Embed Size (px)
Citation preview
560 Vol. 4, No. 10 n November/December 2004
CASE REPORTA healthy 45-year-old man (a physician) developed a
papule on his left arm while attending a yoga retreat in thejungle near Puerto Viejo, Costa Rica. Three weeks afterreturning from Costa Rica, the papule became more nodu-lar and itchy. Initially, he thought this was an inflammatoryreaction, but the papule did not respond to self-prescribedtopical triamcinolone ointment.
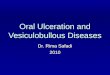
About 10 weeks after the exposure, the lesion began toulcerate and ooze serous fluid. Examination of the papulerevealed a 6-cm 3 5-cm erythematous nodular ulceratedlesion with a raised indurated border and central crusting(Figure 1). At this stage, the patient presented to his prima-ry care physician (PCP), who arranged a biopsy. The patientsuggested that a sand fly might have bitten him prior to thedevelopment of the papule.
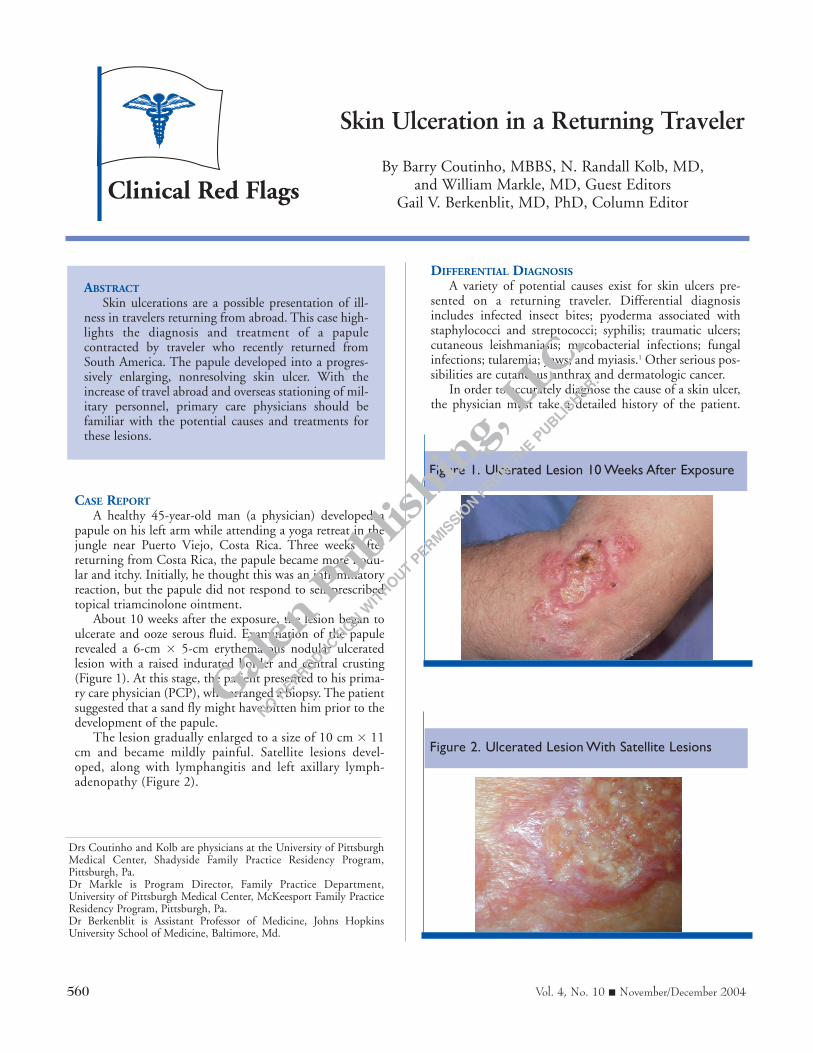
The lesion gradually enlarged to a size of 10 cm 3 11cm and became mildly painful. Satellite lesions devel-oped, along with lymphangitis and left axillary lymph-adenopathy (Figure 2).
DIFFERENTIAL DIAGNOSISA variety of potential causes exist for skin ulcers pre-
sented on a returning traveler. Differential diagnosisincludes infected insect bites; pyoderma associated withstaphylococci and streptococci; syphilis; traumatic ulcers;cutaneous leishmaniasis; mycobacterial infections; fungalinfections; tularemia; yaws; and myiasis.1 Other serious pos-sibilities are cutaneous anthrax and dermatologic cancer.
In order to accurately diagnose the cause of a skin ulcer,the physician must take a detailed history of the patient.
Clinical Red Flags
Drs Coutinho and Kolb are physicians at the University of PittsburghMedical Center, Shadyside Family Practice Residency Program,Pittsburgh, Pa.Dr Markle is Program Director, Family Practice Department,University of Pittsburgh Medical Center, McKeesport Family PracticeResidency Program, Pittsburgh, Pa.Dr Berkenblit is Assistant Professor of Medicine, Johns HopkinsUniversity School of Medicine, Baltimore, Md.
Skin Ulceration in a Returning Traveler
By Barry Coutinho, MBBS, N. Randall Kolb, MD, and William Markle, MD, Guest Editors
Gail V. Berkenblit, MD, PhD, Column Editor
ABSTRACTSkin ulcerations are a possible presentation of ill-
ness in travelers returning from abroad. This case high-lights the diagnosis and treatment of a papulecontracted by traveler who recently returned fromSouth America. The papule developed into a progres-sively enlarging, nonresolving skin ulcer. With theincrease of travel abroad and overseas stationing of mil-itary personnel, primary care physicians should befamiliar with the potential causes and treatments forthese lesions.
