Embed Size (px)
Citation preview
Introduction
High-resolution ultrasonography (US) has been provedto be a reliable and accurate imaging modality in theevaluation of scrotal abnormalities in children [1±3].Simple intratesticular cysts are rare in children andhave been considered the most uncommon cause ofscrotal cystic masses in this age group. The exact etiolo-gy of these lesions is still unclear.
Preoperative sonographic diagnosis is extremely im-portant in order to plan conservative surgery, with exci-sion of the cyst and preservation of the testis [3±6]. Inthis paper we report on five infants who exhibited ascrotal mass and had a simple intratesticular cyst, all di-agnosed preoperatively by sonography, with histologicalcorrelation.
Materials and methods
We reviewed the clinical characteristics and sonographical, intra-operative, and pathological findings for five children undergoingtesticular surgery for a simple cyst. The patients' mean age was7 months (a range of from 4 to 10 months), and they all presentedwith a nontender, unilateral scrotal swelling that was clinically feltas a testicular mass and was detected during a routine physical ex-amination; three of the cases involved the right testis and two, theleft testis. Two patients were siblings and all the infants were other-wise normal.
High-resolution ultrasonography (US) of the scrotum was per-formed preoperatively, with 7.5-mHz or 12-mHz transducers beingused in every case. All patients had scrotal surgery. Surgical speci-mens were sent for pathological examination, where morphologicand histologic characteristics were studied. Follow-up scrotal USwas performed between 2 and 11 months after surgery on three pa-tients.
Cristiµn J. GarcíaSergio Zu æigaHelmar RosenbergJosØ D.ArceFelipe Zu æiga
Simple intratesticular cysts in children:preoperative sonographic diagnosisand histological correlation
Received: 13 November 1998Accepted: 24 May 1999
C.J. García ()) ´ S. Zu æiga ´H. RosenbergHospital Clínico Universidad Católica,Departamentos de Radiologia,Cirurgia y Anatomia PatológicaMarcoleta 367, Santiago, Chile
J.D. ArceServicio de Radiologia,Unidad BaumØdica, Santiago, Chile
F. Zu æigaFacultad de Medicina Sur,Universidad de Chile, Santiago, Chile
Abstract Background. Simple in-tratesticular cysts are rare in chil-dren and have been considered themost uncommon cause of scrotalcystic masses in this age group. Theexact etiology of these lesions is stillunclear. High-resolution ultra-sonography has been proved to be areliable and accurate imaging mo-dality in the evaluation of scrotalabnormalities in children.Patients and methods. We report thesonographic findings in five boysaged from 4 to 10 months who pre-sented with a scrotal mass and had asimple intratesticular cyst. Ultra-sonography showed that all of themdisplayed a characteristic appear-ance and provided the necessary in-formation to perform conservativesurgery, with testicular preservation
in four infants. In one infant, the cystinvolved most of the testis, and anorchiectomy was performed.Results. Pathological examinationrevealed a single smooth-walledcystic structure, with clear and se-rous fluid, lined with flattened epi-thelial cells in all of the infants.Conclusion. Our findings appear tosupport the hypothesis that thesecysts could correspond to mesothe-lial inclusions. Sonographically, dif-ferential diagnosis should includemainly epidermoid cysts of the tes-tis, which are mostly cystic but char-acteristically contain some echoeswithin them, in contrast to simplecysts and cysts of the tunica albugin-ea, which lie outside the testicularparenchyma.
