaria, and if it occurs, it is oftenassociated with severe haemolysis or renal impairment.
Other electrolyte abnormalities have been detected, e.g.,hypophosphataemia (i.e., ,0.8 mmol/L phosphate in 43%adult patients and ,0.3 mmol/L in 11/14 severely ill pa-tients) (Davis et al., 1991) and less commonly hyperphos-phataemia, but their significance in the pathophysiology ofinfection is unknown. Mildly abnormal plasma calcium(corrected) levels and magnesium levels were commonlyobserved, but are unlikely to contribute significantly to patho-physiology (Davis et al., 1991). By contrast, in childrenwith severe malaria, serum calcium, potassium, urate, andphosphate concentrations were significantly elevated in fatalcases compared with survivors (Waller et al., 1995). Whilstmean serum calcium and potassium concentrations werestill within the normal range in fatal cases, mean phosphateand urate concentrations were increased above normal.
Electrolyte abnormalities can assist in choice of intrave-nous fluid in the initial management of children with se-vere malaria, but accurate assessment of the circulating in-travascular volume is necessary to estimate the amounts offluid needed. Intravascular circulating volume is notori-ously difficult to assess clinically in children and in severemalaria, especially in hypotensive children. Central venouspressure (CVP) measurements are probably the most accu-rate way to estimate fluid requirements. Where possible,these measurements should be interpreted in conjunctionwith plasma electrolytes to determine the nature and rate offluid replacement in severely ill children.
7.10. Renal Impairment and Blackwater Fever
Acute renal failure and pulmonary oedema are commoncomplications of falciparum malaria and a major cause of
death in adults (Warrell, 1987; Tran et al., 1996a; MateKole et al., 1996; Trang et al., 1992), but are rarely seen inAfrican children (Waller et al., 1995; Marsh et al., 1995;Molyneux et al., 1989b). Elevation in plasma creatinine,however, is common in childhood CM (Sowunmi, 1996b),and although it is associated with death (Waller et al.,1995), none of the children die from renal failure. A dispro-portionate increase in urea suggests that the elevated creat-inine is probably caused by hypovolaemia (English et al.,1996b) and aggressive intravascular volume repletion maybe required in some children (English et al., 1996c). Therehave been no clinical trials to determine if rate of rehydra-tion and type of intravenous fluid therapy influence out-come in severe disease. There is little evidence that suchaggressive fluid therapy is detrimental to the brain in chil-dren with CM. Whole blood transfusion, for example, im-proves the perfusion pressure, with a mild increase in ICP(Newton et al., 1994). Renal impairment can also be causedby a glomerulonephritis from the circulating immune com-plexes, intravascular haemolysis manifesting as blackwaterfever. The glomerulonephritis is seen in nonimmune patients(Anonymous, 1976; Boonpucknavig and Boonpucknavig,1988), but rarely documented in African children.
Blackwater fever was often associated with malaria infec-tions in the past, but the incidence appears to have fallen(Mate Kole et al., 1996). It is more frequently seen in non-immune patients (Warrell, 1987), particularly in SoutheastAsia (Tran et al., 1996a), where the outcome is better thanearlier reports from Africa. In Africa, it is occasionally seen inchildren with severe malaria, but is often caused by otherinfections or haemoglobinopathies (Delacollette et al., 1995).
7.11. Secondary Infections
Superimposed bacterial infections (pneumonia, septicaemia,and urinary tract infections) can complicate malaria innonimmune adults (Phillips et al., 1986) and may be de-tected in African children and contribute to mortality.Non-typhi Salmonella septicaemia was found in Gambianchildren with malarial parasitaemia (Mabey et al., 1987),but septicaemia was rarely found in African children withCM in one study (Molyneux et al., 1989b).
8. ANTIMALARIAL TREATMENT8.1. Introduction
This article focuses on supportive care, but would be incom-plete without a brief description of the main groups of anti-malarial drugs. Often antimalarial treatment is unavailableat the primary health care level when parents present withtheir sick child, frequently after delays induced by arduoustravel, the need to care for the remaining children in thefamily, consultation with traditional healers, and the lack ofmoney. In this context, a simple (nonparenteral) method ofadministering antimalarials could make the difference be-tween progression of infection to severe disease and death, or

34 C. R. J. C. Newton and S. Krishna
survival. Intrarectal formulations of antimalarials currentlyare being developed to examine this interventional strategyin the near future (Barennes et al., 1996; Hien, 1994).
In essence, modern management of severe malaria con-sists of the rapid administration of an appropriate antima-larial and the treatment of complications, such as hypogly-caemia, anaemia, intravascular volume depletion, andconvulsions. Administration of a rapidly acting parasiticidalantimalarial is, therefore, one of the immediate aims ofmanagement. Which antimalarial and by what dose and routeare questions that have to be answered individually for par-ticular geographic areas. All antimalarials require time inwhich to exert their maximum antimalarial effects. Theseeffects, and their speed of inhibition, vary between antima-larials and have been studied in detail in vitro (Watkins etal., 1993; ter Kuile et al., 1993). Thus, parasite killing, in-hibition of parasite metabolism (glycolysis, nucleic acidsynthesis, and protein synthesis), and of virulence factors(such as rosetting ability and cytoadherence characteristics)are all endpoints that have potential relevance to patho-physiology of severe disease, as well as variability in theirresponsiveness to different classes of antimalarials (Udom-sangpetch et al., 1996; Kwiatkowski and Bate, 1995). Theartemisinin derivatives as a class are undisputedly the mostrapidly acting of antimalarials (Hien and White, 1993).Additionally, they have the broadest stage specificity of an-timalarial effect. These in vitro (or ex vivo) observations areclearly translated into significantly faster parasite clearanceestimates in vivo compared with other antimalarials, in pa-tients with both severe and uncomplicated malaria (Hienand White, 1993). However, in studies designed to answerthe crucial question of improved survival when arteminisinderivatives are compared with quinine, there is no clearbenefit for artemether over quinine in African children(van Hensbroek et al., 1996a) or Vietnamese adults (Tranet al., 1996b). Indeed, clinical measures of recovery fromdisease (rather than parasitological ones) favoured the useof quinine over artemether (shorter duration of coma andhospitalisation time, and significantly fewer seizures) (vanHensbroek et al., 1996a). These findings highlight a num-ber of important general points about antimalarials.
Relying on parasite clearance estimates as an endpoint insevere malaria is misleading. Apparent benefits such asspeed of parasiticidal activity in vitro do not necessarilymean benefits in vivo, and there may be unsuspected disad-vantages of artemether use (such as seizures) in children.There is little doubt that if and when quinine becomes inef-fective as an antimalarial for severe infections, then thenext line of treatment will rely on one of the arteminisinderivatives for which there is a growing experience inparenteral formulations. Once the toxicity of these com-pounds has been defined better, their availability and usageare, therefore, likely to increase. However, for the moment,the drug of choice for severe malaria in most of sub-SaharanAfrica, where there is established chloroquine resistance inparasites, is quinine. The pharmacokinetics of the cinchonaalkaloids and the aminoquinolines, and their clinical appli-
cations, recently have been reviewed (Krishna et al., 1996)and their usage is briefly covered in the following sections.
8.2. Cinchona Alkaloids
Quinine is the preferred antimalarial for the treatment ofsevere malaria in both children and adults. In some coun-tries such as the United States, quinine has been unavail-able since 1991, and quinidine, the diastereomer of qui-nine, is the alternative (Miller et al., 1989a; Phillips et al.,1985). Unfortunately, with the introduction of newer anti-arrhythmic agents, even quinidine availability is becomingincreasingly and worryingly limited in the United States(Rosenthal et al., 1996).
Recent debate on quinine use has focused on the ques-tion of applicability of a loading dose in severe malaria, andthe exact recommended dose. In patients who have not re-ceived previous quinine treatment, we favour the use of aloading dose to ensure a rapid increase in plasma concen-trations in children with severe disease. In centres that lackintensive care facilities, quinine can be given by the intra-muscular rather than the intravenous route, and at a 12-hourly rather than an 8-hourly maintenance regimen in chil-dren for a number of reasons. First, it is simpler, with fewerdoses required overall. Second, in many settings, intrave-nous infusions may not be monitored as closely as necessaryto prevent excessively rapid quinine administration and at-tendant cardiotoxicity. Third, it may be cheaper as there isless requirement for sterile disposables. Fourth, intravenousaccess is not a prerequisite, as antimalarial treatment canbegin without delay and intravenous access can be estab-lished later. Finally, there are no important pharmacoki-netic differences in profiles and behaviour of intramuscularcompared with intravenous quinine, even in patients whoare severely ill (Pasvol et al., 1991). A potential disadvan-tage of intramuscular quinine is local toxicity, but this canbe minimised if the quinine is diluted 1:1 (v:v) with eitherwater for injection or sterile normal saline. The loadingdose is then administered divided equally into both thighs,and maintenance doses are carefully alternated betweenthighs. Tetanus is a rare complication, which should beavoidable by scrupulous adherence to sterile technique(Yen et al., 1994). Quinine can cause hypoglycaemia bystimulating insulin release (Section 7.6). This complicationis much more common in adults (particularly in preg-nancy), but hypoglycaemia should be also excluded in chil-dren wherever possible by regular monitoring. Children re-ceiving glucose supplementation rarely develop refractoryhypoglycaemia (Taylor et al., 1988).
The doses and frequency of administration of differentregimens of quinine are summarised in Table 7. Quinineshould be given for 7 days when used as a single antimalar-ial agent. Shorter regimens (e.g., 5 days) can be completedwith pyrimethamine-sulphadoxine. A recent report of in-tramuscular quinine in children with global malnutrition(not kwashiorkor) and malaria suggests that an 8-hourlymaintenance regimen may be preferred because of in-

Pathophysiology and Supportive Treatment of Severe Malaria 35
creased quinine clearance in the malnourished group com-pared with controls who were not undernourished (Treluyeret al., 1996). The rectal route for quinine administrationwas once considered too toxic, but recently, preparations ofcinchona alkaloids (.95% quinine in Quinimax™) havebeen successfully used after dilution in water for uncompli-cated malaria (Barennes et al., 1996). This route has notbeen studied in severe malaria. Quinidine is used in lowerdoses than quinine because of its greater potential for car-diotoxicity. Optimal dosing regimens have been debated re-cently (Krishna et al., 1996).
8.3. 4-Aminoquinolines
Chloroquine (and its structural relative amodiaquine)should only be used to treat severe malaria when there isconfidence that parasites still retain responsiveness to thedrug. In areas of emerging resistance, the acute infectionmay be managed with chloroquine, but cure may no longer beachievable. The choice of when to change from chloroquineto quinine is particularly difficult under these circumstances.Quinine is the preferred antimalarial, but the financial im-plications of a change in policy can be devastating in somesub-Saharan countries.
Chloroquine’s pharmacokinetics dictate that small fre-quent dosing is preferable to larger, less frequent dosing, aschloroquine has a small central compartment relative to itsvolume of distribution. Higher doses of chloroquine, there-fore, can give dangerously high peak concentrations. Chlo-roquine can be administered by a variety of routes in severemalaria (subcutaneously, intramuscularly, intravenously, oreven via nasogastric tube) and is absorbed rapidly fromparenteral sites. Our preferred regimen is via the intramus-cular or subcutaneous route (3.5 mg base/kg), given every 6 hrto a total dose of 25 mg/kg. Amodiaquine is a prodrug fordesethylamodiaquine, which has similar (though not iden-tical) pharmacokinetic properties to chloroquine.
8.4. Artemisinin Derivatives
The artemisinin derivatives, like quinine, are plant extractsthat have had a long-standing role in the treatment of ma-laria in China, but are now much more widely available.There are a variety of formulations of the arteminisin deriva-tives, which are principally distinguished by their solubilityin oil or water. These formulations (e.g., artemether or arte-misinin, which are oil soluble, and artesunate, which is watersoluble) have been administered via oral, rectal, intravenous,and intramuscular routes. In severe malaria, a number of re-
cent large prospective studies in African children and South-east Asian adults have compared intramuscular artemetherwith quinine. Artemether is similar in efficacy to quinine forthe treatment of severe malaria and is conveniently adminis-tered. Concerns about toxicity have led to caution in recom-mendations for use. Currently, toxicological aspects of arte-misinin derivatives are being investigated intensively.
The availability and usage of artemisinin derivativeseventually will be determined by drug regulatory bodies andthe WHO, but currently they are not licensed for use inWestern Europe or the United States. They are, however,widely available in sub-Saharan Africa, but generally aremore expensive than chloroquine or quinine. Pharmacoki-netic studies on these compounds have been hampered bytechnical difficulties with assays that only recently havebeen overcome, so that dosing regimens have been basedprimarily on studies of drug efficacy. In children, arte-mether can be given in a loading dose (3.2 mg/kg, intra-muscularly) followed by a maintenance dose of 1.6 mg/kgdaily for a minimum of 5 days. Artesunate can be given in-travenously or intramuscularly in severe malaria (loadingdose of 2.4 mg/kg, followed after 12 hr by 1.2 mg/kg, then at24 hr by 1.2 mg/kg, and 1.2 mg/kg every 24 hr for 7 days).Artesunate tablets can be substituted when tolerated.These regimens may be modified as pharmacological andtoxicological experience accumulates.
9. ADJUNCTIVE MEASURES
Good nursing care is crucial to the management of childrenwith severe malaria (Murphy et al., 1995a; Krishna andWhite, 1989). Children should be transferred to a dedi-cated (intensive care type) unit wherever possible andcared for by experienced nurses. Those children who de-velop signs of deepening coma or abnormal brainstem signsshould be considered for assisted ventilation, if facilities ex-ist for this supportive measure. These children should notbe made normocapnic, since this may precipitate transten-torial herniation (Looareesuwan et al., 1995). Childrenshould be monitored regularly for vital signs and the com-plications of hypoglycaemia and seizures. A nasogastrictube should be inserted in those with impaired conscious-ness or those at risk of aspiration pneumonitis, and eye careand oral hygiene measures should be instituted.
9.1. Antipyretics
Reasons to treat fever in malaria include making the pa-tient more comfortable, minimising metabolic stresses of
TABLE 7. Dose Regimen of Quinine Dihydrochloride in Severe Falciparum Malaria
Reference Route Loading dose Maintenance dose
Winstanley et al., 1993 Intravenous 7.5 mg/kg in 30 min, then 7.5 mg/kg over 1.5 hr 10 mg/kg over 2 hr every 12 hrWinstanley et al., 1994 Intravenous 15 mg/kg over 2 hr 10 mg/kg over 2 hr every 12 hrWaller et al., 1990 Intramuscular 20 mg/kg (2-site injection) 10 mg/kg every 8 hrPasvol et al., 1991 Intramuscular 20 mg/kg (2-site injection) 10 mg/kg every 12 hr

36 C. R. J. C. Newton and S. Krishna
infection, and perhaps reducing the risk of convulsions andneurological sequelae in children. There are no studies inmalaria that have shown an improvement in these parame-ters in parallel with a reduction in fever, although nonim-mune adults with uncomplicated malaria reported an im-provement in headaches following the use of ibuprofen(Krishna et al., 1995b). It is not clear if a reduction in coretemperature benefits cerebral consequences of severe malaria.
Whenever they have been studied, antimalarials, such aschloroquine and quinine, have not been found to have use-ful antipyretic properties (Krishna et al., 1995b; Vani-janonta et al., 1996) contrary to dogma. Specific anti-pyretic treatment is often used as an adjunct to antimalarialtreatment. In most developing countries, although aspirinis frequently used, paracetamol is the antipyretic of choice.In suppository formulation, paracetamol is convenient toadminister. Recently, however, paracetamol has been shownto prolong parasite clearance in Gabonese children withnon-severe malaria, possibly from a decreased production ofTNF-a and ROS (Brandts et al., 1997). In this study, it of-fered no benefit over mechanical antipyresis. However, oralparacetamol reduces fever in Thai adults with uncompli-cated malaria (Krishna et al., 1995b), and ibuprofen (10mg/kg), a nonsteroidal anti-inflammatory drug, is signifi-cantly more effective (Krishna et al., 1995b). Indomethacinis also superior to paracetamol in adults with uncompli-cated infection. Fever begins to recur 3–4 hr after paraceta-mol (15 mg/kg), so the dosing frequency may have to be upto 4 hourly until the underlying pyretic tendency subsides.Ibuprofen has a more sustained antipyretic action and,therefore, can be given less frequently (6–8 hourly).
Although salicylates are not recommended in childrenbecause of the danger of provoking Reye’s syndrome, inmany countries aspirin is still used as an antipyretic. Addi-tionally, aspirin may aggravate or even cause metabolic aci-dosis (English et al., 1996a) or, rarely, precipitate a bleed-ing tendency (Warrell et al., 1990). Parenteral antipyretics,e.g., dipyrone, are not widely used because of a significantrisk of fatal agranulocytosis (Warrell et al., 1990). Mono-clonal antibodies against TNF reduce the temperature inGambian children, but are unlikely to gain currency as an-tipyretics. The role of other measures, e.g., fanning and tepidsponging, are controversial since the rate of cooling is notsignificantly different from acetaminophen alone, althoughif these measures are used together, then they appear to re-duce the temperature more quickly than either alone(Steele et al., 1970). Fanning and sponging may not reducecore temperatures [Royal College of Physicians (London),1991], and may even aggravate hyperthermia (especially ifice water is used) by inducing vasoconstriction.
9.2. Anticonvulsants
It is prudent to prevent or terminate seizures since they areassociated with a poor outcome in CM and cause neuronaldamage in other encephalopathies, as well as in experimen-tal models (Wasterlain and Shirasaka, 1994). In the pre-
vention of malaria-associated seizures, phenobarbitone isthe only drug that has been studied in any detail. In a ran-domised double-blind study of 48 nonimmune Thai adultswith CM, phenobarbitone (3.5 mg/kg, intramuscular) re-duced the incidence of seizures after admission from 54 to12.5% (White et al., 1988). This effect was surprising sincethis dose is not usually associated with anticonvulsant ef-fects (Shorvon, 1994), although plasma phenobarbitoneconcentrations were not measured in this study. A slightlyhigher dose (5 mg/kg, intramuscular) administered to Gam-bian children with CM did not cause a deterioration inlevel of consciousness, and subsequently, studies using 7 mg/kg of phenobarbitone showed it was clinically well toler-ated, even when other anticonvulsants had to be added(S. Krishna, personal observation).
A small study of Southeast Asian children with severefalciparum malaria demonstrated that phenobarbitone (alsoused at 7 mg/kg, intramuscular) was well absorbed, reachinga peak (7 mg/L) within 4 hr, but failing to reach concentra-tions above 15 mg/L (ter Kuile et al., 1992), the level thoughtto prevent febrile seizures (Faero et al., 1972). This dose wasassociated with depression of consciousness level in somepatients. In 12 Kenyan children with severe malaria, ahigher dose (10 mg/kg, intramuscular) only achieved maxi-mal concentrations above 15 mg/L in 4 patients, and did notappear to reduce the incidence of seizures or affect the dura-tion and depth of coma (Winstanley et al., 1992). Currently,a larger prophylactic dose is undergoing clinical trials.
Seizures in severe malaria may abort spontaneously, butdata from other encephalopathies suggests that seizures lastinglonger than 5 min should be actively terminated. Diazepamand paraldehyde are effective drugs for the termination ofseizures, although there have been no studies conducted ontheir relative efficacy in children with malaria. In manyhospitals, these drugs, particularly diazepam, may be givenin inappropriate doses by intramuscular injection or toorapidly by the intravenous route, with the attendant risk ofrespiratory depression. Diazepam-induced respiratory de-pression is rapidly reversed by flumazenil, but this drug isexpensive and not widely available. If diazepam overdose issuspected, children, therefore, should be ventilated by bagand mask or endotracheal tube until spontaneous respira-tions return. Paraldehyde is well absorbed from intramuscu-lar injections and rectal administration (Shorvon, 1994). Itis generally safe (C. R. J. C. Newton, personal observa-tions), although it causes sedation and may prolong comafollowing the post-ictal phase. Other side effects are rareand include hypotension, metabolic acidosis, and pulmo-nary oedema (Shorvon, 1994). The rectal administration ofan outdated drug has caused severe proctitis, excoriatingrash, and large-bowel perforation. The chemical interac-tion of paraldehyde with plastic syringes has limited thedrug’s use, but if paraldehyde is quickly administered afterbeing drawn up, there appear to be no adverse effects.
The treatment of repeated or continuous seizures notcontrolled with diazepam or paraldehyde should follow thestandard treatment of status epilepticus. This may require