Figure 1. Ulcerated Lesion 10 Weeks After Exposure
Figure 2. Ulcerated Lesion With Satellite Lesions

Advanced Studies in Medicine 561
CLINICAL RED FLAGS
PCPs should consider recent travel locations and local diseasepatterns and exposure. Physical characteristics should beassessed, along with a combination of either microscopicanalysis of skin scrapings, punch biopsy, serologic testing, orneedle aspiration and culture.
With this in mind, physicians should understand which testis appropriate to make a proper diagnosis. When used for cuta-neous leishmaniasis, serologic testing has low sensitivity and islikely to produce a negative result early in the disease course.2
Serologic testing is more useful in helping to diagnose syphilis,yaws, or tularemia. Biopsy and culture are helpful in diagnosingbacterial and fungal infections. Cutaneous anthrax can be iden-tified by its appearance; this includes edema out of proportionto the size of the lesion, gram staining, and culture results of theulcer exudate. In this case, the patient’s biopsy showed leishman-iasis with amastigotes.
Cutaneous leishmaniasis, a vector-borne parasitic disease, isendemic in areas of the tropics, subtropics, and southernEurope. Travelers—including military personnel—who visit orthose who live in these areas are at an increased risk for this dis-ease.3 In October 2003, cases of cutaneous leishmaniasis werereported among US military personnel serving in Iraq (especial-ly in the urban and periurban areas of An Nasiriyah andBaghdad), near the Iraqi border in Kuwait, and in Afghanistan.3
Parasites from the genus Leishmania, such as Leishmaniabraziliensis and Leishmania mexicana, cause cutaneous leishman-iasis. The disease is transmitted when an individual is bitten bya female sand fly.
TREATMENTPatients returning from various South American countries
(eg, Colombia, Costa Rica, Honduras, Venezuela) have possi-bly contracted L braziliensis. These patients require adequatesystemic therapy, since their symptoms are more likely toprogress to a mucocutaneous disease than those infected byother Leishmania species.1
Reasons for seeking early treatment include the growth ofchronic or multiple lesions, the appearance of cosmeticallyunacceptable lesions, the spread of lesions over the joints,lesions found on immunosuppressed patients, or the develop-ment of associated lymphangitis.4 In these situations, the pre-ferred treatment is intravenous (IV) pentavalent antimonialcompound sodium stibogluconate. Other treatment optionsinclude amphotericin-B and ketoconazole.
Effective treatment of cutaneous leishmaniasis is usuallyachieved with pentavalent antimonial compound sodium sti-bogluconate at a dosage of 20 mg/kg a day for 20 days.Unfortunately, this product is not licensed for use in theUnited States. However, the military is provided with sodiumstibogluconate under the Investigational New Drug (IND)protocols held by the Surgeon General of the Army with theUS Food and Drug Administration (FDA). The Centers forDisease Control and Prevention has a separate IND protocolwith the FDA, which allows for provision of this drug to civil-ians infected with leishmaniasis.3
Side effects from antimony treatment are common andinclude malaise, anorexia, myalgia, and arthralgia. Antimonytreatment is associated with elevations in serum aminotransferas-
es, chemical pancreatitis, mild leukopenia, and thrombocytope-nia. Electrocardiogram (ECG) changes, including T- wave flat-tening and prolongation of the Q-T interval, also are possible.Whereas treatment should be monitored, in most cases theseabnormalities settle rapidly upon completion of therapy. Once apatient begins treatment, lesions usually heal within a month andbecome progressively less indurated and flatter with subsequentepithelialization; larger lesions may take longer to heal.1,2
After consultation with an infectious disease specialist, thepatient received treatment at the Family Health Center inPittsburgh. Based on the epidemiology of diseases acquired inCosta Rica and the behavior of the skin lesions, the patient’s con-dition was diagnosed as secondary to L braziliensis. Treatmentbegan and tissue samples were sent for a confirmatory culture.During the course of treatment, the patient developed significantgeneralized arthralgias, mild elevations of lipase, and mild ECGabnormalities, which improved after completion of therapy.Figure 3 shows the regression of the lesion after 9 days of therapy;by the final day of treatment, the lesion was an asymptomaticatrophic scar.
CONCLUSIONCutaneous leishmaniasis is an uncommon disease among
returning US travelers. However, when evaluating a patientwith a progressive ulcerative lesion, travel history and poten-tial exposure always should be considered. With the increaseof travel abroad by private citizens and military personnel,physicians should be aware of the diagnosis and treatmentmethods for this disease.
References1. Hepburn NC. Cutaneous leishmaniasis: an overview. J Postgrad Med.
2003;49:50-54.2. Cutaneous leishmaniasis of the New World. In: Hunter GW, Strickland
GT, eds. Hunter's Tropical Medicine and Emerging Infectious Diseases. 8thed. Philadelphia: Saunders; 2000:665-687.
3. Aronson N, Coleman R, Coyne P, et al. Cutaneous leishmaniasis in USmilitary personnel: Southwest/Central Asia, 2002-2003. MMWR MorbMortal Wkly Rep. 2003;52:1009-1012.
4. Markle WH, Makhoul K. Cutaneous leishmaniasis: recognition andtreatment. Am Fam Physician. 2004;69:455-460.
Figure 3. Lesion After Treatment


![Patient education for preventing diabetic foot ulceration … · [Intervention Review] Patient education for preventing diabetic foot ulceration Johannes AN Dorresteijn 1, Didi MW](https://img.pdfslide.net/doc/110x75/5ecb99029d0d2c34515c80a4/patient-education-for-preventing-diabetic-foot-intervention-review-patient.jpg)