Pediatr Radiol (1999) 29: 851±855Ó Springer-Verlag 1999
Results
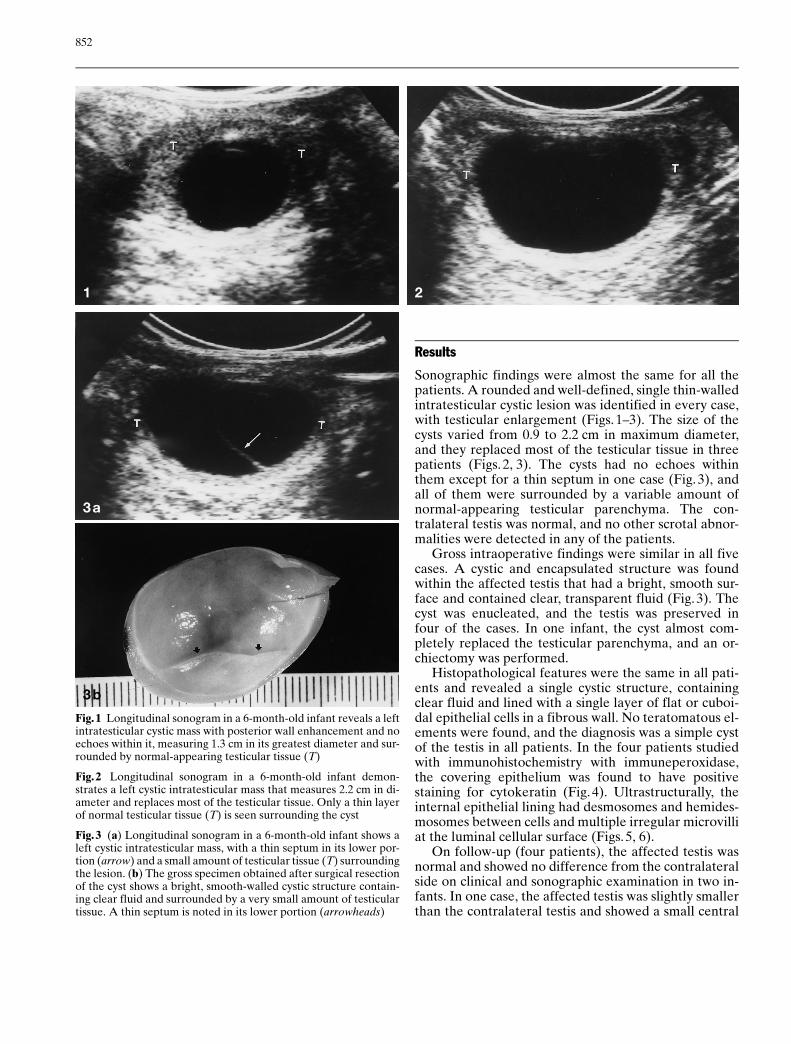
Sonographic findings were almost the same for all thepatients. A rounded and well-defined, single thin-walledintratesticular cystic lesion was identified in every case,with testicular enlargement (Figs. 1±3). The size of thecysts varied from 0.9 to 2.2 cm in maximum diameter,and they replaced most of the testicular tissue in threepatients (Figs. 2, 3). The cysts had no echoes withinthem except for a thin septum in one case (Fig. 3), andall of them were surrounded by a variable amount ofnormal-appearing testicular parenchyma. The con-tralateral testis was normal, and no other scrotal abnor-malities were detected in any of the patients.
Gross intraoperative findings were similar in all fivecases. A cystic and encapsulated structure was foundwithin the affected testis that had a bright, smooth sur-face and contained clear, transparent fluid (Fig. 3). Thecyst was enucleated, and the testis was preserved infour of the cases. In one infant, the cyst almost com-pletely replaced the testicular parenchyma, and an or-chiectomy was performed.
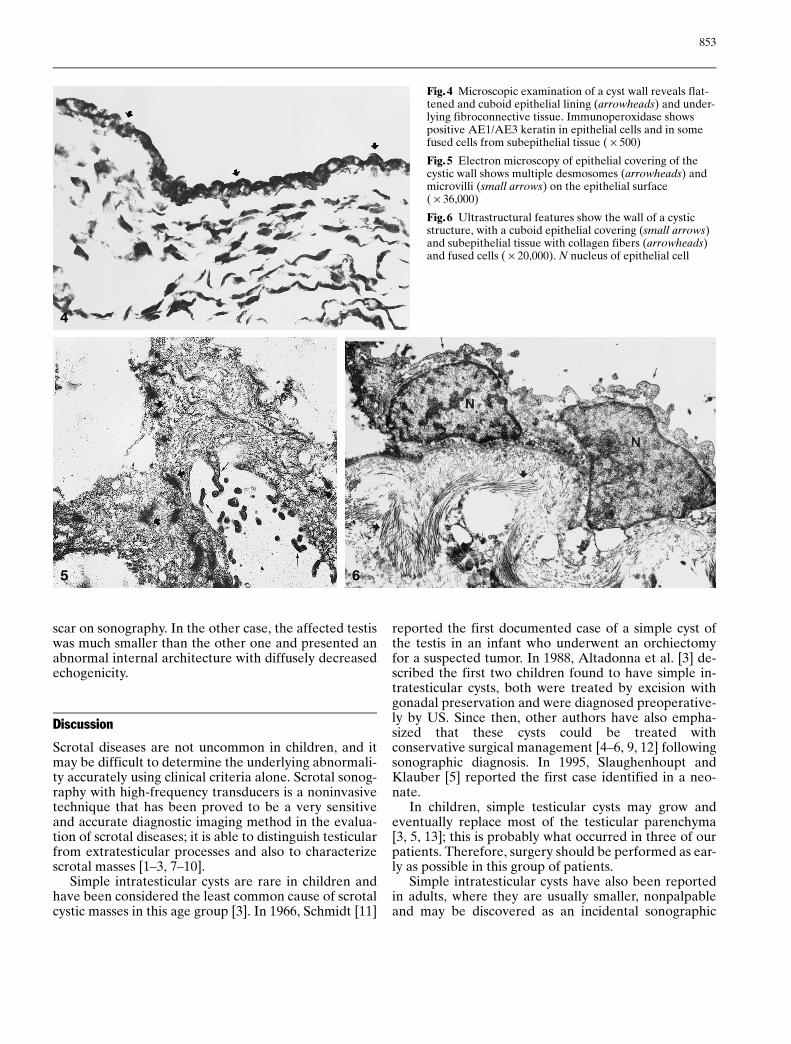
Histopathological features were the same in all pati-ents and revealed a single cystic structure, containingclear fluid and lined with a single layer of flat or cuboi-dal epithelial cells in a fibrous wall. No teratomatous el-ements were found, and the diagnosis was a simple cystof the testis in all patients. In the four patients studiedwith immunohistochemistry with immuneperoxidase,the covering epithelium was found to have positivestaining for cytokeratin (Fig. 4). Ultrastructurally, theinternal epithelial lining had desmosomes and hemides-mosomes between cells and multiple irregular microvilliat the luminal cellular surface (Figs.5, 6).
On follow-up (four patients), the affected testis wasnormal and showed no difference from the contralateralside on clinical and sonographic examination in two in-fants. In one case, the affected testis was slightly smallerthan the contralateral testis and showed a small central
852
1 2
3a
3b
Fig.1 Longitudinal sonogram in a 6-month-old infant reveals a leftintratesticular cystic mass with posterior wall enhancement and noechoes within it, measuring 1.3 cm in its greatest diameter and sur-rounded by normal-appearing testicular tissue (T)