Pathophysiology and Supportive Treatment of Severe Malaria 37
access to facilities for assisted ventilation. Phenobarbitoneand phenytoin have both been used successfully, althoughnot directly compared in malaria. Phenobarbitone can begiven in a loading dose of 15–20 mg/kg (preferably intrave-nously, but may also be given intramuscularly), followed by5 mg/kg 12 hr later. Toxic effects of phenobarbitone in-clude decreasing the level of consciousness, respiratory de-pression, and hypotension (reputably after diazepam); al-though these effects are rarely seen in status epilepticus(Shorvon, 1994). Phenytoin (20 mg/kg) should be infusedover 20 min into a line that does not contain dextrose (toprevent precipitation), preferably with the patient’s ECGmonitored for excessive QTc prolongation, which predis-poses to ventricular arrhythmias. Phenytoin has relativelylittle respiratory and cerebral depression, although it maypotentiate the effects of benzodiazepines and barbiturates. Ifseizure control is not achieved with the use of one of thesedrugs, the second should be added, although not in a solu-tion containing other drugs, as precipitation may occur.Other measures (e.g., thiopentone, hypothermia) may oc-casionally be necessary.
9.3. Measures to Reduce Raised Intracranial Pressure
Of the many modalities for reducing ICP, osmotic diureticsare the only agents that have been tested in malaria. Man-nitol and glycerol are thought to reduce ICP by creating anosmotic gradient across the BBB, thereby causing extracel-lular fluid to be drawn into the intravascular space (Go,1991). The BBB must be relatively impermeable to theagent for the gradient to develop. The decrease in ICP iscorrelated with the increase in plasma osmolality that theseagents achieve, although the changes in ICP do not parallelthe changes in osmolality (Heinemeyer, 1987). Thus, theseagents may act by other mechanisms. For example, Muize-laar et al. (1984) have suggested that mannitol causes vaso-constriction by reducing blood viscosity, if autoregulation isintact. The vasoconstriction reduces cerebral blood volumeand thus, ICP. In general, the reduction of ICP followingthe administration of osmotic agents depends upon the ICPlevel at which the treatment is instituted, the rate ofchange in the osmolality, and the degree of hyperosmolalityinduced (McGraw et al., 1978).
Osmotic diuretics are used in children with head injury(Muizelaar et al., 1984; Marshall et al., 1978) and Reye’ssyndrome. In Reye’s syndrome, mannitol, in doses as low as0.25 g/kg, reduces ICP (Brown et al., 1978), although re-peated doses are often required (Marshall et al., 1978), andsome clinicians have used continuous infusions of mannitolto control raised ICP (Berman et al., 1975). Mannitol canmake the BBB more permeable and may cause a reboundphenomenon in which the ICP rapidly rises after an initialfall. This is thought to occur because the mannitol passesinto the interstitial space of the brain, drawing fluid fromthe intravascular space (Go, 1991).
Osmotic agents may also have other effects that contrib-ute to a reduction in ICP. Mannitol scavenges ROS, which
in experimental models have been shown to be associatedwith raised ICP. Also, PRBC are particularly susceptible tolysis with osmotic agents (K. Silamut, N. J. White and S.Krishna, unpublished observations), although the concen-trations required for lysis are significantly higher than can beachieved with the safe administration of these agents in hu-mans. Osmotic diuretics have been used in African chil-dren with CM, but their efficacy is difficult to assess sincerandomised control trials have not been conducted. King-ston (1971) reported an improved outcome in Liberianchildren who were given 30% urea in 10% invert sugar af-ter the children had deteriorated or were in prolongedcoma. Commey et al. (1980) thought that mannitol (1 g/kgevery 8 hr) improved the level of consciousness and per-haps outcome in Ghanaian children (Commey, 1984). InKenyan children, mannitol (0.5–1.0 g/kg) reduced ICP andimproved CPP in all cases, although in children with severeIH, this caused only transient improvements and did notprevent the development of intractable IH. A major ques-tion to arise from this study was whether osmotherapy con-tributed to the outcome in the group with intermediate IH.In 74% of children, the ICP was greater than 20 mm Hg formore than 15 min, a level that would be actively treated inmost intensive care units. All of these children except onewere given mannitol, and 70% had a good outcome. It wasnot possible to determine if severe IH was a consequence ofuntreated intermediate IH or whether severe IH reflects thedevelopment of widespread cerebral damage secondary toother concurrent pathogenic processes. At present, thereare not enough data to recommend an empirical regimenfor control of ICP.
The effectiveness of other modalities that can be used toreduce ICP has not been tested in CM. Two controlled tri-als of steroids have been conducted in Asian adults (Hoff-man, S. L. et al., 1988; Warrell et al., 1982a), but the effecton ICP was not monitored, and steroids did not reduce mor-tality. Hyperventilation has not been studied in CM sincemost patients are not ventilated. Indeed, spontaneous hy-perventilation, secondary to metabolic acidosis, may reducethe ICP and, therefore, increasing the PaCO2 in ventilatedpatients may increase the blood volume and precipitate tran-stentorial herniation in adults (Looareesuwan et al., 1995).
9.4. Correction of Hypoglycaemia
Theoretically, correcting hypoglycaemia in the presence oftissue hypoxia can worsen tissue acidosis, as original studiesby Seisjo and colleagues in animal models clearly demon-strated (Siesjo, 1978). However, similar studies monitoringtissue pH responses to correction of hypoglycaemia havenot been carried out in patients with CM, and would betechnically and ethically challenging. Consequently, indi-rect measurements monitoring, for example, plasma lactateconcentrations after administration of hypertonic glucosein adult patients with severe malaria suggest this procedure isnot associated with major adverse systemic effects (Pukritta-yakamee et al., 1991a).

38 C. R. J. C. Newton and S. Krishna
The correction of hypoglycaemia (blood sugar ,2.2mmol/L) or incipient hypoglycaemia (blood sugar .2.2–3.3mmol/L) requires hypertonic glucose (1 mL/kg of 50% dex-trose or 2 mL/kg of 25% dextrose). The maintenance require-ments of glucose in children with severe malaria are muchhigher than for uninfected children. In uncomplicated infec-tion in Kenyan children, the rate of glucose utilisation was 5.0(4.1–8.4) mg/kg/min (Dekker et al., 1996). Guidelines fromstudies carried out in adults suggest glucose should be replacedat z3 mg/kg/min, and are presently a reasonable basis for de-termining glucose infusion rates (Davis et al., 1993).
Other options have been suggested for correction of hy-poglycaemia in severe malaria, but none are appropriate forAfrican children presenting with this complication. Thus,in Thai patients with hyperinsulinaemic hypoglycaemia dueto quinine, Sandostatin (SMS 201-995, a long-acting so-matostatin analogue) given with glucagon boluses effec-tively restored plasma glucose levels and reduced circulat-ing insulin concentrations (Phillips et al., 1993). However,the treatments are expensive and have not been studied inAfrican children, where the natural history of postadmis-sion hypoglycaemic episodes is somewhat different. Simi-larly, galactose infusions in adults are readily converted toglucose, but similar studies are not available in Africanchildren (Pukrittayakamee et al., 1991b).
9.5. Acidosis
No human studies have demonstrated an improvement inmortality when lactic acidosis is treated with adjunctivetherapies (Stacpoole et al., 1992). The initial managementof patients with lactic acidosis from any cause, therefore, re-
lies on the effective treatment of the underlying disease, aswell as measures designed to optimise oxygen delivery totissues and to improve tissue perfusion (Stacpoole et al.,1994). In severe malaria, this involves the rapid administra-tion of antimalarials, correction of intravascular volume de-pletion and severe anaemia, anticonvulsant therapy if indi-cated, and general measures such as reduction in hightemperature. However, in a significant proportion of pa-tients, severe lactic acidosis still persists. In this group, animportant unresolved question is whether lactic acidosis perse can contribute directly to mortality from severe disease.This question can only be adequately resolved by studyinglactate metabolism in severe malaria, and then by interven-ing with a specific therapy to assess its impact on mortality.
Dichloroacetate (DCA) acts specifically to stimulate therate-limiting enzyme complex pyruvate dehydrogenase,which regulates the entry of pyruvate into Krebs’ cycle(Stacpoole, 1989). Its mechanism of action is shown in Fig.12. DCA maintains pyruvate dehydrogenase kinase in itsactive dephosphorylated state, allowing greater utilisationof pyruvate by aerobic metabolism, concomitantly reducingacid (i.e., free protons), as well as the lactate anion. Thepharmacokinetics and pharmacodynamics of DCA havebeen studied in great detail in animal models and a varietyof disease states in humans, and its safety in severe disease isestablished (Krishna et al., 1995a; Stacpoole, 1989).
DCA was first examined in malaria in a P. berghei youngrat model of severe metabolic dysfunction, where it attenu-ated rapidly rising lactate levels when given with quinine(Holloway et al., 1991). Subsequent studies established thatDCA could ameliorate malaria-associated lactic acidosis sig-nificantly more rapidly in both adults and children (Krishna
FIGURE 12. Site of action ofDCA.

Pathophysiology and Supportive Treatment of Severe Malaria 39
et al., 1994a, 1995a). These studies also examined the pharma-cokinetics of DCA in severe disease, as well as its efficacy.In order to justify further studies in patients, a large prospec-tive single-blind mortality study was carried out in the ro-dent model of severe malaria (Holloway et al., 1995). Ratswith lactic acidosis due to P. berghei infections (n 5 183with lactate .5 mM) were randomised to receive either aloading dose of quinine (and saline placebo, n 5 84) or qui-nine with DCA (n 5 99). Mortality was monitored for 2parasite life cycles (50 hr). DCA treatment significantly re-duced mortality (by 33%, odds ratio .2.2, P ,0.021) com-pared with placebo. These findings confirmed that DCA as anadjunct therapy with quinine in severe malaria has the po-tential to reduce mortality in patients. Furthermore, the pre-vious studies in patients have already established that in spiteof lactic acidosis, aerobic metabolism of lactic acid can beaugmented by the addition of DCA, implying that oxygendelivery to tissues may not be the limiting factor in allowingaerobic metabolism in some patients. In order to test thishypothesis further and to assess the relevance of DCA in se-vere malaria, a large placebo-controlled, double-blind mor-tality study of DCA is now underway in Ghanaian children.
Sodium bicarbonate has been considered useful in thepast in the management of lactic acidosis complicating se-vere disease states. However, its use may be harmful be-cause of the dangers of volume overload and paradoxicaltissue acidification (Stacpoole, 1986). We do not recom-mend its use in malaria-associated lactic acidosis or, indeed,in lactic acidosis complicating any severe disease. Otheragents such as carbicarb have not been studied in malaria.
9.6. Anaemia and Exchange Transfusion
The role of blood transfusions in the treatment of severemalaria remains controversial. Blood transfusions are ex-pensive and potentially dangerous in many malaria-endemicareas, since a high proportion of blood donors are hepatitisB surface antigen and human immunodeficiency virus-seropositive, and screening for these pathogens is not al-ways possible. Other viruses (such as hepatitis C) are alsocommon, but not routinely tested for in blood banks. Forthese reasons, most clinicians prefer to restrict blood trans-fusions to individuals with clear signs of cardio-respiratorycompromise, hyperparasitaemia, or CM and associatedanaemia (English et al., 1996c; Newton, 1992; Lackritz etal., 1992).
In a study of 24 Kenyan children, metabolic acidosis wasattributed to anaemia in 80% of the patients (English et al.,1996b). In many children, the acidosis responded to aggres-sive intravascular volume repletion, although z20% of thechildren continued to have sustained hyperlactataemia 4 hrafter CVP guided treatment was begun, and unfortunately,the study lacked a control comparison group. Blood (20mL/kg) was transfused if haemoglobin was 5 g/dL or below.These findings independently confirm that in the majorityof survivors with metabolic acidosis due to malaria, simpleresuscitative measures are sufficient to rapidly reverse meta-
bolic abnormalities (Krishna et al., 1994a), whatever thepostulated mechanisms of action of these interventions(which include the correction of anaemia as one possibil-ity). In symptomatic children, particularly those with signsof severe disease, it is reasonable to transfuse blood (orpacked red cells) as soon as practicable. CVP guidance canassist in assessing additional requirements for crystalloid(e.g., if CVP readings are ,5 cm). The risk of transfusion-associated pulmonary oedema appears to be low.
The role of exchange transfusion in malaria is more con-troversial. Exchange transfusions are usually partial rather thancomplete when carried out in the context of malaria treat-ment. Automated equipment to assist exchanges, the require-ment for larger quantities of safe blood, difficulties with venousaccess (or the higher cost of central lines), and more inten-sive monitoring rule out exchange transfusion as an option inthe management of malaria in most children. Even if avail-able, should exchange transfusion be used in spite of thesedisadvantages? In the absence of guidelines from any ade-quately powered prospective studies (Looareesuwan et al.,1990), the requirement for exchange is a matter for individualclinical judgement. The potential benefits are rapid removalof high circulating parasitaemia at a satisfyingly predictablerate (Wilkinson et al., 1994; Van den Ende et al., 1994) (andtheoretically, perhaps undefined plasma associated “tox-ins”); the rapid correction of severe anaemia, whilst mini-mising the risk of circulatory overload; and in Africa, theinfusion of antibodies, which may assist the infant’s responseto malaria infection. However, the circulating parasitaemiacan effectively be managed with antimalarials (e.g., it respondsparticularly quickly to artemisinin derivatives) and is a poorsurrogate marker of prognosis or disease severity, as it doesnot represent the sequestered parasite biomass. Severeanaemia is safely corrected by conventional blood transfu-sion, and in semi-immune children, high parasitaemias canbe surprisingly well tolerated. If available, then the next de-cision is at what level of parasitaemia should exchangetransfusion be contemplated? If the patient is not only hyper-parasitaemic, but clinically very ill (deep coma, hypoglycae-mia, acidosis, or severe anaemia), then we suggest exchangesshould be considered at parasitaemias of 20% and should bemore likely at parasitaemias .50%. However, the level ofparasitaemia by itself should never be used as the sole criterionon which to base a decision to proceed to exchange transfu-sion. A controlled clinical trial of partial exchange transfu-sion in severely ill children with high parasitaemias is longoverdue, but unlikely to be implemented in the near future.
9.7. Desferrioxamine
Desferrioxamine has been studied as an adjuvant agent inmalaria. It is an iron chelating agent, used in conditionssuch as haemochromatosis and thalassaemia requiring regu-lar transfusions, and successfully induces negative iron bal-ance when used chronically. Desferrioxamine reduces theformation of ROS by reducing the amount of free iron. Invitro and animal studies showed that desferrioxamine has