Fig.2 Longitudinal sonogram in a 6-month-old infant demon-strates a left cystic intratesticular mass that measures 2.2 cm in di-ameter and replaces most of the testicular tissue. Only a thin layerof normal testicular tissue (T) is seen surrounding the cyst
Fig.3 (a) Longitudinal sonogram in a 6-month-old infant shows aleft cystic intratesticular mass, with a thin septum in its lower por-tion (arrow) and a small amount of testicular tissue (T) surroundingthe lesion. (b) The gross specimen obtained after surgical resectionof the cyst shows a bright, smooth-walled cystic structure contain-ing clear fluid and surrounded by a very small amount of testiculartissue. A thin septum is noted in its lower portion (arrowheads)
scar on sonography. In the other case, the affected testiswas much smaller than the other one and presented anabnormal internal architecture with diffusely decreasedechogenicity.
Discussion
Scrotal diseases are not uncommon in children, and itmay be difficult to determine the underlying abnormali-ty accurately using clinical criteria alone. Scrotal sonog-raphy with high-frequency transducers is a noninvasivetechnique that has been proved to be a very sensitiveand accurate diagnostic imaging method in the evalua-tion of scrotal diseases; it is able to distinguish testicularfrom extratesticular processes and also to characterizescrotal masses [1±3, 7±10].
Simple intratesticular cysts are rare in children andhave been considered the least common cause of scrotalcystic masses in this age group [3]. In 1966, Schmidt [11]
reported the first documented case of a simple cyst ofthe testis in an infant who underwent an orchiectomyfor a suspected tumor. In 1988, Altadonna et al. [3] de-scribed the first two children found to have simple in-tratesticular cysts, both were treated by excision withgonadal preservation and were diagnosed preoperative-ly by US. Since then, other authors have also empha-sized that these cysts could be treated withconservative surgical management [4±6, 9, 12] followingsonographic diagnosis. In 1995, Slaughenhoupt andKlauber [5] reported the first case identified in a neo-nate.