40 C. R. J. C. Newton and S. Krishna
antimalarial properties in its own right (Whitehead andPeto, 1990), probably by withholding iron from the parasite(Peto and Thompson, 1986; Hershko and Peto, 1988). Re-cently, a third mechanism has been proposed, i.e., desferri-oxamine enhances interferon-g activity and macrophageactivation, and those effects promote the destruction ofparasites through NO (Weiss et al., 1997). This may lead toenhancement of T1-cell-mediated immunity and possiblyto impaired T2-cell responses (Thuma et al., 1996).
These observations encouraged the trial of desferriox-amine in uncomplicated infections, and more recently as anadjunctive therapy in Zambian children with CM (Gor-deuk et al., 1992). In adults with mild or moderate malaria,desferrioxamine (100 mg/kg/day) enhanced the clearanceof asexual parasites in the absence of other antimalarials(Mabeza et al., 1996), although recrudescences were com-mon. In a controlled trial as an adjuvant treatment to qui-nine in Zambian children with CM, it appeared to reducethe duration of deep coma, and perhaps hasten the clear-ance of parasitaemia, although the study did not show anydifference in outcome or neurological sequelae (Gordeuk etal., 1992). Gordeuk and colleagues also showed that the du-ration of coma was inversely proportional to the transferrinlevels in these children (Gordeuk et al., 1995) and that desfer-rioxamine was associated with persistently raised neopterinlevels (Weiss et al., 1997). The significance of these clinicalfindings is not entirely clear, particularly because childrendid not receive a loading dose of quinine and control patientshad unusually prolonged coma recovery times. Desferrioxam-ine has been combined safely with artesunate in the treat-ment of patients with uncomplicated malaria (Looareesu-wan et al., 1996), and further trials in CM are in progress.Indeed, a recent report on 352 children with CM con-cluded that desferrioxamine given as an adjunct therapy toa loading dose of quinine did not reduce mortality whencompared with placebo (Thurma et al., 1998).
9.8. Anti-Inflammatory Agents9.8.1. Corticosteroids. Steroids have long been advocatedfor the treatment of CM, but two controlled trials in SoutheastAsian adults have shown no benefit (Hoffman, S. L. et al.,1988; Warrell et al., 1982a). The earlier trial concluded thatdexamethasone (1–2 mg/kg over 48 hr) was deleterious be-cause it prolonged coma in survivors and there was an in-creased incidence of side effects, such as pneumonia and gas-trointestinal bleeding (Warrell et al., 1982a). The otherstudy used larger doses (11.4 mg/kg dexamethasone over 48hr), but was smaller and included patients who were notstrictly defined as having CM. No studies have been re-ported in African children.
9.9. Agents that Improve Microcirculatory Flow9.9.1. Pentoxifylline. Pentoxifylline (or oxpentifylline) isa methylxanthine derivative that has many effects of poten-tial benefit in the management of severe malaria. It is a va-sodilator that reduces red cell deformability and blood viscos-
ity, decreasing systemic vascular resistance, and impairsplatelet aggregation, thus improving microcirculatory flow. Ithas been shown to be useful in animal models of ischaemia,particularly during reperfusion. It is useful in the manage-ment of peripheral vascular disease, but studies in humancerebrovascular disease have been unconvincing. It preventsthe neurological signs in mice infected with P. berghei, possi-bly by inhibiting the release of TNF (Kremsner et al., 1991).Furthermore, it inhibits rosette formation and promotes redblood cell detachment from rosettes in blood taken from Ga-bonese children with nonsevere malaria (Lehman et al.,1997). It has been studied prospectively in a trial of Africanchildren with CM, where it appeared to reduce the durationof coma (Di Perri et al., 1995), but this study was too small tostudy effects on mortality with confidence. A study in non-immune adults was abandoned because patients had moregastrointestinal complaints and there was no effect on in-flammatory markers (Hemmer et al., 1997).
9.9.2. Miscellaneous agents. Heparin and dextran havebeen suggested as agents that may improve microcirculatoryflow by reducing the viscosity of blood. No large controlledstudies have been conducted. In one study, heparin (300IU/kg intramuscularly/day) given to 21 Indonesian childrenwith CM, as adjunct therapy to quinine did not signifi-cantly improve the outcome compared with controls orthose given dexamethasone (Rampengan, 1991). It is un-clear if these children were adequately heparinised, but it isunlikely that a significant difference would be found in thisstudy (Type II error). Similarly, there is no evidence thatdextran improves outcome in CM, although again, propercontrolled studies have not been conducted.
9.10. Other Agents
Prostacyclin, an inhibitor of platelet aggregation, has been de-scribed in a single case report (Weston et al., 1982), but it isimpossible to assess the effect on the outcome of the patient.
10. DISCUSSION AND FUTURE STUDIES
Many potentially important pathophysiological events havebeen identified in severe malarial infection, but the testingof appropriate interventions to reverse them still remainsone of the most challenging tasks for investigators. In orderto test adjunctive therapies rigorously, very large clinicaltrials are needed, and the infrastructure and expertise to im-plement such studies, even if funding were to be madeavailable, is frequently lacking. Thus, to demonstrate a re-duction in mortality with an adjunctive intervention effec-tive at reducing mortality by 20% in severe disease wherethe underlying mortality is z25%, .1000 patients willneed to be enrolled. Recent studies have shown that manyof the surrogate markers that have been considered useful inmonitoring response to therapy in severe malaria may notcorrelate with the most important outcome measure, mortal-ity. Thus, duration of coma, estimates of parasite clearance

Pathophysiology and Supportive Treatment of Severe Malaria 41
time, and even perhaps seizures, although significantly differ-ent between treatment groups in one large study, were not as-sociated with any difference in mortality (Tran et al.,1996b). It is, therefore, inappropriate to generalise from im-provements in surrogate markers of infection (including pe-ripheral parasitaemia) and to anticipate corresponding im-provements in survival. Therefore, interventional studies onsevere malaria designed to assess usefulness in management(as opposed to answering pathophysiological questions or pi-lot Phase II studies), perforce, will have to be sufficientlylarge as to assess mortality, or they should not be conductedat all.
Much of what has been learned about disease mecha-nisms and management of severe malaria has been derivedfrom studies carried out in adults in Southeast Asia. As em-phasised in this review, there are important differences be-tween patterns of disease in African children comparedwith adults. Such differences may reflect age, genotypicvariations, and patterns of transmission, as well as immuno-logical responses. In order to optimise the treatment of se-vere malaria in children, more studies are necessary in thispopulation. These studies should be designed to examinethe pathophysiological basis of severe disease, as well asnewer treatment regimens, particularly adjunctive thera-pies, and are urgently needed. Many prognostic indicators,both laboratory and clinical, are now available to identifychildren at risk of dying from severe infection. In assessingpotentially new indicators that may then point to future in-terventional studies, it is important to relate these indica-tors to those that already have been identified. This ap-proach of assimilating new correlates of severe disease intowhat is already known about infection relies on more diffi-cult statistical techniques. It may be more statistically de-manding, but it is also potentially more valuable in assess-ing a new prognostic indicator’s true value.
The recent advances in understanding the molecular ba-sis of many of the central pathophysiological events in se-vere malaria suggest interventions that are directed at re-versing these processes. We know that antimalarial drugskill parasites, but require hours before they can exert theirmaximum effects. During this time, it may be advantageousto employ interventions that can immediately reverse, forexample, the cytoadherence of PRBCs from capillary bedsin the brains of patients with CM. Such approaches havebeen attempted in the past (the use of hyperimmunoglobu-lin is one example), and a hope for the future is that morespecific therapies guided by current molecular understand-ing may fare better. Before such approaches can be imple-mented at the bedside, however, the importance of manynew and exciting laboratory observations needs to be exam-ined in geographically different patient populations.
Acknowledgements–We thank all of our colleagues with whom we have car-ried out investigations into malaria, in Kenya, Thailand, The Gambia, andGhana, and Professor M. Bland, St. George’s Medical School, for help inconstructing Table 3. CRJCN holds a Wellcome Trust Career Post inTropical Medicine (No. 050533) and SK is a Wellcome Trust Senior Re-search Fellow in Clinical Science.
ReferencesAbdalla, S. H. (1990) Iron and folate status in Gambian children
with malaria. Ann. Trop. Paediatr. 10: 265–272.Abdalla, S. and Weatherall, D. J. (1982) The direct antiglobulin
test in P. falciparum malaria. Br. J. Haematol. 51: 415–425.Abdalla, S., Weatherall, D. J., Wickramasinghe, S. N. and
Hughes, M. (1980) The anaemia of P. falciparum malaria. Br. J.Haematol. 46: 171–183.
Abdalla, S. H., Kasili, F. G. and Weatherall, D. J. (1983) TheCoombs direct antiglobulin test in Kenyans. Trans. R. Soc.Trop. Med. Hyg. 77: 99–102.
Adams, J. H., Sim, B. K., Dolan, S. A., Fang, X., Kaslow, D. C. andMiller, L. H. (1992) A family of erythrocyte binding proteins ofmalaria parasites. Proc. Natl. Acad. Sci. USA 89: 7085–7089.
Agbenyega, T., Angus, B., Bedu-Addo, G., Baffoe-Bonnie, B.,Griffin, G., Vallance, P. and Krishna, S. (1997) Plasma nitro-gen oxides and blood lactate concentrations in Ghanaian chil-dren with malaria. Trans. R. Soc. Trop. Med. Hyg. 91: 298–302.
Ahmad, S. H., Moonis, R., Kidwai, T., Khan, T. A., Khan, H. M.and Shahab, T. (1986) Cerebral malaria in children. 53:409–413.
Aikawa, M. (1988) Human cerebral malaria. Am. J. Trop. Med.Hyg. 39: 3–10.
Aikawa, M., Suzuki, M. and Gutierrez, Y. (1980) Pathology ofmalaria. In: Malaria. Pathology, Vector Studies, and Culture,Vol. 2, pp. 47–102, Kreier, J. P. (ed.) Academic Press, New York.
Akpede, G. O., Sykes, R. M. and Abiodun, P. O. (1993) Convul-sions with malaria: febrile or indicative of cerebral involve-ment? J. Trop. Pediatr. 39: 350–355.
Allan, R. J., Rowe, A. and Kwiatkowski, D. (1993) Plasmodium fal-ciparum varies in its ability to induce tumor necrosis factor.Infect. Immun. 61: 4772–4776.
Allan, R. J., Beattie, P., Bate, C., van Hensbroek, M. B., Morris-Jones, S., Greenwood, B. M. and Kwiatkowski, D. (1995) Strainvariation in tumor necrosis factor induction by parasites fromchildren with acute falciparum malaria. Infect. Immun. 63:1173–1175.
Allen, S. J., O’Donnell, A., Alexander, N. D. E. and Clegg, J. B.(1996a) Causes of coma in children with malaria in Papua NewGuinea. Lancet 348: 1168–1169.
Allen, S. J., O’Donnell, A., Alexander, N. D. E. and Clegg, J. B.(1996b) Severe malaria in children in Papua New Guinea. Q. J.Med. 89: 779–788.
Alonso, P. L., Smith, T., Armstrong Schellenberg, J. R., Masanja,H., Mwankuyse, S., Urassa, H., de Azevedo, I. B., Chongela, J.,Kobero, S. and Menendez, C. (1994) Randomised trial of effi-cacy of SPf66 vaccine against Plasmodium falciparum malaria inchildren in southern Tanzania. Lancet 344: 1175–1181.
Al Yaman, F. M., Genton, B., Mokela, D., Raiko, A., Kati, S.,Rogerson, S., Reeder, J. and Alpers, M. (1995) Human cerebralmalaria: lack of significant association between erythrocyterosetting and disease severity. Trans. R. Soc. Trop. Med. Hyg.89: 55–58.
Al Yaman, F. M., Mokela, D., Genton, B., Rockett, K. A., Alpers,M. P. and Clark, I. A. (1996) Association between serum levelsof reactive nitrogen intermediates and coma in children withcerebral malaria in Papua New Guinea. Trans. R. Soc. Trop.Med. Hyg. 90: 270–273.
Al Yaman, F. M., Rockett, K. A. and Clark, I. A. (1997) Reactivenitrogen intermediates and cerebral malaria: a reply. Trans. R.Soc. Trop. Med. Hyg. 91: 92–93.

42 C. R. J. C. Newton and S. Krishna
Angus, B. J., Thanikkul, K., Silamut, K., White, N. J. and Udom-sangpetch, R. (1996) Short report: rosette formation in Plasmo-dium ovale infection. Am. J. Trop. Med. Hyg. 55: 560–561.
Anonymous (1976) Renal lesions in human malaria. Br. Med. J.272: 132.
Anonymous (1987) Man over monkey [editorial]. Lancet i: 1016.Anstey, N. M., Weinberg, J. B., Hassanali, M. Y., Mwaikambo, E. D.,
Manyenga, D., Misukonis, M. A., Arnelle, D. R., Hollis, D.,McDonald, M. I. and Granger, D. L. (1996) Nitric oxide inTanzanian children with malaria: inverse relationship betweendisease severity and nitric oxide production/nitric oxide syn-thetase type 2 expression. J. Exp. Med. 184: 557–567.
Arieff, A. I. and Griggs, R. C. (1994) General considerations inmetabolic encephalopathies and systemic disorders affectingthe nervous system. In: Metabolic Brain Dysfunction in Sys-temic Disorders, pp. 1–20, Arieff, A. I. and Griggs, R. C. (eds.)Little, Brown & Company, Boston.
Armengaud, M., Louvain, M. and Diop-Mar, L. (1962) Étudepourtant sur 448 cas de paludisme chez l’Africain de la régionDakaroïse. Bull. Soc. Med. Afr. Noire Lang. Fr. 7: 167–169.
Aung-Kyaw-Zaw, Khin-Maung-U, and Myo-Thwe (1988) Endo-toxaemia in complicated falciparum malaria. Trans. R. Soc.Trop. Med. Hyg. 82: 513–514.
Badibanga, B., Dayal, R., Depierreux, M., Pidival, G. and Lambert,P. H. (1986) Étude des principaux facteurs immunologiques etde la barrière hemato-meniné, au cause de la malaria cérébralechez l’enfant en pays d’endemie (Zaire). Ann. Soc. Belg. Med.Trop. 66: 23–37.
Baier-Bitterlich, G., Fuchs, D., Murr, C., Reibnegger, G., Werner-Felmayer, G., Sgonc, R., Bock, G., Dierich, M. and Wachter,H. (1995) Effect of neopterin and 7,8,dihydroneopterin ontumor necrosis factor-a induced programmed cell death. FEBSLett. 364: 234–238.
Barennes, H., Pussard, E., Mahaman Sani, A., Clavier, F., Kahia-tani, F., Granic, G., Henzel, D., Ravinet, L. and Verdier, F.(1996) Efficacy and pharmacokinetics of a new intrarectal qui-nine formulation in children with Plasmodium falciparummalaria. Br. J. Clin. Pharmacol. 41: 389–395.
Baruch, D. I., Pasloske, B. L., Singh, H. B., Bi, X., Ma, X. C., Feld-man, M., Taraschi, T. F. and Howard, R. J. (1995) Cloning theP. falciparum gene encoding PfEMP1, a malarial variant anti-gen and adherence receptor on the surface of parasitized humanerythrocytes, Cell 82: 77–87.
Bate, C. A. and Kwiatkowski, D. (1994) Inhibitory immunoglobu-lin M antibodies to tumor necrosis factor-inducing toxins inpatients with malaria. Infect. Immun. 62: 3086–3091.
Bell, D. R., Reid, H. A. and Stephens, A. J. (1976) Parasites whichmigrate to the brain [letter]. Lancet i: 1292.
Berclaz, P. Y., Benedek, C., Jequier, E. and Schutz, Y. (1996)Changes in protein turnover and resting energy expenditureafter treatment of malaria in Gambian children. Pediatr. Res.39: 401–409.
Berendt, A. R., Turner, G. D. H. and Newbold, C. I. (1994) Cere-bral malaria: the sequestration hypothesis. Parasitol. Today 10:412–413.
Berman, W., Pizzi, F., Schut, L., Raphaely, R. and Holtzapple, P.(1975) The effects of exchange transfusion on intracranial pres-sure in patients with Reye syndrome. J. Pediatr. 87: 887–891.
Bernadino, L. and River, R. P. (1986) Análise de 254 internamen-tos por malária cerebral em crianças dos 0–9 anos noprimeiro semestre de 1986 no serviço de pediatra do Hospi-tal Josina Machel de Luanda. Acta. Med. Ang. 5: 61–69.
Berner, H. (1975) Malaria bei Kindern unter besonderer berück-sichtigung der Cerebralen Malaria. Klin. Paediatr. 187: 401–406.
Bethell, D. B., Phuong, P. T., Phuong, C. X., Nosten, F., Waller,D., Davis, T. M., Day, N. P., Crawley, J., Brewster, D., Pukrit-tayakamee, S. and White, N. J. (1996) Electrocardiographicmonitoring in severe falciparum malaria. Trans. R. Soc. Trop.Med. Hyg. 90: 266–269.
Bloland, P. B., Lackritz, E. M., Kazembe, P. N., Were, J. B., Steke-tee, R. and Campbell, C. C. (1993) Beyond chloroquine: impli-cations of drug resistance for evaluating malaria therapy efficacyand treatment policy in Africa. J. Infect. Dis. 167: 932–937.
Bonadio, W. A. (1992) The cerebrospinal fluid: physiologicaspects and alterations associated with bacterial meningitis.Pediatr. Infect. Dis. J. 11: 423–432.
Bondi, F. S. (1992) The incidence and outcome of neurologicalabnormalities in childhood cerebral malaria: a long term follow-up of 62 surviviors. Trans. R. Soc. Trop. Med. Hyg. 86: 17–19.
Boonpucknavig, V. and Boonpucknavig, S. (1988) The histopa-thology of malaria. In: Malaria. Principles and Practice ofMalariology, pp. 674–708, Wernsdorfer, W. H. and McGregor,I. A. (eds.) Churchill Livingstone, Edinburgh.
Brandts, C. H., Ndjave, M., Graninger, W. and Kremsner, P. G.(1997) Effect of paracetamol on parasite clearance time in Plas-modium falciparum malaria. Lancet 350: 704–709.
Brewster, D. R., Kwiatkowski, D. and White, N. J. (1990) Neuro-logical sequelae of cerebral malaria in children. Lancet 336:1039–1043.
Brown, D. A., Brown, F., Ganz, E. and Huttenlocher, P. R. (1978)Treatment of elevated intracranial pressure in Reye syndrome.Ann. Neurol. 4: 275–278.
Brown, M. M. and Marshall, J. (1985) Regulation of cerebralblood flow in response to changes in blood viscosity. Lancet i:604–609.
Brown, N. (1995) Severe malaria in children at Port Moresby gen-eral hospital, Papua New Guinea. Trop. Geog. Med. 47: 107–110.
Burchard, G. D., Radloff, P., Phillips, J., Nyemi, M., Knobiock, J.and Kremsner, P. G. (1995) Increased erythropoietin produc-tion in children with severe malarial anemia. Am. J. Trop. Med.Hyg. 53: 547–551.
Burgmann, H., Looareesuwan, S., Kapiotis, S., Viravan, C., Vani-janonta, S., Hollenstein, U., Wiesinger, E., Presterl, E., Win-kler, S. and Graninger, W. (1996) Serum levels of erythropoietinin acute Plasmodium falciparum malaria. Am. J. Trop. Med. Hyg.54: 280–283.
Byass, P., Campbell, H., O’Dempsey, T. J. and Greenwood, B. M.(1991) Coincidence of malaria parasitaemia and abnormalchest X-ray findings in young Gambian children. J. Trop. Med.Hyg. 94: 22–23.
Carlson, J. (1993) Erythrocyte rosetting in Plasmodium falciparummalaria—with special reference to the pathogenesis of cerebralmalaria. Scand. J. Infect. Dis. Suppl. 86: 1–79.
Carlson, J., Helmby, H., Hill, A. V. S., Brewster, D., Green-wood, B. M. and Wahlgren, M. (1990) Human cerebral malaria:association with erythrocyte rosetting and lack of anti-rosettingantibodies. Lancet 336: 1457–1460.
Carlson, J., Nash, G. B., Gabutti, V., al Yaman, F. and Wahlgren,M. (1994) Natural protection against severe Plasmodium falci-parum malaria due to impaired rosette formation. Blood 84:3909–3914.
Carme, B., Bouquety, J. C. and Plassart, H. (1993) Mortality andsequelae due to cerebral malaria in African children in Brazza-ville. Am. J. Trop. Med. Hyg. 48: 216–221.

Pathophysiology and Supportive Treatment of Severe Malaria 43
Chapel, H. M., Warrell, D. A., Looareesuwan, S., White, N. J.,Phillips, R. E., Warrell, M. J., Supawanta, V. and Tharavanij, S.(1987) Intrathecal immunoglobulin synthesis in cerebral malaria.Clin. Exp. Immunol. 67: 524–530.
Clark, H. C. and Tomlinson, W. J. (1949) The pathological anat-omy of malaria. In: Clinical Malariology, pp. 874–883, Boyd, M.F. (ed.) W.B. Saunders, Philadelphia.
Clark, I. A. (1978) Does endotoxin cause both the disease andparasite death in acute malaria and babesiosis? Lancet ii: 75–77.
Clark, I. and Chaudhri, G. (1988) Tumour necrosis factor maycontribute to the anaemia of malaria by causing dyserythropoie-sis and erythrophagocytosis. Br. J. Haematol. 70: 99–103.
Clark, I. A. and Hunt, N. H. (1983) Evidence for reactive oxygenintermediates causing hemolysis and parasite death in malaria.Infect. Immun. 39: 1–6.
Clark, I. A. and Rockett, K. A. (1994) The cytokine theory ofhuman cerebral malaria. Parasitol. Today 10: 410–412.
Clark, I. A., Cowden, W. B., Butcher, G. A. and Hunt, N. H.(1983) Free oxygen radicals in malaria [letter]. Lancet i: 359–360.
Clark, I. A., Hunt, N. M. and Cowden, W. B. (1986) Oxygen-derived free radicals in the pathogenesis of parasitic disease.Adv. Parasitol. 25: 1–44.
Clark, I. A., Cowden, W. B., Butcher, G. A. and Hunt, N. H.(1987) Possible roles of tumor necrosis factor in the pathologyof malaria. Am. J. Pathol. 127: 192–198.
Clark, I. A., Rockett, K. A. and Cowden, W. B. (1991) Role ofTNF in cerebral malaria. Lancet 337: 302–303.
Clark, I. A., Rockett, K. A. and Cowden, W. B. (1992) Possiblecentral role of nitric oxide in conditions clinically similar tocerebral malaria. Lancet 340: 894–896.
Collomb, H., Rey, M., Dumas, M., Nouhouayi, A. and Petit, M.(1967) Les hémiplegies au cours du paludisme aigu. Bull. Soc.Med. Afr. Noire. Lang. Fr. 7: 791–795.
Commey, J. O. (1984) Is it cerebral malaria? [letter] Lancet ii:1037.
Commey, J. O., Mills-Tetteh, D. and Phillips, B. J. (1980) Cere-bral malaria in Accra, Ghana. Ghana Med. J. 19: 68–72.
Cooke, B. M., Morris-Jones, S., Greenwood, B. M. and Nash,G. B. (1993) Adhesion of parasitized red blood cells to culturedendothelial cells: a flow-based study of isolates from Gambianchildren with falciparum malaria. Parasitology 107: 359–368.
Cooke, B. M., Morris-Jones, S., Greenwood, B. M. and Nash, G.B. (1995) Mechanisms of cytoadhesion of flowing, parasitizedred blood cells from Gambian children with falciparum malaria.Am. J. Trop. Med. Hyg. 53: 29–35.
Cot, S., Ringwald, P., Mulder, B., Miailhes, P., Yap-Yap, J., Nus-sler, A. K. and Eling, W. M. (1994) Nitric oxide in cerebralmalaria [letter]. J. Infect. Dis. 169: 1417–1418.
Coulter, J. B. S. (1991) Lumbar puncture for cerebral malaria. Afr.Health November: 27.
Crawley, J., Smith, S., Kirkham, F. J., Muthinji, P., Waruiru, C.and Marsh, K. (1996) Seizures and status epileticus in child-hood cerebral malaria. Q. J. Med. 89: 591–597.
Cropper, J. (1908) Phenomenal abundance of parasites in a fatalcase of pernicious malaria. Lancet ii: 16–17.
D’Alessandro, U., Leach, A., Drakeley, C. J., Bennett, S., Olaleye,B. O., Fegan, G. W., Jawara, M., Langerock, P., George, M. O.,Targett, G. A. and Greenwood, B. M. (1995a) Efficacy trial ofmalaria vaccine SPf66 in Gambian infants. Lancet 346: 462–467.
D’Alessandro, U., Olaleye, B. O., McGuire, W., Langerock, P.,Bennett, S., Aikins, M. K., Thomson, M. C., Cham, M. K.,Cham, B. A. and Greenwood, B. M. (1995b) Mortality and
morbidity from malaria in Gambian children after introductionof an impregnated bednet programme. Lancet 345: 479–483.
D’Alessandro, U., Olaleye, B. O., McGuire, W., Thomson, M. C.,Langerock, P., Bennett, S. and Greenwood, B. M. (1995c) Acomparison of the efficacy of insecticide-treated and untreatedbed nets in preventing malaria in Gambian children. Trans. R.Soc. Trop. Med. Hyg. 89: 596–598.
Das, B. S., Mohanty, S., Mishra, S. K., Patnaik, J. K., Satpathy, S. K.,Mohanty, D. and Bose, T. K. (1991) Increased cerebrospinalfluid protein and lipid peroxidation products in patients withcerebral malaria. Trans. R. Soc. Trop. Med. Hyg. 85: 733–734.
Davis, T. M. E., Krishna, S., Looareesuwan, S., Supanaranond, W.,Pukrittayakamee, S., Attatamsoonthorn, K. and White, N. J.(1990a) Erythrocyte sequestration and anemia in severe falci-parum malaria. J. Clin. Invest. 86: 793–800.
Davis, T. M. E., Pukrittayakamee, S., Supanaranond, W., Looaree-suwan, S., Krishna, S., Nagachinta, B., Turner, R. C. andWhite, N. J. (1990b) Glucose metabolism in quinine-treatedpatients with uncomplicated falciparum malaria. Clin. Endo-crinol. (Oxf.) 33: 739–749.
Davis, T. M. E., Pukrittayakamee, S., Woodhead, J. S., Holloway,P., Chaivisuth, B. and White, N. J. (1991) Calcium and phos-phate metabolism in acute falciparum malaria. Clin. Sci. 81:297–304.
Davis, T. M. E., Suputtamongkol, Y., Spencer, J. L., Ford, S.,Chienkul, N., Schulenburg, W. E. and White, N. J. (1992)Measures of capillary permeability in acute falciparum malaria:relation to severity of infection and treatment. Clin. Infect. Dis.15: 256–266.
Davis, T. M. E., Looareesuwan, S., Pukrittayakamee, S., Levy, J. C.,Nagachinta, B. and White, N. J. (1993) Glucose turnover insevere falciparum malaria. Metabolism 42: 334–340.
Davis, T. M. E., Suputtamongkol, Y., Spencer, J. L., Wilson, S. G.,Mekhton, S., Croft, K. D. and White, N. J. (1994) Glucoseturnover in pregnant women with acute malaria. Clin. Sci. 86:83–90.
Davis, T. M. E., Benn, J. J., Supputamangkol, Y., Weinberg, J.,Umpleby, A. M., Chierakul, N. and White, N. J. (1996) Lac-tate turnover and forearm lactate metabolism in severe falci-parum malaria. Endocrinol. Metab. 3: 105–115.
Day, N. P., Phu, N. H., Bethell, D. P., Mai, N. T., Chau, T. T.,Hien, T. T. and White, N. J. (1996) The effects of dopamineand adrenaline infusions on acid-base balance and systemichaemodynamics in severe infection. Lancet 348: 219–223.
Dekker, E., Romijn, J. A., Waruiru, C., Ackermans, M. T., Wever-ling, G. J., Sauerwein, R. W., Endert, E., Peshu, N., Marsh, K.and Sauerwein, H. P. (1996) The relationship between glucoseproduction and plasma glucose concentration in children withfalciparum malaria. Trans. R. Soc. Trop. Med. Hyg. 90: 654–657.
Dekker, E., Romijn, J. A., Moeniralam, H. S., Waruiru, C. M.,Ackermans, M. T., Timmer, J. G., Endert, E., Peshu, N., Marsh,K. and Sauerwein, H. P. (1997) The influence of alanine infu-sion on glucose production in “malnourished” African childrenwith falciparum malaria. Q. J. Med. 90: 455–460.
Delacollette, C., Taelman, H. and Wery, M. (1995) An etiologicstudy of hemoglobinuria and blackwater fever in the KivuMountains, Zaire. Ann. Soc. Belg. Med. Trop. 75: 51–63.
Deloron, P., Dumont, N., Nyongabo, T., Aubry, P., Astagneau, P.,Ndarugirire, F., Menetrier-Caux, C., Burdin, N., Brelivet, J. C.and Peyron, F. (1994) Immunologic and biochemical alter-ations in severe falciparum malaria: relations to neurologicalsymptoms and outcome. Clin. Infect. Dis. 19: 480–485.

44 C. R. J. C. Newton and S. Krishna
de Naotunne, T., Karunaweera, N. D., Mendis, K. N. and Carter, R.(1993) Cytokine-mediated inactivation of malarial gametocytesis dependent on the presence of white blood cells and involvesreactive nitrogen intermediates. Immunology 78: 555–562.
Descamps Latscha, B., Lunel Fabiani, F., Kara Binis, A. andDruilhe, P. (1987) Generation of reactive oxygen species inwhole blood from patients with acute falciparum malaria. Para-site Immunol. 9: 275–279.
de Silva, H. J., de Silva, N. R. and Snook, J. A. (1992) Delayedcerebellar ataxia following falciparum malaria: lack of evidencefor antibody mediation. Trans. R. Soc. Trop. Med. Hyg. 86: 608.
Dhayagude, R. G. and Purandare, M. B. (1943) Autopsy study ofcerebral malaria with special reference to malarial granuloma.Arch. Pathol. 36: 550–558.
Di Perri, G., Di Perri, I. G., Monteiro, G. B., Bonora, S., Hennig,C., Cassatella, M., Micciolo, R., Vento, S., Dusi, S., Bassetti, D.and Concia, E. (1995) Pentoxifylline as a supportive agent inthe treatment of cerebral malaria in children. J. Infect. Dis. 171:1317–1322.
Dobbie, M., Crawley, J., Waruiru, C., Marsh, K. and Surtees, R.(1997) Cerebrospinal fluid concentrations of quinolinic acid,total neopterin and nitrate plus nitrite in Kenyan childrenrecovering from cerebral malaria. J. Neurochem. 69: 5181.
Dondorp, A. M., Angus, B. J., Hardeman, M. R., Chotivanich,K. T., Silamut, K., Ruangveerayuth, R., Kager, P. A., White,N. J. and Vreeken, J. (1997) Prognostic significance of reducedred cell deformability in severe falciparum malaria. Am. J. Trop.Med. Hyg. 57: 507–511.
Dorn, A., Stoffel, R., Matile, H., Bebndorf, A. and Ridley, R.(1995) Malaria haemozoin/b-haematin supports haem polymer-ization in the absence of protein. Nature 374: 269–271.
Dubey, M. L., Rai, S. K., Ganguly, N. K., Kalra, A., Varma, S. C.and Mahajan, R. C. (1991) Generation of reactive oxygen spe-cies by blood monocytes in human Plasmodium falciparum andP. vivax infections. APMIS 99: 210–212.
Dudgeon, L. S. and Clarke, C. (1917) A contribution to themicroscopical histology of malaria. Lancet ii: 153–156.
Edington, G. M. (1967) Pathology of malaria in West Africa. Br.Med. J. 1: 715–718.
Edington, G. M. and Gilles, H. M. (1976) Malaria. In: Pathologyin the Tropics, pp. 20–23, Edward Arnold, London.
Elford, B. C., Cowan, G. M. and Ferguson, D. J. (1995) Parasite-regulated membrane transport processes and metabolic controlin malaria infected erythrocytes. Biochem. J. 308: 361–374.
English, M., Marsh, V., Amukoye, E., Lowe, B., Murphy, S. andMarsh, K. (1996a) Chronic salicylate poisoning and severemalaria. Lancet 347: 1736–1737.
English, M. C., Waruiru, C., Lightowler, C., Murphy, S. A.,Kirigha, G. and Marsh, K. (1996b) Hyponatraemia and dehy-dration in severe malaria. Arch. Dis. Child. 74: 201–205.
English, M., Waruiru, C. and Marsh, K. (1996c) Transfusion forrespiratory distress in life-threatening childhood malaria. Am. J.Trop. Med. Hyg. 55: 525–530.
English, M., Sauerwein, R. W., Waruiru, C. M., Mosobo, M., Obi-ero, J., Lowe, B. and Marsh, K. (1997) Acidosis in severe child-hood malaria. Q. J. Med. 90: 263–270.
Eross, J., Sihnu, M. and Dorman, D. (1981) Cerebrospinal fluid lacticacidosis in bacterial meningitis. Arch. Dis. Child. 56: 692–698.
Facer, C. A., Bray, R. S. and Brown, J. (1979) Direct Coombsantiglobulin reactions in Gambian children with Plasmodiumfalciparum malaria. I. Incidence and class specificity. Clin. Exp.Immunol. 35: 119–127.
Faero, O., Kastrup, K. W., Lykkegaard-Nielsen, E., Melchior, J. C.and Thorn, I. (1972) Successful prophylaxis of febrile convul-sions with phenobarbital. Epilepsia 13: 279–285.
Fisher, C. W. S. (1983) Clinical curio: acidosis and hypoglycaemiain malaria. Br. Med. J. 286: 1261.
Fitz-Hugh, T. (1944) The cerebral form of malaria. Bull. US ArmyMed. Dept. 83: 39–48.
Fraser, A. and Evan, G. (1996) A license to kill. Cell 85: 781–784.Friedland, J. S., Ho, M., Remick, D. G., Bunnag, D., White,
N. J. and Griffin, G. E. (1993) Interleukin-8 and Plasmodiumfalciparum malaria in Thailand. Trans. R. Soc. Trop. Med.Hyg. 87: 54–55.
Gaskell, J. F. and Miller, W. L. (1920) Studies on malignantmalaria in Macedonia. Q. J. Med. 13: 381–426.
Gelfand, M. (1973) Neurological complications of parasitic dis-ease. In: Tropical Neurology, pp. 247–251, Spillane, J. D. (ed.)Oxford University Press, London.
Genton, B., Al-Yaman, F., Alpers, M. P. and Mokein, D. (1997)Indicators of fatal outcome in paediatric cerebral malaria: astudy of 134 comatose Papua New Guinean children. Int. J.Epidemiol. 26: 670–676.
Go, K. G. (1991) Cerebral Pathophysiology: An Integral Approachwith Some Emphasis on Clinical Applications. Elsevier SciencePublishers B.V., Amsterdam.
Goitein, K. J., Fainmesser, P. and Sohmer, H. (1983) Cerebral per-fusion pressure and auditory brain-stem responses in childhoodCNS diseases. Am. J. Dis. Child. 137: 777–781.
Gopinathan, V. P. and Subramanian, A. R. (1986) Vivax and fal-ciparum malaria seen at an Indian service hospital. J. Trop.Med. Hyg. 89: 51–55.
Gordeuk, V., Thuma, P., Brittenham, G., McLaren, C., Parry, D.,Backenstose, A., Biemba, G., Msiska, R., Holmes, L., McKin-ley, E., Vargas, L., Gilkeson, R. and Poltera, A. A. (1992) Effectof iron chelation therapy on recovery from deep coma in chil-dren with cerebral malaria. N. Engl. J. Med. 327: 1473–1477.
Gordeuk, V. R., Thuma, P. E., McLaren, C. E., Biemba, G., Zulu,S., Poltera, A. A., Askin, J. E. and Brittenham, G. M. (1995)Transferrin saturation and recovery from coma in cerebralmalaria. Blood 85: 3297–3301.
Gozal, D. (1992) The incidence of pulmonary manifestations dur-ing Plasmodium falciparum malaria in non immune subjects.Trop. Med. Parasitol. 43: 6–8.
Grau, G. E., Piguet, P. F., Engers, H. D., Louis, J. A., Vassalli, P.and Lambert, P. H. (1986) L3T41 T lymphocytes play a majorrole in the pathogenesis of murine cerebral malaria. J. Immunol.137: 2348–2354.
Grau, G. E., Fajardo, L. F., Piguet, P. F., Allet, B., Lambert, P. H. andVassalli P. (1987a) Tumor necrosis factor (cachectin) as an essen-tial mediator in murine cerebral malaria. Science 237: 1210–1212.
Grau, G. E., Gretener, D. and Lambert, P. H. (1987b) Preventionof murine cerebral malaria by low-dose cyclosporin A. Immu-nology 61: 521–525.
Grau, G. E., Piguet, P. F., Vassalli, P. and Lambert, P. H. (1989)Involvement of tumour necrosis factor and other cytokines inimmune-mediated vascular pathology. Int. Arch. Allergy Appl.Immunol. 88: 34–39.
Greenberg, A. E., Ntumbanzondo, M., Ntula, N., Mawa, L., How-ell, J. and Davachi, F. (1989) Hospital-based surveillance ofmalaria-related paediatric morbidity and mortality in Kinshasa,Zaire. Bull. WHO 67: 189–196.
Greenwood, B. M. (1991) Cerebral malaria [letter]. Lancet 337: 1282.Greenwood, B. (1996) Fever and malaria. Lancet 248: 280–281.