In children, simple testicular cysts may grow andeventually replace most of the testicular parenchyma[3, 5, 13]; this is probably what occurred in three of ourpatients. Therefore, surgery should be performed as ear-ly as possible in this group of patients.
Simple intratesticular cysts have also been reportedin adults, where they are usually smaller, nonpalpableand may be discovered as an incidental sonographic
853
4
5 6
Fig.4 Microscopic examination of a cyst wall reveals flat-tened and cuboid epithelial lining (arrowheads) and under-lying fibroconnective tissue. Immunoperoxidase showspositive AE1/AE3 keratin in epithelial cells and in somefused cells from subepithelial tissue ( ´ 500)
Fig.5 Electron microscopy of epithelial covering of thecystic wall shows multiple desmosomes (arrowheads) andmicrovilli (small arrows) on the epithelial surface( ´ 36,000)
Fig.6 Ultrastructural features show the wall of a cysticstructure, with a cuboid epithelial covering (small arrows)and subepithelial tissue with collagen fibers (arrowheads)and fused cells ( ´ 20,000). N nucleus of epithelial cell

finding; they have a higher incidence than in children [2,6, 8, 9, 12, 14±17] and may not change in size for a longperiod of time [5, 8]. Most of them are not detected byphysical examination [5].
The exact pathogenesis of simple cysts of the testis isnot clear, and various pathogenetic theories have beenpostulated. The wide age range of patients at the timeof clinical presentation suggests the possibility of morethan one etiology, although inclusion of ectopic epithe-lial cells from remnants of wolffian or mullerian ductshas been thought to be the most plausible explanationin infants [8, 9, 11, 12, 16]. Others have postulated thatthey could be derived from the testicular tubules ornests of celomic mesothelium [13, 18] or be post-trau-matic or post-inflammatory [8, 9, 16], mostly in adults,where they might originate from the rete testis [2, 3, 19].
Our findings would support the theory that simple in-tratesticular cysts may correspond to simple mesothelialcysts.
The fact that most cases reported in children corre-spond to infants [3, 11, 16], including our five patients,suggests that in young children, testicular cysts may becongenital and may then grow after birth until they arediscovered, in most cases incidentally. A genetic predis-position should also be considered, particularly in viewof the fact that the five cases studied included two sib-lings with this condition. We did not find this previouslyreported in the literature, and it obviously needs confir-mation. Testicular US might be recommended as ascreening procedure for all infants with a sibling knownto have this type of lesion.
Morphologically, simple intratesticular cysts are usu-ally well delineated, isolated, and contain clear serousfluid, without any cellular elements. Histologically theyare lined by flattened epithelial cells, with areas ofcuboidal cells supported by cellular connective tissueand surrounded by normal testicular tissue [9, 11, 19].Sonographically, simple cysts within the testicular pa-
renchyma must be distinguished from other cystlikespace-occupying lesions. The differential diagnosis of asolitary cystic testicular mass using US should take intoconsideration epidermoid cysts, cysts of the tunica al-buginea, intratesticular cysts, and cystic mature terato-mas. Cystic areas may also be found in tumors and inintratesticular abscesses or hematomas that may some-times display cystic changes. Characteristically, simpleintratesticular cysts appear as a single, thin-walled an-echoic intratesticular mass, with posterior wall enhance-ment and no internal echoes [3±5, 7, 16].
Epidermoid cysts of the testis are more common inadults, and sonographically they are similar in appear-ance to simple cysts; however, they are usually sur-rounded by a ring of higher echogenicity, the wall mayappear thick, they contain some internal echoes becauseof keratin deposits, and acoustic enhancement may beabsent [8, 20±23].
Cysts of the tunica albuginea are also simple cysts,but are located at the testicular surface. They usually ap-pear in adults and can be easily identified by US [24, 25].
Cystic testicular teratoma is rare in children andcharacteristically appears as an inhomogeneous masson US, often with cystic spaces caused by its varied tis-sue elements [26]. Only rarely will some mature terato-mas present a predominantly cystic appearance [2].Other testicular neoplasms may occasionally containcystic areas, but these areas are usually within a larger,primarily solid mass [2].