Pathophysiology and Supportive Treatment of Severe Malaria 45
Greenwood, B. M. (1997) Malaria transmission and vector con-trol. Parasitol. Today 13: 90–92.
Greenwood, B. M., Stratton, D., Williamson, W. A. and Moham-med, I. (1978) A study of the role of immunological factors inthe pathogenesis of the anaemia of acute malaria. Trans. R.Soc. Trop. Med. Hyg. 72: 378–385.
Guignard, J. (1965) Le paludisme pernicieux du nourrisson et del’enfant. Ann. Pediatr. (Paris) 41: 2474–2484.
Heinemeyer, G. (1987) Clinical pharmacokinetic considerationsin the treatment of increased intracranial pressure. Clin. Phar-macokinet. 13: 1–25.
Hemmer, C. J., Bierhaus, A., Riedesel, J., Gabat, S., Lilensiek, B.,Pitronik, P., Lin, J., Grauer, A., Amiral, J., Zielger, R., Schief-fer, S., Kern, P., Egbring, R., Dietricj, M. and Nawroth, P. P.(1994) Elevated thrombomodulin plasma levels as a result ofendothelial involvement in Plasmodium falciparum malaria.Thromb. Haemost. 72: 457–464.
Hemmer, C. J., Hort, G., Chiwakata, C. B., Seitz, R., Egbring, R.,Gaus, W., Hogel, J., Hassemer, M., Nawroth, P. P., Kern, P. andDietrich, M. (1997) Supportive pentoxifylline in falciparummalaria: no effect on tumour necrosis factor alpha levels or clin-ical outcome: a prospective, randomized, placebo-controlledstudy. Am. J. Trop. Med. Hyg. 56: 397–403.
Hero, M., Harding, S. P., Riva, C. E., Winstanley, P. A., Peshu, N.and Marsh, K. (1997) Photographic and angiographic charac-terization of the retina of Kenya children with severe malaria.Arch. Ophthalmol. 115: 997–1103.
Hershko, C. and Peto, T. E. (1988) Desferroxamine inhibition ofmalaria is independent of host iron status. J. Exp. Med. 168:375–387.
Hien, T. T. (1994) An overview of the clinical use of artemisininand its derivatives in the treatment of falciparum malaria in VietNam. Trans. R. Soc. Trop. Med. Hyg. 88 (Suppl. 1): S7–S8.
Hien, T. T. and White, N. J. (1993) Qinghaosu. Lancet 341: 603–608.
Ho, M., Davis, T. M. E., Silamut, K., Bunnag, D. and White, N. J.(1991) Rosette formation of Plasmodium falciparum-infectederythrocytes from patients with acute malaria. Infect. Immun.59: 2135–2139.
Hoffman, S. L., Rustama, D., Punjabi, N. H., Surampaet, B., San-jaya, B., Dimpudus, A. J., McKee, K. T., Jr., Paleologo, F. P.,Campbell, J. R., Marwoto, H. and Laughlin, L. (1988) High-dose dexamethasone in quinine-treated patients with cerebralmalaria: a double-blind, placebo-controlled trial. J. Infect. Dis.158: 325–331.
Hoffman, W. H., Steinhart, C. M., Gammal, T. E., Steele, S.,Cuadrado, A. R. and Morse, P. K. (1988) Cranial CT in chil-dren and adolescents with diabetic ketoacidosis. Am. J. Neuro-radiol. 9: 733–739.
Holloway, P. A. H., Krishna, S. and White, N. J. (1991) Plasmo-dium berghei: lactic acidosis and hypoglycaemia in a rodentmodel of severe malaria; effects of glucose, quinine, anddichloroacetate. Exp. Parasitol. 72: 1–11.
Holloway, P. A. H., Knox, K., Bajaj, N., Chapman, D., White, N. J.,O’Brien, R., Stacpoole, P. W. and Krishna, S. (1995) Plasmodiumberghei infection: dichloroacetate improves survival in rats withlactic acidosis. Exp. Parasitol. 80: 624–632.
Howard, R. J., Handunnetti, S. M., Hasler, T., Gilladoga, A., deAguiar, J. C., Pasloske, B. L., Morehead, K., Albrecht, G. R.and van Schravendijk, M. R. (1990) Surface molecules on Plas-modium falciparum-infected erythrocytes involved in adherence.Am. J. Trop. Med. Hyg. 43: 15–29.
Hurn, P. D., Kirsch, J. R.. Helfaer, M. A. and Traystman. R. J.(1996) Brain damage and free radicals. In: Tissue Perfusion andOrgan Function: Ischemia/Reperfusion Injury, pp. 71–84,Kamada, T., Shiga, T. and McCuskey, R. S. (eds.) Elsevier,Amsterdam.
Ikpatt, N. W., Asindi, A. A., Ekanem, I. A. and Khalil, M. I.(1990) Preliminary observations on cerebral malaria in Nige-rian children. East Afr. Med. J. 67: 341–347.
Jakobsen, P. H., McKay, V., Morris-Jones, S. D., McGuire, W.,van Hensbroek, M. B., Meisner, S., Bendtzen, K., Schousboe, I.,Bygbjerg, I. C. and Greenwood, B. M. (1994) Increased con-centrations of interleukin-6 and interleukin-1 receptor antago-nist and decreased concentrations of beta-2-glycoprotein I inGambian children with cerebral malaria. Infect. Immun. 62:4374–4379.
Janota, I. and Doshi, B. (1979) Cerebral malaria in the UnitedKingdom. J. Clin. Pathol. 32: 769–772.
Jeje, O. M., Kelton, J. G. and Blajchman, M. A. (1983) Quantita-tion of red cell membrane associated immunoglobulin in chil-dren with Plasmodium falciparum parasitaemia. Br. J. Haematol.54: 567–572.
Jones, E. S. and McGregor, I. A. (1954) Pathological processes indisease. V. Blood physiology of Gambian children infected withPlasmodium falciparum. Ann. Trop. Med. Parasitol. 48: 95–101.
Kanaani, J. and Ginsburg, H. (1991) Transport of lactate in Plas-modium falciparum-infected human erythrocytes. J. Cell Biol.149: 469–476.
Karunaweera, N. D., Grau, G. E., Gamage, P., Carter, R. and Men-dis, K. N. (1992) Dynamics of fever and serum TNF levels areclosely associated during clinical paroxysms in Plasmodium vivaxmalaria. Proc. Natl. Acad. Sci. USA 89: 3200–3203.
Kataoka, K., Okuno, T., Mikawa, H. and Hojo, H. (1988) Cranialcomputed tomographic and electroencephalographic abnormal-ities in children with post-hemiconvulsive hemiplegia. Eur.Neurol. 28: 279–284.
Kaul, D. K., Roth, E. F., Ngel, R. L., Howard, R. J. and Handun-netti, S. M. (1991) Rosetting of Plasmodium falciparum-infectedred blood cells with uninfected red blood cells enhances microvas-cular obstruction under flow conditions. Blood 78: 812–819.
Kawo, N. G., Msengi, A. E., Swai, A. B. M., Chuwa, L. M.,Alberti, K. G. M. M. and McLarty, D. G. (1990) Specificity ofhypoglycaemia for cerebral malaria in children. Lancet 336:454–457.
Kayembe, D., Maertens, K. and De Laey, J. J. (1980) Complica-tions oculaires de la malaria cérébrale. Bull. Soc. Belge. Ophtal-mol. 190: 53–60.
Kelton, J. G., Keystone, J., Moore, J., Denomme, G., Tozman, E.,Glynn, M., Neame, P. B., Gauldie, J. and Jensen, J. (1983)Immune-mediated thrombocytopenia in malaria. J. Clin. Invest.71: 832–836.
Kern, P., Hemmer, C. J., Van Dame, J., Gruss, H. J. and Dietrich,M. (1989) Elevated tumor necrosis factor alpha and interleu-kin-6 serum levels as markers for complicated Plasmodium falci-parum malaria. Am. J. Med. 87: 139–143.
Khan, N. U. and Durham, M. D. (1945) Cerebral malaria. J. R.Army Med. Corps 84: 263–267.
Kingston, M. E. (1971) Experience with urea in invert sugar for thetreatment of cerebral malaria. J. Trop. Med. Hyg. 74: 249–252.
Kirkham, F. J. (1991) Intracranial pressure and cerebral blood flowin non-traumatic coma in childhood. In: Problems of Intracra-nial Pressure in Childhood, pp. 283–348, Minns, R. A. (ed.)Mac Keith Press, London.

46 C. R. J. C. Newton and S. Krishna
Kirkham, F. J., Newton, C. R. J. C., Winstanley, P. A., Pasvol, G.,Peshu, N., Warrell, D. A. and Marsh, K. (1991) Cerebralmalaria. Lancet 337: 1282–1283.
Kirkham, F. J., Newton, C. R. J. C., Winstanley, P. A., Peshu, N.and Marsh, K. (1994) Crises d’epilepsie dans le paludisme cere-bral. In: Neurologie Tropicale, pp. 381–382, Dumas, M., Gior-dano, C., Gentilini, M. and Chieze, F. (eds.) John Libbey &Company, Paris.
Kremsner, P. G., Grundmann, H., Neifer, S., Sliwa, K., Sahlmuller,G., Hegenscheid, B. and Bienzle, U. (1991) Pentoxifylline pre-vents murine cerebral malaria. J. Infect. Dis. 164: 605–608.
Krishna, S. and White, N. J. (1989) Management of severe malar-ial infection. Indian J. Pediatr. 56: 155–163.
Krishna, S. and White, N. J. (1996) Pharmacokinetics of quinine,chloroquine and amodiaquine. Clinical implications. Clin.Pharmacokinet. 30: 263–299.
Krishna, S., Shoubridge, E. A., White, N. J., Weatherall, D. J. andRadda, G. K. (1983) Plasmodium yoelii: blood oxygen and brainfunction in the infected mouse. Exp. Parasitol. 56: 391–396.
Krishna, S., Supanaranond, W., Pukrittayakamee, S., Karter, D.,Supputamongkol, Y., Davis, T. M. E., Holloway, P. A., White,N. J. and Davis, T. M. (1994a) Dichloroacetate for lactic acido-sis in severe malaria: a pharmacokinetic and pharmacodynamicassessment. Metabolism 43: 974–981.
Krishna, S., Waller, D. W., ter Kuile, F., Kwiatkowski, D., Craw-ley, J., Craddock, C. F., Nosten, F., Chapman, D., Brewster, D.,Holloway, P. A. and White, N. J. (1994b) Lactic acidosis andhypoglycaemia in children with severe malaria: pathophysiolog-ical and prognostic significance. Trans. R. Soc. Trop. Med.Hyg. 88: 67–73.
Krishna, S., Agbenyenga, T., Angus, B. J., Bedu-Addo, G., Ofori-Amanfo, G., Henderson, G., Szwandt, I. S. I., O’Brien, R. andStacpoole, P. W. (1995a) Pharmacokinetics and pharmacody-namics of dichloracetate in children with lactic acidosis due tosevere malaria. Q. J. Med. 88: 341–349.
Krishna, S., Pukrittayakamee, S., Supanaranond, W., ter Kuile, F.,Ruprah, M., Sura, T. and White, N. J. (1995b) Fever in uncom-plicated Plasmodium falciparum malaria: randomized double-”blind” comparison of ibuprofen and paracetamol treatment.Trans. R. Soc. Trop. Med. Hyg. 89: 507–509.
Krishna, S., Supanaranond, W., Pukrittayakamee, S., Kuile, F. T.,Ruprah, M. and White, N. J. (1996) The disposition and effectsof two doses of dichloroacetate in adults with severe falciparummalaria. Br. J. Clin. Pharmacol. 41: 29–34.
Kwiatkowski, D. (1989) Febrile temperatures can synchronize thegrowth of Plasmodium falciparum in vitro. J. Exp. Med. 169:357–361.
Kwiatkowski, D. and Bate, C. (1995) Inhibition of tumour necro-sis factor (TNF) production by antimalarial drugs used in cere-bral malaria. Trans. R. Soc. Trop. Med. Hyg. 89: 215–216.
Kwiatkowski, D., Cannon, J. G., Manogue, K. R., Cerami, A.,Dinarello, C. A. and Greenwood, B. M. (1989) Tumour necro-sis factor production in falciparum malaria and its associationwith schizont rupture. Clin. Exp. Immunol. 77: 361–366.
Kwiatkowski, D., Hill, A. V., Sambou, I., Twumasi, P., Castra-cane, J., Manogue, K. R., Cerami, A., Brewster, D. R. andGreenwood, B. M. (1990) TNF concentration in fatal cerebral,non-fatal cerebral, and uncomplicated Plasmodium falciparummalaria. Lancet 336: 1201–1204.
Kwiatkowski, D., Molyneux, M., Taylor, T., Klein, N., Curtis, N.and Smit, M. (1991) Cerebral malaria [letter]. Lancet 337:1281–1282.
Kwiatkowski, D., Molyneux, M. E., Stephens, S., Curtis, N., Klein,N., Pointaire, P., Smit, M., Allan, R., Brewster, D. R., Grau, G. E.and Greenwood, B. M. (1993) Anti-TNF therapy inhibits feverin cerebral malaria. Q. J. Med. 86: 91–98.
Lackritz, E. M., Campbell, C. C., Ruebush, T. K., 2d, Hightower,A. W., Wakube, W., Steketee, R. W. and Were, J. B. (1992)Effect of blood transfusion on survival among children in aKenyan hospital. Lancet 340: 524–528.
Lafaix, C., Dumas, M., Nouhouayi, A. and Rey, M. (1970) Cécitéconsecutive au paludisime cérébrale (d’après sept cas). Bull. Soc.Med. Afr. Noire Lang. Fr. 15: 423–433.
Lalloo, D. G., Trevett, A. J., Paul, M., Korinhona, A., Laurenson,I. F., Mapao, J., Nwokolo, N., Danga Christian, B., Black, J.,Saweri, A., Naraqi, S. and Warrell, D. A. (1996) Severe andcomplicated falciparum malaria in Melanesian adults in PapuaNew Guinea. Am. J. Trop. Med. Hyg. 55: 119–124.
Laveran, C. A. (1880) Un nouveau parasite trouvé dans le sangdes malades atteints de fièvre palustre. Origine parasitaire desaccidents de l’impaludisme. Bull. Mem. Soc. Méd. Hôp. Paris17: 158–164.
Leaver, R. J., de Baetselier, H., Bagshawe, A. and Watters, D. A.(1990) Cerebral malaria: what is unarousable coma? Lancet335: 44–45.
Lee, S. H., Looareesuwan, S., Chan, J., Wilairatana, P., Vani-janonta, S., Chong, S. M. and Chong, B. H. (1997) Plasmamacrophage colony-stimulating factor and P-selectin levels inmalaria-associated thrombocytopaenia. Thromb. Haemost. 72:2898-293.
Leete, T. H. and Rubin, H. (1996) Malaria and the cell cycle. Par-asitol. Today 12: 442–444.
Lehman, L. G., Vu-Quoc, B., Carlson, J. and Kremsner, P. G.(1997) Plasmodium falciparum: inhibition of erythrocyte rosetteformation and detachment of rosettes by pentoxifylline. Trans.R. Soc. Trop. Med. Hyg. 91: 74–75.
Lemercier, G., Rey, M. and Collomb, H. (1966) Lesions cérébralesdans le paludisme de l’enfant. Bull. Soc. Pathol. Exot. 59: 533–548.
Lemercier, G., Bert, J., Nouhoayi, A., Rey, M. and Collomb, H.(1969) Le neuropaludisme: aspects électroencéphalographiques,neuropathologiques, problèmes physiopathologiques. Path. Biol.(Paris) 17: 459–472.
Lewallen, S., Taylor, T. E., Molyneux, M. E., Wills, B. A. andCourtright, P. (1993) Ocular fundus findings in Malawian chil-dren with cerebral malaria. Opthalmology 100: 857–861.
Lipton, S. A., Choi, Y., Pan, Z., Lei, S. Z., Chen, H. S., Sucher, N. J.,Loscalzo, J., Singel, D. J. and Stamler, J. S. (1993) A redox-based mechanism for the neuroprotective and neurodestructiveeffects of nitric oxide and related nitroso-compounds. Nature364: 626–632.
Looareesuwan, S., Warrell, D. A., White, N. J., Chanthavanich,P., Warrell, M. J., Chantaratherakitti, S., Changswek, S.,Chongmankongcheep, L. and Kanchanaranya, C. (1983) Reti-nal hemorrhage, a common sign of prognostic significance incerebral malaria. Am. J. Trop. Med. Hyg. 32: 911–915.
Looareesuwan, S., Ho, M., Wattanagoon, Y., White, N. J., War-rell, D. A., Bunnag, D., Harinasuta, T. and Wyler, D. J. (1987)Dynamic alteration in splenic function during acute falciparummalaria. N. Engl. J. Med. 317: 675–679.
Looareesuwan, S., Phillips, R. E., Karbwang, J., White, N. J.,Flegg, P. J. and Warrell, D. A. (1990) Plasmodium falciparumhyperparasitaemia: use of exchange transfusion in seven patientsand a review of the literature. Q. J. Med. 227: 471–481.

Pathophysiology and Supportive Treatment of Severe Malaria 47
Looareesuwan, S., Davis, J. G., Allen, D. L., Lee, S. H., Bunnag,D. and White, N. J. (1992) Thrombocytopenia in malaria.Southeast Asian J. Trop. Med. Public Health 23: 44–50.
Looareesuwan, S., Wilairatana, P., Krishna, S., Kendall, B., Van-naphan, S., Viravan, C. and White, N. J. (1995) Magnetic reso-nance imaging of the brain in patients with cerebral malaria.Clin. Infect. Dis. 21: 300–309.
Looareesuwan, S., Wilairatana, P., Vannaphan, S., Gordeuk, V. R.,Taylor, T. E., Meshnick, S. R. and Brittenham, G. M. (1996)Co-administration of desferrioxamine B with artesunate inmalaria: an assessment of safety and tolerance. Ann. Trop. Med.Parasitol. 90: 551–554.
Lucas, S. K., Hounnou, A., Bell, J., Peacock, C., Andoh, J.,Honde, M., De Cock, K. M. and Warrell, D. A. (1996) Severecerebral swelling is not observed in children dying with malaria.Q. J. Med. 89: 351–353.
Lynk, A. and Gold, R. (1989) Review of 40 children withimported malaria. Pediatr. Infect. Dis. J. 8: 745–750.
Mabey, D. C., Brown, A. and Greenwood, B. M. (1987) Plasmo-dium falciparum malaria and Salmonella infections in Gambianchildren. J. Infect. Dis. 155: 1319–1321.
Mabeza, G. F., Moyo, V. M., Thuma, P. E., Biemba, G., Parry, D.,Khumalo, H., Nyarugwe, P., Zulu, S. and Gordeuk, V. R.(1995) Predictors of severity of illness on presentation in chil-dren with cerebral malaria. Ann. Trop. Med. Parasitol. 89: 221–228.
Mabeza, G. F., Biemba, G. and Gordeuk, V. R. (1996) Clinicalstudies of iron chelators in malaria. Acta Haematol. 95: 78–86.
MacDougall, L. G. (1962) Low cerebrospinal fluid protein in Africanchildren with febrile convulsions. Arch. Dis. Child. 37: 309–313.
MacPherson, G. G., Warrell, M. J., White, N. J., Looareesuwan, S.and Warrell, D. A. (1985) Human cerebral malaria. A quanti-tative ultrastructural analysis of parasitized erythrocyte seques-tration. Am. J. Pathol. 119: 385–401.
Maegraith, B. (1969) Comments on pathophysiology. Milit. Med.134: 1129–1131.
Maegraith, B. and Fletcher, A. (1972) The pathogenesis of mam-malian malaria. Adv. Parasitol. 10: 49–75.
Maguire, M. J. (1983) The management of cerebral malaria inAfrican children. East Afr. Med. J. 60: 260–265.
Marchiafava, E. and Bignami, A. (1894) On Summer-AutumnMalaria Fevers. The New Sydenham Society, London.
Marsh, K., Marsh, V. M., Brown, J., Whittle, H. C. and Green-wood, B. M. (1988) Plasmodium falciparum: the behavior of clin-ical isolates in an in vitro model of infected red blood cellsequestration. Exp. Parasitol. 65: 202–208.
Marsh, K., Forster, D., Waruiru, C., Mwangi, I., Winstanley, M.,Marsh, V., Newton, C., Winstanley, P., Warn, P., Peshu, N.,Pasvol, G. and Snow, R. W. (1995) Indicators of life-threateningmalaria in African children. N. Engl. J. Med. 332: 1399–1404.
Marshall, L. F., Smith, R. W., Rauscher, L. A. and Shapiro, H. M.(1978) Mannitol dose requirements in brain-injured patients. J.Neurosurg. 48: 169–172.
Mate Kole, M. O., Yeboah, E. D., Affram, R. K. and Adu, D.(1996) Blackwater fever and acute renal failure in expatriates inAfrica. Ren. Fail. 18: 525–531.
Matthews, D. S., Bullock, R. E., Matthews, J. N., Aynsley Green,A. and Eyre, J. A. (1995) Temperature response to severe headinjury and the effect on body energy expenditure and cerebraloxygen consumption. Arch. Dis. Child. 72: 507–515.
Mbogo, C. N., Snow, R. W., Kabiru, E. W., Ouma, J. H., Githure,J. I., Marsh, K. and Beier, J. C. (1993) Low-level Plasmodium fal-
ciparum transmission and the incidence of severe malaria infec-tions on the Kenyan coast. Am. J. Trop. Med. Hyg. 49: 245–253.
McCaslin, R. I., Pikis, A. and Rodriquez, W. J. (1994) PediatricPlasmodium falciparum malaria: a ten-year experience from Wash-ington DC. Pediatr. Infect. Dis. J. 13: 709–715.
McGraw, C. P., Alexander, E. and Howard, G. (1978) Effect ofdose and dose schedule on the response of intracranial pressureto mannitol. Surg. Neurol. 10: 127–130.
McGuire, W., Hill, A. V. S., Allsopp, C. E. M., Greenwood, B. M.and Kwiatkowski, D. (1994) Variation in the TNF-a promoterregion associated with the susceptibility to cerebral malaria.Nature 371: 508–510.
McGuire, W., Hill, A. V., Greenwood, B. M. and Kwiatkowski, D.(1996) Circulating ICAM-1 levels in falciparum malaria arehigh but unrelated to disease severity Trans. R. Soc. Trop. Med.Hyg. 90: 274–276.
Mercado, T. I. and von Brand, T. (1954) Glycogen studies onwhite rats infected wth Plasmodium berghei. Exp. Parasitol. 3:259–266.
Merry, A. H., Looareesuwan, S., Phillips, R. E., Chanthavanich,P., Supanaranond, W., Warrell, D. A. and Weatherall, D. J.(1986) Evidence against immune haemolysis in falciparummalaria in Thailand. Br. J. Haematol. 64: 187–194.
Metzger, W. G., Mordmuller, B. G. and Kremsner, P. G. (1995)Malaria pigment in leucocytes. Trans. R. Soc. Trop. Med. Hyg.89: 637–638.
Migasena, P. and Maegraith, B. G. (1968a) The movement of flu-orescent isothiocyanate (F.I.T.C.) labelled human albuminfrom blood into brain tissue examined by fluorescent techniquein normal and Plasmodium knowlesi infected Macaca mulatta.Med. J. Malaysia 22: 250.
Migasena, P. and Maegraith, B. G. (1968b) Factor affecting on themovement of protein across the blood:brain:C.S.F. barriers inPlasmodium knowlesi infected Macaca mulatta. Med. J. Malaysia22: 251.
Migasena, S. (1983) Hypoglycaemia in falciparum malaria. Ann.Trop. Med. Parasitol. 77: 323–324.
Miller, K. D., Greenberg, A. E. and Campbell, C. C. (1989a)Treatment of severe malaria in the United States with a contin-uous infusion of quinidine gluconate and exchange transfusion.N. Engl. J. Med. 321: 65–70.
Miller, K. D., White, N. J., Lott, J. A., Roberts, J. M. and Green-wood, B. M. (1989b) Biochemical evidence of muscle injury inAfrican children with severe malaria. J. Infect. Dis. 159: 139–142.
Miller, L. H. (1969) Distribution of mature trophozoites and schiz-onts of Plasmodium falciparum in the organs of Aotus trivirga-tus, the night monkey. Am. J. Trop. Med. Hyg. 18: 860–865.
Miller, L. H., Fremount, H. N. and Luse, S. A. (1971) Deep vascu-lar schizogony of Plasmodium knowlesi in Macaca mulatta. Distri-bution in organs and ultrastructure of parasitized red cells. Am.J. Trop. Med. Hyg. 20: 816–824.
Molyneux, M. E., Looareesuwan, S., Menzies, I. S., Grainger, S. L.,Phillips, R. E., Wattanagoon, Y., Thompson, R. P. H. and War-rell, D. A. (1989a) Reduced hepatic blood flow and intestinalmalabsorption in severe falciparum malaria. Am. J. Trop. Med.Hyg. 40: 470–476.
Molyneux, M. E., Taylor, T. E., Wirima, J. J. and Borgstein, A.(1989b) Clinical features and prognostic indicators in paediat-ric cerebral malaria: a study of 131 comatose Malawian chil-dren. Q. J. Med. 71: 441–459.

48 C. R. J. C. Newton and S. Krishna
Molyneux, M. E., Taylor, T. E., Wirima, J. J. and Grau, G. E.(1991) Tumour necrosis factor, interleukin-6, and malaria. Lan-cet 337: 1098.
Mordes, J. P., Tranquada, R. E. and Rossini, A. A. (1996) Lacticacidosis. In: Intensive Care Medicine, pp. 1330–1337, Rippe, J. M.,Irwin, R. S., Fink, M. P. and Cerra, F. B. (eds.) Little, Brownand Company, New York.
Morrison, D. B. and Jeskey, H. A. (1948) Alterations in some con-stituents of the monkey erythrocytes infected with Plasmodiumknowlesi as related to pigment formation. J. Nat. Malaria Soc. 7:259–264.
Muizelaar, J. P., Lutz, H. A. and Becker, D. P. (1984) Effect ofmannitol on ICP and CBF and correlation with pressure auto-regulation in severely head-injured patients. J. Neurosurg. 61:700–706.
Muntendam, A. H., Jaffar, S., Bleichrodt, N. and van Hensbroek,M. B. (1996) Absence of neuropsychological sequelae followingcerebral malaria in Gambian children. Trans. R. Soc. Trop.Med. Hyg. 90: 391–394.
Murphy, S., English, M., Omar, A., Crawley, J., Waruiru, C.,Mwangi, I., Amukoye, E., Peshu, N., Newton, C. R., Winstan-ley, P. A. and Marsh, K. (1995a) The management of severemalaria in children: a review. East Afr. Med. J. 72: 536–539.
Murphy, S., Watkins, W. M., Bray, P. G., Lowe, B., Winstanley,P. A., Peshu, N. and Marsh, K. (1995b) Parasite viability duringtreatment of severe falciparum malaria: differential effects ofartemether and quinine. Am. J. Trop. Med. Hyg. 53: 303–305.
Murphy, S., English, M., Waruiru, C., Mwangi, I., Amukoye, E.,Crawley, J., Newton, C., Winstanley, P., Peshu, N. and Marsh,K. (1996) An open randomized trial of artemether versus qui-nine in the treatment of cerebral malaria in African children.Trans. R. Soc. Trop. Med. Hyg. 90: 298–301.
Musoke, L. K. (1966) Neurological manifestations of malaria inchildren. East Afr. Med. J. 43: 561–564.
Nagatake, T., Hoang, V. T., Tegoshi, T., Rabbege, J., Ann, T. K.and Aikawa, M. (1992) Pathology of falciparum malaria inVietnam. Am. J. Trop. Med. Hyg. 47: 259–264.
Nash, G. B., O’Brien, E., Gordon-Smith, E. C. and Dormandy, J. A.(1989) Abnormalities in the mechanical properties of red bloodcells caused by Plasmodium falciparum. Blood 74: 855–861.
Nash, G. B., Cooke, B. M., Marsh, K., Berendt, A., Newbold, C.and Stuart, J. (1992) Rheological analysis of the adhesive inter-actions of red blood cells parasitized by Plasmodium falciparum.Blood 79: 798–807.
Neequaye, J., Ofori-Adjei, E., Ofori-Adjei, D. and Renner, L.(1991) Comparative trial of oral versus intramuscular chlo-roquine in children with cerebral malaria. Trans. R. Soc. Trop.Med. Hyg. 85: 718–722.
Nevill, C. G., Some, E. S., Mung’ala, V. O., Mutemi, W., New, L.,Marsh, K., Lengeler, C. and Snow, R. W. (1996) Insecticide-treated bednets reduce mortality and severe morbidity frommalaria among children on the Kenyan coast. Trop. Med. Int.Health 1: 139–146.
Newton, C. R. J. C. (1992) The contribution of malaria to severeanaemia in children on the Kenyan coast. Br. J. Haematol. 82:268–269.
Newton, C. R. J. C. (1995) Intracranial hypertension in Kenyanchildren with cerebral malaria. M.D. Thesis, University of CapeTown.
Newton, C. R. J. C. and Warrell, D. A. (1998) Neurological manifes-tations of Plasmodium falciparum malaria. Ann. Neurol., in press.
Newton, C. R., Pasvol, G., Winstanley, P. A. and Warrell, D. A.
(1990) Cerebral malaria: what is unarousable coma? [letter].Lancet 335: 472.
Newton, C. R., Kirkham, F. J., Winstanley, P. A., Pasvol, G.,Peshu, N., Warrell, D. A. and Marsh, K. (1991a) Intracranialpressure in African children with cerebral malaria. Lancet 337:573–576.
Newton, C. R., Winstanley, P. A. and Marsh, K. (1991b) Retinalhaemorrhages in falciparum malaria. Arch. Dis. Child. 66: 753.
Newton, C. R., Peshu, N., Kendall, B., Kirkham, F. J., Sowunmi,A., Waruiru, C., Mwangi, I., Murphy, S. A. and Marsh, K.(1994) Brain swelling and ischaemia in Kenyans with cerebralmalaria. Arch. Dis. Child. 70: 281–287.
Newton, C. R. J. C., Marsh, K., Peshu, N. and Kirkham, F. J.(1996a) Perturbations of cerebral hemodynamics in Kenyanchildren with cerebral malaria. Pediatr. Neurol. 15: 41–49.
Newton, C. R. J. C., Peshu, N., Chong, K., Crawley, J. and Marsh,K. (1996b) Computerized tomographic appearances of Kenyanchildren with neurological sequelae following cerebral malaria.Am. J. Trop. Med. Hyg. 55: 239.
Newton, C. R. J. C., Chokwe, T., Armstrong-Schellenberg, J. R. M.,Winstanley, P. A., Forster, D., Peshu, N., Kirkham, F. J. andMarsh, K. (1997a) Coma scales in children with severe falci-parum malaria. Trans. R. Soc. Trop. Med. Hyg. 91: 161–165.
Newton, C. R. J. C., Crawley, J., Sowunmi, A., Waruiru, C.,Mwangi, I., Murphy, S. A., English, M., Marsh, K. andKirkham, F. J. (1997b) Intracranial hypertension in Kenyanchildren with cerebral malaria. Arch. Dis. Child. 76: 219–226.
Newton, C. R. J. C., Kirkham, F. J., Cope, M., Sowunmi, A.,Peshu, N. and Marsh, K. (1997c) Changes in cerebral oxyhe-moglobin and deoxyhemoglobin during seizures in childrenwith cerebral malaria. J. Cereb. Blood Flow Metab. 17: S56.
Newton, C. R. J. C., Warn, P. A., Winstanley, P. A., Peshu, N.,Snow, R. W., Pasvol, G. and Marsh, K. (1997d) Contributionof falciparum malaria to severe anemia in Kenyan children.Trop. Med. Int. Health 2: 165–178.
Newton, C. R. J. C., Whitten, R. O. and Taylor, T. E. (1998)Pathophysiology of fatal falciparum malaria in African children.Am. J. Trop. Med. Hyg., in press.
Nguyen, P. H., Day, N., Pram, T. D., Ferguson, D. J. and White,N. J. (1995) Intraleucocytic malaria pigment and prognosis insevere malaria. Trans. R. Soc. Trop. Med. Hyg. 89: 200–204.
Nguyen, P. H., Day, N. P., Ly, V. C., Waller, D., Nguyen, H. P.,Bethell, D. B., Tran, T. H. and White, N. J. (1996) Post-malaria neurological syndrome. Lancet 348: 917–921.
Nyakundi, J. N., Warn, P., Newton, C., Mumo, J. and JephthahOchola, J. (1994) Serum tumour necrosis factor in children suf-fering from Plasmodium falciparum infection in Kilifi District,Kenya. Trans. R. Soc. Trop. Med. Hyg. 88: 667–670.
O’Dempsey, T. J., McArdle, T. F., Laurence, B. E., Lamont, A. C.,Todd, J. E. and Greenwood, B. M. (1993) Overlap in the clini-cal features of pneumonia and malaria in African children.Trans. R. Soc. Trop. Med. Hyg. 87: 662–665.
Olumese, P. E., Sodeinde, O., Gbadegesin, R. A., Nafiu, O.,Oguche, S. and Walker, O. (1995) Respiratory distress adverselyaffects the outcome of childhood cerebral malaria. Trans. R. Soc.Trop. Med. Hyg. 89: 634.
Olurin, O. (1970) Cortical blindness following convulsions andfever in Nigerian children. Pediatrics 46: 102–107.
Omanga, U., Ngandu, K., Disengomoka, I. and Badibanga, B.(1977) Accès pernieux palustre chez l’enfant. Afrique Med. 16:507–516.
Omanga, U., Ntihinyurwa, M., Shako, D. and Mashako, M.

Pathophysiology and Supportive Treatment of Severe Malaria 49
(1983) Les hémiplegies au cours de l’acces pernicieux a plasmo-dium falciparum de l’enfant. Ann. Pediat. 30: 294–296.
Oo, M. M., Aikawa, M., Than, T., Aye, T. M., Myint, P. T., Iga-rashi, I. and Schoene, W. C. (1987) Human cerebral malaria:a pathological study. J. Neuropathol. Exp. Neurol. 46: 223–231.
Orringer, C. E., Eustace, J. C., Wunsch, C. D. and Gardner, L. B.(1977) Natural history of lactic acidosis after grand mal seizures.N. Engl. J. Med. 297: 796–797.
Pasvol, G., Newton, C. R., Winstanley, P. A., Watkins, W. M.,Peshu, N. M., Were, J. B., Marsh, K. and Warrell, D. A. (1991)Quinine treatment of severe falciparum malaria in African chil-dren: a randomized comparison of three regimens. Am. J. Trop.Med. Hyg. 45: 702–713.
Pasvol, G., Clough, B., Carlsson, J. and Snounou, G. (1995) Thepathogenesis of severe falciparum malaria. In: Malaria, pp. 249–270, Pasvol, G. (ed.) Baillière Tindall, London.
Petersen, C., Nelson, R., Magowan, C., Wollish, W., Jensen, J.and Leech, J. (1989) The mature erythrocyte surface antigen ofPlasmodium falciparum is not required for knobs or cytoadher-ence. Mol. Biochem. Parasitol. 36: 61–66.
Peto, T. E. and Thompson, J. L. (1986) A reappraisal of the effects ofiron and desferrioxamine on the growth of Plasmodium falciparum‘in vitro’: the unimportance of serum iron. Br. J. Haematol. 63:273–280.
Phillips, R. E., Warrell, D. A., White, N. J., Looareesuwan, S. andKarbwang, J. (1985) Intravenous quinidine for the treatment ofsevere falciparum malaria. Clinical and pharmacokinetic stud-ies. N. Engl. J. Med. 312: 1273–1278.
Phillips, R. E., Looareesuwan, S., Warrell, D. A., Lee, S. H., Kar-bwang, J., Warrell, M. J., White, N. J., Swasdichai, C. andWeatherall, D. J. (1986) The importance of anaemia in cere-bral and uncomplicated falciparum malaria: role of complica-tions, dyserythropoiesis and iron sequestration. Q. J. Med. 58:305–323.
Phillips, R. E., Looareesuwan, S., Molyneux, M. E., Hatz, C. andWarrell, D. A. (1993) Hypoglycaemia and counterregulatoryhormone responses in severe falciparum malaria: treatmentwith Sandostatin. Q. J. Med. 86: 233–240.
Phu, N. H., Day, N., Diep, P. T., Ferguson, D. J. P. and White,N. J. (1995) Intraleucocyte malaria pigment and prognosis insevere malaria. Trans. R. Soc. Trop. Med. Hyg. 89: 200–204.
Plum, F. and Posner, J. B. (1980) The Diagnosis of Stupor andComa, 4th ed. F. A. Davis, Philadelphia.
Polder, T. W., Jerusalem, C. R. and Eling, W. M. (1991) Morpho-logical characteristics of intracerebral arterioles in clinical(Plasmodium falciparum) and experimental (Plasmodium berghei)cerebral malaria. J. Neurol. Sci. 101: 35–46.
Pongponratn, E., Riganti, M., Punpoowong, B. and Aikawa, M.(1991) Microvascular sequestration of parasitized erythrocytesin human falciparum malaria: a pathological study. Am. J. Trop.Med. Hyg. 44: 168–175.
Porta, J., Carota, A., Pizzolato, G. P., Wildi, E., Widmer, M. C., Mar-gairaz, C. and Grau, G. E. (1993) Immunopathological changesin human cerebral malaria. Clin. Neuropathol. 12: 142–146.
Prada, J. and Kremsner, P. G. (1997) Reactive oxygen intermedi-ates and cerebral malaria. Trans. R. Soc. Trop. Med. Hyg. 91:92–93.
Pukrittayakamee, S., Davis, T. M., Levy, J., Looareesuwan, S.,Roche, R. J., Jeerawathanapun, P. and White, N. J. (1991a)The metabolic response to rapid intravenous glucose injectionin acute falciparum malaria. Trans. R. Soc. Trop. Med. Hyg. 85:189–193.
Pukrittayakamee, S., White, N. J., Davis, T. M. E., Looareesuwan,S., Supanaranond, W., Desakorn, V., Chaivisuth, B. and Will-iamson, D. H. (1991b) Hepatic blood flow and metabolism insevere falciparum malaria: clearance of intravenously adminis-tered galactose. Clin. Sci. 82: 63–70.
Pukrittayakamee, S., Supanaranond, W., Looareesuwan, S., Vani-janonta, S. and White, N. J. (1994a) Quinine in severe falci-parum malaria: evidence of declining efficacy in Thailand.Trans. R. Soc. Trop. Med. Hyg. 88: 324–327.
Pukrittayakamee, S., Vanijanonta, S., Chantra, A., Clemens, R.and White, N. J. (1994b) Blood stage antimalarial efficacy ofprimaquine in Plasmodium vivax malaria. J. Infect. Dis. 169:932–935.
Pukrittayakamee, S., White, N. J., Davis, T. M., Supanaranond,W., Crawley, J., Nagachinta, B. and Williamson, D. H. (1994c)Glycerol metabolism in severe falciparum malaria. Metabolism43: 887–892.
Rampengan, T. H. (1991) Cerebral malaria in children. Compara-tive study between heparin, dexamethasone and placebo. Pae-diatr. Indones. 31: 59–66.
Rees, P. (1982) Dexamethasone deleterious in cerebral malaria[letter]. Br. Med. J. 285: 1357.
Rey, M., Nouhouayi, A. and Diop Mar, L. (1966) Les expressionscliniques du paludisme a plasmodium falciparum chez l’enfantnoir African. Bull. Soc. Pathol. Exot. 58: 683–704.
Riganti, M., Pongponratn, E., Tegoshi, T., Looareesuwan, S., Pun-poowong, B. and Aikawa, M. (1990) Human cerebral malariain Thailand: a clinico-pathological correlation. Immunol. Lett.25: 199–205.
Rigdon, R. H. and Fletcher, D. E. (1945) Lesions in the brain asso-ciated with malaria. Pathologic study on man and on experi-mental animals. Arch. Neurol. Psychiatry 53: 191–198.
Ritter, K., Brestrich, H., Nellen, B., Kratzin, H., Eiffert, H. andThomssen, R. (1990) Autoantibodies against triosephosphateisomerase. A possible clue to pathogenesis of hemolytic anemiain infectious mononucleosis. J. Exp. Med. 171: 565–570.
Ritter, K., Kuhlencord, A., Thomssen, R. and Bommer, W. (1993)Prolonged haemolytic anaemia in malaria and autoantibodiesagainst triosephosphate isomerase. Lancet 342: 1333–1334.
Roberts, D. J., Craig, A. G., Berendt, A. R., Pinches, R., Nash, G.,Marsh, K. and Newbold, C. I. (1992) Rapid switching to multi-ple antigenic and adhesive phenotypes in malaria. Nature 357:689–692.
Rogerson, S. J., Reeder, J. C., al Yaman, F. and Brown, G. V. (1994)Sulfated glycoconjugates as disrupters of Plasmodium falciparumerythrocyte rosettes. Am. J. Trop. Med. Hyg. 51: 198–203.
Rogier, C., Commenges, D. and Trape, J. F. (1996) Evidence of anage-dependent pyrogenic threshold of Plasmodium falciparumparasitaemia in highly endemic population. Am. J. Trop. Med.Hyg. 54: 613–619.
Rosenthal, P. J., Petersen, C., Geertsma, F. R. and Kohl, S. (1996)Availability of intravenous quinidine for falciparum malaria[letter]. N. Engl. J. Med. 335: 138.
Rothe, H. (1956) One hundred cases of cerebral malaria. East Afr.Med. J. 33: 405–407.
Rowe, A., Obeiro, J., Newbold, C. I. and Marsh, K. (1995) Plasmo-dium falciparum rosetting is associated with malaria severity inKenya. Infect. Immun. 63: 2323–2326.
Royal College of Physicians (London) (1991) Guidelines for themanagement of convulsions with fever. Br. Med. J. 303: 634–636.
Saeed, B. O., Atabani, G. S., Nawwaf, A., Nasr, A. M., Abdul-