Although rare, simple intratesticular cysts should beconsidered in the differential diagnosis of unilateralpainless testicular enlargement in young children. Thediagnosis is easily made by US, and surgery should beindicated as early as possible in order to permit the pres-ervation of the testis. The prognosis for the testicle willdepend mostly on the amount of normal testicular pa-renchyma remaining at the time of surgery.
854
References
1. Finkelstein MS, Rosenberg HK, SnyderHM, et al (1986) Ultrasound evaluationof the scrotum in pediatrics. Urology 28:1±9
2. Hamm B, Fobbe F, Volker L (1988)Testicular cysts: differentiation with USand clinical findings. Radiology 168:19±23
3. Altadonna V, Snyder HM, RosenbergHK, et al (1988) Simple cysts of the tes-tis in children: preoperative diagnosisby ultrasound and excision with testicu-lar preservation. J Urol 140: 1505±1507
4. Peretsman SJ, Maldazys JD (1995) In-fantile testicular cyst: diagnosis andconservative surgical management.J Pediatr Surg 30: 1488±1489
5. Slaughenhoupt, Klauber GT (1995)Simple intratesticular cyst in a neonate.J Pediatr Surg 30: 1488±1489
6. Kratzik CH, Hainz A, Kuber W, et al(1990) Surveillance strategy for intra-testicular cysts: preliminary report.J Urol 143: 313±315
7. Rifkin MD, Jacobs JA (1983) Simpletesticular cysts diagnosed preoperative-ly by ultrasound. J Urol 129: 982±983
8. Hobarth K, Kratzik CH (1992) High-resolution ultrasonography in the diag-nosis of simple intratesticular cysts. Br JUrol 70: 546±549
9. Takihara H, Valvo JR, Tokuhara M,et al (1982) Intratesticular cysts. Urolo-gy 20: 80±82
10. Haas GP, Shumaker BP, Cerny JC(1986) The high incidence of benigntesticular tumors. J Urol 136: 1219±1222
11. Schmidt SS (1966) Congenital simplecyst of the testis: a hitherto undescribedlesion. J Urol 96: 236±238
12. Haber MM, Cohen MB ( 1992) Simplecyst of the testis. Urology 39: 563±565

855
13. Kaplan GW (1988) Editorial comment.J Urol 140: 1507
14. Leung ML, Gooding GAW, WilliamsRD (1984) High-resolution sonographyof scrotal contents in asymptomaticsubjects. AJR 143: 161±164
15. Gooding GAW, Leonhard W, Stein R(1987) Testicular cysts: US findings.Radiology 163: 537±538
16. Dmochowsky RR, Rudy DC, CorriereJN (1989) Simple cysts of the testis.J Urol 142: 1078±1081
17. Belville WD, Insalaco SJ, Dresner M,et al (1982) Benign testis tumors. J Urol128: 1198±1200
18. Nistal M, Paniagua R (1984) Testicularand epidydimal pathology, Thieme-Stratton, New York
19. Nistal M, Iæiguez L, Paniagua R (1989)Cysts of the testicular parenchyma andtunica albuginea. Arch Lab Med 113:902±906
20. Shah KH, Maxted WC, Chun B (1981)Epidermoid cysts of the testis: a reportof three cases and an analysis of 141cases from the world literature. Cancer47: 577±582
21. Price EB (1969) Epidermoid cysts ofthe testis: a clinical and pathologicanalysis of 69 cases from the testiculartumor registry. J Urol 102: 708±713
22. Buckspan MB, Skeldon SL, Klotz PG,et al (1985) Epidermoid cysts of thetesticle. J Urol 134: 960±964
23. Heidenreich A, Engelmann UH,Vietsch HV, et al (1995) Organ preserv-ing surgery in testicular epidermoidcysts. J Urol 153: 1147±1150
24. Warner KE, Noyes DT, Ross JS (1984)Cysts of the tunica albuginea: a reportof three cases with a review of the liter-ature. J Urol 132: 131±132
25. Mevorach RA, Lerner RM, Linke C,et al (1985) Ultrasound diagnosis of tu-nica albuginea cysts. Clinical perspec-tive. Urology 25: 551±553
26. Liu P, Phillips MJ, Edwards VD, et al(1992) Sonographic findings of testicu-lar teratoma with pathological correla-tion. Pediatr Radiol 22: 99±101