50 C. R. J. C. Newton and S. Krishna
hadi, N. H., Abu Zeid, Y. A., Alrasoul, M. A. and Bayoumi, R. A.(1990) Hypoglycaemia in pregnant women with malaria. Trans.R. Soc. Trop. Med. Hyg. 84: 349–350.
Sanohko, A., Dareys, J. P. and Charreau, M. (1968) État encépha-litique prolongé et acces pernicieux palustres. Bull. Soc. Med.Afr. Noire. Lang. Fr. 3: 662–669.
Schmid, A. H. (1974) Cerebral malaria. On the nature and signif-icance of vascular changes. Eur. Neurol. 12: 197–208.
Schmutzhard, E. and Gerstenbrand, F. (1984) Cerebral malaria inTanzania. Its epidemiology, clinical symptoms and neurologicallong term sequelae in the light of 66 cases. Trans. R. Soc. Trop.Med. Hyg. 78: 351–353.
Schofield, L. and Hackett, F. (1993) Signal transduction in hostcells by a glycosylphosphatidylinositol toxin of malaria para-sites. J. Exp. Med. 177: 145–153.
Schofield, L., Novakovic, S., Gerold, P., Schwarz, R. T., McCon-ville, M. J. and Tachado, S. D. (1996) Glycosylphosphatidyli-nositol toxin of Plasmodium up-regulates intercellular adhesionmolecule-1, vascular cell adhesion molecule-1, and E-selectinexpression in vascular endothelial cells and increases leukocyteand parasite cytoadherence via tyrosine kinase-dependent sig-nal transduction. J. Immunol. 156: 1886–1896.
Scuderi, P., Sterling, K. E., Lam, K. S., Finley, P. R., Ryan, K. J.,Ray, C. G., Petersen, E., Slymen, D. J. and Salmon, S. E. (1986)Raised serum levels of tumour necrosis factor in parasitic infec-tions. Lancet ii: 1364–1365.
Sein, K. K., Brown, A. E., Maeno, Y., Smith, C. D., Corcoran, K. D.,Hansukjariya, P., Webster, H. K. and Aikawa, M. (1993)Sequestration pattern of parasitized erythrocytes in cerebrum,mid-brain, and cerebellum of Plasmodium coatneyi-infected rhesusmonkeys (Macaca mulatta). Am. J. Trop. Med. Hyg. 49: 513–519.
Shaffer, N., Grau, G. E., Hedberg, K., Davachi, F., Lyamba, B., High-tower, A. W., Breman, J. G. and Phuc, N. D. (1991) Tumornecrosis factor and severe malaria. J. Infect. Dis. 163: 96–101.
Sharma, Y. D. (1991) Knobs, knob proteins and cytoadherence infalciparum malaria. Int. J. Biochem. 23: 775–789.
Sherman, I. W. (1979) Biochemistry of Plasmodium (malarial par-asites). Microbiol. Rev. 43: 453–495.
Shorvon, S. (1994) Status Epilepticus. Its Clinical Features andTreatment in Children and Adults. Cambridge UniversityPress, Cambridge.
Siesjo, B. K. (1978) Brain Energy Metabolism. John Wiley &Sons, Chichester.
Siesjo, B. K., Agard, C. and Bengtsson, F. (1989) Free radicals andbrain damage. Cerebrovasc. Brain Metab. Rev. 1: 165–211.
Silamut, K. and White, N. J. (1993) Relation of the stage of para-site development in the peripheral blood to prognosis in severefalciparum malaria. Trans. R. Soc. Trop. Med. Hyg. 87: 436–443.
Slater, A. F. G. and Cerami, A. (1992) Inhibition by chloroquineof a novel haem polymerase activity in malaria trophozoites.Nature 355: 167–169.
Slutsker, L., Taylor, T. E., Wirima, J. J. and Steketee, R. W.(1994) In-hospital morbidity and mortality due to malaria-asso-ciated severe anaemia in two areas of Malawi with different pat-terns of malaria infection. Trans. R. Soc. Trop. Med. Hyg. 88:548–551.
Smith, J. D., Chitnis, C. E., Craig, A. G., Roberts, D. J., Hudson-Taylor, D. E., Peterson, D. S., Pinches, R., Newbold, C. andMiller, L. H. (1995) Switches in expression of Plasmodium falci-parum var genes correlate with changes in antigenic and cytoad-herent phenotypes of infected erythrocytes. Cell 82: 101–110.
Smith, T., Hurt, N., Teuscher, T. and Tanner, M. (1995) Is fever agood sign for clinical malaria in surveys of endemic communi-ties? Am. J. Trop. Med. Hyg. 52: 306–310.
Snow, R. W., Omumbo, J. A., Lowe, B., Molyneux, C. S., Obiero,J., Palmer, A., Weber, M. W., Pinder, M., Nahlen, B., Obonyo, C.,Newbold, C., Gupta, S. and Marsh, K. (1997) Relation betweensevere malaria morbidity in children and level of Plasmodiumfalciparum transmission in Africa. Lancet 349: 1650–1654.
Solomon, T., Felix, J. M., Samuel, M., Dengo, G. A., Saldanha,R. A., Schapira, A. and Phillips, R. E. (1994) Hypoglycaemiain paediatric admissions in Mozambique. Lancet 343: 149–150.
Sowunmi, A. (1993) Psychosis after cerebral malaria in children.J. Natl. Med. Assoc. 85: 695–696.
Sowunmi, A. (1996a) Hyponatraemia in severe falciparummalaria: a clinical study of 19 comatose African children. Afr. J.Med. Med. Sci. 25: 47–52.
Sowunmi, A. (1996b) Renal impairment in children with severefalciparum malaria. Arch. Dis. Child. 74: 293–298.
Sowunmi, A., Walker, O. and Salako, L. A. (1992) Hyperparasi-taemia: not a reliable indicator of severity or poor prognosis infalciparum malaria in children in endemic African countries.Ann. Trop. Paediatr. 12: 155–158.
Spitz, S. (1946) The pathology of acute falciparum malaria. Milit.Surg. 99: 555–572.
Srichaikul, T., Pulket, C., Sirisatepisarn, T. and Prayoonwiwat,W. (1988) Platelet dysfunction in malaria. Southeast Asian J.Trop. Med. Public Health 19: 225–233.
Stace, J., Bilton, P., Coates, K. and Stace, N. (1980) Cerebralmalaria in children: retrospective study of admissions toMadang hospital. PNG Med. J. 25: 230–234.
Stacpoole, P. W. (1986) Lactic acidosis: the case against bicarbon-ate therapy. Ann. Intern. Med. 105: 276–279.
Stacpoole, P. W. (1989) The pharmacology of dichloroacetate.Metabolism 38: 1124–1144.
Stacpoole, P. W. (1997) Lactic acidosis and other mitochondrialdisorders. Metabolism 46: 306–321.
Stacpoole, P. W., Wright, E. C., Baumgartner, T. G., Bersin, R. M.,Buchalter, S., Curry, S. H., Duncan, C. A., Harman, E. M., Hend-erson, G. N., Jenkinson, S., Lachin, J. M., Lorenz, A., Schneider,S. H., Siegel, S., Summer, S., Thompson, D., Wollfe, C. L.,Zorovich, B. and the Dichloroacetate-Lactic Acidosis StudyGroup (1992) A controlled clinical trial of dichloroacetate fortreatment of lactic acidosis in adults. The Dichloroacetate-Lac-tic Acidosis Study Group. N. Engl. J. Med. 327: 1564–1569.
Stacpoole, P. W., Wright, E. C., Baumgartner, T. G., Bersin, R. M.,Buchalter, S., Curry, S. H., Duncan, C., Harman, E. M., Hender-son, G. N., Jenkinson, S., Lachin, J. M., Lorenz, A., Schneider,S. H., Siegel, S., Summer, S., Thompson, D., Wollfe, C. L.,Zorovich, B. and the DCA-Lactic Acidosis Study Group (1994)Natural history and course of acquired lactic acidosis in adults.DCA-Lactic Acidosis Study Group. Am. J. Med. 97: 47–54.
Steele, R. W., Tanaka, P. T., Lara, R. P. and Bass, J. W. (1970)Evaluation of sponging and of oral antipyretic therapy to reducefever. J. Pediatr. 77: 824–829.
Steketee, R. W., Wirima, J. J., Slutsker, L., Heymann, D. L. andBreman, J. G. (1996) The problem of malaria and malaria con-trol in pregnancy in sub-Saharan Africa. Am. J. Trop. Med. Hyg.55: 2–7.
Stettler, N., Schutz, Y., Whitehead, R. and Jequier, E. (1992)Effect of malaria and fever on energy metabolism in Gambianchildren. Pediatr. Res. 31: 102–106.
Stocker, R., Hunt, N. H., Clark, I. A. and Weidemann, M. J.

Pathophysiology and Supportive Treatment of Severe Malaria 51
(1984) Production of luminol-reactive oxygen radicals duringPlasmodium vinckei infection. Infect. Immun. 45: 708–712.
Stoute, J. A., Slaoui, M., Heppner, G., Momin, P., Kester, K. E.,Desmons, P., Wellde, B. T., Garcon, N., Krzych, U., Ballou, R.and Cohen, J. D. for the RTSS Malaria Vaccine EvaluationGroup (1997) A preliminary evalution of a recombinant cir-cumsporozoite protein vaccine against Plasmodium falciparummalaria. N. Engl. J. Med. 336: 86–91.
Sturchler, D. (1990) How much malaria is there worldwide? Para-sitol. Today 5: 12.
Su, X. Z., Heatwole, V. M., Wertheimer, S. P., Guinet, F., Herr-feldt, J. A., Peterson, D. S., Ravetch, J. A. and Wellems, T. E.(1995) The large diverse gene family var encodes proteinsinvolved in cytoadherence and antigenic variation of Plasmo-dium falciparum-infected erythrocytes. Cell 82: 89–100.
Sullivan, A. D. and Meshnick, S. R. (1996) Haemozoin: identifi-cation and quantification. Parasitol. Today 12: 161–163.
Sullivan, D. J., Gluzman, I. Y. and Goldberg, D. E. (1996) Plasmo-dium hemozoin formation mediated by histidine rich proteins.Science 271: 219–222.
Tachado, S. D., Gerold, P., McConville, M. J., Baldwin, T., Qui-lici, D., Schwarz, R. T. and Schofield, L. (1996) Glycosylphos-phatidylinositol toxin of Plasmodium induces nitric oxidesynthase expression in macrophages and vascular endothelialcells by a protein tyrosine kinase-dependent and protein kinaseC-dependent signaling pathway. J. Immunol. 156: 1897–1907.
Targett, G. A. T. (1995) Malarial vaccines. Curr. Opin. Infect.Dis. 8: 322–327.
Taylor, T. E., Molyneux, M. E., Wirima, J. J., Fletcher, A. andMorris, K. (1988) Blood glucose levels in Malawian childrenbefore and during the adminstration of intravenous quinine forsevere falciparum malaria. N. Engl. J. Med. 319: 1040–1047.
Taylor, T. E., Molyneux, M. E., Wirima, J. J., Borgstein, A., Gold-ring, J. D. and Hommel, M. (1992) Intravenous immunoglobu-lin in the treatment of paediatric cerebral malaria. Clin. Exp.Immunol. 90: 357–362.
Taylor, T. E., Borgstein, A. and Molyneux, M. E. (1993) Acid-base status in paediatric Plasmodium falciparum malaria. Q. J.Med. 86: 99–109.
Teasdale, G. and Jennett, B. (1974) Assessment of coma andimpaired consciousness. A practical scale. Lancet ii: 81–84.
ter Kuile, F., Nosten, F., Chongsuphajaisiddhi, T., Holloway, P.,Maelankirri, L. and White, N. J. (1992) Absorption of intra-muscular phenobarbitone in children with severe falciparummalaria. Eur. J. Clin. Pharmacol. 42: 107–110.
ter Kuile, F., White, N. J., Holloway, P., Pasvol, G. and Krishna, S.(1993) Plasmodium falciparum: in vitro studies of the pharmaco-dynamic properties of drugs used for the treatment of severemalaria. Exp. Parasitol. 76: 85–95.
Thapa, B. R., Marwaha, R. K., Kumar, L. and Mehta, S. (1988)Cerebral malaria in children: therapeutic considerations.Ind. Paediatr. 25: 61–65.
Thomas, J. D. (1971) Clinical and histopathological correlation ofcerebral malaria. Trop. Geogr. Med. 23: 232–238.
Thomson, J. G. and Annecke, S. (1926) Observations of thepathology of the central nervous system in malignant tertianmalaria, with remarks on certain clinical phenomena. J. Trop.Med. Hyg. 29: 313–346.
Thuma, P. E., Weiss, G., Herold, M. and Gordeuk, V. R. (1996)Serum neopterin, interleukin-4, and interleukin-6 concentra-tions in cerebral malaria patients and the effect of iron chela-tion therapy. Am. J. Trop. Med. Hyg. 54: 164–168.
Thuma, P. E., Mabeza, G. F., Biemba, G., Bhat, G. J., McLaren,C. E., Moyo, V. M., Zulu, S., Khumalo, H., Mabeza, P.,M’Hango, A. M., Parry, D., Poltera, A. A., Brittenham, G. M.and Gordeuk, V. R. (1998) Effect of iron chelation therapy onmortality in Zambian children with cerebral malaria. Trans. R.Soc. Trop. Med. Hyg. 92: 214–218.
Thumwood, C. M., Hunt, N. H., Clark, I. A. and Cowden, W. B.(1988) Breakdown of the blood-brain barrier in murine cerebralmalaria. Parasitology 96 (Part 3): 579–589.
Thumwood, C. M., Hunt, N. H., Cowden, W. B. and Clark, I. A.(1989) Antioxidants can prevent cerebral malaria in Plasmo-dium berghei-infected mice. Br. J. Exp. Pathol. 70: 293–303.
Thun-Hohenstein, L., Schmitt, B., Steinlin, H., Martin, E. andBoltshauser, E. (1992) Cortical visual impairment following bac-terial meningitis: magnetic resonance imaging and visual evokedpotentials findings in two cases. Eur. J. Pediatr. 151: 779–782.
Toro, G. and Roman, G. (1978) Cerebral malaria. A disseminatedvasculomyelinopathy. Arch. Neurol. 35: 271–275.
Tran, T. H., Day, N. P., Ly, V. C., Nguyen, T. H., Pham, P. L.,Nguyen, H. P., Bethell, D. B., Dihn, X. S. and White, N. J.(1996a) Blackwater fever in southern Vietnam: a prospectivedescriptive study of 50 cases. Clin. Infect. Dis. 23: 1274–1281.
Tran, T. H., Day, N. P., Nguyen, H. P., Nguyen, T. H., Pham, P. L.,Dinh, X. S., Ly, V. C., Ha, V., Waller, D., Peto, T. E. andWhite, N. J. (1996b) A controlled trial of artemether or qui-nine in Vietnamese adults with severe falciparum malaria [seecomments]. N. Engl. J. Med. 335: 76–83.
Trang, T. T., Phu, N. H., Vinh, H., Hien, T. T., Cuong, B. M.,Chau, T. T., Mai, N. T., Waller, D. J. and White, N. J. (1992)Acute renal failure in patients with severe falciparum malaria.Clin. Infect. Dis. 15: 874–880.
Trape, J. F., Quinet, Q. M. C., Nzigoula, S., Senga, P., Tchichelle,F., Carme, B., Candito, D., Mayanda, H. and Zoulani, A. (1987)Malaria and urbanization in central Africa: the example of Braz-zaville. Part V: pernicious attacks and mortality. Trans. R.Soc. Trop. Med. Hyg. 81 (Suppl. 2): 34–42.
Treluyer, J. M., Roux, A., Mugnier, C., Flouvat, B. and Lagardere,B. (1996) Metabolism of quinine in children with global mal-nutrition. Pediatr. Res. 40: 558–563.
Treutiger, C. J., Hedlund, I., Helmby, H., Carlson, J., Jepson, A.,Twumasi, P., Kwiatkowski, D., Greenwood, B. M. and Wahlgren,M. (1992) Rosette formation in Plasmodium falciparum isolatesand anti-rosette activity of sera from Gambians with cerebral oruncomplicated malaria. Am. J. Trop. Med. Hyg. 46: 503–510.
Turner, G. (1997) Cerebral malaria. Brain Pathol. 7: 569–582.Turner, G. D. H., Morrison, H., Jones, M., Davis, T. M. E., Looa-
reesuwan, S., Buley, I. D., Gatter, K. C., Newbold, C. I. andPukrittayakamee, S. (1994) An immunohistochemical study ofthe pathology of fatal malaria. Am. J. Pathol. 145: 1057–1069.
Udomsangpetch, R., Wåhlin, B., Carlson, J., Berzins, K., Torii, M.,Aikawa, M., Perlmann, P. and Wahlgren, M. (1989) Plasmo-dium falciparum-infected erythrocytes form spontaneous eryth-rocyte rosettes. J. Exp. Med. 169: 1835–1840.
Udomsangpetch, R., Thanikkul, K., Pukrittayakamee, S. andWhite, N. J. (1995) Rosette formation by Plasmodium vivax.Trans. R. Soc. Trop. Med. Hyg. 89: 635–637.
Udomsangpetch, R., Pipitaporn, B., Krishna, S., Angus, B., Pukrit-tayakamee, S., Bates, I., Suputtamongkol, Y., Kyle, D. E. andWhite, N. J. (1996) Antimalarial drugs reduce cytoadherence androsetting of Plasmodium falciparum. J. Infect. Dis. 173: 691–698.
Usawattanakul, W., Tharavanij, S., Warrell, D. A., Looareesuwan,S., White, N. J., Supavej, S. and Soikratoke, S. (1985) Factors

52 C. R. J. C. Newton and S. Krishna
contributing to the development of cerebral malaria. II. Endo-toxin. Clin. Exp. Immunol. 61: 562–568.
Vallance, P. and Collier, J. (1994) Biology and clinical relevanceof nitric oxide. Br. Med. J. 309: 453–456.
Van den Ende, J., Moorkens, G., Van Gómpel, A., Demey, H.,Lins, R., Maldague, P., Pelfrene, E., Van den Enden, E., Tael-man, H., Van der Stuyft, P. and Colebunders, R. (1994) Twelvepatients with severe malaria treated with partial exchange trans-fusion. Comparison between mathematically predicted andobserved effect on parasitaemia. Trop. Geogr. Med 46: 340–345.
van Hensbroek, M. B. (1996) Cerebral malaria in children: patho-genesis, treatment and outcome. Ph.D. Thesis, University ofAmsterdam.
van Hensbroek, M. B., Onyiorah, E., Jaffar, S., Schneider, G.,Palmer, A., Frenkel, J., Enwere, G., Forck, S., Nusmeijer, A.,Bennett, S., Greenwood, B. and Kwiatkowski, D. (1996a) Atrial of artemether or quinine in children with cerebral malaria.N. Engl. J. Med. 335: 69–75.
van Hensbroek, M. B., Palmer, A., Onyiorah, E., Schneider, G.,Jaffar, S., Dolan, G., Memming, H., Frenkel, J., Enwere, G., Ben-nett, S., Kwiatkowski, D. and Greenwood, B. (1996b) The effectof a monoclonal antibody to tumor necrosis factor on survivalfrom childhood cerebral malaria. J. Infect. Dis. 174: 1091–1097.
van Hensbroek, M., Palmer, A., Jaffar, S., Schneider, G. and Kwi-atkowski, D. (1997) Residual neurologic sequelae after child-hood malaria. J. Pediatr. 131: 125–129.
Vanijanonta, S., Chantra, A., Phophak, N., Chindanond, D., Cle-mens, R. and Pukrittayakamee, S. (1996) Therapeutic effects ofchloroquine in combination with quinine in uncomplicated fal-ciparum malaria. Ann. Trop. Med. Parasitol. 90: 269–275.
Vietze, G. (1978) Malaria and other protozoal diseases. In: Infec-tions of the Nervous System, Part III, Handbook of ClinicalNeurology, Vol. 35, pp. 143–160, Vinken, P. J. and Bruyn, G. W.(eds.) Elsevier/North Holland Biomedical Press, Amsterdam.
von Seidlein, L., Jaffar, S. and Greenwood, B. M. (1997) Prolon-gation of the QTc interval in African children treated for falci-parum malaria. Am. J. Trop. Med. Hyg. 56: 494–497.
Vouldoukis, I., Rivernos-Moreno, V., Dugas, B., Ouaaz, F.,Becherael, P., Debre, P., Moncada, S. and Mossalayi, M. D.(1995) The killing of Leishmania major by human macrophagesby nitric oxide induced after the ligation of FCeRII/CD23 sur-face antigen. Proc. Natl. Acad. Sci. USA 92: 7804–7808.
Wahlgren, M., Carlson, J., Udomsangpetch, R. and Perlmann, P.(1991) Why do Plasmodium falciparum-infected erythrocytes formspontaneous erythrocyte rosettes. Parasitol. Today 5: 183–185.
Walker, O., Salako, L. A., Sowunmi, A., Thomas, J. O., Sodeine,O. and Bondi, F. S. (1992) Prognostic risk factors and post mor-tem findings in cerebral malaria in children. Trans. R. Soc.Trop. Med. Hyg. 86: 491–493.
Walker, O., Salako, L. A., Omokhodion, S. I. and Sowunmi, A.(1993) An open randomized comparative study of intramuscu-lar artemether and intravenous quinine in cerebral malaria inchildren. Trans. R. Soc. Trop. Med. Hyg. 87: 564–566.
Waller, D., Krishna, S., Craddock, C., Brewster, D., Jammeh, A.,Kwiatkowski, D., Karbwang, J., Molunto, P. and White, N. J.(1990) The pharmacokinetic properties of intramuscular qui-nine in Gambian children with severe falciparum malaria.Trans. R. Soc. Trop. Med. Hyg. 84: 488–491.
Waller, D., Crawley, J., Nosten, F., Chapman, S., Krishna, S.,Craddock, C., Brewster, D. and White, N. J. (1991) Intracra-nial pressure in childhood cerebral malaria. Trans. R. Soc.Trop. Med. Hyg. 85: 362–364.
Waller, D., Krishna, S., Crawley, J., Miller, K., Nosten, F., Chap-man, D., ter Kuile, F. O., Craddock, C., Berry, C., Holloway, P. A.,Brewster, D., Greenwood, B. M. and White, N. J. (1995) Clini-cal features and outcome of severe malaria in Gambian chil-dren. Clin. Infect. Dis. 21: 577–587.
Warrell, D. A. (1987) Pathophysiology of severe falciparummalaria in man. Parasitology 94 (Suppl.): S53–S76.
Warrell, D. A. (1989) Cerebral malaria [editorial]. Q. J. Med. 71:369–371.
Warrell, D. A., Looareesuwan, S., Warrell, M. J., Kasemsarn, P.,Intaraprasert, R., Bunnag, D. and Harinasuta, T. (1982a) Dexam-ethasone proves deleterious in cerebral malaria. A double-blindtrial in 100 comatose patients. N. Engl. J. Med. 306: 313–319.
Warrell, D. A., White, N. J. and Warrell, M. J. (1982b) Dexa-methasone deleterious in cerebral malaria [letter]. Br. Med. J.[Clin. Res.] 285: 1652.
Warrell, D. A., Looareesuwan, S., Phillips, R. E., White, N. J.,Warrell, M. J., Chapel, H. M., Areekul, S. and Tharavanij, S.(1986) Function of the blood-cerebrospinal fluid barrier inhuman cerebral malaria: rejection of the permeability hypothe-sis. Am. J. Trop. Med. Hyg. 35: 882–889.
Warrell, D. A., White, N. J., Veall, N., Looareesuwan, S., Chantha-vanich, P., Phillips, R. E., Karbwang, J., Pongpaew, P. and Krishna,S. (1988) Cerebral anaerobic glycolysis and reduced cerebraloxygen transport in human cerebral malaria. Lancet ii: 534–538.
Warrell, D. A., Molyneux, M. E. and Beales, P. F. (1990) Severeand complicated malaria. Trans. R. Soc. Trop. Med. Hyg. 84(Suppl. 2): 1–65.
Waruiru, C. M., Newton, C. R. Forster, D., New, L., Winstanley,P., Mwangi, I., Marsh, V., Winstanley, M., Snow, R. W. andMarsh, K. (1996) Epileptic seizures and malaria in Kenyan chil-dren. Trans. R. Soc. Trop. Med. Hyg. 90: 152–155.
Wasterlain, C. G. and Shirasaka, Y. (1994) Seizures, brain damageand brain development. Brain Dev. 16: 279–295.
Watkins, W. M., Woodrow, C. and Marsh, K. (1993) Falciparummalaria: differential effects of antimalarial drugs on ex vivo para-site viability during the critical early phase of therapy. Am. J.Trop. Med. Hyg. 49: 106–112.
Wattanagoon, Y., Srivilairit, S., Looareesuwan, S. and White, N. J.(1994) Convulsions in childhood malaria. Trans. R. Soc. Trop.Med. Hyg. 88: 426–428.
Wei, X., Charles, I. G., Smith, A., Ure, J., Feng, G., Huang, F.,Xu, D., Muller, W., Moncada, S. and Liew, F. Y. (1995) Alteredimmune response in mice lacking inducible nitric oxide syn-thase. Nature 375: 408–411.
Weiss, G., Thuma, P. E., Mabeza, G., Werner, E. R., Herold, M.and Gordeuk, V. R. (1997) Modulatory potential of iron chela-tion therapy on nitric oxide formation in cerebral malaria. J.Infect. Dis. 175: 226–230.
Westendorp, R. G. J., Langermans, J. A. M., Huizinga, T. W. J.,Elouali, A. H., Verweij, C. L., Boomsma, D. I. and Vanden-borouke, J. P. (1997) Genetic influence in cytokine productionand fatal meningococcal disease. Lancet 349: 170–173.
Weston, M. J., Jackman, N., Rudge, C., Bowles, J., Brady, C.,Bielawska, C. and O’Grady, J. (1982) Prostacyclin in falci-parum malaria. Lancet ii: 609.
White, N. J. (1991) Lumbar puncture in cerebral malaria. Lancet338: 640–641.
White, N. J. (1992) Antimalarial drug resistance: the pace quick-ens. J. Antimicrob. Chemother. 30: 571–585.
White, N. J. and Ho, M. (1992) The pathophysiology of malaria.Adv. Parasitol. 31: 83–173.

Pathophysiology and Supportive Treatment of Severe Malaria 53
White, N. J. and Krishna, S. (1989) Treatment of malaria: someconsiderations and limitations of the current methods of assess-ment. Trans. R. Soc. Trop. Med. Hyg. 83: 767–777.
White, N. J. and Looareesuwan, S. (1987) Cerebral malaria. In:Infections of the Nervous System, pp. 118–143, Kennedy, P. G. E.and Johnson, R. T. (eds.) Butterworths, London.
White, N. J., Warrell, D. A., Chanthavanich, P., Looareesuwan,S., Warrell, M. J., Krishna, S., Williamson, D. H. and Turner,R. C. (1983) Severe hypoglycemia and hyperinsulinemia in fal-ciparum malaria. N. Engl. J. Med. 309: 61–66.
White, N. J., Warrell, D. A., Looareesuwan, S., Chanthavanich,P., Phillips, R. E. and Pongpaew, P. (1985) Pathophysiologicaland prognostic significance of cerebrospinal-fluid lactate incerebral malaria. Lancet i: 776–778.
White, N. J., Miller, K. D., Brown, J., Marsh, K. and Greenwood,B. M. (1987a) Prognostic value of CSF lactate in cerebralmalaria [letter]. Lancet i: 1261.
White, N. J., Miller, K. D., Marsh, K., Berry, C. D., Turner, R. C.,Williamson, D. H. and Brown, J. (1987b) Hypoglycaemia inAfrican children with severe malaria. Lancet i: 708–711.
White, N. J., Watt, G., Bergqvist, Y. and Njelesani, E. K. (1987c)Parenteral chloroquine for treating falciparum malaria. J. Infect.Dis. 155: 192–201.
White, N. J., Looareesuwan, S., Phillips, R. E., Chanthavanich, P.and Warrell, D. A. (1988) Single dose phenobarbitone preventsconvulsions in cerebral malaria. Lancet ii: 64–66.
White, N. J., Chapman, D. and Watt, G. (1992a) The effects ofmultiplication and synchronicity on the vascular distribution ofparasites in falciparum malaria. Trans. R. Soc. Trop. Med. Hyg.86: 590–597.
White, N. J., Krishna, S. and Looareesuwan, S. (1992b) Encepha-litis, not cerebral malaria, is likely cause of coma with negativeblood smears [letter]. J. Infect. Dis. 166: 1195–1196.
Whitehead, S. and Peto, T. E. (1990) Stage-dependent effect ofdeferoxamine on growth of Plasmodium falciparum in vitro.Blood 76: 1250–1255.
Wick, T. M. and Louis, V. (1991) Cytoadherence of Plasmodiumfalciparum-infected erythrocytes to human umbilical vein andhuman dermal microvascular endothelial cells under shear con-ditions. Am. J. Trop. Med. Hyg. 45: 578–586.
Wilkinson, R. J., Brown, J. L., Pasvol, G., Chiodini, P. L. andDavidson, R. N. (1994) Severe falciparum malaria: predictingthe effect of exchange transfusion. Q. J. Med. 87: 553–557.
Winstanley, P. A., Newton, C. R. J. C., Pasvol, G., Kirkham, F. J.,Mberu, E., Peshu, N., Ward, A. A., Were J. B. O., Warrell, D. A.and Marsh, K. (1992) Prophylactic phenobarbitone in youngchildren with severe falciparum malaria: pharmacokinetics andclinical effects. Br. J. Clin. Pharmacol. 33: 149–154.
Winstanley, P., Newton, C., Watkins, W., Mberu, E., Ward, S.,Warn, P., Mwangi, I., Waruiru, C., Pasvol, G., Warrell, D. andMarsh, K. (1993) Towards optimal regimens of parenteral qui-nine for young African children with cerebral malaria: theimportance of unbound quinine concentration. Trans. R. Soc.Trop. Med. Hyg. 87: 201–206
Winstanley, P. A., Mberu, E. K., Watkins, W. M., Murphy, S. A.,Lowe, B. and Marsh, K. (1994) Towards optimal regimens ofparenteral quinine for young African children with cerebralmalaria: unbound quinine concentrations following a simple load-ing dose regimen. Trans. R. Soc. Trop. Med. Hyg. 88: 577–580.
Wolf-Gould, C., Osei, L., Commey, J. O. O. and Bia, F. J. (1991)Pediatric cerebral malaria in Accra, Ghana. J. Trop. Pediatr. 38:290–294.
Woodruff, A. W. and Dickinson, C. J. (1968) Use of dexametha-sone in cerebral malaria. Br. Med. J. 3: 31–32.
World Health Organisation (1993) A global strategy to controlmalaria. Report No. 839, Geneva.
World Health Organisation (1996) Malaria. Report No. 94 Factsheet, Geneva.
Wright, B. D. (1968) The effect of neonatal thymectomy on thesurvival of golden hamsters infected with Plasmodium berghei.Br. J. Exp. Pathol. 49: 379–384.
Wright, D. H., Masembe, R. M. and Bazira, E. R. (1971) Theeffect of anti-thymocyte serum on golden hamsters infectedwith Plasmodium berghei. Br. J. Exp. Pathol. 52: 465–477.
Wright, P. W., Avery, W. G., Ardill, W. D. and McLarty, J. W.(1993) Initial clinical assessment of the comatose patient: cere-bral malaria vs. meningitis. Pediatr. Infect. Dis. J. 12: 37–41.
Yen, L. M., Dao, L. M., Day, N. P., Waller, D. J., Bethell, D. B.,Son, L. H., Hien, T. T. and White, N. J. (1994) Role of quininein the high mortality of intramuscular injection tetanus. Lancet344: 786–787.
Zucker, J. R., Lackritz, E. M., Ruebush, T. K., Hightower, A. W.,Adungosi, J. E., Were, J. B., Metchock, B., Patrick, E. andCampbell, C. C. (1996) Childhood mortality during and afterhospitalization in western Kenya: effect of malaria treatmentregimens. Am. J. Trop. Med. Hyg. 55: 655–660.






![Review Article TheHostGeneticDiversityinMalariaInfection§a V R R T… · against P. falciparum malaria [37] and protection against severe malaria forms [38]. The presence of a single](https://img.pdfslide.net/doc/110x75/5f095af17e708231d42670a9/review-article-thehostgeneticdiversityinmalariainfection-a-v-r-r-t-against-p.jpg)
![Long-term Behavioral Problems in Children With Severe …pediatrics.aappublications.org/content/pediatrics/138/5/...consciousness (Blantyre coma score [BCS] ≤2) and Plasmodium falciparum](https://img.pdfslide.net/doc/110x75/5ac1a5947f8b9a5a4e8d6456/long-term-behavioral-problems-in-children-with-severe-blantyre-coma-score-bcs.jpg)